Preliminary Finnish Measures of Eating Competence Suggest Association with Health-Promoting Eating Patterns and Related Psychobehavioral Factors in 10–17 Year Old Adolescents

Abstract
:1. Introduction
2. Methods
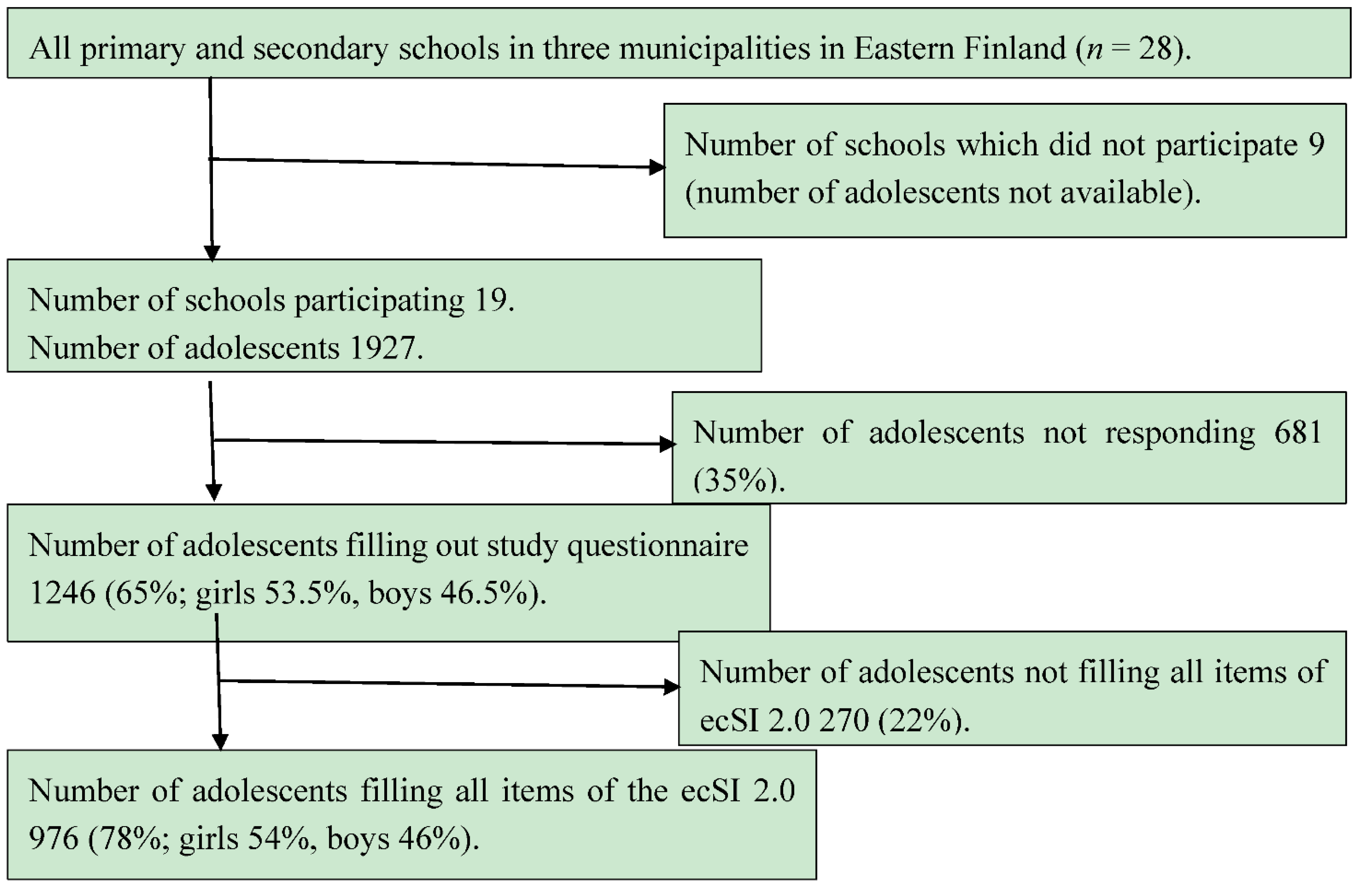
2.1. Data Collection

2.2. Study Questionnaire
2.3. Statistical Analyses
3. Results
3.1. Construct Validity of ecSI 2.0

3.2. Eating Competence and Related Psychobehavioral Factors

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Never/Rarely | Some-Times | Often/Fairly Often | |
|---|---|---|---|
| ←%→ | |||
| Eating Attitudes | |||
| I am relaxed about eating. | 8 | 26 | 66 |
| I am comfortable about eating enough. | 4 | 15 | 81 |
| I enjoy food and eating. | 10 | 22 | 68 |
| I am comfortable with my enjoyment of food and eating. | 7 | 20 | 73 |
| I feel it is okay to eat food that I like. | 5 | 18 | 77 |
| Food Acceptance | |||
| I experiment with new food and learn to like it. | 16 | 29 | 55 |
| If the situation demands, I “can make do” by eating food I don`t much care for. | 16 | 33 | 51 |
| I eat a wide variety of food. | 15 | 23 | 62 |
| Internal Regulation | |||
| I trust myself to eat enough for me. | 6 | 24 | 70 |
| I eat as much as I am hungry for. | 10 | 20 | 70 |
| I eat until I feel satisfied. | 12 | 24 | 64 |
| Contextual Skills | |||
| I tune in to food and pay attention to eating. | 12 | 24 | 64 |
| I make time to eat. | 15 | 28 | 57 |
| I have regular meals. | 19 | 28 | 53 |
| I consider what is good for me when I eat. | 13 | 28 | 59 |
| I plan for feeding myself. | 38 | 29 | 33 |
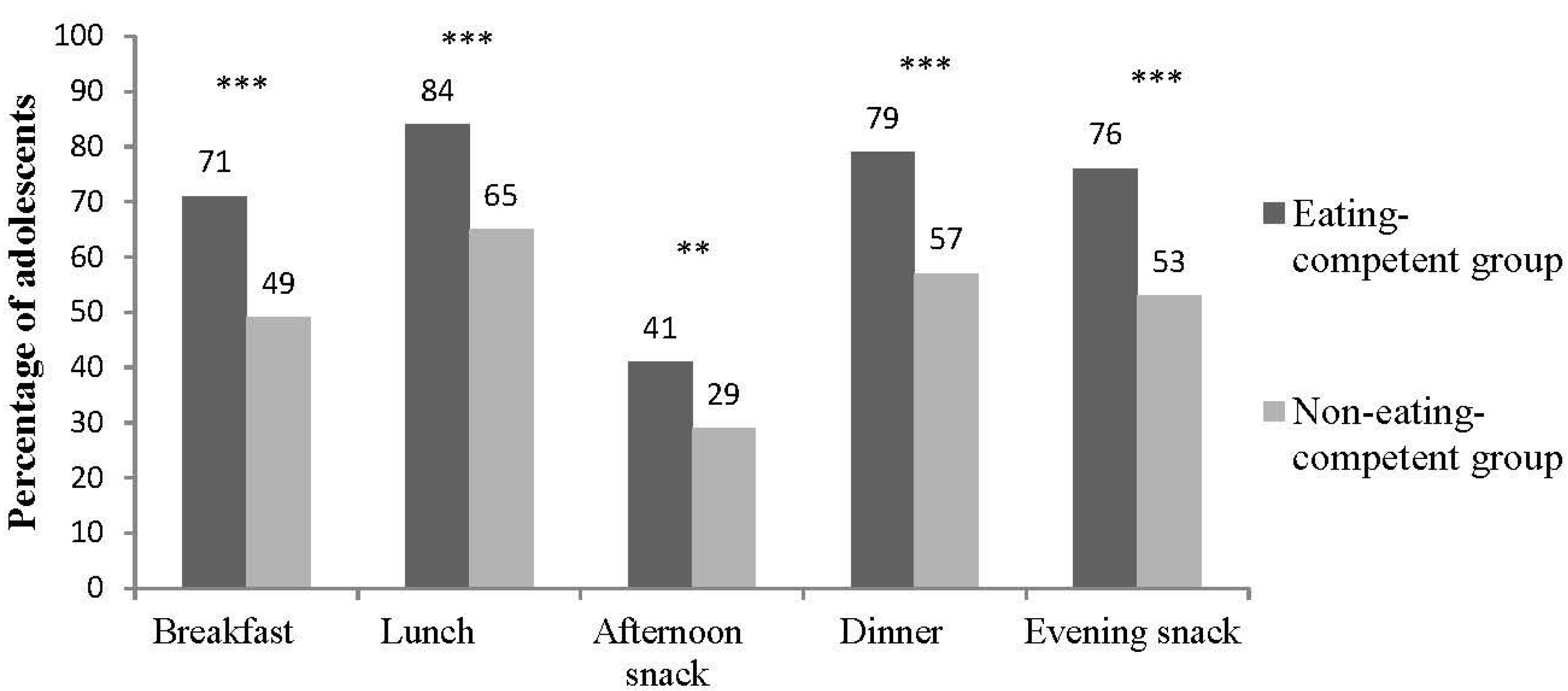
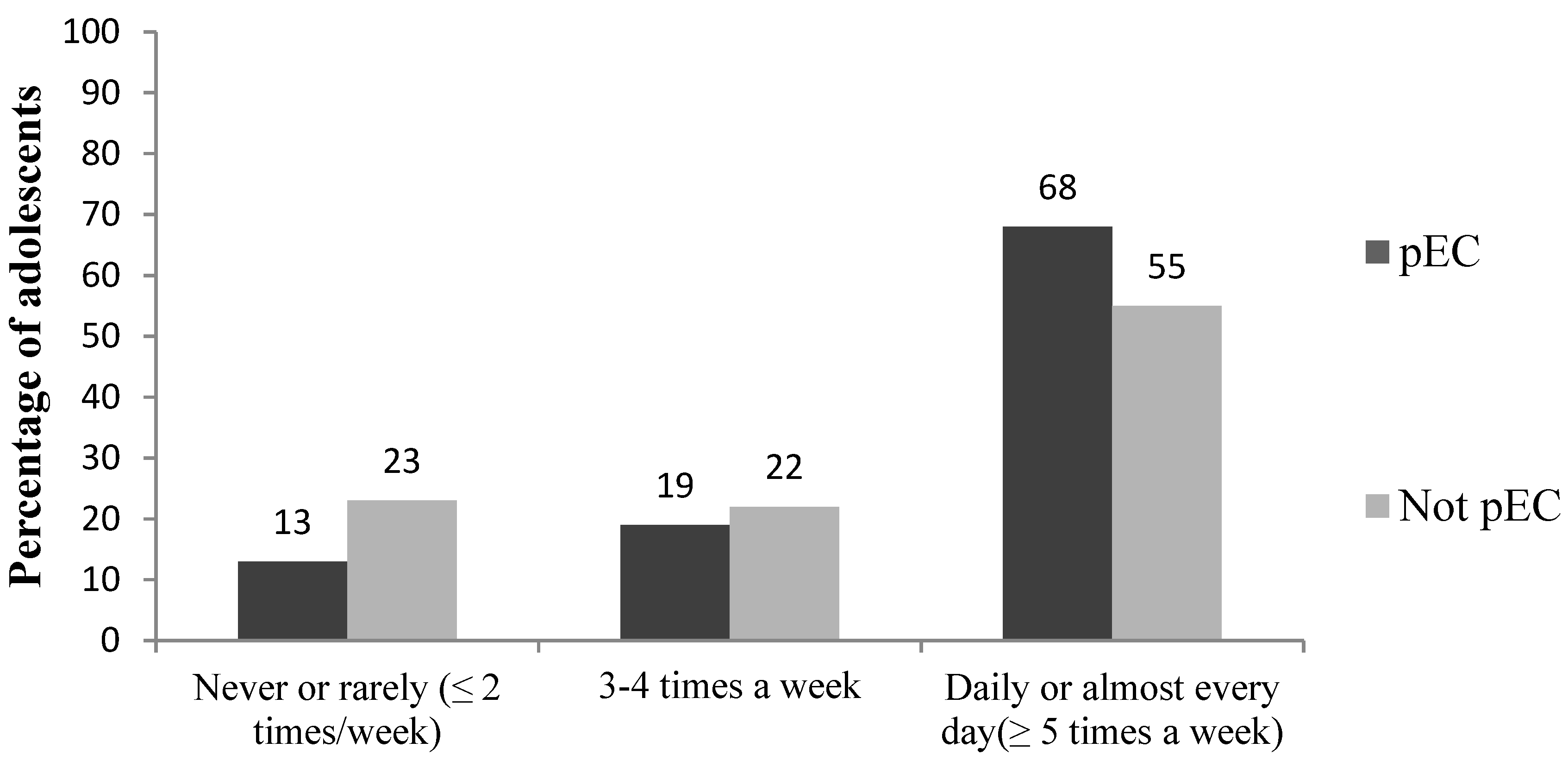
3.3. Associations between Eating Competence and Eating Patterns
| Characteristic | pEC | p-Value 1 |
|---|---|---|
| % (CI), Number of Subjects | ||
| Girls | 62 (58–66), n = 324 | |
| Boys | 53 (48–58), n = 230 | |
| 0.006 | ||
| Primary school students | 63 (57–68), n = 202 | |
| Secondary school students | 57 (53–62), n = 319 | |
| 0.14 | ||
| Overweight 2 | 60 (51–69), n = 67 | |
| Normal weight 2 | 63 (58–67), n = 327 | |
| Underweight 2 | 52 (40–65), n = 33 | |
| 0.45 | ||
| Perception of body image | ||
| appropriate size | 63 (59–69), n = 350 | |
| somewhat fat or too fat | 47 (41–53), n = 126 | |
| somewhat thin or too thin | 59 (50–68), n = 73 | |
| < 0.001 | ||
| Tried to lose weight during last year | 47 (41–52), n = 140 | |
| < 0.001 | ||
| High self-esteem 3 | 77 (72–82), n = 234 | |
| Moderate self-esteem 3 | 51 (45–56), n = 158 | |
| Low self-esteem 3 | 44 (38–50), n = 115 | |
| < 0.001 | ||
| Strong SOC (scores 62–91) 4 | 76 (69–81), n = 146 | |
| Moderate SOC (scores 53–60) 4 42 (35–49), n = 83 | ||
| Weak SOC (scores 17–52) 4 | 45 (39–52), n = 94 | |
| < 0.001 | ||

| pEC | not pEC | p-Value 1 | |
|---|---|---|---|
| Statement | ←%→ | ||
| Family eating patterns | |||
| In our family we have regular meal frequency. | 82 | 60 | < 0.001 |
| We have vegetables included in every family meal. | 83 | 54 | < 0.001 |
| In our family fruits are offered daily. | 91 | 68 | < 0.001 |
| My parents pay attention to the quality of the diet. | 93 | 73 | < 0.001 |
| We don’t usually have salty snacks available at home. | 67 | 62 | 0.64 |
| We don’t usually have sweet snacks available at home. | 68 | 60 | 0.08 |
| We don’t usually have soft drinks available at home. | 67 | 71 | 0.005 |
| Children’s possibility to influence food and eating | |||
| I can influence the type of food eaten at home. | 93 | 77 | < 0.001 |
| I can influence when I eat at home. | 74 | 69 | 0.11 |
| I can influence what I eat at home. | 82 | 61 | < 0.001 |
| I can influence how much I eat at home. | 94 | 82 | < 0.001 |
| I take part in food preparation at home. | 73 | 46 | < 0.001 |

3.4. Factors Associated with Eating Competence
4. Discussion
4.1. Usefulness of Eating Competence Concept
| Variable | PR | 95% CI | P-Value |
|---|---|---|---|
| Possibility to influence how much to eat at meals 3 | 1.237 | 1.070–1.428 | 0.004 |
| Meal frequency 4 | 1.017 | 1.004–1.030 | 0.009 |
| Availability of vegetables at family meals 3 | 1.165 | 1.037–1.310 | 0.010 |
| Self-esteem 5 | 1.010 | 1.000–1.021 | 0.059 |
4.2. Eating Competence and Family Eating Patterns
4.3. Eating Competence, Weight and Body Satisfaction
4.4. Eating Competence, Self-Esteem and SOC
4.5. Eating Competence and Gender
4.6. Strengths and Limitations
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Satter, E.M. Eating competence: Definition and evidence for the Satter eating competence model. J. Nutr. Educ. Behav. 2007, 39, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Satter, E. Satter eating competence: Nutrition education with the Satter eating competence model. J. Nutr. Educ. Behav. 2007, 13, 189–194. [Google Scholar] [CrossRef]
- Lohse, B.A.; Satter, E.; Horacek, T.; Gebreselassie, T.; Oakland, M.J. Measuring eating competence: Psychometric properties and validity of the ecSatter inventory. J. Nutr. Educ. Behav. 2012, 39, 154–166. [Google Scholar] [CrossRef]
- Krall, J.; Lohse, B.A. Validation of a measure of the Satter eating competence model with low-income females. Int. J. Behav. Nutr. Phys. Act 2011, 7, 26. [Google Scholar] [CrossRef]
- Lohse, B. The Satter Eating Competence Inventory for low-income persons is a valid measure of eating competence for persons of higher socioeconomic position. Appetite 2015, 87, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Lohse, B.A.; Arnold, K.N. Measuring eating competence: Congruence between two Satter inventories supports supplanting the original version with the low-income adaptation. J. Acad. Nutr. Diet. 2012, 112, A63. [Google Scholar] [CrossRef]
- Krall, J.S.; Lohse, B. Cognitive testing with female nutrition and education assistance program participants informs validity of the Satter eating competence inventory. J. Nutr. Educ. Behav. 2010, 42, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Lohse, B.; Bailey, R.; Krall, J.; Wall, D.E.; Mitchell, D.C. Diet quality is related to eating competence in cross-sectional sample of low-income females in Pennsylvania. Appetite 2012, 58, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Lohse, B.; Psota, T.; Estruch, R.; Zazpe, I.; Sorli, J.V.; Salas-Salvadó, J.; Serra, M.; Krall, J.S.; Márquez, F.; Ros, E.; et al. Eating competence of elderly Spanish adults is associated with a healthy diet and a favorable cardiovascular disease risk profile. J. Nutr. 2010, 140, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Psota, T.; Lohse, B.; West, S. Associations between eating competence and cardiovascular disease biomarkers. J. Nutr. Educ. Behav. 2007, 39, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Lohse, B.; Cunningham-Sabo, L. Eating competence of Hispanic parents is associated with attitudes and behaviors that may mediate fruit and vegetable-related behaviors of 4th Grade Youth. J. Nutr. 2012, 142, 1903–1909. [Google Scholar] [CrossRef] [PubMed]
- Hoppu, U.; Lehtisalo, J.; Tapanainen, H.; Pietinen, P. Dietary habits and nutrient intake of Finnish adolescents. Public Health Nutr. 2010, 13, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Lawlor, D.; Kimm, S. Childhood obesity. Lancet 2010, 375, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Speiser, P.W.; Rudolf, M.C.J.; Anhalt, H.; Camacho-Hubner, C.; Chiarelli, F.; Eliakim, A.; Freemark, M.; Gruters, A.; Hershkovitz, E.; Iughetti, L.; et al. Consensus statement: Childhood obesity. J. Clin. Endocrinol. Metab. 2005, 90, 1871–1887. [Google Scholar] [CrossRef] [PubMed]
- Ojala, K. Adolescents’ Self-Perceived Weight and Weight Reduction Behaviour—Health Behaviour in School-Aged Children (HBSC) Study, a WHO Cross-National Survey. Ph.D. Thesis, University of Jyväskylä, Jyväskylä, Finland, April 2011. [Google Scholar]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, C.; de Looze, M.; Roberts, C.; Samdal, O.; Smith, O.; Barnekow, V. Social determinants of health and well-being among young people. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey. World Health Organization. Available online: http://www.euro.who.int/__data/assets/pdf_file/0003/163857/Social-determinants-of-health-and-well-being-among-young-people.pdf (accessed on 17 November 2014).
- Birch, L.; Ventura, A. Preventing childhood obesity: What works? Int. J. Obes. 2009, 33, 74–81. [Google Scholar] [CrossRef]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Krall, T.; Rauh, E. Eating behaviors of children in the context of their family environment. Physiol. Behav. 2010, 100, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Ray, C.; Kalland, M.; Lehto, R.; Roos, E. Does parental warmth and responsiveness moderate the associations between parenting practices and children’s health-related behaviors? J. Nutr. Educ. Behav. 2013, 45, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Pallant, J.F.; Lae, L. Sense of coherence, well-being, coping and personality factors: Further evaluation of the sense of coherence scale. Personal. Individ. Differ. 2002, 33, 39–48. [Google Scholar] [CrossRef]
- Antonovsky, A. Health, Stress and Coping; Jossay Bass Publishers: San Francisco, CA, USA, 1979. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossay Bass Publishers: San Francisco, CA, USA, 1987. [Google Scholar]
- Mattila, M.L.; Rautava, P.; Honkinen, P.L.; Ojanlatva, A.; Jaakkola, S.; Aromaa, M.; Suominen, S.; Helenius, H.; Sillanpää, M. Sense of coherence and health behavior in adolescence. Acta Paediatri. 2010, 100, 1590–1595. [Google Scholar] [CrossRef]
- Lindmark, U.; Stegmayr, B.; Nilsson, B.; Lindahl, B.; Johansson, I. Food selection associated with sense of coherence in adults. Nutr. J. 2005, 28, 4. [Google Scholar]
- Wainwright, N.W.J.; Surtees, P.G.; Welch, A.A.; Luben, R.N.; Khaw, K.T.; Bingham, S.A. Healthy lifestyle choices: Could sense of coherence aid health promotion? J. Epidemiol. Community Health 2007, 61, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, N.W.J.; Surtees, P.G.; Welch, A.A.; Luben, R.N.; Khaw, K.T.; Bingham, S.A. Sense of coherence, lifestyle choices and mortality? J. Epidemiol. Community Health 2008, 62, 829–831. [Google Scholar] [CrossRef] [PubMed]
- Myrin, B.; Lagerström, M. Health behaviour and sense of coherence among pupils aged 14–15. Scand. J. Caring Sci. 2006, 20, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Tilles-Tirkkonen, T.; Suominen, S.; Liukkonen, J.; Poutanen, K.; Karhunen, L. Determinants of a regular intake of a nutritionally balanced school lunch among 10- to 17-year-old schoolchildren with special reference to sense of coherence. J. Hum. Nutr. Diet. 2014, 19. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 6, 1240–1243. [Google Scholar] [CrossRef]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ 2007, 28, 194. [Google Scholar] [CrossRef]
- World Health Organization. Health Behavior of School Aged Children Study (HBSC). Available online: http://www.euro.who.int/en/home (accessed on 17 November 2014).
- Finnish National Institute for Health and Welfare. The School Health Promotion Study (SHP). Available online: http://www.thl.fi/attachments/kouluterveyskysely/Lomakkeet/KTK2011_PK_FIN.pdf (accessed on 17 November 2014).
- The Finnish National Nutrition Recommendations. Available online: http://www.ravitsemusneuvottelukunta.fi/portal/en/ (accessed on 29 January 2015).
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image, Prevised ed.; Wesleyan University Press: Middletown, CT, USA, 1989. [Google Scholar]
- Honkinen, P.L.; Suominen, S.; Rautava, P.; Hakanen, J.; Kalimo, R. The adult sense of coherence scale is applicable to 12-year-old schoolchildren—An additional tool in health promotion. Acta Paediatr. 2006, 95, 952–955. [Google Scholar] [CrossRef] [PubMed]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Model; Bollen, K.A., Long, J.S., Eds.; Sage: Beverly Hills, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Brown, L.B.; Larsen, K.J.; Nyland, N.K.; Eggett, D.L. Eating competence of college students in an introductory nutrition course. J. Nutr. Educ. Behav. 2013, 45, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Birch, L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Neumark-Sztainer, D.; French, S. Individual and environmental influences on adolescent eating behavior. J. Am. Diet. Assoc. 2002, 102, 40–51. [Google Scholar] [CrossRef]
- Cullen, K.W.; Baranowski, T.; Rittenberry, L.; Cosart, C.; Hebert, D.; de Moor, C. Child-reported family and peer influences on fruit, juice and vegetable consumption: Reliability and validity of measures. Health Educ. Res. 2001, 16, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Satter, E. The Satter Feeding Dynamics Model. Available online: http://www.ellynsatterinstitute.org/other/fdsatter.php (accessed on 15 January 2015).
- Alsharairi, N.A.; Somerset, S.M. Associations between Parenting Styles and Children’s Fruit and Vegetable Intake. Ecol. Food Nutr. 2015, 54, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Carnell, S.; Wardle, J. Appetitive traits and child obesity: measurement, origins and implications for intervention. Proc. Nutr. Soc. 2008, 67, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Faith, M.S.; Scanlon, K.S.; Birch, L.L.; Francis, L.A.; Sherry, B. Parent-child feeding strategies and their relationships to child eating and weight status. Obes. Res. 2004, 12, 1711–1722. [Google Scholar] [CrossRef] [PubMed]
- Megalakaki, O.; Mouveaux, M.; Hubin-Gayte, M.; Wypych, L. Body image and cognitive restraint are risk factors for obesity in French adolescents. Eat. Weight Disord. 2013, 18, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Sonneville, K.R.; Calzo, J.P.; Horton, N.J.; Haines, J.; Austin, S.B.; Field, A.E. Body satisfaction, weight gain and binge eating among overweight adolescent girls. Int. J. Obes. 2012, 36, 944–949. [Google Scholar] [CrossRef]
- Parkinson, K.N.; Drewett, R.F.; Le Couteur, A.S.; Adamson, A.J.; Gateshead Millennium Study core team. Earlier predictors of eating disorder symptoms in 9-year-old children. A longitudinal study. Appetite 2012, 59, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Hammons, A.J.; Fiese, B.H. Is frequency of shared family meals related to the nutritional health of children and adolescents? Pediatrics 2011, 127, 1565–1574. [Google Scholar] [CrossRef]
- Jääskeläinen, A.; Schwab, U.; Kolehmainen, M.; Kaakinen, M.; Savolainen, M.J.; Froguel, P.; Cauchi, S.; Järvelin, M.R.; Laitinen, J. Meal frequencies modify the effect of common genetic variants on body mass index in adolescents of the northern Finland birth cohort 1986. PLoS ONE 2013, 10, 8. [Google Scholar]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Dennison, M.; Whittle, S.; Yücel, M.; Vijayakumar, N.; Kline, A.; Simmons, J.; Allen, N.B. Mapping subcortical brain maturation during adolescence: evidence of hemisphere- and sex-specific longitudinal changes. Dev. Sci. 2013, 16, 772–791. [Google Scholar] [CrossRef] [PubMed]
- Tilles-Tirkkonen, T.; University of Eastern Finland, Kuopio, Finland. Unpublished work. 2015.
- Brettschneider, A.K.; Rosario, A.S.; Ellert, U. Validity and predictors of BMI derived from self-reported height and weight among 11- to 17-year-old German adolescents from the KiGGS study. BMC Res. Notes 2011, 4, 414. [Google Scholar] [CrossRef] [PubMed]
- Elgar, F.J.; Roberts, C.; Tudor-Smith, C.; Moore, L. Validity of self-reported height and weight and predictors of bias in adolescents. J. Adolesc. Health 2005, 37, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Quick, V.; Byrd-Bredbenner, C.; Shoff, S.; White, A.A.; Lohse, B.; Horacek, T.; Kattelmann, K.; Phillips, B.; Hoerr, S.L.; Greene, G. Concordance of self-report and measured height and weight of college students. J. Nutr. Educ. Behav. 2015, 47, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Sherry, B.; Jefferds, M.E.; Grummer-Strawn, L.M. Accuracy of adolescent self-report of height and weight in assessing overweight status: a literature review. Arch. Pediatr. Adolesc. Med. 2007, 161, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanja, T.-T.; Outi, N.; Sakari, S.; Jarmo, L.; Kaisa, P.; Leila, K. Preliminary Finnish Measures of Eating Competence Suggest Association with Health-Promoting Eating Patterns and Related Psychobehavioral Factors in 10–17 Year Old Adolescents. Nutrients 2015, 7, 3828-3846. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053828
Tanja T-T, Outi N, Sakari S, Jarmo L, Kaisa P, Leila K. Preliminary Finnish Measures of Eating Competence Suggest Association with Health-Promoting Eating Patterns and Related Psychobehavioral Factors in 10–17 Year Old Adolescents. Nutrients. 2015; 7(5):3828-3846. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053828
Chicago/Turabian StyleTanja, Tilles-Tirkkonen, Nuutinen Outi, Suominen Sakari, Liukkonen Jarmo, Poutanen Kaisa, and Karhunen Leila. 2015. "Preliminary Finnish Measures of Eating Competence Suggest Association with Health-Promoting Eating Patterns and Related Psychobehavioral Factors in 10–17 Year Old Adolescents" Nutrients 7, no. 5: 3828-3846. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053828