The Impact of Impulsivity on Weight Loss Four Years after Bariatric Surgery

Abstract
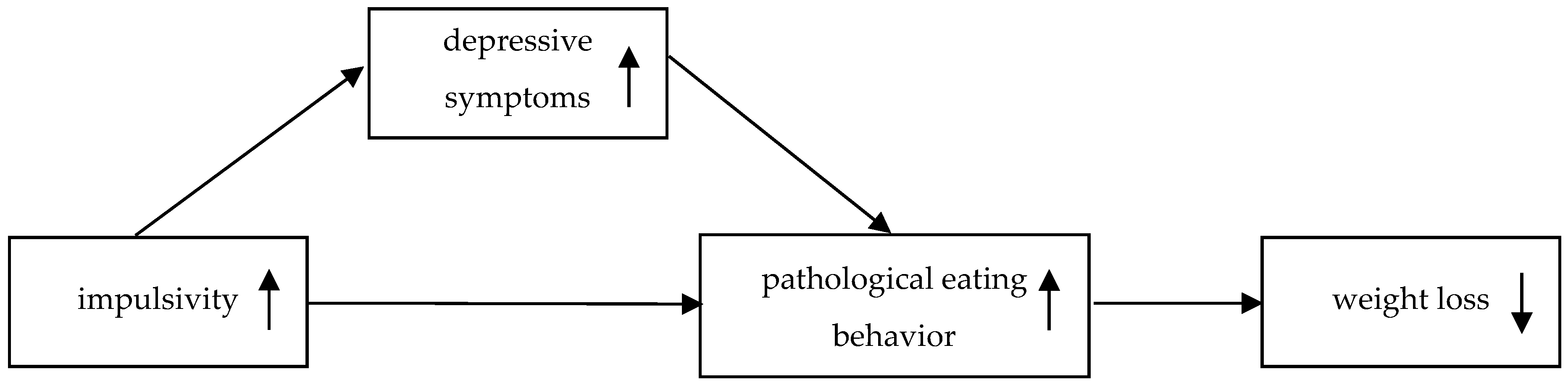
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measurements
2.2.1. Body Mass Index (BMI), Body Weight Loss (%BWL), and Excess Weight Loss (%EWL)
2.2.2. Impulsivity
2.2.3. Pathological Eating Behavior
2.2.4. Depression
2.3. Statistical Analyses
3. Results
3.1. Sample Characterisitics
3.2. Correlational Analyses
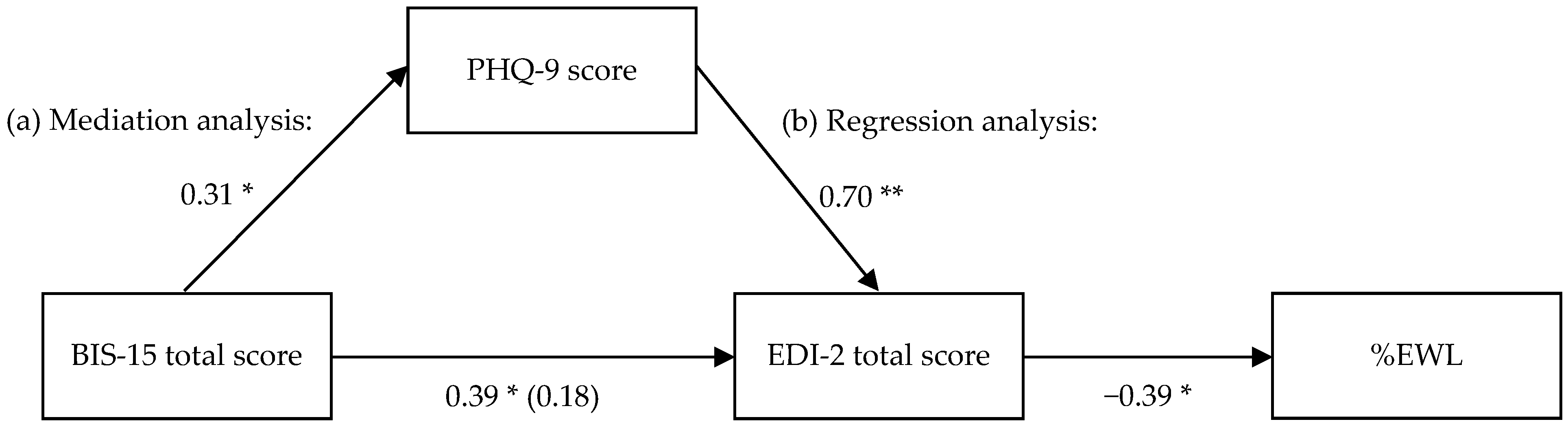
3.3. Regression and Mediation Analyses
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel. Expert Panel Report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity (Silver Spring) 2014, 22, S41–S410. [Google Scholar]
- Miras, A.D.; Le Roux, C.W. Mechanisms underlying weight loss after bariatric surgery. Nat. Rev. Gastroenterol. Hapatol. 2013, 10, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Fruhbeck, G.; Ryan, D.H.; Wilding, J.P. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Wadden, T.A.; Fabricatore, A.N. Psychosocial and Behavioral Aspects of Bariatric Surgery. Obes. Res. 2005, 13, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Eldar, S.; Heneghan, H.M.; Brethauer, S.A.; Schauer, P.R. Bariatric surgery for treatment of obesity. Int. J. Obes. 2011, 35, S16–S21. [Google Scholar] [CrossRef] [PubMed]
- Belanger, S.B.; Wechsler, F.S.; Nademin, M.E.; Virden, T.B. Predicting Outcome of Gastric Bypass Surgery Utilizing Personality Scale Elevations, Psychosocial Factors, and Diagnostic Group Membership. Obes. Surg. 2010, 20, 1361–1371. [Google Scholar] [CrossRef] [PubMed]
- Livhits, M.; Mercado, C.; Yermilov, I.; Parikh, J.A.; Dutson, E.; Mehran, A.; Ko, C.Y.; Gibbons, M.M. Preoperative Predictors of Weight Loss Following Bariatric Surgery: Systematic Review. Obes. Surg. 2012, 22, 70–89. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Mitchell, J.E.; Engel, S.; Crosby, R.; Wonderlich, S. Psychopathology in bariatric surgery candidates: A review of studies using structured diagnostic interviews. Compr. Psychiatr. 2014, 55, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Aguera, Z.; Garcia-Ruiz-de-Gordejuela, A.; Vilarrasa, N.; Sanchez, I.; Bano, M.; Camacho, L.; Granero, R.; Jimenez-Murcia, S.; Virgili, N.; Lopez-Urdiales, R.; et al. Psychological and Personality Predictors of Weight Loss and Comorbid Metabolic Changes After Bariatric Surgery. Eur. Eat. Disord. Rev. 2015, 23, 509–516. [Google Scholar] [CrossRef] [PubMed]
- De Panfilis, C.; Generali, I.; Dall'Aglio, E.; Marchesi, F.; Ossola, P.; Marchesi, C. Temperament and one-year outcome of gastric bypass for severe obesity. Surg. Obes. Relat. Dis. 2014, 10, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Leombruni, P.; Piero, A.; Dosio, D.; Novelli, A.; Abbate-Daga, G.; Morino, M.; Toppino, M.; Fassino, S. Psychological predictors of outcome in vertical banded gastroplasty: A 6 months prospective pilot study. Obes. Surg. 2007, 17, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, G.; Herpertz, S.; Loeber, S. Personality traits and obesity: A systematic review. Obes. Rev. 2015, 16, 32–63. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.G.; Robbins, T.W. The Neurobiological Underpinnings of Obesity and Binge Eating: A Rationale for Adopting the Food Addiction Model. Biol. Psychiatr. 2013, 73, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Gullo, M.J.; Loxton, N.J.; Dawe, S. Impulsivity: Four ways five factors are not basic to addiction. Addict. Behav. 2014, 39, 1547–1556. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.; Markon, K.E.; Clark, L.A. Toward a theory of distinct types of “impulsive” behaviors: A meta-analysis of self-report and behavioral measures. Psychol. Bull. 2014, 140, 374–408. [Google Scholar] [CrossRef] [PubMed]
- Schag, K.; Schönleber, J.; Teufel, M.; Zipfel, S.; Giel, K.E. Food-related impulsivity in obesity and Binge Eating Disorder—A systematic review. Obes. Rev. 2013, 14, 477–495. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, J.; Yao, J.; Ji, G.; Qian, L.; Wang, J.; Zhang, G.; Tian, J.; Nie, Y.; Zhang, Y.E.; et al. Obesity: Pathophysiology and intervention. Nutrients 2014, 6, 5153–5183. [Google Scholar] [CrossRef] [PubMed]
- Sarmugam, R.; Worsley, A. Dietary Behaviours, Impulsivity and Food Involvement: Identification of Three Consumer Segments. Nutrients 2015, 7, 8036–8057. [Google Scholar] [CrossRef] [PubMed]
- Houben, K.; Nederkoorn, C.; Jansen, A. Eating on impulse: The relation between overweight and food-specific inhibitory control. Obesity (Silver Spring) 2014, 22, E6–E8. [Google Scholar] [CrossRef] [PubMed]
- Opolski, M.; Chur-Hansen, A.; Wittert, G. The eating-related behaviours, disorders and expectations of candidates for bariatric surgery. Clin. Obes. 2015, 5, 165–197. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.K.; Eriksen, L.; Vedul-Kjelsas, E.; Strommen, M.; Kulseng, B.; Marvik, R.; Holen, A. Prevalence of all relevant eating disorders in patients waiting for bariatric surgery: A comparison between patients with and without eating disorders. Eat. Weight Disord. 2010, 15, e247–e255. [Google Scholar] [CrossRef] [PubMed]
- Agh, T.; Kovacs, G.; Pawaskar, M.; Supina, D.; Inotai, A.; Voko, Z. Epidemiology, health-related quality of life and economic burden of binge eating disorder: A systematic literature review. Eat. Weight Disord. 2015, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Leehr, E.J.; Krohmer, K.; Schag, K.; Dresler, T.; Zipfel, S.; Giel, K.E. Emotion regulation model in binge eating disorder and obesity—A systematic review. Neurosci. Biobehav. Rev. 2015, 49, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Pearson, C.M.; Zapolski, T.C.; Smith, G.T. A longitudinal test of impulsivity and depression pathways to early binge eating onset. Int. J. Eat. Disord. 2015, 48, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Sheets, C.S.; Peat, C.M.; Berg, K.C.; White, E.K.; Bocchieri-Ricciardi, L.; Chen, E.Y.; Mitchell, J.E. Post-operative Psychosocial Predictors of Outcome in Bariatric Surgery. Obes. Surg. 2015, 25, 330–345. [Google Scholar] [CrossRef] [PubMed]
- Konttinen, H.; Kiviruusu, O.; Huurre, T.; Haukkala, A.; Aro, H.; Marttunen, M. Longitudinal associations between depressive symptoms and body mass index in a 20-year follow-up. Int. J. Obes. 2014, 38, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Brandão, I.; Ramalho, S.; Pinto-Bastos, A.; Arrojado, F.; Faria, G.; Calhau, C.; Coelho, R.; Conceição, E. Metabolic profile and psychological variables after bariatric surgery: Association with weight outcomes. Eat. Weight Disord. 2015, 20, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Meany, G.; Conceicao, E.; Mitchell, J.E. Binge eating, binge eating disorder and loss of control eating: Effects on weight outcomes after bariatric surgery. Eur. Eat. Disord. Rev. 2014, 22, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Mack, I.; Ölschläger, S.; Sauer, H.; von Feilitzsch, M.; Weimer, K.; Junne, F.; Peeraully, R.; Enck, P.; Zipfel, S.; Teufel, M. Does Laparoscopic Sleeve Gastrectomy Improve Depression, Stress and Eating Behaviour? A 4-Year Follow-up Study. Obes. Surg. 2016, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Thonney, B.; Pataky, Z.; Badel, S.; Bobbioni-Harsch, E.; Golay, A. The relationship between weight loss and psychosocial functioning among bariatric surgery patients. Am. J. Surg. 2010, 199, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Konttinen, H.; Homberg, J.R.; Engels, R.C.; Winkens, L.H. Emotional eating as a mediator between depression and weight gain. Appetite 2016, 100, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Vögele, C.; Kübler, A. Psychometrische Evaluation der deutschen Barratt Impulsiveness Scale—Kurzversion (BIS-15). Diagnostica 2011, 57, 126–133. [Google Scholar] [CrossRef]
- Paul, T.; Thiel, A. Eating Disorder Inventory-2. German Version; Hogrefe: Göttingen, Germany, 2005. [Google Scholar]
- Löwe, B.; Spitzer, R.L.; Zipfel, S.; Herzog, W. Gesundheitsfragebogen für Patienten (PHQ-D). In Komplettversion und Kurzform, 2nd ed.; Pfizer: Karlsruhe, Germany, 2002. [Google Scholar]
- Krönke, K.; Spitzer, R.L. The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. 2002, 32, 1–7. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, 23.0 ed.; IBM Corp: Armonk, NY, USA, 2015. [Google Scholar]
- Dempster, A.P.; Laird, N.M.; Rubin, D.B. Maximum Likelihood from Incomplete Data via the EM Algorithm. J. R. Stat. Soc. Ser. B (Methodological) 1977, 39, 1–38. [Google Scholar]
- The PROCESS macro for SPSS and SAS. Available online: http://processmacro.org/index.html (accessed on 20 July 2016).
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, S.E.; Cole, D.A.; Mitchell, M.A. Bias in cross-sectional analyses of longitudinal mediation: Partial and complete mediation under an autoregressive model. Multivar. Behav. Res. 2011, 46, 816–841. [Google Scholar] [CrossRef] [PubMed]
- Wild, B.; Hunnemeyer, K.; Sauer, H.; Hain, B.; Mack, I.; Schellberg, D.; Muller-Stich, B.P.; Weiner, R.; Meile, T.; Rudofsky, G.; et al. A 1-year videoconferencing-based psychoeducational group intervention following bariatric surgery: Results of a randomized controlled study. Surg. Obes. Relat. Dis. 2015, 11, 1349–1360. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | Mean | SD | Range | |
|---|---|---|---|---|
| sex 1 | 65 | 39 ♀ 26 ♂ | - | - |
| age (years) | 65 | 49.0 | ±11.6 | 28.0–74.0 |
| BMI (kg/m2) | 64 | 36.9 | ±8.5 | 22.9–63.7 |
| %EWL 2 | 64 | 52.0 | ±27.3 | −20.7–113.3 |
| %BWL 2 | 64 | 24.3 | ±12.4 | −8.6–51.3 |
| BIS-15 total score | 59 | 30.4 | ±6.3 | 19–45 |
| EDI-2 total score | 54 | 239.1 | ±53.8 | 149–370 |
| PHQ-9 score | 61 | 6.7 | ±5.8 | 0–27 |
| %EWL 1 | BIS-15 Total Score 1 | PHQ-9 Score 2 | EDI-2 Total Score 1 | |
|---|---|---|---|---|
| %BWL 1 | 0.94 * | −0.16 | −0.19 | −0.41 * |
| %EWL 1 | - | −0.16 | −0.20 | −0.39 * |
| BIS-15 total score 1 | - | - | 0.36 * | 0.41 * |
| PHQ-9 score 2 | - | - | - | 0.72 * |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schag, K.; Mack, I.; Giel, K.E.; Ölschläger, S.; Skoda, E.-M.; Von Feilitzsch, M.; Zipfel, S.; Teufel, M. The Impact of Impulsivity on Weight Loss Four Years after Bariatric Surgery. Nutrients 2016, 8, 721. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8110721
Schag K, Mack I, Giel KE, Ölschläger S, Skoda E-M, Von Feilitzsch M, Zipfel S, Teufel M. The Impact of Impulsivity on Weight Loss Four Years after Bariatric Surgery. Nutrients. 2016; 8(11):721. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8110721
Chicago/Turabian StyleSchag, Kathrin, Isabelle Mack, Katrin E. Giel, Sabrina Ölschläger, Eva-Maria Skoda, Maximilian Von Feilitzsch, Stephan Zipfel, and Martin Teufel. 2016. "The Impact of Impulsivity on Weight Loss Four Years after Bariatric Surgery" Nutrients 8, no. 11: 721. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8110721