Nutrition in Pediatric Inflammatory Bowel Disease: From Etiology to Treatment. A Systematic Review

 ,
,
Abstract
:
1. Introduction
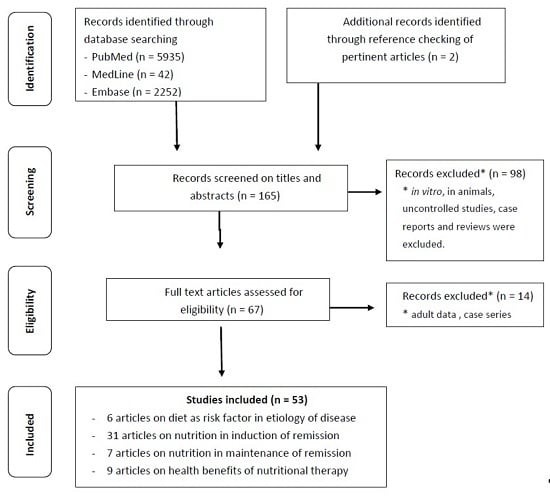
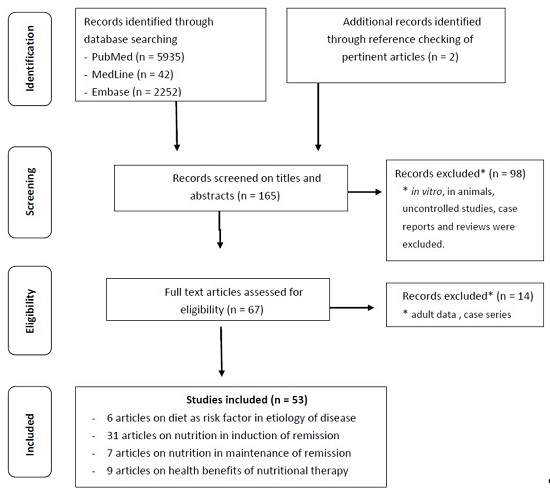
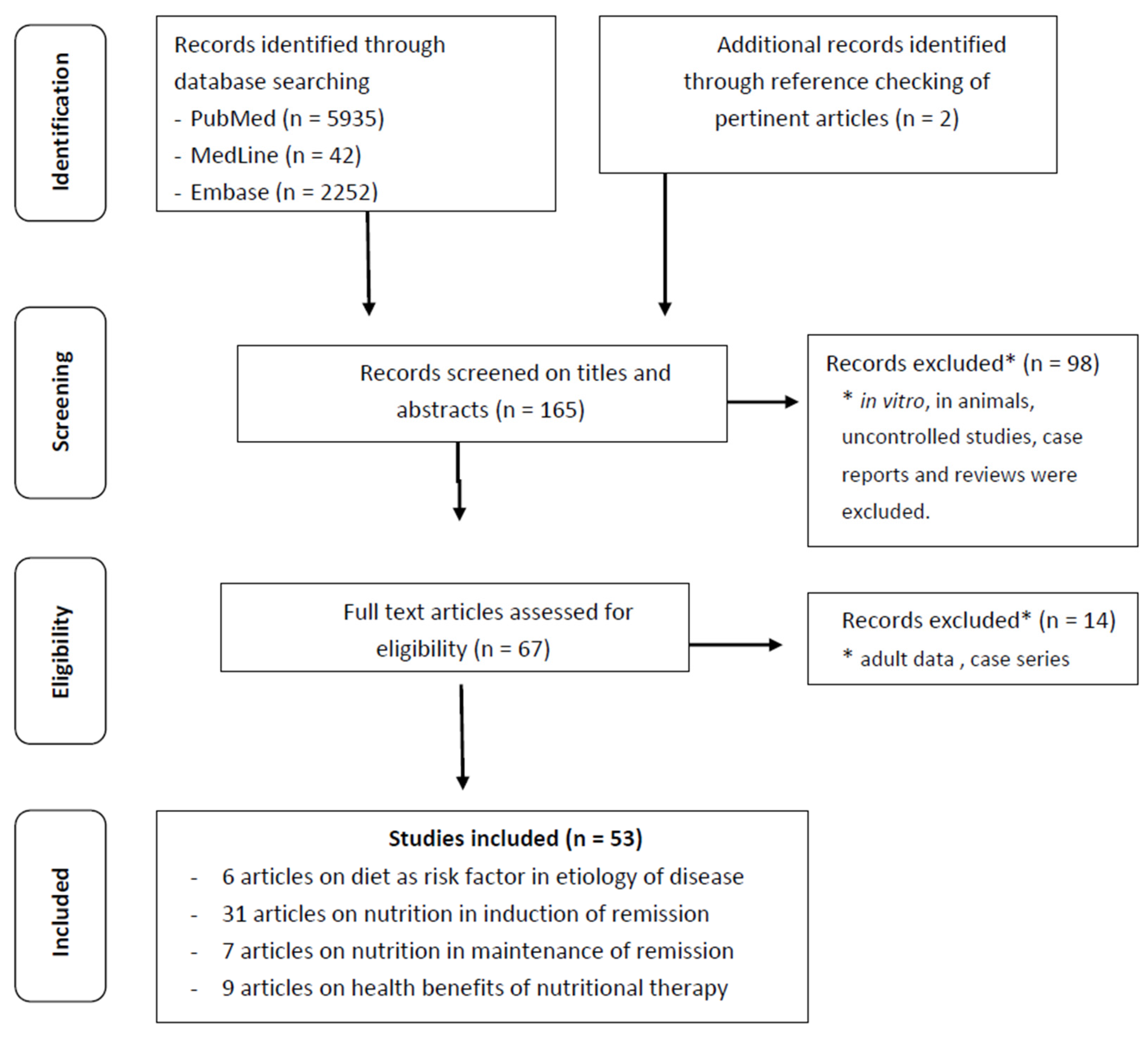
2. Methods
3. Nutrition in Etiology of Pediatric Inflammatory Bowel Disease
4. Nutrition in Induction of Remission in Pediatric Inflammatory Bowel Disease
5. Nutrition in Maintenance of Remission in Pediatric IBD
6. Health Benefits of Nutritional Therapy in Pediatric IBD
7. Strengths and Limitations
8. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Thia, K.T.; Loftus, E.V., Jr.; Sandborn, W.J.; Yang, S.K. An update on the epidemiology of inflammatory bowel disease in Asia. Am. J. Gastroenterol. 2008, 103, 3167–3182. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.K.; Abraham, B.; El-Serag, H. Dietary intake and risk of developing inflammatory bowel disease: A systematic review of the literature. Am. J. Gastroenterol. 2011, 106, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Khalili, H.; Konijeti, G.G.; Higuchi, L.M.; de Silva, P.; Fuchs, C.S.; Willett, W.C.; Richter, J.M.; Chan, A.T. Long term intake of dietary fat and risk of ulcerative colitis and Crohn’s disease. Gut 2014, 63, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Jantchou, P.; Morois, S.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; Carbonnel, F. Animal protein intake and risk of inflammatory bowel disease: The E3N prospective study. Am. J. Gastroenterol. 2010, 105, 2195–2201. [Google Scholar] [CrossRef] [PubMed]
- Tjonneland, A.; Overvad, K.; Bergmann, M.M.; Nagel, G.; Linseisen, J.; Hallmans, G.; Palmqvist, R.; Sjodin, H.; Hagglund, G.; Berglund, G.; et al. IBD in EPIC Study Investigators. Linoleic acid, a dietary n-6 polyunsaturated fatty acid, and the aetiology of ulcerative colitis: A nested case-control study within a European prospective cohort study. Gut 2009, 58, 1606–1611. [Google Scholar] [PubMed]
- De Silva, P.S.; Luben, R.; Shrestha, S.S.; Khaw, K.T.; Hart, A.R. Dietary arachidonic and oleic acid intake in ulcerative colitis etiology: A prospective cohort study using 7-day food diaries. Eur. J. Gastroenterol. Hepatol. 2014, 26, 11–18. [Google Scholar] [CrossRef] [PubMed]
- John, S.; Luben, R.; Shrestha, S.S.; Welch, A.; Khaw, K.T.; Hart, A.R. Dietary n-3 polyunsaturated fatty acids and the aetiology of ulcerative colitis: A UK prospective cohort study. Eur. J. Gastroenterol. Hepatol. 2010, 22, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Khalili, H.; Konijeti, G.G.; Higuchi, L.M.; de Silva, P.; Korzenik, J.R.; Fuchs, C.S.; Willett, W.C.; Richter, J.M.; Chan, A.T. A prospective study of long term intake of dietary fiber and risk of Crohn’s disease and ulcerative colitis. Gastroenterology 2013, 145, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Albenberg, L.; Compher, C.; Baldassano, R.; Piccoli, D.; Lewis, J.D.; Wu, G.D. Diet in the pathogenesis and treatment of inflammatory bowel diseases. Gastroenterology 2015, 148, 1087–1106. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology Group of the Research Committee of Inflammatory Bowel Disease in Japan. Dietary and other risk factors of ulcerative colitis. A case-control study in Japan. J. Clin. Gastroenterol. 1994, 19, 166–171. [Google Scholar]
- Amre, D.K.; D’Souza, S.; Morgan, K.; Seidman, G.; Lambrette, P.; Grimard, G.; Israel, D.; Mack, D.; Ghadirian, P.; Deslandres, C.; et al. Imbalances in dietary consumption of fatty acids, vegetables, and fruits are associated with risk for Crohn’s disease in children. Am. J. Gastroenterol. 2007, 102, 2016–2025. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, S.; Levy, E.; Mack, D.; Israel, D.; Lambrette, P.; Ghadirian, P.; Deslandres, C.; Morgan, K.; Seidman, E.G.; Amre, D.K. Dietary patterns and risk for Crohn’s disease in children. Inflamm. Bowel Dis. 2008, 14, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, C.; Paerregaard, A.; Munkholm, P.; Wewer, V. Environmental factors and risk of developing paediatric inflammatory bowel disease—A population based study 2007–2009. J. Crohn’s Colitis 2013, 7, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Gilat, T.; Hacohen, D.; Lilos, P.; Langman, M.J. Childhood factors in ulcerative colitis and Crohn’s disease. An international cooperative study. Scand. J. Gastroenterol. 1987, 22, 1009–1024. [Google Scholar] [CrossRef] [PubMed]
- Baron, S.; Turck, D.; Leplat, C.; Merle, V.; Gower-Rousseau, C.; Marti, R.; Yzet, T.; Lerebours, E.; Dupas, J.L.; Debeugny, S.; et al. Environmental risk factors in paediatric inflammatory bowel diseases: A population based case control study. Gut 2005, 54, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Galvez, J.; Rodríguez-Cabezas, M.E.; Zarzuelo, A. Effects of dietary fiber on inflammatory bowel disease. Mol. Nutr. Food Res. 2005, 49, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Navarro, J.; Vargas, J.; Cezard, J.P.; Charritat, J.L.; Polonovski, C. Prolonged constant rate elemental enteral nutrition in Crohn’s disease. J. Pediatr. Gastroenterol. Nutr. 1982, 1, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, I.R.; Udeen, S.; Davies, P.S.; Savage, M.O.; Walker-Smith, J.A. Remission induced by an elemental diet in small bowel Crohn’s disease. Arch. Dis. Child. 1987, 62, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Heuschkel, R.B.; Menache, C.C.; Megerian, J.T.; Baird, A.E. Enteral nutrition and corticosteroids in the treatment of acute Crohn’s disease in children. J. Pediatr. Gastroenterol. Nutr. 2000, 31, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Dziechciarz, P.; Horvath, A.; Shamir, R.; Szajewska, H. Meta-analysis: enteral nutrition in active Crohn’s disease in children. Aliment. Pharmacol. Ther. 2007, 26, 795–806. [Google Scholar] [CrossRef] [PubMed]
- Zachos, M.; Tondeur, M.; Griffiths, A.M. Enteral nutritional therapy for induction of remission in Crohn’s disease. Cochrane Database Syst. Rev. 2007, 1, CD000542. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, E.; Gaunt, W.W.; Cardigan, T.; Garrick, V.; McGrogan, P.; Russell, R.K. The use of exclusive enteral nutrition for induction of remission in children with Crohn’s disease demonstrates that disease phenotype does not influence clinical remission. Aliment. Pharmacol. Ther. 2009, 30, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Fell, J.M.; Paintin, M.; Arnaud-Battandier, F.; Beattie, R.M.; Hollis, A.; Kitching, P.; Donnet-Hughes, A.; MacDonald, T.T.; Walker-Smith, J.A. Mucosal healing and a fall in mucosal pro-inflammatory cytokine mRNA induced by a specific oral polymeric diet in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2000, 14, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Afzal, N.A.; Van Der Zaag-Loonen, H.J.; Arnaud-Battandier, F.; Davies, S.; Murch, S.; Derkx, B.; Heuschkel, R.; Fell, J.M. Improvement in quality of life of children with acute Crohn’s disease does not parallel mucosal healing after treatment with exclusive enteral nutrition. Aliment. Pharmacol. Ther. 2004, 20, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Bannerjee, K.; Camacho-Hübner, C.; Babinska, K.; Dryhurst, K.M.; Edwards, R.; Savage, M.O.; Sanderson, I.R.; Croft, N.M. Anti-inflammatory and growth-stimulating effects precede nutritional restitution during enteral feeding in Crohn disease. J. Pediatr. Gastroenterol. Nutr. 2004, 38, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Gavin, J.; Anderson, C.E.; Bremner, A.R.; Beattie, R.M. Energy intakes of children with Crohn’s disease treated with enteral nutrition as primary therapy. J. Hum. Nutr. Diet. 2005, 18, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Afzal, N.A.; Davies, S.; Paintin, M.; Arnaud-Battandier, F.; Walker-Smith, J.A.; Murch, S.; Heuschkel, R.; Fell, J. Colonic Crohn’s disease in children does not respond well to treatment with enteral nutrition if the ileum is not involved. Dig. Dis. Sci. 2005, 50, 1471–1475. [Google Scholar] [CrossRef] [PubMed]
- Knight, C.; El-Matary, W.; Spray, C.; Sandhu, B.K. Long-term outcome of nutritional therapy in paediatric Crohn’s disease. Clin. Nutr. 2005, 24, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Day, A.S.; Whitten, K.E.; Lemberg, D.A.; Clarkson, C.; Vitug-Sales, M.; Jackson, R.; Bohane, T.D. Exclusive enteral feeding as primary therapy for Crohn’s disease in Australian children and adolescents: A feasible and effective approach. J. Gastroenterol. Hepatol. 2006, 21, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- De Bie, C.; Kindermann, A.; Escher, J. Use of exclusive enteral nutrition in paediatric Crohn’s disease in The Netherlands. J. Crohns Colitis 2013, 7, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Grover, Z.; Burgess, C.; Muir, R.; Reilly, C.; Lewindon, P.J. Early Mucosal Healing with Exclusive Enteral Nutrition is Associated with Improved Outcomes in Newly Diagnosed Children with Luminal Crohn’s disease. J. Crohn’s Colitis 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Akobeng, A.K.; Miller, V.; Stanton, J.; Elbadri, A.M.; Thomas, A.G. Double-blind randomized controlled trial of glutamine-enriched polymeric diet in the treatment of active Crohn’s disease. J. Pediatr. Gastroenterol. Nutr. 2000, 30, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Krantz, M.; Bodin, L.; Stenhammar, L.; Lindquist, B. Elemental versus polymeric enteral nutrition in paediatric Crohn’s disease: A multicentre randomized controlled trial. Acta Paediatr. 2004, 93, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.; Macdonald, S.; Hill, S.M.; Thomas, A.; Murphy, M.S. Treatment of active Crohn’s disease in children using partial enteral nutrition with liquid formula: A randomised controlled trial. Gut 2006, 55, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.F.; Johnson, T.; Davies, P.; Murphy, M.S. Does polymeric formula improve adherence to liquid diet therapy in children with active Crohn’s disease? Arch. Dis. Child. 2007, 92, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Hartman, C.; Berkowitz, D.; Weiss, B.; Shaoul, R.; Levine, A.; Adiv, O.E.; Shapira, R.; Fradkin, A.; Wilschanski, M.; Tamir, A.; et al. Nutritional supplementation with polymeric diet enriched with transforming growth factor-beta 2 for children with Crohn’s disease. Isr. Med. Assoc. J. 2008, 10, 503–507. [Google Scholar] [PubMed]
- Rubio, A.; Pigneur, B.; Garnier-Lengliné, H.; Talbotec, C.; Schmitz, J.; Canioni, D.; Goulet, O.; Ruemmele, F.M. The efficacy of exclusive nutritional therapy in paediatric Crohn’s disease, comparing fractionated oral vs. continuous enteral feeding. Aliment. Pharmacol. Ther. 2011, 33, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Grogan, J.L.; Casson, D.H.; Terry, A.; Burdge, G.C.; El-Matary, W.; Dalzell, A.M. Enteral feeding therapy for newly diagnosed pediatric Crohn’s disease: A double-blind randomized controlled trial with two years follow-up. Inflamm. Bowel Dis. 2012, 18, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Baldassano, R.N.; Otley, A.R.; Albenberg, L.; Griffiths, A.M.; Compher, C.; Chen, E.Z.; Li, H.; Gilroy, E.; Nessel, L.; et al. Comparative Effectiveness of Nutritional and Biological Therapy in North American Children with Active Crohn’s Disease. Inflamm. Bowel Dis. 2015, 21, 1786–1793. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.G.; Taylor, F.; Miller, V. Dietary intake and nutritional treatment in childhood Crohn’s disease. J. Pediatr. Gastroenterol. Nutr. 1993, 17, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Ruuska, T.; Savilahti, E.; Mäki, M.; Ormälä, T.; Visakorpi, J.K. Exclusive whole protein enteral diet versus prednisolone in the treatment of acute Crohn’s disease in children. J. Pediatr. Gastroenterol. Nutr. 1994, 19, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Terrin, G.; Canani, R.B.; Ambrosini, A.; Viola, F.; De Mesquita, M.B.; Di Nardo, G.; Dito, L.; Cucchiara, S. A semielemental diet (Pregomin) as primary therapy for inducing remission in children with active Crohn’s disease. Ital. J. Pediatr. 2002, 28, 401–405. [Google Scholar]
- Borrelli, O.; Cordischi, L.; Cirulli, M.; Paganelli, M.; Labalestra, V.; Uccini, S.; Russo, P.M.; Cucchiara, S. Polymeric diet alone versus corticosteroids in the treatment of active pediatric Crohn’s disease: A randomized controlled open-label trial. Clin. Gastroenterol. Hepatol. 2006, 4, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Berni Canani, R.; Terrin, G.; Borrelli, O.; Romano, M.T.; Manguso, F.; Coruzzo, A.; D’Armiento, F.; Romeo, E.F.; Cucchiara, S. Short- and long-term therapeutic efficacy of nutritional therapy and corticosteroids in paediatric Crohn’s disease. Dig. Liver. Dis. 2006, 38, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Soo, J.; Malik, B.A.; Turner, J.M.; Persad, R.; Wine, E.; Siminoski, K.; Huynh, H.Q. Use of exclusive enteral nutrition is just as effective as corticosteroids in newly diagnosed pediatric Crohn’s disease. Dig. Dis. Sci. 2013, 58, 3584–3591. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Yu, J.; Zhao, H.; Lou, J.; Chen, F.; Peng, K.; Chen, J. Short-Term Efficacy of Exclusive Enteral Nutrition in Pediatric Crohn’s Disease: Practice in China. Gastroenterol. Res. Pract. 2015, 2015, 428354. [Google Scholar] [CrossRef] [PubMed]
- Grover, Z.; Muir, R.; Lewindon, P. Exclusive enteral nutrition induces early clinical, mucosal and transmural remission in paediatric Crohn’s disease. J. Gastroenterol. 2014, 49, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Noble, A.; Kachelries, K.E.; Albenberg, L.; Kelsen, J.R.; Grossman, A.B.; Baldassano, R.N. A novel enteral nutrition protocol for the treatment of pediatric Crohn’s disease. Inflamm. Bowel Dis. 2013, 19, 1374–1378. [Google Scholar] [CrossRef] [PubMed]
- Suskind, D.L.; Wahbeh, G.; Gregory, N.; Vendettuoli, H.; Christie, D. Nutritional therapy in pediatric Crohn disease: The specific carbohydrate diet. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.A.; Gold, B.D.; Oliva, S.; Lewis, J.; Stallworth, A.; Koch, B.; Eshee, L.; Mason, D. Clinical and mucosal improvement with specific carbohydrate diet in pediatric Crohn disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Sigall-Boneh, R.; Pfeffer-Gik, T.; Segal, L.; Zangen, T.; Boaz, M.; Levine, A. Partial enteral nutrition with a Crohn’s disease exclusion diet is effective for induction of remission in children and young adults with Crohn’s disease. Inflamm. Bowel Dis. 2014, 20, 1353–1360. [Google Scholar] [CrossRef] [PubMed]
- Strisciuglio, C.; Giannetti, E.; Martinelli, M.; Sciorio, E.; Staiano, A.; Miele, E. Does cow’s milk protein elimination diet have a role on induction and maintenance of remission in children with ulcerative colitis? Acta Paediatr. 2013, 102, e273–e278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruemmele, F.M.; Veres, G.; Kolho, K.L.; Griffiths, A.; Levine, A.; Escher, J.C.; Amil Dias, J.; Barabino, A.; Braegger, C.P.; Bronsky, J.; et al. Consensus guidelines of ecco/espghan on the medical management of pediatric Crohn’s disease. J. Crohn’s Colitis 2014, 8, 1179–1207. [Google Scholar] [CrossRef] [PubMed]
- Belli, D.C.; Seidman, E.; Bouthillier, L.; Weber, A.M.; Roy, C.C.; Pletincx, M.; Beaulieu, M.; Morin, C.L. Chronic intermittent elemental diet improves growth failure in children with Crohn’s disease. Gastroenterology 1988, 94, 603–610. [Google Scholar] [PubMed]
- Duncan, H.; Buchanan, E.; Cardigan, T.; Garrick, V.; Curtis, L.; McGrogan, P.; Barclay, A.; Russell, R.K. A retrospective study showing maintenance treatment options for paediatric CD in the first year following diagnosis after induction of remission with EEN: Supplemental enteral nutrition is better than nothing! BMC Gastroenterol. 2014, 14, 50. [Google Scholar] [CrossRef] [PubMed]
- Takagi, S.; Utsunomiya, K.; Kuriyama, S.; Yokoyama, H.; Takahashi, S.; Iwabuchi, M.; Takahashi, H.; Takahashi, S.; Kinouchi, Y.; Hiwatashi, N.; et al. Effectiveness of an ‘half elemental diet’ as maintenance therapy for Crohn’s disease: A randomized-controlled trial. Aliment. Pharmacol. Ther. 2006, 24, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Nakahigashi, M.; Umegae, S.; Kitagawa, T.; Matsumoto, K. Impact of long-term enteral nutrition on clinical and endoscopic recurrence after resection for Crohn’s disease: A prospective, non-randomized, parallel, controlled study. Aliment. Pharmacol. Ther. 2007, 25, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Shiraki, M.; Nakahigashi, M.; Umegae, S.; Matsumoto, K. Enteral nutrition to suppress postoperative Crohn’s disease recurrence: A five-year prospective cohort study. Int. J. Colorectal Dis. 2013, 28, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Hirai, F.; Ishihara, H.; Yada, S.; Esaki, M.; Ohwan, T.; Nozaki, R.; Ashizuka, S.; Inatsu, H.; Ohi, H.; Aoyagi, K.; et al. Effectiveness of concomitant enteral nutrition therapy and infliximab for maintenance treatment of Crohn’s disease in adults. Dig. Dis. Sci. 2013, 58, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Nakahigashi, M.; Umegae, S.; Matsumoto, K. Prospective clinical trial: Enteral nutrition during maintenance infliximab in Crohn’s disease. J. Gastroenterol. 2010, 45, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Wilschanski, M.; Sherman, P.; Pencharz, P.; Davis, L.; Corey, M.; Griffiths, A. Supplementary enteral nutrition maintains remission in paediatric Crohn’s disease. Gut 1996, 38, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Chiba, M.; Abe, T.; Tsuda, H.; Sugawara, T.; Tsuda, S.; Tozawa, H.; Fujiwara, K.; Imai, H. Lifestyle-related disease in Crohn’s disease: Relapse prevention by a semi-vegetarian diet. World J. Gastroenterol. 2010, 16, 2484–2495. [Google Scholar] [CrossRef] [PubMed]
- Obih, C.; Wahbeh, G.; Lee, D.; Braly, K.; Giefer, M.; Shaffer, M.L.; Nielson, H.; Suskind, D.L. Specific carbohydrate diet for pediatric inflammatory bowel disease in clinical practice within an academic ibd center. Nutrition 2015, 32, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Goel, A.; Kunnumakkara, A.B.; Aggarwal, B.B. Curcumin as “curcumin”: From kitchen to clinic. Biochem. Pharmacol. 2008, 75, 787–809. [Google Scholar] [CrossRef] [PubMed]
- Basile, V.; Ferrari, E.; Lazzari, S.; Belluti, S.; Pignedoli, F.; Imbriano, C. Curcumin derivatives: Molecular basis of their anti-cancer activity. Biochem. Pharmacol. 2009, 78, 1305–1315. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan-Coyne, G.; O’Sullivan, G.C.; O’Donovan, T.R.; Piwocka, K.; McKenna, S.L. Curcumin induces apoptosis-independent death in oesophageal cancer cells. Br. J. Cancer 2009, 101, 1585–1595. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, T.; Fong, C. The resolution of inflammation: Anti-inflammatory roles for nf-kappab. Int. J. Biochem. Cell Biol. 2010, 42, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Hanai, H.; Sugimoto, K. Curcumin has bright prospects for the treatment of inflammatory bowel disease. Curr. Pharm. Des. 2009, 15, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Hanai, H.; Iida, T.; Takeuchi, K.; Watanabe, F.; Maruyama, Y.; Andoh, A.; Tsujikawa, T.; Fujiyama, Y.; Mitsuyama, K.; Sata, M.; et al. Curcumin maintenance therapy for ulcerative colitis: Randomized, multicenter, double-blind, placebo-controlled trial. Clin. Gastroenterol. Hepatol. 2006, 4, 1502–1506. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.H.; Nawaz, Z.; Pertani, S.A.; Roomi, A.; Mahmood, H.; Saeed, S.A.; Gilani, A.H. Inhibitory effect of curcumin, a food spice from turmeric, on platelet-activating factor- and arachidonic acid-mediated platelet aggregation through inhibition of thromboxane formation and Ca2+ signaling. Biochem. Pharmacol. 1999, 58, 1167–1172. [Google Scholar] [CrossRef]
- Suskind, D.L.; Wahbeh, G.; Burpee, T.; Cohen, M.; Christie, D.; Weber, W. Tolerability of curcumin in pediatric inflammatory bowel disease: A forced-dose titration study. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Akabas, S.R.; Deckelbaum, R.J. Summary of a workshop on n-3 fatty acids: Current status of recommendations and future directions. Am. J. Clin. Nutr. 2006, 83, 1536S–1538S. [Google Scholar] [PubMed]
- Ergas, D.; Eilat, E.; Mendlovic, S.; Sthoeger, Z.M. N-3 fatty acids and the immune system in autoimmunity. Isr. Med. Assoc. J. 2002, 4, 34–38. [Google Scholar] [PubMed]
- Calder, P.C. N-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am. J. Clin. Nutr. 2006, 83, 1505S–1519S. [Google Scholar] [PubMed]
- Calder, P.C. Fatty acids and immune function: Relevance to inflammatory bowel diseases. Int. Rev. Immunol. 2009, 28, 506–534. [Google Scholar] [CrossRef] [PubMed]
- Belluzzi, A.; Brignola, C.; Campieri, M.; Pera, A.; Boschi, S.; Miglioli, M. Effect of an enteric-coated fish-oil preparation on relapses in Crohn’s disease. N. Engl. J. Med. 1996, 334, 1557–1560. [Google Scholar] [CrossRef] [PubMed]
- Lorenz-Meyer, H.; Bauer, P.; Nicolay, C.; Schulz, B.; Purrmann, J.; Fleig, W.E.; Scheurlen, C.; Koop, I.; Pudel, V.; Carr, L. Omega-3 fatty acids and low carbohydrate diet for maintenance of remission in Crohn’s disease. A randomized controlled multicenter trial. Study group members (german Crohn’s disease study group). Scand. J. Gastroenterol. 1996, 31, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Seidner, D.L.; Lashner, B.A.; Brzezinski, A.; Banks, P.L.; Goldblum, J.; Fiocchi, C.; Katz, J.; Lichtenstein, G.R.; Anton, P.A.; Kam, L.Y.; et al. An oral supplement enriched with fish oil, soluble fiber, and antioxidants for corticosteroid sparing in ulcerative colitis: A randomized, controlled trial. Clin. Gastroenterol. Hepatol. 2005, 3, 358–369. [Google Scholar] [CrossRef]
- Meister, D.; Ghosh, S. Effect of fish oil enriched enteral diet on inflammatory bowel disease tissues in organ culture: Differential effects on ulcerative colitis and Crohn’s disease. World J. Gastroenterol. 2005, 11, 7466–7472. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Sandborn, W.J.; Mittmann, U.; Bar-Meir, S.; D’Haens, G.; Bradette, M.; Cohen, A.; Dallaire, C.; Ponich, T.P.; McDonald, J.W.; et al. Omega-3 free fatty acids for the maintenance of remission in Crohn disease: The epic randomized controlled trials. J. Am. Med. Assoc. 2008, 299, 1690–1697. [Google Scholar] [CrossRef] [PubMed]
- Lev-Tzion, R.; Griffiths, A.M.; Leder, O.; Turner, D. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn’s disease. Cochrane Database Syst. Rev. 2014, 2, CD006320. [Google Scholar] [CrossRef] [PubMed]
- Romano, C.; Cucchiara, S.; Barabino, A.; Annese, V.; Sferlazzas, C. Usefulness of omega-3 fatty acid supplementation in addition to mesalazine in maintaining remission in pediatric Crohn’s disease: A double-blind, randomized, placebo-controlled study. World J. Gastroenterol. 2005, 11, 7118–7121. [Google Scholar] [CrossRef] [PubMed]
- Azcue, M.; Rashid, M.; Griffiths, A.; Pencharz, P.B. Energy expenditure and body composition in children with Crohn’s disease: Effect of enteral nutrition and treatment with prednisolone. Gut 1997, 41, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Bannerman, E.; Davidson, I.; Conway, C.; Culley, D.; Aldhous, M.C.; Ghosh, S. Altered subjective appetite parameters in Crohn’s disease patients. Clin. Nutr. 2001, 20, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Gerasimidis, K.; McGrogan, P.; Edwards, C.A. The aetiology and impact of malnutrition in paediatric inflammatory bowel disease. J. Hum. Nutr. Diet. 2011, 24, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Beattie, R.M.; Camacho-Hubner, C.; Wacharasindhu, S.; Cotterill, A.M.; Walker-Smith, J.A.; Savage, M.O. Responsiveness of IGF-1 and IGFBP-3 to therapeutic intervention in children and adolescents with Crohn’s disease. Clin. Endocrinol. 1998, 49, 483–489. [Google Scholar] [CrossRef]
- Motil, K.J.; Grand, R.J.; Maletskos, C.J.; Young, V.R. The effect of disease, drug, and diet on whole body protein metabolism in adolescents with Crohn’s disease and growth failure. J. Pediatr. 1982, 101, 345–351. [Google Scholar] [CrossRef]
- O’Morain, C.; Segal, A.M.; Levi, A.J.; Valman, H.B. Elemental diet in acute Crohn’s disease. Arch. Dis. Child. 1983, 58, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Polk, D.B.; Hattner, J.A.; Kerner, J.A., Jr. Improved growth and disease activity after intermittent administration of a defined formula diet in children with Crohn’s disease. J. Parenter. Enteral. Nutr. 1992, 16, 499–504. [Google Scholar] [CrossRef]
- Cosgrove, M.; Jenkins, H.R. Experience of percutaneous endoscopic gastrostomy in children with Crohn’s disease. Arch. Dis. Child. 1997, 76, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, F.A.; Leopold, S.; Lincoln, M.; Hyams, J.S.; Griffiths, A.M.; Lerer, T. A two-year longitudinal study of persistent lean tissue deficits in children with Crohn’s disease. Clin. Gastroenterol. Hepatol. 2009, 7, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, J.S.; Klibanski, A.; Neer, R.M. A longitudinal evaluation of bone mineral density in adult men with histories of delayed puberty. J. Clin. Endocrinol. Metab. 1996, 81, 1152–1155. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.H.; Sdepanian, V.L.; Szejnfeld, V.L.; de Morais, M.B.; Fagundes-Neto, U. Risk factors for low bone mineral density in children and adolescents with inflammatory bowel disease. Dig. Dis. Sci. 2008, 53, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- Whitten, K.E.; Leach, S.T.; Bohane, T.D.; Woodhead, H.J.; Day, A.S. Effect of exclusive enteral nutrition on bone turnover in children with Crohn’s disease. J. Gastroenterol. 2010, 45, 399–405. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Dietary Factors and Etiology in Pediatric IBD | |||
|---|---|---|---|
| Author/Year | Study Type | Population | Main Findings |
| Gilat et al. 1987 [14] | Case-control study | Patients with IBD (n = 499; UC = 197, CD = 302) aged < 25 years with disease onset before 20 years of age. For each patient two age and sex matched health controls. | - Patients with CD and UC consumed significantly lower fruits and vegetables than controls (p < 0.01). For UC: low consumption (0 and <1/day) vs. high consumption (1–3 and >4/day) OR = 0.77; 95% CI 0.45 to 1.35. For CD: low consumption (0 and <1/day) vs. high consumption (1–3 and >4/day) OR = 0.58; 95% CI 0.37 to 0.91. - No significant differences were found between patients and controls in the frequency of breast feeding (p < 0.01), cereal consumption (p < 0.01) and sugar added to milk in infancy (p < 0.01). |
| Japanese Epidemiology Group of the Research Committee of IBD, 1994 [10] | Case-control study | Patients with UC (n = 101) who were aged 10–39 years at the time of disease onset. Healthy control subjects (n = 143). | - Combined consumption of Western foods (bread for breakfast, butter, margarine, cheese, meats, and ham and sausage) was significantly related to an increased risk of UC (Relative risk (RR) for low consumption 1.0, RR for intermediate consumption 1.9; 95% CI 1.0 to 3.7, RR for high consumption 2.1, 95% CI 1.0 to 4.1; trend, p = 0.04). - Margarine (as an individual Western food item) was positively associated with UC (trend, p = 0.005). |
| Baron et al. 2005 [15] | Case-control study | IBD patients (n = 282; CD 222, UC 60) with onset before 17 years of age and healthy controls matched for age, sex, and geographical location (n = 282). | - Breastfeeding either partially or exclusively was a risk factor for CD (CD OR = 2.1; 95% CI 1.3 to 3.4, p = 0.003). - Regular drinking of tap water was a protective factor for CD (CD = OR 0.6; 95% CI 0.3 to 1, p = 0.05). |
| Amre et al. 2007 [11] | Case-control study | Children and adolescents ≤20 years (n = 130), newly diagnosed with CD mean age at diagnosis (±SD) 14.2 ± 2.7 years. Healthy controls matched for age and sex (n = 202). | - Higher amounts of vegetables (OR = 0.69; 95% CI 0.33 to 1.44, p = 0.03), fruits (OR = 0.49; 95% CI 0.25–0.96, p = 0.02), fish (OR = 0.46; 95% CI 0.20 to 1.06, p = 0.02) and dietary fiber (OR = 0.12; 95%, CI 0.04 to 0.37, p < 0.001) protected from CD. - Consumption of LC ω-3 (OR = 0.44; 95%, CI 0.19 to 1.00, p < 0.001) were negatively associated with CD. - A higher ratio of LC ω-3/ω-6 fatty acids (OR = 0.32, 95% CI 0.14 to 0.71, p = 0.02) were significantly associated with lower risks for CD. |
| D’Souza et al. 2008 [12] | Case-control study | Children and adolescents ≤20 years (n = 149), newly diagnosed with CD mean age at diagnosis (±SD) 13.3 ± 2.6 years. Healthy controls matched for age and sex (n = 251). | - Meats, fatty foods and desserts (OR = 4.7; 95% CI 1.6 to 14.2) were positively associated with CD. - Vegetables, fruits, olive oil, fish, grains, and nuts were inversely associated with CD in both genders (girls: OR = 0.3; 95% CI 0.1 to 0.9; boys: OR = 0.2; 95% CI 0.1 to 0.5). |
| Jakobsen et al. 2012 [13] | Case-control study | Children and adolescents with IBD (n = 118; CD 59, UC 56, IBD-unclassified 3) aged <15 years. Healthy controls matched for age and sex (n = 477). | - High sugar intakes were a risk factor for IBD (IBD OR = 2.5; 95% CI 1.0 to 6.2, CD OR = 2.9; 95% CI 1.0 to 8.5). - Protective factors were daily vs. less than daily vegetable consumption (CD OR = 0.3; 95% CI 0.1 to 1.0, UC OR = 0.3; 95% CI 0.1 to 0.8) and whole-meal bread consumption (IBD OR = 0.5; 95% CI 0.3 to 0.9, CD OR = 0.4; 95% CI 0.2 to 0.9). |
| Clinical Studies on Efficacy of Exclusive Enteral Nutrition | ||||
|---|---|---|---|---|
| Author/Year | Study Type | Population | Method | Main Findings |
| Navarro et al. 1982 [17] | Clinical trial | Children with active CD (n = 17) | Exclusive constant rate enteral nutrition (CREN) using a combination of elemental diet and continuous alimentation for 2–7 months, subsequently CREN used to supplement oral alimentation from 12 to 22 months. | After 7 months of exclusive CREN: all children’s symptoms improved; 100% of children presented moderate disease (Lloyd Still and Green scoring >50). |
| Fell et al. 2000 [23] | Clinical trial | Children with active CD (n = 29) | EEN with TGFβ2 enriched PF for 8 weeks. | - After 8 weeks 79% (23/29) of children were in clinical remission. - PCDAI declined with treatment. Median PCDAI at baseline 30 (range 12.5–72.5) declined with treatment by a median of 15 at 2 weeks and 25 at 8 weeks (p < 0.00001). - Macroscopic and histological healing in the terminal ileum and colon was associated with a decline in ileal and colonic interleukin-1β. (pre-treatment to post-treatment ratio 0.008 and 0.06: p = 0.001, p = 0.006). |
| Afzal et al. 2004 [24] | Clinical trial | Children and adolescents with active CD (n = 26), mean age 14 years | EEN with PF for 8 weeks. | 88.6% achieved clinical remission. |
| Bannerjee et al. 2004 [25] | Clinical trial | Children with active CD (n = 12) | EEN with PF for 6 weeks. | Significant improvements in inflammatory markers by day 3 (p < 0.05) and in clinical activity index PCDAI by day 7. |
| Gavin et al. 2005 [26] | Retrospective cohort study | Children and adolescents with new onset CD (n = 40), aged 6–16 years | EEN with PF for 8 weeks. | All patients improved symptomatically and gained weight after 8 weeks of EEN. |
| Afzal et al. 2005 [27] | Prospective cohort study | Children and adolescents with active CD (n = 65), aged 8–17 years. Disease localization: ileal (n = 12), ileocolonic (n = 39), colonic (n = 14). | EEN with PF for 8 weeks. | 77% remission rate. Remission rates: Colonic group: 50% (7/14), ileocolon group 82.1% (32/39), ileum group 91.7% (11/12), (χ2 test, p = 0.021)). The colonic disease group showed the least fall in PCDAI scores at completion of treatment with EEN (p = 0.03), with the lowest remission rate (50%). |
| Knight et al. 2005 [28] | Retrospective cohort study | Children with CD (n = 44) | Treatment with EEN as primary treatment for 6–8 weeks. | 90% (40/44) of patients responded to EEN with a median time to remission of 6 weeks. Crohn’s disease activity index (CDAI) decreased from pre-EEN to post-EEN, mean values of CDAI not available. |
| Day et al. 2006 [29] | Retrospective cohort study | Children with newly diagnosed CD (group 1, n = 15) and with active known long-standing CD (group 2, n = 12), mean age 11.8 years | - Group 1: EEN with PF for 6–8 weeks as sole initial therapy - Group 2: EEN with PF for 6–8 weeks in addition to any current medical therapy. | Twenty-four (89%) of 27 children completed their prescribed course of EEN. Nineteen (79%) of 24 children entered clinical remission (80% (12/15) in group 1 and 58% (7/12) in group 2). There was no clear relationship between disease location and response to treatment: 75% (3/4) with isolated small bowel, 72.5% (10/14) with ileocolonic and 67% (6/9) with pancolic disease attained remission (p > 0.05). In group 1 successful response to EEN was associated with positive weight gains (average weight gain 4.7 ± 3.5 kg) with mean PCDAI decreasing from 37.1 ± 10.8 to 6.7 ± 5.1 after 8 weeks (p < 0.0001). Also in group 2, despite a minor rate of remission, the overall average PCDAI scores significantly fell at 8 weeks (p < 0.0001) with an improvement of body weight and in at least one markers of inflammation. |
| De Bie et al. 2013 [30] | Retrospective cohort study | Children with newly diagnosed CD (n = 77), median age 13.9 years | Patients received EEN (as either hyperosmolar sip feeds or PF by nasogastric tube) for 6 weeks as remission induction therapy, combined with azathioprine maintenance treatment in 92%. | In patients completing a 6-week course of EEN (58) complete remission was achieved in 71% of patients, partial remission in 26%, and no response in 3%. Complete remission rates were higher in children presenting with isolated ileal/ileocaecal disease and malnutrition. |
| Grover et al. 2016 [31] | Clinical trial | Children with newly diagnosed predominantly luminal CD (n = 54), median age 12.4 years | EEN for 6–8 weeks in association with early thiopurine treatment (<3 months from diagnosis). Median duration between pre and post EEN assessments was 60.5 days (IQR 56–69.5) | Post EEN: remission rate (PCDAI < 10) 83% (45/54), biochemical remission (CRP < 5 mg/dL) 72% (39/54), complete mucosal healing 33% (18/54). Sustained remission was superior in those with complete mucosal healing vs. endoscopic disease 72% (13/18) vs. 28% (10/36), p = 0.003 at 1 year, 50% (8/16) vs. 8% (3/24), p = 0.008 at 2 years and 50% (8/16) vs. 6% (1/19), p = 0.005 at 3 years. |
| Clinical Studies Comparing Efficacy between Two Enteral Nutrition Regimens | ||||
|---|---|---|---|---|
| Author/Year | Study Type | Population | Method | Main Findings |
| Akobeng et al. 2000 [32] | Randomized controlled trial | Children with active CD (n = 18). | Standard PF with a low glutamine content (4% of amino-acid composition, group S) vs. glutamine enriched PF (42% of amino acid composition, group G) for 4 weeks. | - No difference in remission rates at week 4 between the two groups’ remission 5/9 (55.5%) in group S, 4/9 (44.4%) in group G (p = 0.5). ARC −0.11 (exact 95% CI: −0.57 to 0.35). - Improvement in mean PCDAI was significantly more in group S (p = 0.002). |
| Ludvigsson et al. 2004 [33] | Randomized controlled trial | Children with active CD (n = 33) involving small bowel, colon and perianal region. | Exclusive EEN with ED (n = 16) vs. PF (n = 17) for 6 weeks. | - Similar remission rates at 6 weeks (ED 11/16 (69%), PF 14/17 (82%); p = 0.438). Patients on PF gained more weight compared to ED (p = 0.004). ARC 0.14 (exact 95% CI: −0.15 to 0.42). |
| Johnson et al. 2006 [34] | Randomized controlled trial | Children with active CD (n = 50) involving small bowel and/or colon. | Patients randomly assigned to receive: - 50% total energy requirements with ED (PEN, n = 26) for 6 weeks. - 100% energy requirements with ED (EEN, n = 24) for 6 weeks. | Remission rate with PEN was lower than with EEN (PEN 4/26 (15%), EEN 10/24 (42%) p = 0.035). Although PCDAI fell in both groups, the reduction was greater with EEN (PCDAI reduction PEN −13, 95% CI (−7 to −19) p = 0.001; EEN −26 95% CI (−19 to −33), p = 0.001) (p = 0.005). ARC = −0.26 (exact 95% CI −0.50 to −0.02). |
| Rodrigues et al. 2007 [35] | Retrospective cohort study | Children with active CD (n = 98) involving small bowel and/or colon. | Children received EEN at the time of first presentation either PF (n = 45, median age 12.2 years) or ED (n = 53, median age 11.8 years). | Remission rates were similar between children receiving PF and ED (ED 64%, 95% CI 51–77 vs. PF 51%, 95% CI 37–66, p = 0.19). ARC = −0.13 (exact 95% CI −0.32 to 0.06). The use of PF did not affect adherence to EEN but was significantly associated with reduced need for nasogastric tube administration. |
| Hartman et al. 2008 [36] | Retrospective cohort study | Children with CD (n = 64) involving small bowel, colon and upper GI tract. | Group 1 (n = 28, median age 14 years) and group 2 (n = 18, median age 12.7 years) received TGFβ2-enriched PF vs. standard PF, respectively, as a supplement to their regular nutrition (35%–50% of total caloric intake), for a median follow-up of 5.3 months for group 1 and 4.5 months for group 2. Group 3 (n = 18, median age 12.8 years) without formula supplementation, for a median follow-up of 5.5 months. | Supplementation of the diet with PF (both TGFβ enriched and standard) was associated with a decrease in PCDAI (in group 1 from 34.3 to 15.7, p < 0.0001; in group 2 from 35 to 22, p = 0.02). No significant decrease in PCDAI was recorded in group 3. Remission rates at follow-up: 57% (16/28, p = 0.001) in TGFβ2-enriched PF group, 22.2% (4/18, p = 0.03) in standard PF group. Remission rate in group 3 was 22.2 (4/18, p = 0.03). ARC = 0.35 (exact 95% CI 0.08 to 0.61). Significant improvements in body mass index (p = 0.01) and erythrocyte sedimentation rate (p = 0.03) were recorded at follow-up (median 3.4 months) only in the TGFβ2-enriched PF group. |
| Rubio et al. 2011 [37] | Retrospective cohort study | Children with newly diagnosed CD or with a first relapse of an established disease on stable medical treatment (n = 106). | Children received EEN with PF for 8 weeks as remission induction therapy either per os (group 1, n = 45, mean age 11.3 years) or by continuous enteral route via a nasogastric tube (group 2, n = 61, mean age 10.9 years). | Fractionated oral nutritional therapy (group 1) didn’t significantly differ from continuous enteral administration (group 2) in inducing remission (75% vs. 85%, respectively, p = 0.157). All patients showed a significant decrease in disease severity assessed by PCDAI (p < 0.0001) and significant improvements in anthropometric measures and inflammatory indices. |
| Grogan et al. 2012 [38] | Double-blind randomized controlled trial | Children with newly diagnosed CD (n = 34). | Children were randomized to ED (n = 15, mean age 12.6 years) or PF (n = 19, mean age 11.7 years) for 6 weeks and were followed up for 2 years. | No significant difference was recorded between ED and PF in inducing remission (93% 14/15 vs. 79% 15/19, respectively). ARC = 0.14 (exact 95% CI −0.08 to 0.37). One-third of children maintained remission at 2 years. |
| Lee et al. 2015 [39] | Prospective study | Children with active CD (n = 90). | Children were treated with anti-TNF (n = 52), with EEN (n = 22), and with PEN plus ad lib diet (n = 16) for 8 weeks. | Clinical remission (final PCDAI ≤ 10) was achieved by 50% on PEN, 76% EEN, and 73% anti-TNF (p = 0.08). ARC= −0.15 (exact 95% CI −0.47 to −0.16). Mucosal healing (estimated by fecal calprotectin ≤ 250 μg/g) was achieved with PEN in 14%, EEN 45%, and anti-TNF 62% (p = 0.001). ARC = −0.25 (exact 95% CI −0.52 to 0.02). |
| Clinical Studies Comparing Exclusive Enteral Nutrition to Corticosteroids | ||||
|---|---|---|---|---|
| Author/Year | Study Type | Population | Method | Main Findings |
| Sanderson et al. 1987 [18] | Randomized controlled trial | Children and adolescents with active CD aged 8.6–17.2 years (n = 17) involving the small bowel. | - 8 children treated with CS - 9 children treated with exclusive ED via nasogastric tube | - Disease activity (Lloyd–Still activity index) of the children improved significantly in both ED and PF groups after 6 weeks (p < 0.01). Growth velocity improved more in the ED group |
| Thomas et al. 1993 [40] | Randomized controlled trial | Children with active CD (n = 24): - 8% (2/24) confined to the small bowel - 29% (7/24) had ileal ± caecal involvement - 25% (6/24) ileocolic disease - 38% (9/24) disease confined to the colon | Children randomized to receive ED (n = 12) or CS (n = 12) for 4 weeks. | - Similar improvement in disease activity (PCDAI) and remission duration in both groups regardless of site of disease. In CS group activity index at baseline: 74, at week 4: 85, median change +11, (p < 0.01); in ED group activity index at baseline: 77, at week 4: 88, median change +11 (p < 0.01). - Growth velocity significantly better in ED group compared to CS group. |
| Ruuska et al. 1994 [41] | Randomized controlled trial | Children with new onset or relapsing CD (n = 19). Ten children had widespread disease affecting both colon and small intestine; in three the disease was limited to the colon and rectum, and six children had only small bowel disease. | - 10 children treated with a whole-protein based formula through a nasogastric tube for 11 weeks -9 children received high dose CS for 11 weeks | - Similar improvements of PCDAI index, clinical symptoms and inflammatory markers within 2 weeks of treatment in both groups. After the end of the follow-up period 2 months after cessation of the treatment, PCDAI was still low in both groups (PCDAI 11.9 ± 7.9 in enteral diet group and 14.3 ± 9.6 in CS group) - During the routine follow-up after the trial (0.3–2.5 years, mean 1.3 years), five of the CS group 55.5% (5/9) whereas only one from the enteral group 10% (1/10) experienced a clinical relapse. ARC = −0.46 (exact 95% CI −0.8 to −0.08). |
| Terrin et al. 2002 [42] | Randomized controlled trial | Children with active CD (n = 20), aged 7–17 years, involving the terminal ileum and different areas of the colon; no fistulae or strictures were detected. | - Group A: CS and mesalazine (n = 10) - Group B: enteral nutrition group treated with extensively hydrolyzed formula for 8 weeks (n = 10) | - Clinical remission was achieved in 90% (9/10) of patients in group B but only in 50% (5/10) in corticosteroid group (p < 0.01). ARC = 0.40 (exact 95% CI 0.04 to 0.76). Both treatments were effective in reducing PCDAI scores (baseline group A 32.0 ± 4.7, group B 34.0 ± 4.3; at week 8 group A 13.0 ± 5.18, group B 7.2 ± 3.15, p < 0.01), endoscopic scores (baseline group A 3.7 ± 0.48, group B 3.8 ± 0.42; at week 8 group A 2.4 ± 0.96, group B 1.1 ± 0.87, p < 0.01) and histological scores (baseline group A 3.3 ± 0.67, group B 3.5 ± 0.52; at week 8 group A 2.5 ± 0.52, group B 1.3 ± 0.82, p < 0.05 for group A, p < 0.01 for group B). Group B had significantly lower post-trial PCDAI scores than the CS group (PCDAI scores change group B 14.6 ± 3.6, p < 0.01, group A 24.8 ± 4.4, not significant)) |
| Borrelli et al. 2006 [43] | Randomized controlled trial | Children with active naïve CD (n = 37). | - 19 children received EEN with PF for 10 weeks - 18 children received oral CS for 10 weeks | At week 10 the remission rate was comparable between two groups: 15/19 (79%, 95% CI 56–92) in PF group and 12/18 (67%, 95% CI 44–84) in CS group (p = 0.4, not significant). ARC = 0.12 (exact 95% CI −0.16 to 0.40). The proportion of children showing mucosal healing was significantly higher in the PF (14/19, 74%; 95% CI 51 to 89) than the CS group (6/18, 33%; 95% CI 16 to 57; p < 0.05). ARC = 0.40, (exact 95% CI 0.11 to 0.70). At week 10 both endoscopic and histologic scores significantly decreased only in PF group. For endoscopic score: in PF group pre-trial 12.9 ± 0.8, post-trial 5.9 ± 0.5, p < 0.001, in CS group pre-trial 12.9 ± 0.9, post-trial 9.8 ± 1.3, not significant. For histologic scores: in PF group ileum score pre-trial 10.4 ± 0.4, post-trial 3.8 ± 0.5, p < 0.001, in CS group pre-trial 11.0 ± 04, post-trial 9.6 ± 0.7, not significant. |
| Berni Canani et al. 2006 [44] | Retrospective cohort study | Children with newly diagnosed CD (n = 47), mean age 12.1 years. | Children received nutritional therapy (NT) for 8 weeks as - Polymeric formula (n = 12) - Semi-elemental diet (n = 13) - Elemental diet (n = 12) Ten subjects received oral CS for 8 weeks. | Similar clinical remission rates were observed after 8 weeks of treatment: 86.5% (32/37) receiving NT vs. 90% (9/10) treated with CS. ARC = −0.04 (exact 95% CI −0.25 to 0.18). Improvement in mucosal inflammation occurred in 64.8% (26/37) of patients on NT and 40% (4/10) of children on CS (p < 0.05). |
| Soo et al. 2013 [45] | Retrospective cohort study | Children with newly diagnosed CD (n = 105). | Children received either EEN (n = 36, mean age 12.9 years) or corticosteroids (n = 69, mean age 11.2 years) as induce remission therapy | Remission rate similar in two groups 88.9% (32/36) in the EEN group vs. 91.3% (63/69) in the CS group (p = 0.73) at 3 months). ARC= −0.02 (exact 95% CI −0.15 to 0.10). Relapse rate (40.6% vs. 28.6%), similar in both treatment groups (p = 0.12) over 12 months). |
| Luo et al. 2015 [46] | Retrospective cohort study | Children with newly diagnosed mild to moderate CD. | Children received either EEN (n = 10; median age 11.6 years) or CS (n = 18; median age 11.1 years) for 8 weeks. | The remission rate in EEN group was significantly higher than that in CS group (90.0% vs. 50.0%, respectively, p < 0.05). |
| Grover et al. 2015 [47] | Retrospective analysis of records | Children with newly diagnosed CD (n = 89) involving ileal, ileocolonic, and colonic sites. | Children received either EEN (n = 43; median age 13 years) or CS (n = 46; median age 11.5 years) as remission induction therapy together with an early use of thiopurines (within 6 months from diagnosis) as maintenance therapy. They were followed up for at least 2 years. | Choice of EEN over CS induction was associated with reduced linear growth failure (7% vs. 26%, p = 0.02), CS dependency (7% vs. 43%, p = 0.002), and improved primary sustained response to IFX (86% vs. 68%, p = 0.02). |
| Novel Nutritional Approaches for Induction of Remission in Pediatric IBD | ||||
|---|---|---|---|---|
| Author/Year | Study Type | Population | Method | Main Findings |
| Gupta et al. 2013 [48] | Retrospective cohort study | Children with active CD (n = 23), mean age 12.8 years. | Enteral nutrition providing 80%–90% of caloric needs, remaining calories from normal diet | Induction of remission achieved in 65% of cases and response in 87% of cases at a mean follow-up of 2 months. |
| Suskind et al. 2014 [49] | Retrospective cohort study | Children and adolescents with active CD (n = 10), age range 7–16 years | SCD as treatment of active CD (either soon after diagnosis, or as second line therapy if steroid dependent or failure of mesalazine treatment). Duration of dietary therapy: 5–30 months. | Symptoms of all patients resolved at a routine clinic visit 3 months after initiating the diet. Laboratory indices and fecal calprotectin either normalized or significantly improved at the follow-up clinic visits. |
| Cohen et al. 2014 [50] | Clinical trial | Children and adolescents with active CD, mean age 13.6 years (n = 9). | SCD for 101% caloric needs, for 12 and 52 weeks. | At both: 12 week and 52-week endpoint s, there was clinical improvement assessed by PCDAI. In 6/10 patients (60%) remission was achieved by week 12. IR = 0.60 (exact 95% CI 0.26 to 0.88). Mucosal healing (Lewis score < 135) was observed in 40% (4/10) of patients at week 12. IR = 0.40 (exact 95% CI 0.12 to 0.74). 80% showed significant mucosal improvement at week 12 when compared to baseline (p = 0.012). IR = 0.80 (exact 95% CI 0.44 to 0.97). |
| Sigall-Boneh et al. 2014 [51] | Clinical trial | Children and young adults with active CD n = 47 (mean age 16.1 ± 5.6 years, children n = 34) | PEN with a CD exclusion diet + 50% polymeric formula for 6 weeks. | Response and remission was obtained in 37 (78.7%) and 33 (70.2%) patients respectively. IR = 0.79 (exact 95% CI 0.64 to 0.89). Remission was obtained in 70% of children and 69% of adults. IR = 0.70 (exact 95% CI 0.55 to 0.83). |
| Nutrition in Maintenance of Disease Remission in Pediatric IBD | ||||
|---|---|---|---|---|
| Author/Year | Study Type | Population | Method | Main Findings |
| PEN | ||||
| Belli et al. 1988 [54] | Clinical trial | Children and adolescents with CD (n = 8) aged 9.8–14.2 years | - 8 children treated with chronic Intermittent ED for 1 month out of 4, over the course of 1 year - 4 children treated with conventional medical treatment | - CD activity index and prednisone intake decreased significantly in patients receiving ED therapy when compared with controls on conventional medical therapy (p < 0.05). |
| Duncan et al. 2014 [55] | Clinical trial | Children and adolescents newly diagnosed CD (n = 59) aged 2.5–16.33 years | Patients newly diagnosed CD who commenced EEN for 8 weeks, than followed up: - 11/59 poor response to EEN, switched to steroids. 48/59 completed 8 weeks with EEN and achieved remission - 15/48 continued MEN, post EEN completion. Duration of MEN ranged 4–14 months (mean 10.8 months) | - Remission rates at 1 year in patients continuing MEN were 60% (9/15), compared to 15% (2/13) in patients taking no treatment (p = 0.001) and 65% (13/20) in patients taking azathioprine (p = 0.14). |
| Wilschanski et al. 1996 [61] | Retrospective cohort study | Children and adolescents (n = 65) aged 7–17 years | After induction of remission of CD with EEN: - Group 1: patients (n = 28) continued nocturnal nasogastric supplementary feeding combined with a normal diet - Group 2: patients (n = 19) stopped nocturnal supplements after the remission | - Higher relapse rate in group 2 vs. group 2 at 6 and 12 months (At 6 months relapse rate of group 2: 78% (15/19) vs. 17.8% (5/28) of group 1, p < 0.02; at 12 months relapse rate of group 2 78.9% (15/19) vs. group 1 42.8% (12/28), p < 0.02). - Mean changes in height velocity was greater for group 1 (2.87 cm/year) compared to group 2 (0.4 cm/year), p =0.057. |
| Obih et al. 2015 [63] | Retrospective cohort study | Children affected by IBD (n = 26), CD (n = 20) or UC (n = 6) aged 1.5–19 years | - Group of patients (n = 26) who followed a SCD for more than 2 weeks (mean duration 9.6 ± 10.1 months). 15/26 patients were on concurrent medication with SCD; 11/26 were not on IBD-related drugs - Children with IBD (n = 10), CD (n = 7), UC (n = 3) who did not follow SCD but only standard medical therapy | - In SCD group PCDAI improved from 32.8 ± 13.2 at baseline to 20.8 ± 16.6 by week 4 ± 2 w and 8.8 ± 8.5 by month 6. - The mean Pediatric Ulcerative Colitis Index (PUCAI) decreased from baseline 28.3 ± 10.3 to 20.0 + 17.3 at week 4 ± 2 w and to 18.3 ± 31.7 at month 6. - Significant improvement of Crohn’s disease activity index, CRP, and calprotectin in SCD group respect to control group (p = 0.03, 0.03, and 0.03, respectively) - lower BMI, height and weight in SCD group than in control (p = 0.01, 0.03, and 0.009, respectively) |
| Curcumin | ||||
| Hanai H et al. 2006 [69] | Randomized double-blind, placebo-controlled trial | Adolescents and adults with quiescent UC aged 13–65 years (n = 89) | - 43 patients received curcumin 2 g/day plus sulfasalazine or mesalazine; - 39 patients received placebo plus sulfasalazine or mesalazine | - Relapse rate at 6 months of therapy was lower for curcumin group compared to placebo group: - 2/43 (4.65%) in curcumin group vs. 8/39 (20.51%) in placebo group, p = 0.049. ARC = −0.16 (exact 95% CI −0.30 to −0.02). - Curcumin improved both clinical activity index (CAI, p = 0.038) and endoscopic index (EI, p = 0.0001). - High tolerability and no serious side effect associated to curcumin |
| Suskind et al. 2013 [71] | Clinical trial | Children and adolescents (n = 11) aged 11–18 years affective by CD (n = 6) or UC (n = 5). | All patients, in addition to their standard IBD therapy, received increasing doses of curcumin, up to 2 g twice daily for 3 weeks | - High tolerability of curcumin without side effects except for increase in gassiness which was consistently reported in two patients. Three patients had lowering of PUCAI/PCDAI scores. - No patients had IBD relapse or worsening of symptoms. |
| n-3 PUFAs | ||||
| Romano et al. 2005 [82] | Double-blind, randomized, placebo-controlled study | Children and adolescents affected by CD (n = 38) in remission, aged 5–16 years and treated for 12 months. | - Group 1 (n = 18): patients treated with 5-ASA (50 mg/kg/day) and omega-3 fatty acids for 12 months. - Group 2 (n = 20): patients treated with 5-ASA (50 mg/kg/day) plus placebo (olive oil in capsules) for 12 months. | Number of patients who relapsed at 12 months was significantly lower in Omega-3 fatty acid group than in patients receiving placebo (relapse rate group 1 11/18 (61%), group 2 19/20 (95%); p < 0.001). ARC −0.34 (exact 95% CI −0.58 to −0.09). |
| Health Benefits of Nutritional Therapy in Pediatric IBD | ||||
|---|---|---|---|---|
| Author/Year | Study Type | Population | Method | Main Findings |
| Azcue et al. 1997 [83] | Clinical trial | Children and adolescents affected by CD (n = 24); malnourished adolescents with anorexia nervosa (n = 19); healthy control subjects (n = 22) | - Group of patients (n = 12) treated with nocturnal enteral nutrition via nasogastric tube for 5–6 weeks, then 1 night a week for 2 months - Group of patients (n = 12) treated with prednisolone - control group (n = 22), healthy subjects - group of malnourished adolescents with anorexia nervosa (n = 19) | - All body compartments and REE increased significantly in enteral nutrition group compared to patients treated with corticosteroids. In enteral nutrition group REE (kcal/day) from 1153 ± 283 at baseline to 1415 ± 535 at 1 month post-treatment; in prednisolone group REE at baseline 1380 ± 308 to 1432 ± 265 at one month post-treatment. For lean body mass (LBM % weight) in enteral nutrition group 86.6 ± 8.9 at baseline to 88.8 + 9.9 at one month post-treatment, in prednisolone group 87.5 ± 9.4 at baseline to 79.1 ± 9.4 at one month post-treatment. - Significant height increase in enteral nutrition group compared with prednisolone group (p < 0.01). |
| Beattie et al. 1998 [86] | Clinical trial | Children and adolescents affected by CD (n = 23) | - Study A: 14 patients treated with EEN for 8 weeks, then gradual reduction of nutritional support over 2 months - Study B: 9 patients treated with intestinal resection | Study A - Significant weight gain for all patients treated with EEN after 8 and 16 weeks, compared to pre-treatment values (weight SDS at baseline= -0.9 (−1.3 to −0.5), weight SDS at week 8 = −0.5 (−0.9 to 0), at 16 weeks weight SDS = −0.6 (−1.1 to 0) (p < 0.05) - Significant increase of median IGF-1 and IGFBP-3 at 2, 8, and 16 weeks in EEN group compared to pre-treatment values (p < 0.01) Study B - No significant changes in auxological data, IGF-1 and IGFBP-3 in patients who had surgical resection compared to pre-treatment values |
| Wilschanski et al. 1996 [61] | Retrospective cohort study | Children and adolescents (n = 65) aged 7–17 years | After induction of remission of CD with EEN: - Group 1: patients (n = 28) continued nocturnal nasogastric supplementary feeding combined with a normal diet - Group 2: patients (n = 19) stopped nocturnal supplements after the remission | - Mean changes in height velocity was greater for group 1 (2.87 cm/year) compared to group 2 (0.4 cm/year), p = 0.057. |
| Belli et al. 1988 [54] | Clinical trial | Children and adolescents with CD (n = 8) aged 9.8–14.2 years | - 8 children treated with chronic intermittent enteral ED for 1 month out of 4, over the course of 1 year - 4 children treated with conventional medical treatment | - Significant height and weight gains in the ED group vs. controls. Weight gain for ED group 6.9 ± 1.5 kg; 209.8% ± 41.9%; weight gain for control group −0.9 + 1.6 kg; −9.8% ± 52.6% (p < 0.01). Height changes in ED group 7.0 + 0.8 cm; 126.0% ± 11.8% of ideal predicted. Height change in control group 1.7 + 0.8 cm; 28.7% ± 13.1% (p < 0.01). |
| Berni Canani et al. 2006 [44] | Retrospective study | Children and adolescents affected by active CD (n = 47) | Children received nutritional therapy (NT) for 8 weeks as - Polymeric formula (n = 12) - Semi-elemental diet (n = 13) - Elemental diet (n = 12) Ten subjects received oral CS for 8 weeks. | - Significant improvement of serum albumin and iron levels in NT compared to CS group. In NT group elemental: albumin at baseline 13.14 ± 0.47 to 3.98 ± 0.36 at 8 weeks, p < 0.001; NT group semi-elemental: albumin at baseline 3.13 + 0.40 to 3.88 + 0.26 at 8 weeks, p < 0.001; NT group polymeric: albumin at baseline 3.09 + 0.39 to 3.86 + 0.38 at 8 weeks, p < 0.001)). In CS group: albumin at baseline 3.37 ± 0.24 to 3.40 ± 0.22 after 8 weeks, p = 0.28). In NT group elemental: iron at baseline 31.25 ± 20.4 to 72.17 ± 20.4 at 8 weeks, p = 0.001; NT group semi-elemental: iron at baseline 29.46 + 23.7 to 66.69 + 19.8 at 8 weeks, p = 0.002; NT group polymeric: iron at baseline 32.58 + 24.0 to 69.25 + 29.6 at 8 weeks, p = 0.004)). In CS group: iron at baseline 20.80 ± 15.5 to 35.80 ± 16.0 after 8 weeks, p = 0.01). Linear growth recovery was superior in nutritional group compared to CS group (p < 0.05). |
| Motil et al. 1982 [87] | Clinical trial | Adolescents affected by CD | - 6 patients affected by CD received nutritional supplements for 7 months - 5 healthy control subjects | Increase of linear and ponderal growth velocities in patients treated with nutritional support (Height gain cm/month pre-supplements 0.10 ± 0.08, post-supplements 0.50 + 0.16; weight gain kg/month pre-supplements 0.21 ± 0.09, post-supplements 1.22 ± 0.25). Achievement of weight and height gain similar to control group levels after the 7 months treatment with nutritional supplements (height gain cm/month 0.38 ± 0.12, weight gain kg/month 0.40 + 0.17). |
| O’Morain et al. 1983 [88] | Clinical trial | Children and adolescents affected by CD (n = 15) aged 6–20 years | 14 patients received ED as the main energy source for 4 weeks; 1 received corticosteroids. | Improvement of nutritional status, weight, and height gain in children receiving ED. |
| Whitten et al. 2010 [94] | Clinical trial | Children newly diagnosed CD (n = 23) compared to a healthy control group (n = 20) | Children newly diagnosed with CD received 8 weeks EEN for induction of remission | Normalization of serum markers of bone turnover after EEN therapy. CTX levels at diagnosis 2.967 ± 0.881 ng/mL and after EEN 2.260 ± 0.547 ng/mL, p = 0.002. BAP levels at diagnosis 51.24 ± 31.31 microg/L and after EEN 64.82 ± 30.51 microg/L, p = 0.02. |
| Polk et al. 1992 [89] | Clinical trial | Adolescents affected by CD (n = 6) | All patients received enteral nutrition via nasogastric tube during night 1 out of 4 months for 1 year. Then the patients received a 2-week exclusion diet and a 2-week low-residue diet for 2 months, before re-starting a normal diet. | Significant increase of weight, height, IGF-1, and albumin; decrease of steroid use and disease activity compared to pretreatment values |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penagini, F.; Dilillo, D.; Borsani, B.; Cococcioni, L.; Galli, E.; Bedogni, G.; Zuin, G.; Zuccotti, G.V. Nutrition in Pediatric Inflammatory Bowel Disease: From Etiology to Treatment. A Systematic Review. Nutrients 2016, 8, 334. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8060334
Penagini F, Dilillo D, Borsani B, Cococcioni L, Galli E, Bedogni G, Zuin G, Zuccotti GV. Nutrition in Pediatric Inflammatory Bowel Disease: From Etiology to Treatment. A Systematic Review. Nutrients. 2016; 8(6):334. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8060334
Chicago/Turabian StylePenagini, Francesca, Dario Dilillo, Barbara Borsani, Lucia Cococcioni, Erica Galli, Giorgio Bedogni, Giovanna Zuin, and Gian Vincenzo Zuccotti. 2016. "Nutrition in Pediatric Inflammatory Bowel Disease: From Etiology to Treatment. A Systematic Review" Nutrients 8, no. 6: 334. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8060334