Vitamin D and Graves’ Disease: A Meta-Analysis Update

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Outcomes Measures
2.5. Statistical Analysis
3. Results
3.1. Information of the Included Studies

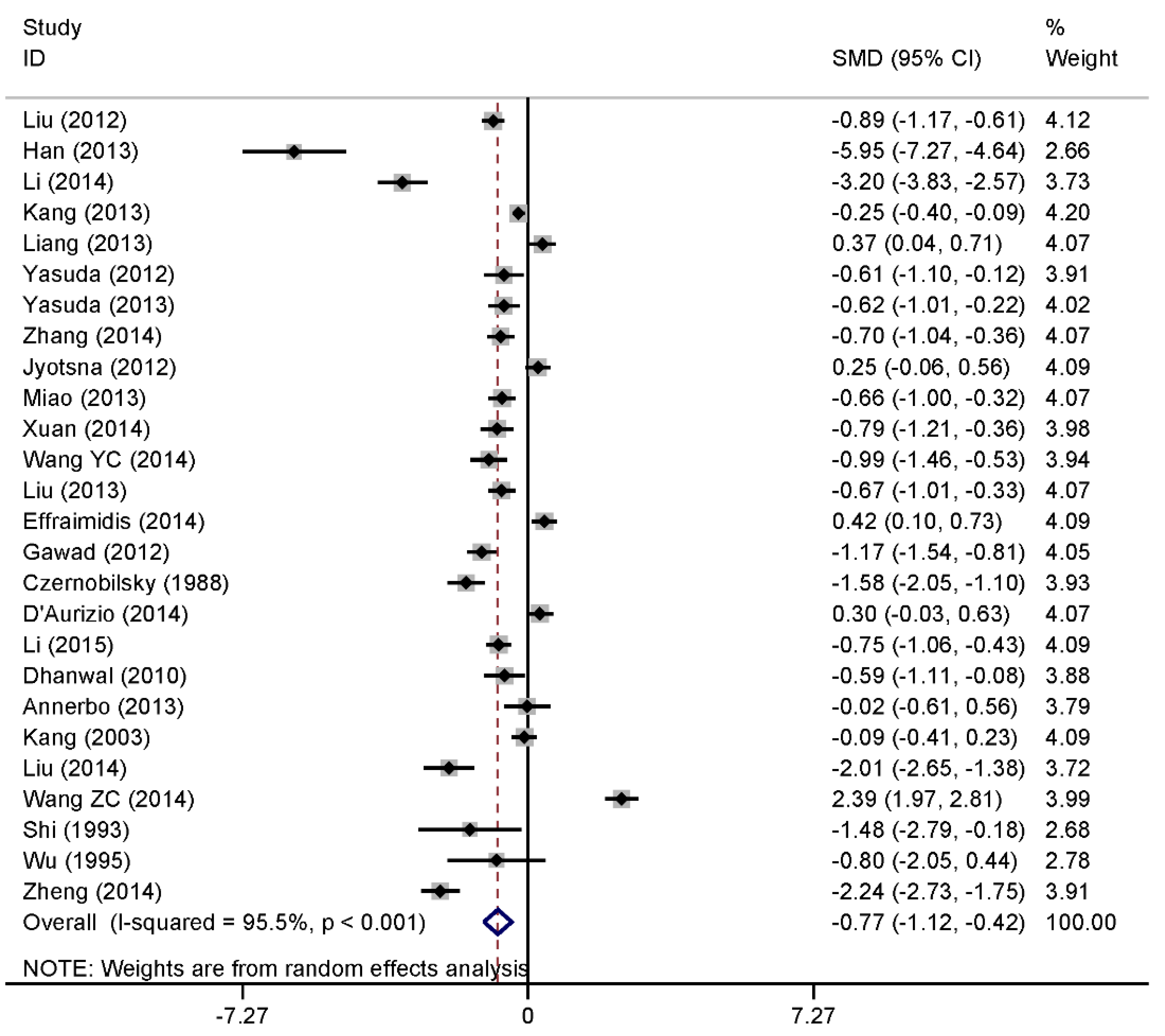
3.2. Continuous Data of Vitamin D Level and Graves’ Disease
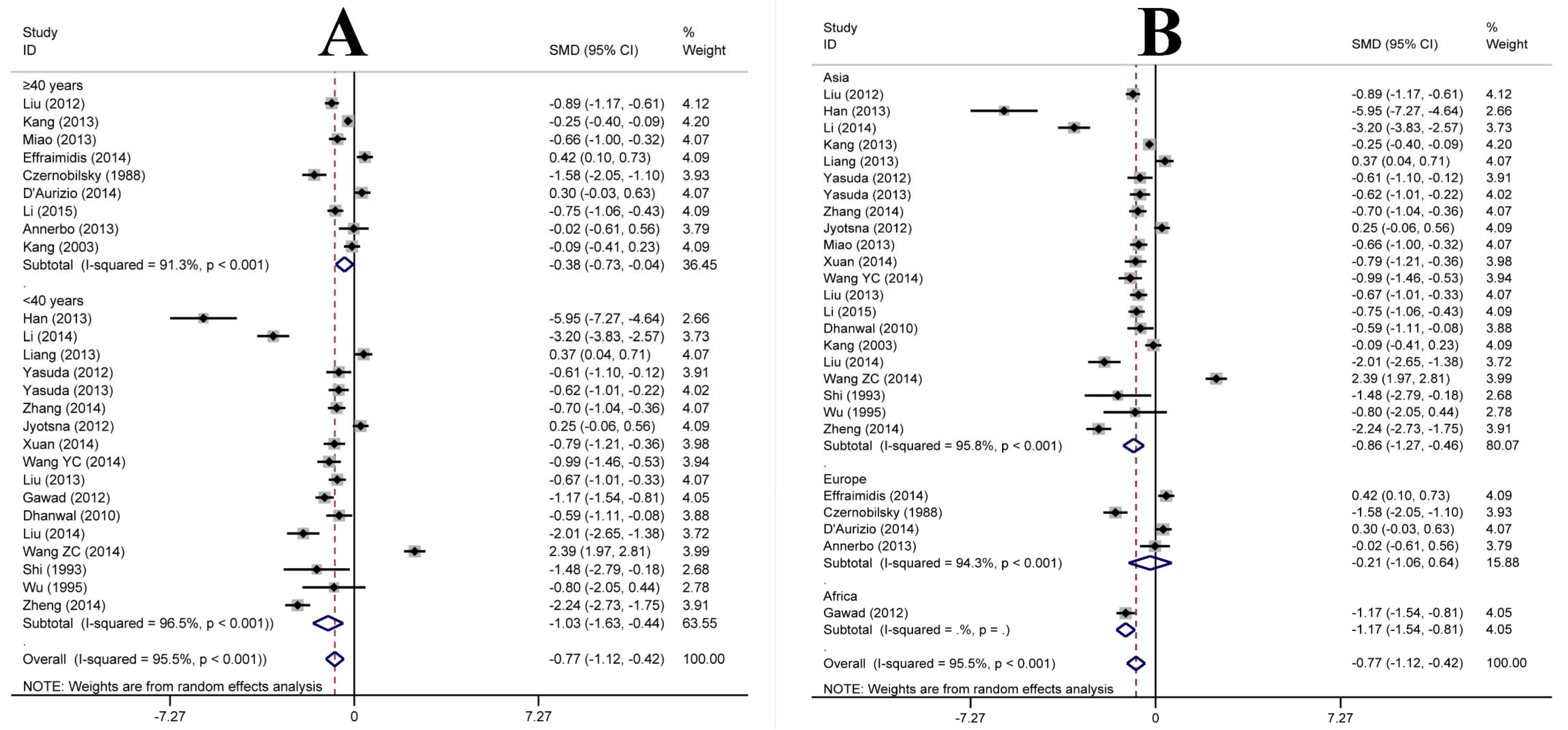
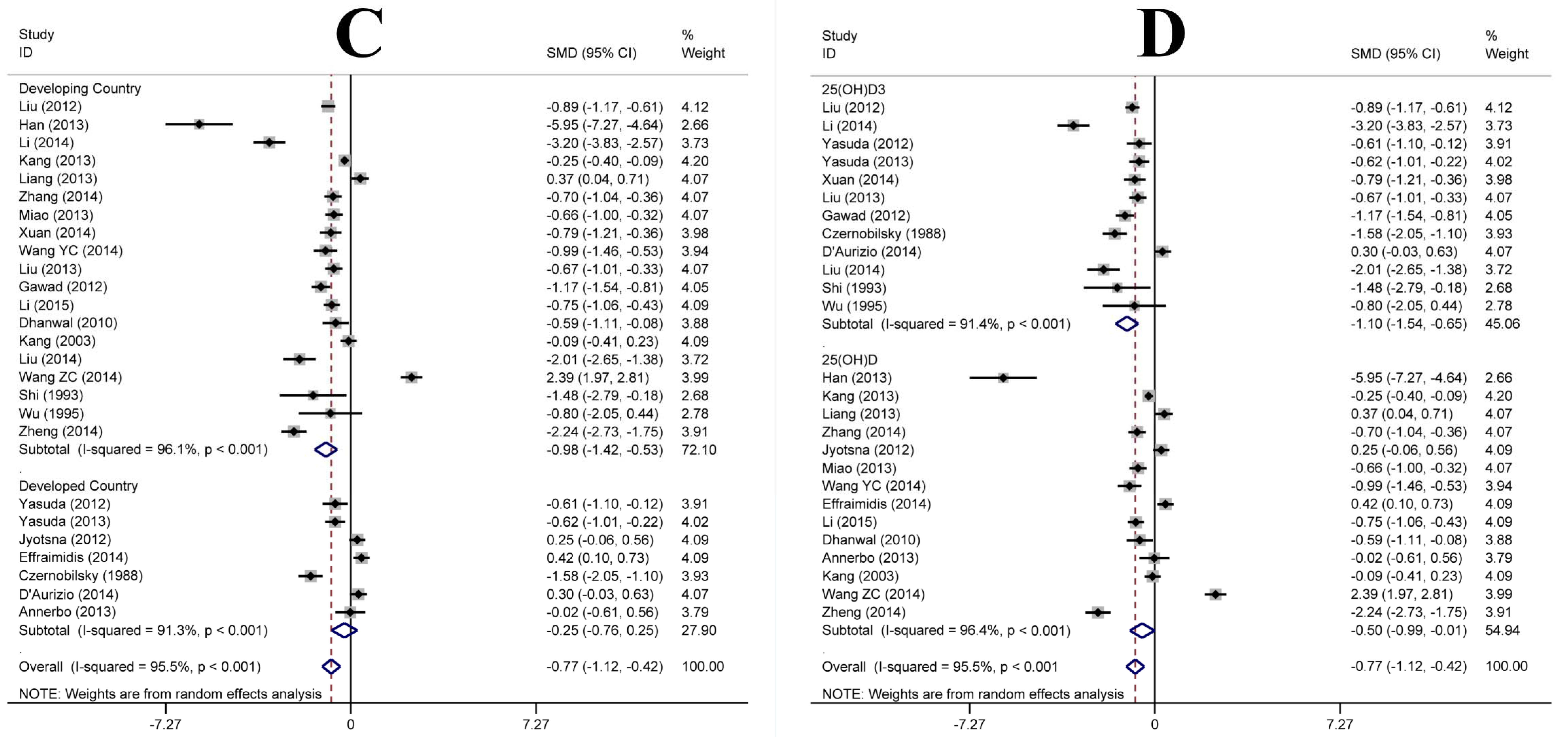
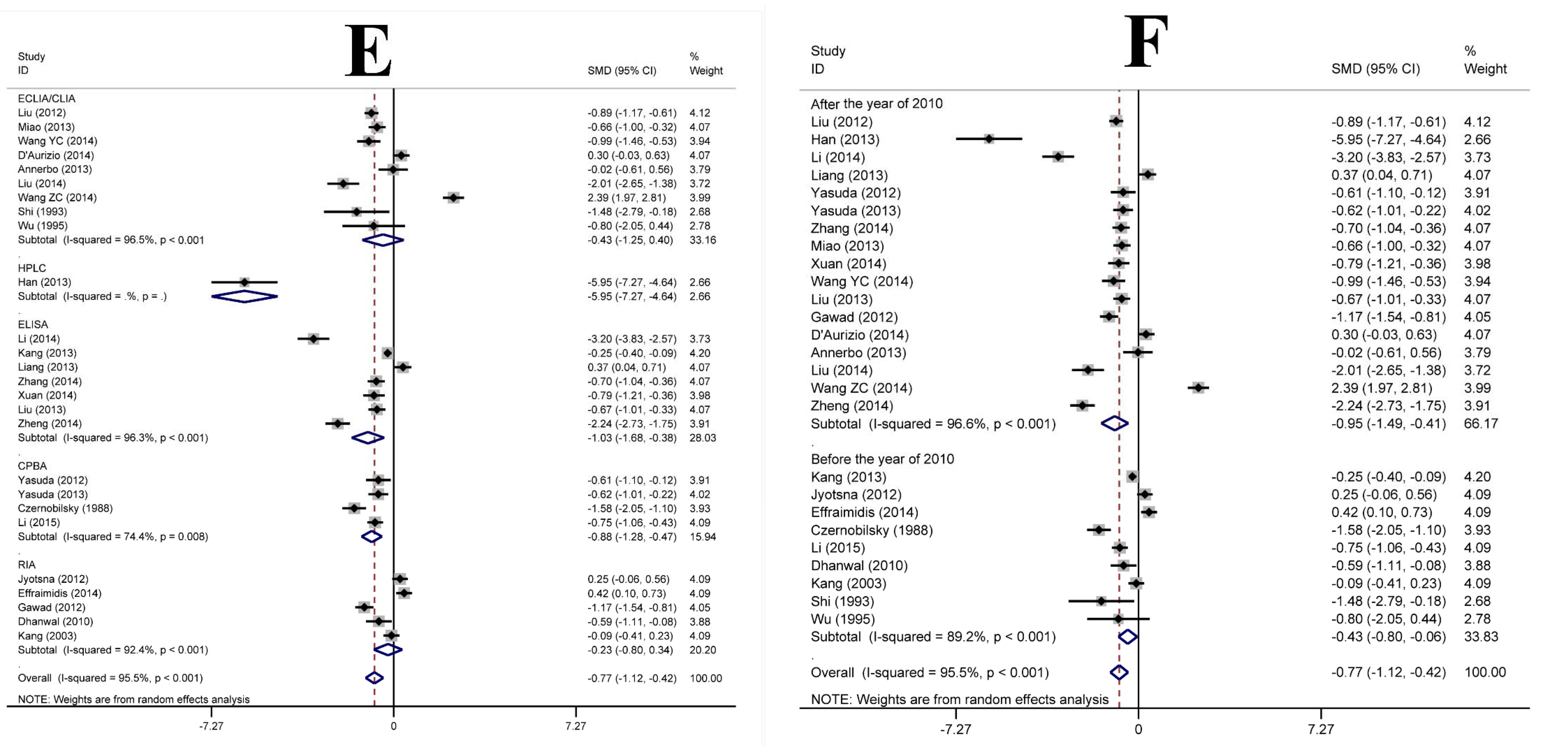
3.3. Subgroup Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | First Author | Year | Country | Study Year | Age of Patients (Mean ± SD) | Detection Index | Assay Method | Sample Size (Case/Control) | Quality Score * |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Li et al. [26] | 2015 | China/Jiangsu | 2010 | 41 ± 10 | 25(OH)D | CPBA | 128/60 | 9 |
| 2 | Li et al. [5] | 2014 | China/Shanxi | 2011–2012 | 34 ± 14 | 25(OH)D3 | ELISA | 40/50 | 8 |
| 3 | Zhang et al. [13] | 2015 | China/Hunan | 2012–2012 | 34 ± 12 | 25(OH)D | ELISA | 70/70 | 8 |
| 4 | Xuan et al. [10] | 2014 | China/Jiangsu | 2013–2014 | 33 ± 12 | 25(OH)D3 | ELISA | 47/45 | 7 |
| 5 | Wang Y.C. et al. [8] | 2014 | China/Anhui | 2013 | 35 ± 8 | 25(OH)D | ECLIA | 60/30 | 7 |
| 6 | Effraimidis et al. [24] | 2012 | Netherland | 2003 | 42 ± 13 | 25(OH)D | RIA | 78/78 | 9 |
| 7 | D’Aurizio et al. [22] | 2015 | Italy | 2014 | 47 ± 16 | 25(OH)D3 | CLIA | 48/126 | 9 |
| 8 | Liu et al. [27] | 2014 | China/Hebei | 2013 | 34 ± 11 | 25(OH)D3 | ECLIA | 35/24 | 9 |
| 9 | Wang Z.S. et al. [9] | 2014 | China/Hainan | 2012–2013 | 32 ± 5 | 25(OH)D | ECLIA | 62/91 | 7 |
| 10 | Zheng et al. [17] | 2014 | China/Zhejiang | 2010–2011 | 36 ± 8 | 25(OH)D | ELISA | 72/39 | 7 |
| 11 | Han et al. [16] | 2013 | China/Guangdong | 2012–2013 | 36 ± 7 | 25(OH)D | HPLC | 30/20 | 7 |
| 12 | Kang et al. [14] | 2013 | China/Shandong | 2009–2010 | 43 ± 8 | 25(OH)D | ELISA | 280/439 | 7 |
| 13 | Liang et al. [31] | 2013 | China/Hunan | 2012–2012 | 34 ± 12 | 25(OH)D | ELISA | 70/70 | 9 |
| 14 | Yasuda et al. [12] | 2013 | Japan | 2011 | 38 ± 7 | 25(OH)D3 | CPBA | 54/49 | 8 |
| 15 | Miao et al. [7] | 2013 | China/Liaoning | 2011–2012 | 40 ± 15 | 25(OH)D | ECLIA | 70/70 | 9 |
| 16 | Liu et al. [28] | 2013 | China/Jiangsu | 2011–2012 | 37 ± 11 | 25(OH)D3 | ELISA | 118/50 | 9 |
| 17 | Annerbo et al. [20] | 2014 | Sweden | 2009–2012 | 41 ± 14 | 25(OH)D | ECLIA | 56/14 | 9 |
| 18 | Liu et al. [6] | 2012 | China/Henan | 2010–2011 | 42 ± 9 | 25(OH)D3 | ECLIA | 80/165 | 8 |
| 19 | Yasuda et al. [11] | 2012 | Japan | 2011 | 37 ± 13 | 25(OH)D3 | CPBA | 26/46 | 8 |
| 20 | Jyotsna et al. [4] | 2012 | India | 2006–2008 | 36 ± 11 | 25(OH)D | RIA | 80/80 | 7 |
| 21 | Abd El Gawad et al. [19] | 2012 | Egypt | 2011 | 38 ± 5 | 25(OH)D3 | RIA | 90/55 | 9 |
| 22 | Kivity et al. [15] | 2011 | Israel | 2006 | 45 ± 16 | 25(OH)D | ECLIA | 22/98 | 8 |
| 23 | Dhanwal et al. [23] | 2010 | India | 2010 | 34 ± 9 | 25(OH)D | RIA | 30/31 | 8 |
| 24 | Kang et al. [25] | 2003 | China/Tianjin | 2000 | 45 ± 12 | 25(OH)D | RIA | 74/80 | 7 |
| 25 | Wu et al. [30] | 1995 | China/Shanghai | 1990 | NA | 25(OH)D3 | ECLIA | 6/5 | 6 |
| 26 | Shi et al. [29] | 1993 | China/Shanghai | 1991 | 32 ± 4 | 25(OH)D3 | ECLIA | 6/6 | 7 |
| 27 | Czernobilsky et al. [21] | 1988 | Germany | 1988 | 40 ± 10 | 25(OH)D3 | CPBA | 38/55 | 9 |




3.4. Meta Regression Analysis
| Factor | Coefficient | SE | 95% CI | t | p | |
|---|---|---|---|---|---|---|
| Age | −0.18 | 0.65 | −1.54 | 1.17 | −0.29 | 0.779 |
| Geographic location | 0.11 | 0.6 | −1.15 | 1.37 | 0.18 | 0.858 |
| Country type | −1.33 | 0.73 | −2.85 | 0.19 | −1.83 | 0.083 |
| Detection index | −0.60 | 0.58 | −1.80 | 0.61 | −1.04 | 0.312 |
| Assay method | −0.58 | 0.27 | −1.16 | −0.01 | −2.11 | 0.048 |
| Study period | −0.53 | 0.64 | −1.86 | 0.81 | −0.82 | 0.420 |
| Constant | 4.75 | 2.33 | −0.13 | 9.63 | 2.04 | 0.056 |
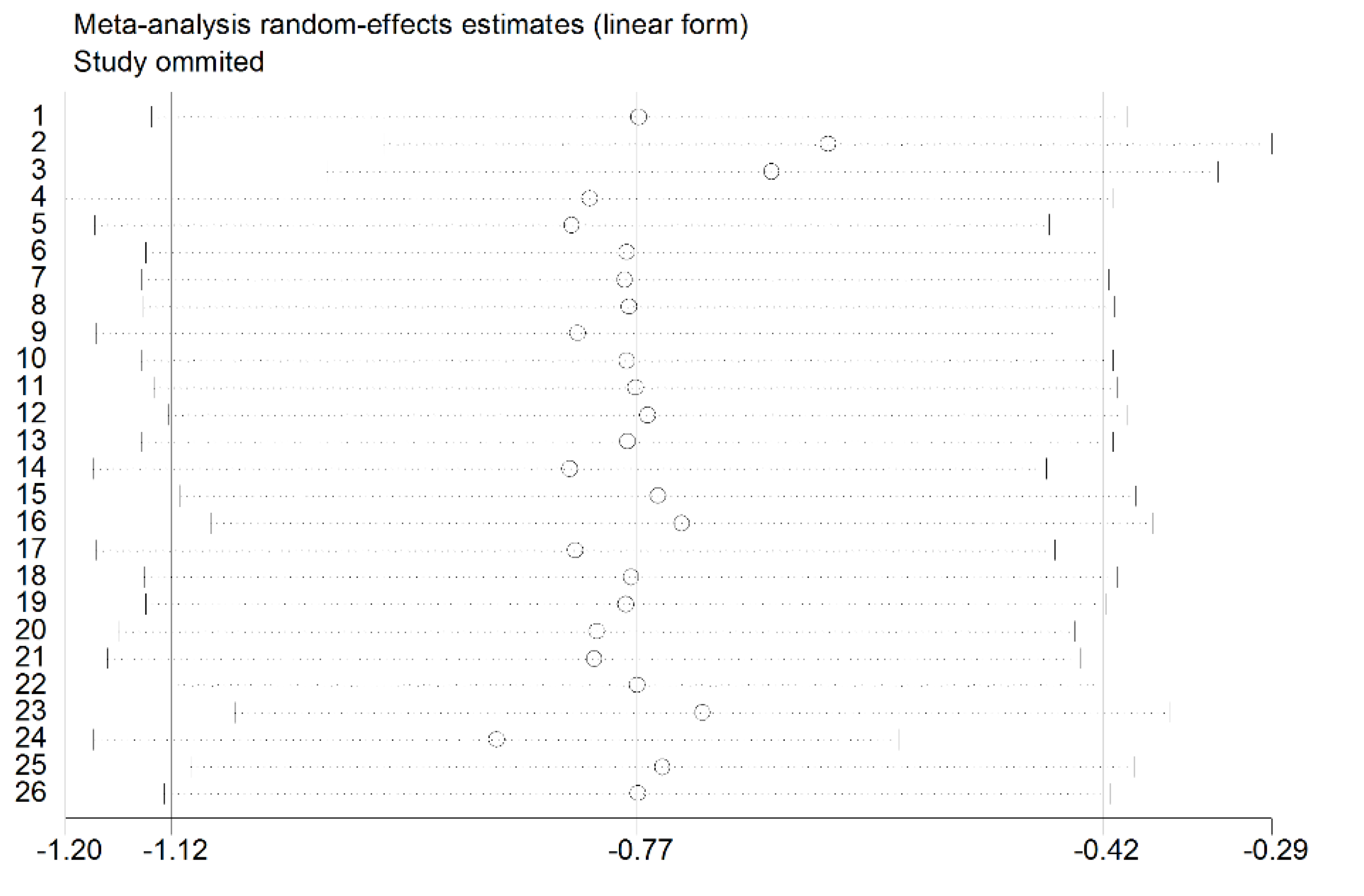
3.5. Sensitivity Analysis

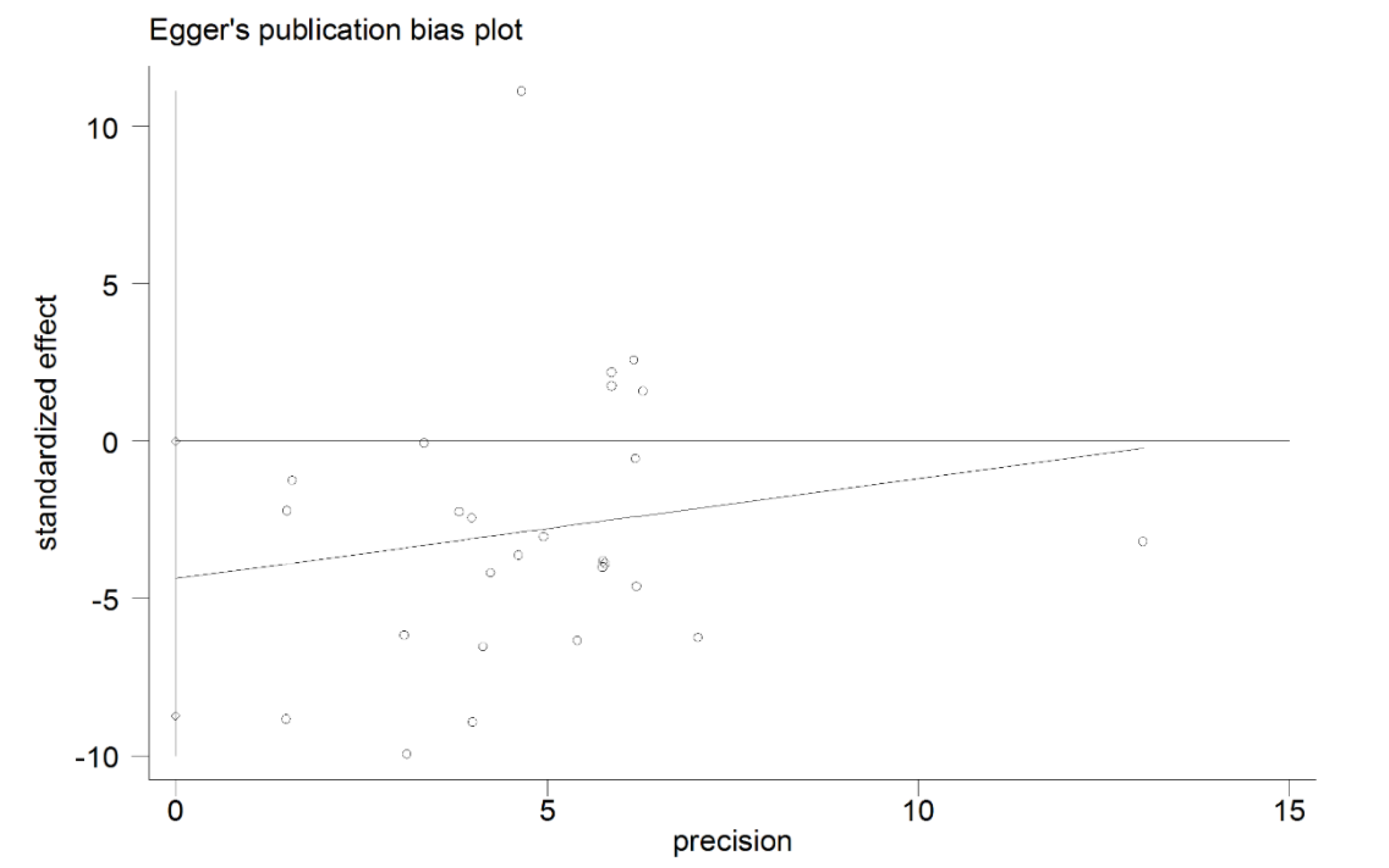
3.6. Publication Bias

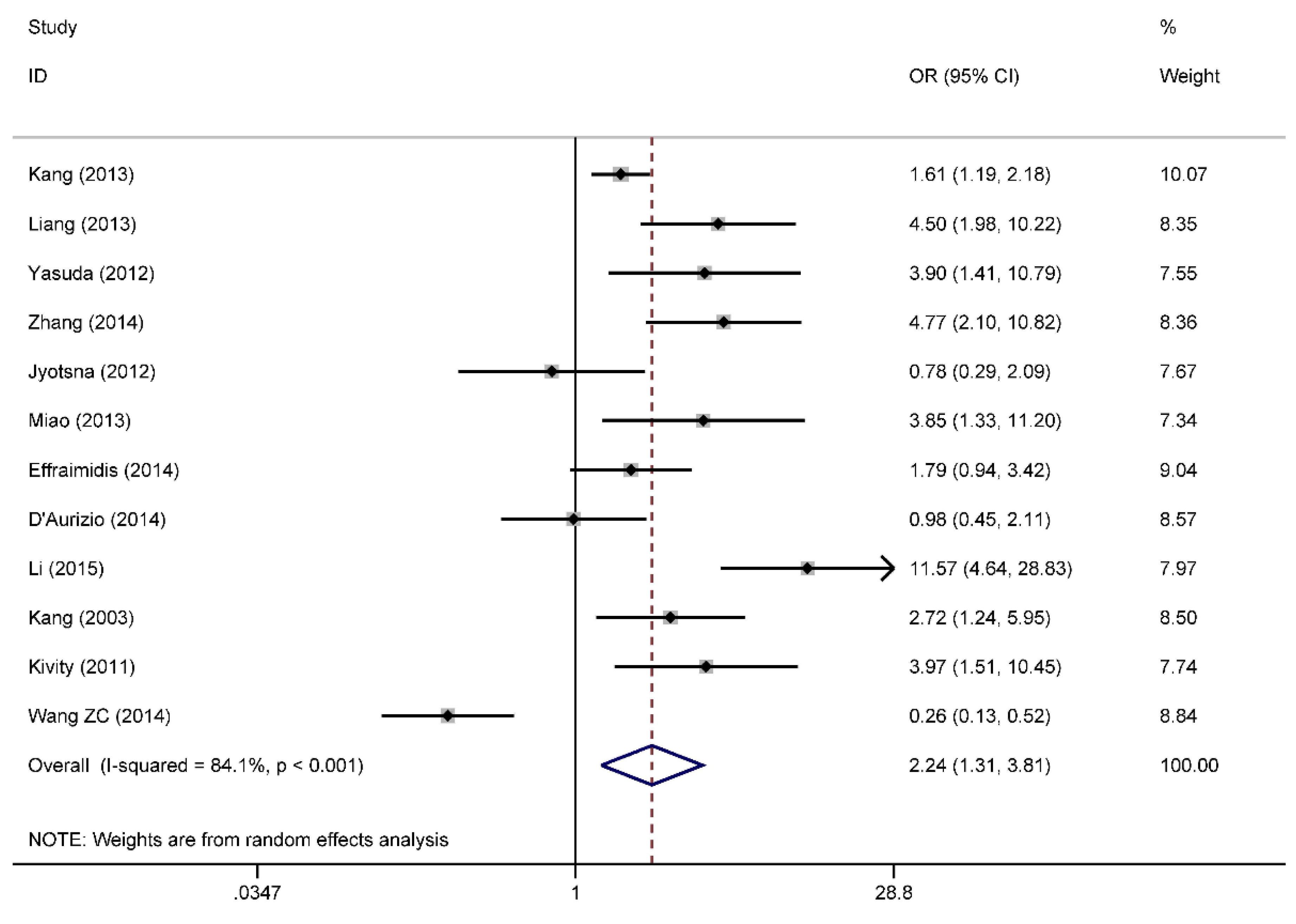
3.7. Categorical Data of Vitamin D Level and Graves’ Disease
4. Discussion


Acknowledgments
Author Contributions
Conflicts of Interest
References
- Menconi, F.; Marcocci, C.; Marino, M. Diagnosis and classification of Graves’ disease. Autoimmun. Rev. 2014, 13, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.S.; Stroehla, B.C. The epidemiology of autoimmune diseases. Autoimmun. Rev. 2003, 2, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Li, H.; Chen, S.F.; Li, W.F.; Zhang, F.B. Polymorphisms in the vitamin D receptor gene and risk of autoimmune thyroid diseases: A meta-analysis. Endocrine 2013, 43, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Jyotsna, V.P.; Sahoo, A.; Ksh, S.A.; Sreenivas, V.; Gupta, N. Bone mineral density in patients of Graves’ disease pre- & post-treatment in a predominantly vitamin D deficient population. Indian J. Med. Res. 2012, 135, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-B.; Xue, X.-H.; Liu, S.-W.; Xi, G.-X.; Zhao, L.-X.; Zhang, X.-L. Clinical research of serum vitamin D in early Graves’ disease. Chin. Rem. Clin. 2014, 14, 242–243. [Google Scholar]
- Liu, X.-H. Correlation between Serum Level of 25-(OH)D3 and Humoral Immunity in Patients with Autoimmune Thyroid Diseases. Master’s Thesis, Zhengzhou University, Zhengzhou, China, 2012. [Google Scholar]
- Miao, W.; Ma, J.; Guo, R.; Wang, Y.-J.; Wang, G.; Guan, H.-X. Research about the correlation between Serum 25(OH)D with Graves’ disease. Chin. J. Pract. Internal Med. 2013, 33, 394–395. [Google Scholar]
- Wang, Y.-C. Analysis of the Relationship between 25(OH)D, IGF-1 and Bone Metabolism in Patients with Graves’ Disease. Master’s Thesis, Anhui Medical University, Hefei, China, 2014. [Google Scholar]
- Wang, Z.-S.; Song, Q.-H.; Wu, Y.-P.; Chen, H.; Tan, L.-L.; Sun, S.-H. Changes of biochemical markers of bone turnover in patients with Graves’ disease. Tianjin Med. J. 2014, 42, 683–686. [Google Scholar]
- Xuan, L.-Y. The Study on the Relation between Vitamin D and sFas in Patients with Autoimmune Thyroid Diseases. Master’s Thesis, Nanchang University, Nanchang, China, 2014. [Google Scholar]
- Yasuda, T.; Okamoto, Y.; Hamada, N.; Miyashita, K.; Takahara, M.; Sakamoto, F.; Miyatsuka, T.; Kitamura, T.; Katakami, N.; Kawamori, D.; et al. Serum vitamin D levels are decreased and associated with thyroid volume in female patients with newly onset Graves’ disease. Endocrine 2012, 42, 739–741. [Google Scholar]
- Yasuda, T.; Okamoto, Y.; Hamada, N.; Miyashita, K.; Takahara, M.; Sakamoto, F.; Miyatsuka, T.; Kitamura, T.; Katakami, N.; Kawamori, D.; et al. Serum vitamin D levels are decreased in patients without remission of Graves’ disease. Endocrine 2013, 43, 230–232. [Google Scholar]
- Zhang, H.; Liang, L.; Xie, Z. Low vitamin D status is associated with increased thyrotropin-receptor antibody titer in Graves’ disease. Endocr. Pract. 2015, 21, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-H.; Wang, Y.; Cao, W.; Wang, P.; Zhang, H.-M. Higher prevalence of vitamin D deficiency in female patients with Graves’ disease. Acta Nutr. Sin. 2013, 25, 299–301. [Google Scholar]
- Kivity, S.; Agmon-Levin, N.; Zisappl, M.; Shapira, Y.; Nagy, E.V.; Danko, K.; Szekanecz, Z.; Langevitz, P.; Shoenfeld, Y. Vitamin D and autoimmune thyroid diseases. Cell. Mol. Immunol. 2011, 8, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Cheng, Y.-K.; Chen, Y.-J.; Li, Y.-M.; Jiang, Y.-Q.; Zhang, S.-F. Abnormality of serum 25(OH)D level and its associations with thyroid hormones and auto-antibody in patients with Graves’ disease. Chin. J. Clin. Res. 2013, 26, 642–646. [Google Scholar]
- Zheng, Y.; Zheng, F.-P.; Li, H. The relationship of blood uric acid level and lumbar vertebra density in Graves’ disease. Chin. J. Gerontol. 2014, 34, 3017–3019. [Google Scholar]
- Wang, J.; Lv, S.; Chen, G.; Gao, C.; He, J.; Zhong, H.; Xu, Y. Meta-analysis of the association between vitamin d and autoimmune thyroid disease. Nutrients 2015, 7, 2485–2498. [Google Scholar] [CrossRef] [PubMed]
- Abd el Gawad, S.S.; Abdul Samee, E.R.; Metwali, A.A.; Abd el Gawad, M.S. Vitamin D receptor gene polymorphism and its association with 1,25-dihydroxyvitamin D(3) in patients with Graves’ disease in an Egyptian population: A pilot study. Endocr. Pract. 2012, 18, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Annerbo, M.; Hultin, H.; Stalberg, P.; Hellman, P. Left-shifted relation between calcium and parathyroid hormone in Graves’ disease. J. Clin. Endocrinol. Metab. 2014, 99, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Czernobilsky, H.; Scharla, S.; Schmidt-Gayk, H.; Ziegler, R. Enhanced suppression of 1,25(OH)2D3 and intact parathyroid hormone in Graves’ disease as compared to toxic nodular goiter. Calcif. Tissue Int. 1988, 42, 5–12. [Google Scholar] [CrossRef] [PubMed]
- D’Aurizio, F.; Villalta, D.; Metus, P.; Doretto, P.; Tozzoli, R. Is vitamin D a player or not in the pathophysiology of autoimmune thyroid diseases? Autoimmun. Rev. 2015, 14, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Dhanwal, D.K.; Kochupillai, N.; Gupta, N.; Cooper, C.; Dennison, E.M. Hypovitaminosis D and bone mineral metabolism and bone density in hyperthyroidism. J. Clin. Densitom. 2010, 13, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Effraimidis, G.; Badenhoop, K.; Tijssen, J.G.; Wiersinga, W.M. Vitamin D deficiency is not associated with early stages of thyroid autoimmunity. Eur. J. Endocrinol. 2012, 167, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-H. Clinical Study on the Injury of 1-a Hydroxylas in Renal Tubule of Hyporalemic Patients with Hyperthyroidism of Graves’ Disease. Doctoral Thesis, Tianjin Medical University, Tianjin, China, 2003. [Google Scholar]
- Li, X.; Wang, G.; Lu, Z.; Chen, M.; Tan, J.; Fang, X. Serum 25-hydroxyvitamin D predict prognosis in radioiodine therapy of Graves’ disease. J. Endocrinol. Invest. 2015. [Google Scholar] [CrossRef]
- Liu, M. The Study on the Relationship between 25-Hydroxy Vitamin D3 Levels and Common Thyroid Diseases. Master’s Thesis, Hebei Medical University, Shijiazhuang, China, 2014. [Google Scholar]
- Liu, Y.; Liu, Y.-Y.; Zhang, R.-D.; Gao, P.-X. The change in metabolic status of serum 25-hydroxy-vitamin D3 in patients with hyperthyroidism. Jiangsu Med. J. 2013, 39, 2565–2567. [Google Scholar]
- Shi, J.-H.; Wu, Z.-C.; Gu, Y.; Shen, X.-K.; Shi, Y.; Cai, M.-X.; Teng, X.-H.; Yu, Y.-C.; Wei, X.-F. The dynamic change of serum after in Graves’ patients serum l α, 25(OH)2D, calcitonin, calcium, phosphorus after intravenous EDTA in Graves’ patients. Endocr. Metab. J. 1993, 2, 50–51. [Google Scholar]
- Wu, Z.-.C.; Heng, S.-.J.; Gu, Y.; Shen, X.-.K.; Teng, X.-.H.; Yu, Y.-C. Graves’ disease after a static calcium gluconate injection, EDTA plasma PTH, calcitonin, 1,25(OH)D, calcium, phosphorus dynamic observation. J. Shanghai Rail. Med. Coll. 1995, 9, 146–150. [Google Scholar]
- Liang, L.-Y. Vitamin D Status is Associated with the Titres of Thyroid Autoantibodies in Graves’ Disease. Master’s Thesis, Central South University, Changsha, China, 2013. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotondi, M.; Chiovato, L. Vitamin D deficiency in patients with Graves’ disease: Probably something more than a casual association. Endocrine 2013, 43, 3–5. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, M.-Y.; Cao, B.; Yin, J.; Wang, D.-F.; Chen, K.-L.; Lu, Q.-B. Vitamin D and Graves’ Disease: A Meta-Analysis Update. Nutrients 2015, 7, 3813-3827. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053813
Xu M-Y, Cao B, Yin J, Wang D-F, Chen K-L, Lu Q-B. Vitamin D and Graves’ Disease: A Meta-Analysis Update. Nutrients. 2015; 7(5):3813-3827. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053813
Chicago/Turabian StyleXu, Mei-Yan, Bing Cao, Jian Yin, Dong-Fang Wang, Kai-Li Chen, and Qing-Bin Lu. 2015. "Vitamin D and Graves’ Disease: A Meta-Analysis Update" Nutrients 7, no. 5: 3813-3827. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053813