Water and Beverage Consumption among Children Aged 4–13 Years in Lebanon: Findings from a National Cross-Sectional Study


Abstract
:1. Introduction
2. Methods
2.1. Study Population and Sampling Framework
2.2. Data Collection
2.3. Dietary Intake Assessment and Interpretation
2.4. Water and Energy Intake and Beverage Classifications
2.5. Statistical Analysis
3. Results
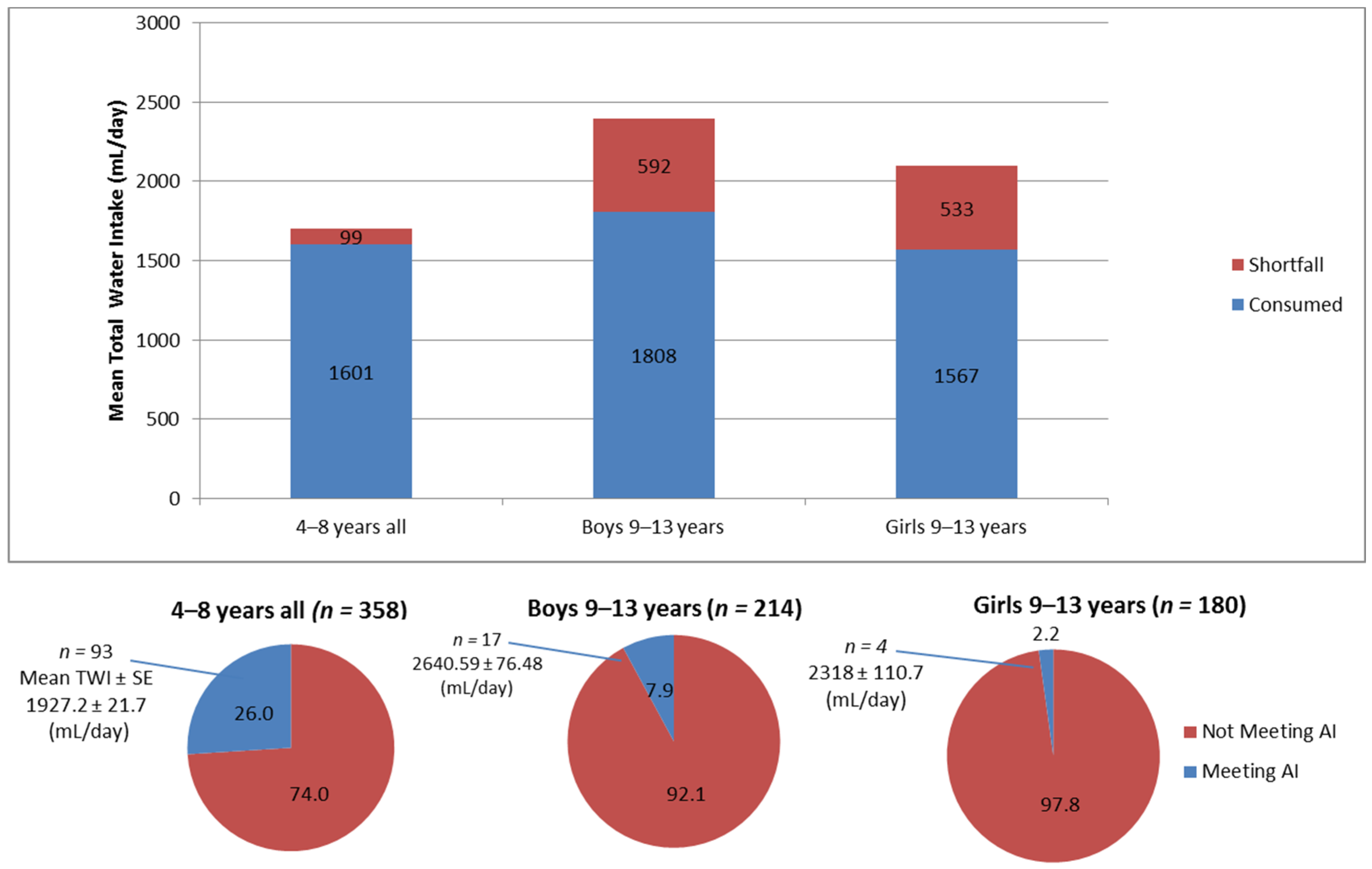
3.1. Total Water Intakes among Study Sample in Relation to Recommended Intakes
3.2. Water Consumption According to Socioeconomic, Physical Activity and Anthropometric Characteristics
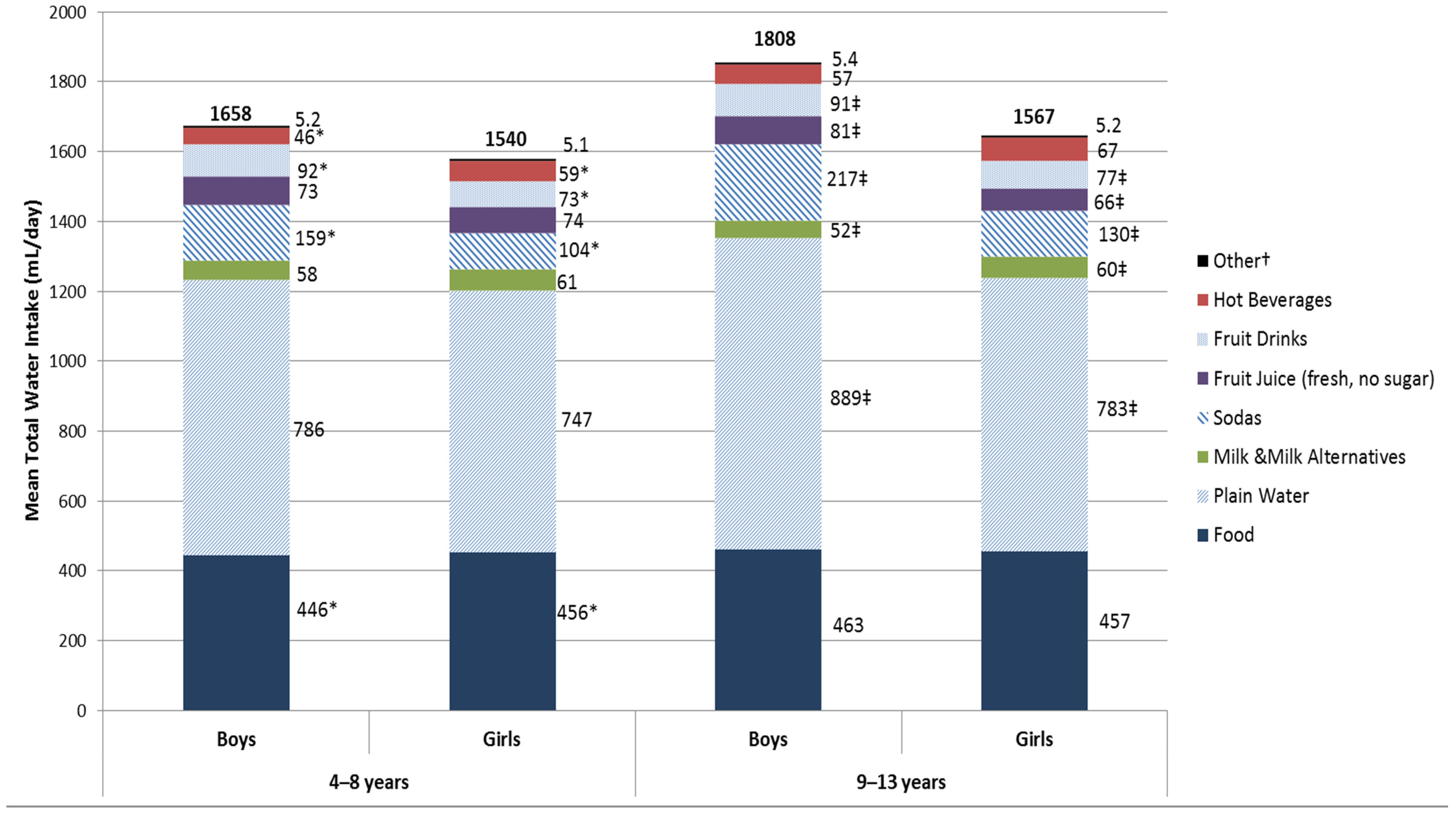
3.3. Patterns of Water Intake from Food and Various Beverage Types by Age and Gender
3.4. Water Intake from Specific Beverages by Socioeconomic, Anthropometric and Physical Activity Characteristics
3.5. Contribution of Various Beverage Sources to Total Daily Energy Intake
3.6. Comparison of Water Intakes amongst Children in Lebanon with Other Countries
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R. Impact of mild dehydration on wellness and on exercise performance. Eur. J. Clin. Nutr. 2003, 57, S19–S23. [Google Scholar] [CrossRef] [PubMed]
- Fadda, R.; Rapinett, G.; Grathwohl, D.; Parisi, M.; Fanari, R.; Calò, C.M.; Schmitt, J. Effects of drinking supplementary water at school on cognitive performance in children. Appetite 2012, 59, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.S.; Rapinett, G.; Glaser, N.S.; Ghetti, S. Hydration status moderates the effects of drinking water on children’s cognitive performance. Appetite 2015, 95, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Manz, F. Hydration in children. J. Am. Coll. Nutr. 2007, 26, 562S–569S. [Google Scholar] [CrossRef] [PubMed]
- Manz, F.; Wentz, A.; Sichert-Hellert, W. The most essential nutrient: Defining the adequate intake of water. J. Pediatr. 2002, 141, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM). Dietary Reference Intakes Tables and Applications. Available online: http://www.nationalacademies.org/hmd/Activities/Nutrition/SummaryDRIs/DRI-Tables.aspx (accessed on 8 July 2016).
- European Food Safety Authority (EFSA). Scientific opinion on dietary reference values for water. Efsa panel on dietetic products, nutrition, and allergies. ESFA J. 2010, 8. [Google Scholar] [CrossRef] [Green Version]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among children age 4–13 years in the united states: Analyses of 2005–2010 nhanes data. Nutr. J. 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Piernas, C.; Barquera, S.; Popkin, B.M. Current patterns of water and beverage consumption among mexican children and adolescents aged 1–18 years: Analysis of the mexican national health and nutrition survey 2012. Public Health Nutr. 2014, 17, 2166–2175. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D.; Constant, F.; Gardner, C.D.; Popkin, B.M. Replacing sweetened caloric beverages with drinking water is associated with lower energy intake. Obesity 2007, 15, 3013–3022. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D.; Constant, F.; Popkin, B.M.; Gardner, C.D. Drinking water is associated with weight loss in overweight dieting women independent of diet and activity. Obesity 2008, 16, 2481–2488. [Google Scholar] [CrossRef] [PubMed]
- Daniels, M.C.; Popkin, B.M. Impact of water intake on energy intake and weight status: A systematic review. Nutr. Rev. 2010, 68, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D. Drinking water and weight management. Nutr. Today 2010, 45, S7–S12. [Google Scholar] [CrossRef]
- Park, S.; Blanck, H.M.; Sherry, B.; Brener, N.; O’Toole, T. Factors associated with low water intake among us high school students—National youth physical activity and nutrition study, 2010. J. Am. Diet. Assoc. 2012, 112, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Vieux, F.; Maillot, M.; Constant, F.; Drewnowski, A. Water and beverage consumption among children aged 4–13 years in France: Analyses of INCA 2 (etude individuelle nationale des consommations alimentaires 2006–2007) data. Public Health Nutr. 2016, 19, 2305–2314. [Google Scholar] [CrossRef] [PubMed]
- Iglesia, I.; Santaliestra-Pasías, A.; Bel-Serrat, S.; Sadalla-Collese, T.; Miguel-Berges, M.; Moreno, L. Fluid consumption, total water intake and first morning urine osmolality in spanish adolescents from zaragoza: Data from the HELENA study. Eur. J. Clin. Nutr. 2015, 70, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Akpata, E.S.; Behbehani, J.; Akbar, J.; Thalib, L.; Mojiminiyi, O. Fluoride intake from fluids and urinary fluoride excretion by young children in kuwait: A non-fluoridated community. Community Dent. Oral. Epidemiol. 2014, 42, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Bello, L.; Al-hammad, N. Pattern of fluid consumption in a sample of saudi arabian adolescents aged 12–13 years. Int. J. Paediat. Dent. 2006, 16, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Hwalla, N.; Itani, L.; Karam, S.; Sibai, A.M.; Nasreddine, L. A western dietary pattern is associated with overweight and obesity in a national sample of lebanese adolescents (13–19 years): A cross-sectional study. Br. J. Nutr. 2015, 114, 1909–1919. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Naja, F.; Akl, C.; Chamieh, M.C.; Karam, S.; Sibai, A.-M.; Hwalla, N. Dietary, lifestyle and socio-economic correlates of overweight, obesity and central adiposity in lebanese children and adolescents. Nutrients 2014, 6, 1038–1062. [Google Scholar] [CrossRef] [PubMed]
- Central Administration of Statistics (CAS) Lebanon. Population Characteristics in 2007. Available online: http://www.cas.gov.lb/index.php/demographic-and-social-en/population-en (accessed on 11 July 2016).
- Melki, I.S. Household crowding index: A correlate of socioeconomic status and inter-pregnancy spacing in an urban setting. J. Epidemiol. Community Health 2004, 58, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Goodyear, R.F.A.; Hay, J. Finding the crowding index that works best for new zealand: Applying different crowding indexes to census of population and dwellings data for 1986–2006. Statistics N. Zeal. 2012, 4, 1–50. [Google Scholar]
- Naja, F.; Nasreddine, L.; Itani, L.; Chamieh, M.C.; Adra, N.; Sibai, A.M.; Hwalla, N. Dietary patterns and their association with obesity and sociodemographic factors in a national sample of lebanese adults. Public Health Nutr. 2011, 14, 1570–1578. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Nasreddine, L.; Itani, L.; Dimassi, H.; Sibai, A.M.; Hwalla, N. Dietary patterns in cardiovascular diseases prevention and management: Review of the evidence and recommendations for primary care physicians in Lebanon. J. Med. Liban 2014, 62, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Maffeis, C.; Banzato, C.; Talamini, G.; Obesity Study Group of the Italian. Waist-to-height ratio, a useful index to identify high metabolic risk in overweight children. J. Pediatr. 2008, 152, 207–213. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, H.D.; Ashwell, M. A study of central fatness using waist-to-height ratios in UK children and adolescents over two decades supports the simple message—‘Keep your waist circumference to less than half your height’. Int. J. Obes. 2006, 30, 988–992. [Google Scholar] [CrossRef] [PubMed]
- Corder, K.; van Sluijs, E.M.; Wright, A.; Whincup, P.; Wareham, N.J.; Ekelund, U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report? Am. J. Clin. Nutr. 2009, 89, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Coledam, D.H.C.; Ferraiol, P.F.; Júnior, R.P.; Ribeiro, E.A.G.; Ferreira, M.A.C.; de Oliveira, A.R. Agreement between two cutoff points for physical activity and associated factors in young individuals. Rev. Paul. Pediatr. (Engl. Ed.) 2014, 32, 215–222. [Google Scholar]
- United States Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Available online: https://health.gov/paguidelines/pdf/paguide.pdf (accessed on 11 July 2016).
- Moghames, P.; Hammami, N.; Hwalla, N.; Yazbeck, N.; Shoaib, H.; Nasreddine, L.; Naja, F. Validity and reliability of a food frequency questionnaire to estimate dietary intake among Lebanese children. Nutr. J. 2016, 15. [Google Scholar] [CrossRef] [PubMed]
- Posner, B.M.; Smigelski, C.; Duggal, A.; Morgan, J.; Cobb, J.; Cupples, L. Validation of two-dimensional models for estimation of portion size in nutrition research. J. Am. Diet. Assoc. 1992, 92, 738–741. [Google Scholar] [PubMed]
- Naja, F.; Hwalla, N.; Itani, L.; Salem, M.; Azar, S.T.; Zeidan, M.N.; Nasreddine, L. Dietary patterns and odds of type 2 diabetes in Beirut, Lebanon: A case–control study. Nutr. Metab. 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Agriculture (USDA). Usda Food Composition Database. Available online: https://ndb.nal.usda.gov/ (accessed on 11 July 2016).
- Pellett, P.L.; Shadarevian, S. Food Composition Tables for Use in the Middle East; American University of Beirut: Beirut, Lebanon, 1970. [Google Scholar]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among adults in the United States: Cross-sectional study using data from NHANES 2005–2010. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V.L.; Quann, E.E. National trends in beverage consumption in children from birth to 5 years: Analysis of NHANES across three decades. Nutr. J. 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- Collison, K.S.; Zaidi, M.Z.; Subhani, S.N.; Al-Rubeaan, K.; Shoukri, M.; Al-Mohanna, F.A. Sugar-sweetened carbonated beverage consumption correlates with BMI, waist circumference, and poor dietary choices in school children. BMC Public Health 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D. Socioeconomic gradient in consumption of whole fruit and 100% fruit juice among US children and adults. Nutr. J. 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Sayegh, A.; Dini, E.; Holt, R.; Bedi, R. Food and drink consumption, sociodemographic factors and dental caries in 4–5-year-old children in Amman, Jordan. Br. Dent. J. 2002, 193, 37–42. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.M.; Yang, S.-J.; Nicklas, T.A. Beverage intake among preschool children and its effect on weight status. Pediatrics 2006, 118, e1010–e1018. [Google Scholar] [CrossRef] [PubMed]
- Oza-Frank, R.; Zavodny, M.; Cunningham, S.A. Beverage displacement between elementary and middle school, 2004–2007. J. Am. Diet. Assoc. 2012, 112, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.I.; Ng, S.W.; Zaghloul, S.; Harrison, G.G.; Qazaq, H.S.; El Sadig, M.; Yeatts, K. High proportion of 6 to 18-year-old children and adolescents in the United Arab Emirates are not meeting dietary recommendations. Nutr. Res. 2013, 33, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Senterre, C.; Dramaix, M.; Thiébaut, I. Fluid intake survey among schoolchildren in Belgium. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- British Nutrition Foundation. Hydration for Children. Available online: https://www.nutrition.org.uk/healthyliving/hydration/hydration-for children.html (accessed on 20 July 2016).
- Bar-Or, O.; Dotan, R.; Inbar, O.; Rotshtein, A.; Zonder, H. Voluntary hypohydration in 10- to 12-year-old boys. J. Appl. Physiol. 1980, 48, 104–108. [Google Scholar] [PubMed]
- Benton, D.; Braun, H.; Cobo, J.; Edmonds, C.; Elmadfa, I.; El-Sharkawy, A.; Feehally, J.; Gellert, R.; Holdsworth, J.; Kapsokefalou, M. Executive summary and conclusions from the European hydration institute expert conference on human hydration, health, and performance. Nutr. Rev. 2015, 73, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Dubuisson, C.; Dufour, A.; Touvier, M.; Calamassi-Tran, G.; Maire, B.; Volatier, J.-L.; Lafay, L. Trends in food intake in French children from 1999 to 2007: Results from the INCA (étude individuelle nationale des consommations alimentaires) dietary surveys. Br. J. Nutr. 2010, 103, 585–601. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Environment/LEDO. Lebanon State of the Environment Report; 2001; pp. 109–129. Available online: http://www.moe.gov.lb/ledo/soer2001pdf/preface.pdf (accessed on 22 July 2016).
- Vereecken, C.; Maes, L. Young children’s dietary habits and associations with the mothers’ nutritional knowledge and attitudes. Appetite 2010, 54, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Patrick, H.; Nicklas, T.A. A review of family and social determinants of children’s eating patterns and diet quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef] [PubMed]
- De Coen, V.; Vansteelandt, S.; Maes, L.; Huybrechts, I.; De Bourdeaudhuij, I.; Vereecken, C. Parental socioeconomic status and soft drink consumption of the child. The mediating proportion of parenting practices. Appetite 2012, 59, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Hwalla, N.; Itani, L.; Baalbaki, S.; Sibai, A.; Nasreddine, L. A novel mediterranean diet index from lebanon: Comparison with Europe. Eur. J. Nutr. 2015, 54, 1229–1243. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Naja, F.; Chamieh, M.C.; Adra, N.; Sibai, A.-M.; Hwalla, N. Trends in overweight and obesity in Lebanon: Evidence from two national cross-sectional surveys (1997 and 2009). BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- NIH Consensus Panel. Nih consensus development on optimal calcium intake. J. Am. Med. Assoc. 1994, 272, 1942–1948. [Google Scholar]
- Rampersaud, G.C.; Bailey, L.B.; Kauwell, G.P. National survey beverage consumption data for children and adolescents indicate the need to encourage a shift toward more nutritive beverages. J. Am. Diet. Assoc. 2003, 103, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.J.; Popkin, B.M. Changes in beverage intake between 1977 and 2001. Am. J. Prev. Med. 2004, 27, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; Garnett, S.P.; Cowell, C.T.; Campbell, K.; Cabrera, G.; Baur, L.A. Soft drink consumption and excess weight gain in australian school students: Results from the nepean study. Int. J. Obes. 2006, 30, 1091–1093. [Google Scholar] [CrossRef] [PubMed]
- Must, A.; Barish, E.; Bandini, L. Modifiable risk factors in relation to changes in BMI and fatness: What have we learned from prospective studies of school-aged children&quest. Int. J. Obes. 2009, 33, 705–715. [Google Scholar]
- Abi, H.G.; Lahham, S.N.; Afifi, R. Jarrib Baleha—A pilot nutrition intervention to increase water intake and decrease soft drink consumption among school children in Beirut. J. Med. Liban 2010, 59, 55–64. [Google Scholar]



{kind=link}
{kind=link}
| Total Mean ± SE or n (%) | TWI from Foods and Beverages (mL/Day) | Water Intakes from All Beverages (mL/Day) | ||
|---|---|---|---|---|
| Plain Water (Bottled and Tap) (mL/Day) | Beverages (Excluding Plain Water) (mL/Day) | |||
| Mean ± SE | ||||
| Age | 9.07 ± 0.10 | |||
| 4–8 years | 358 (47.6) | 1600.63 ± 12.93 a | 767.32 ± 11.22 a | 376.21 ± 7.95 a |
| 9–13 years | 394 (52.4) | 1697.68 ± 16.55 b | 840.49 ± 13.39 b | 401.13 ± 9.24 b |
| Gender | ||||
| Boys | 397 (52.8) | 1738.77 ± 17.72 a | 841.58 ± 13.50 a | 440.54 ± 9.91 a |
| Girls | 355 (47.2) | 1553.87 ± 8.81 b | 765.48 ± 10.97 b | 331.92 ± 5.47 b |
| Father’s educational level | ||||
| Intermediate or less | 435 (58.2) | 1646.44 ± 13.60 a | 804.73 ± 11.53 a | 396.18 ± 7.49 a |
| High school/technical diploma | 203 (27.2) | 1660.32 ± 22.73 a | 812.81 ± 18.60 a | 378.70 ± 14.37 a |
| University Degree or more | 109 (14.6) | 1645.37 ± 27.34 a | 793.63 ± 21.15 a | 372.21 ± 12.91 a |
| Mother’s educational level | ||||
| Intermediate or less | 363 (48.3) | 1632.03 ± 14.98 a | 790.21 ± 12.32 a | 391.70 ± 9.36 a |
| High school/technical diploma | 227 (30.2) | 1674.59 ± 20.87 a | 830.57 ± 17.45 a | 393.16 ± 10.89 a |
| University Degree or more | 162 (21.5) | 1662.68 ± 22.69 a | 805.37 ± 18.64 a | 378.35 ± 12.04 a |
| Father’s employment status | ||||
| Unemployed | 32 (4.3) | 1669.58 ± 62.48 a | 794.76 ± 60.61 a | 436.67 ± 33.85 a |
| Employed | 711 (95.7) | 1651.28 ± 11.01 a | 807.07 ± 8.99 a | 386.36 ± 6.28 a |
| Mother’s employment status | 743 (100) | |||
| Unemployed | 556 (74.0) | 1644.78 ± 12.56 a | 802.36 ± 10.43 a | 388.29 ± 7.22 a |
| Employed | 195 (26.0) | 1669.90 ± 21.04 a | 814.06 ± 17.21 a | 391.98 ± 11.88 a |
| Monthly family income (LBP) | ||||
| <1,000,000 | 310 (41.8) | 1636.68 ± 16.11 a | 807.52 ± 14.25 a | 391.02 ± 8.91 a |
| 1,000,000–1,999,999 | 279 (37.6) | 1643.13 ± 16.75 a | 790.03 ± 14.02 a | 386.28 ± 9.05 a |
| ≥2,000,000 | 153 (20.6) | 1701.01 ± 27.93 a | 835.94 ± 20.22 a | 391.31 ± 17.74 a |
| Crowding index (person/room) | 1.62 ± 0.03 | |||
| <2 | 534 (71.2) | 1654.31 ± 13.01 a | 808.22 ± 10.58 a | 388.52 ± 7.50 a |
| ≥2 | 216 (28.8) | 1644.11 ± 19.30 a | 799.48 ± 16.74 a | 390.62 ± 10.72 a |
| BMI z-score | 0.92 ± 0.06 | |||
| BMI status | ||||
| Normal weight | 443 (58.9) | 1640.08 ± 13.96 a | 787.19 ± 10.82 a | 390.21 ± 8.49 a |
| Overweight | 152 (20.2) | 1657.23 ± 23.68 a | 824.72 ± 20.89 a | 376.22 ± 12.41 a |
| Obese | 157 (20.9) | 1678.07 ± 24.21 a | 839.29 ± 21.70 a | 399.24 ± 12.33 a |
| Waist Circumference (cm) | 64.11 ± 0.46 | |||
| Waist to height ratio (WHtR) | 0.48 ± 0.00 | |||
| <0.5 | 489 (65.4) | 1660.89 ± 14.08 a | 807.59 ± 242.03 a | 392.54 ± 8.17 a |
| ≥0.5 | 259 (34.6) | 1631.77 ± 260.18 a | 803.33 ± 250.37 a | 382.24 ± 144.39 a |
| Level of physical activity | ||||
| Active | 434 (57.7) | 1676.47 ± 13.94 a | 817.52 ± 12.16 a | 404.27 ± 7.39 a |
| Inactive | 318 (42.3) | 1617.37 ± 16.78 b | 789.46 ± 12.95 a | 368.80 ± 10.41 b |
| Total 752 | 4–8 Years 183 (46.1%) | 9–13 Years 214 (53.9%) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SE | % of TWI | Mean ± SE | % of TWI | Mean ± SE | % of TWI † | ||
| Total water intake from all food and beverages | 1651.48 ± 10.77 | 100 | 1600.63 ± 12.93 a | 100 | 1697.68 ± 16.55 b | 100 | p < 0.001 |
| Water intake from food only | 455.79 ± 1.87 | 28.09 | 450.69 ± 2.33 a | 28.54 | 460.41 ± 2.86 b | 27.68 ** | p = 0.009 |
| Plain Water | 805.66 ± 8.91 | 48.36 | 767.32 ± 11.22 a | 47.61 | 840.49 ± 13.39 b | 49.05 * | p < 0.001 |
| Bottled water | 685.54 ± 6.98 | 41.75 | 671.51 ± 8.67 a | 42.15 | 698.29 ± 10.72 b | 41.39 | p = 0.053 |
| Tap water | 96.36 ± 6.75 | 5.62 | 81.26 ± 8.67 a | 4.89 | 110.08 ± 10.15 b | 6.29 | p = 0.031 |
| Water intake from all beverages (excluding plain water) | 1194.92 ± 8.91 | 71.60 | 1143.53 ± 14.17 a | 70.85 | 1241.62 ± 17.47 b | 72.28 | p < 0.001 |
| Milk and milk alternatives | 57.72 ± 0.90 | 3.54 | 59.59 ± 1.32 a | 3.75 | 56.02 ± 1.22 b | 3.34 ** | p = 0.048 |
| Milk | 25.62 ± 0.81 | 1.56 | 26.75 ± 1.20 a | 1.67 | 24.59 ± 1.09 a | 1.45 * | p = 0.182 |
| Milk Alternatives ǂ | 32.10 ± 0.32 | 1.98 | 32.84 ± 0.44 a | 2.08 | 31.43 ± 0.45 b | 1.89 ** | p = 0.026 |
| Sodas | 155.68 ± 5.35 | 9.25 | 132.14 ± 7.15 a | 8.09 | 177.06 ± 7.74 b | 10.31 ** | p < 0.001 |
| Regular | 142.61 ± 4.81 | 8.50 | 114.04 ± 5.15 a | 7.06 | 168.68 ± 7.66 b | 9.80 ** | p < 0.001 |
| Diet | 13.01 ± 2.83 | 0.75 | 18.10 ± 5.50 a | 1.03 | 8.38 ± 2.05 a | 0.50 | p = 0.098 |
| Fruit Juice | 160.77 ± 1.39 | 9.91 | 163.20 ± 2.21 a | 10.33 | 158.55 ± 1.72 a | 9.53 ** | p = 0.094 |
| Fresh Fruit Juice (100% Natural) | 69.15 ± 0.20 | 4.29 | 69.02 ± 0.28 a | 4.39 | 69.23 ± 0.28 a | 4.19 ** | p = 0.603 |
| Bottled Fruit Juice (with sugar)/Fruit Drink | 85.18 ± 0.78 | 5.25 | 85.90 ± 1.11 a | 5.43 | 84.52 ± 1.09 a | 5.08 ** | p = 0.379 |
| Bottled Fruit Juice (without sugar) | 6.46 ± 1.18 | 0.38 | 8.28 ± 2.07 a | 0.51 | 4.80 ± 1.25 a | 0.27 | p = 0.152 |
| Vegetable Juice | 2.89 ± 0.91 | 0.17 | 4.33 ± 1.80 a | 0.27 | 1.58 ± 0.60 a | 0.09 | p = 0.149 |
| Fresh Vegetable Juice | 1.26 ± 0.31 | 0.07 | 1.65 ± 0.52 a | 0.10 | 0.91 ± 0.35 a | 0.05 | p = 0.232 |
| Bottled Vegetable Juice | 1.63 ± 0.86 | 0.10 | 2.67 ± 1.73 a | 0.16 | 0.68 ± 0.50 a | 0.04 | p = 0.268 |
| Hot Beverages | 57.06 ± 2.04 | 3.44 | 52.14 ± 2.80 a | 3.26 | 61.53 ± 2.93 b | 3.61 | p = 0.021 |
| Sports and Energy Drinks | 1.84 ± 0.62 | 0.10 | 0.81 ± 0.53 a | 0.05 | 2.77 ± 1.07 a | 0.14 | p = 0.103 |
| Sports Drinks | 0.85 ± 0.49 | 0.05 | 0.47 ± 0.47 a | 0.03 | 1.20 ± 0.84 a | 0.06 | p = 0.463 |
| Energy Drinks | 0.99 ± 0.32 | 0.05 | 0.34 ± 0.24 a | 0.02 | 1.58 ± 0.57 b | 0.08 | p = 0.047 |
| Alcoholic beverages | 0.51 ± 0.21 | 0.03 | 0.02 ± 0.02 a | 0.00 | 0.95 ± 0.40 b | 0.06 * | p = 0.019 |
| Bottled Water | Tap Water | Milk and Milk Alternatives | Regular Soft Drinks | Fresh Fruit Juice | Fresh Veg. Juice | Energy Drinks | |
|---|---|---|---|---|---|---|---|
| 685.54 ± 6.98 | 96.36 ± 6.75 | 57.72 ± 0.90 | 142.67 ± 4.81 | 69.13 ± 0.20 | 1.26 ± 0.31 | 0.99 ± 0.32 | |
| Father’s educational level | |||||||
| Intermediate or less | 670.04 ± 9.09 a | 115.67 ± 9.65 a | 56.48 ± 1.18 a | 155.95 ± 6.20 a | 69.10 ± 0.26 a | 1.41 ± 0.47 a | 0.92 ± 0.40 a |
| High school/technical diploma | 699.88 ± 14.23 a,b | 82.80 ± 12.37 a,b | 58.98 ± 1.68 a | 125.42 ± 9.16 b | 68.95 ± 0.42 a | 1.25 ± 0.48 a | 1.63 ± 0.83 a |
| University Degree or more | 722.11 ± 16.45 b | 41.01 ± 9.12 b | 60.30 ± 2.53 a | 106.77 ± 9.95 b,c | 69.53 ± 0.50 a | 0.76 ± 0.44 a | 0.11 ± 0.08 a |
| Mother’s educational level | |||||||
| Intermediate or less | 653.90 ± 9.453 a | 122.48 ± 10.76 a | 53.28 ± 1.00 a | 168.61 ± 8.00 a | 68.87 ± 0.30 a | 0.92 ± 0.33 a | 1.95 ± 0.66 a |
| High school/technical diploma | 714.72 ± 13.68 b | 82.44 ± 11.64 b | 62.03 ± 1.95 b | 125.89 ± 7.36 b | 69.31 ± 0.34 a | 1.06 ± 0.47 a | 0.04 ± 0.03 b |
| University Degree or more | 715.57 ± 14.52 b,c | 57.33 ± 10.77 b,c | 61.64 ± 2.14 b,c | 108.04 ± 7.19 b,c | 69.48 ± 0.44 a | 2.30 ± 1.02 a | 0.13 ± 0.10 a,b |
| Monthly family income (LBP) | |||||||
| ≤1,000,000 | 647.53 ± 10.90 a | 144.24 ± 12.73 a | 54.55 ± 1.21 a | 162.71 ± 8.15 a | 68.80 ± 0.31 a | 0.87 ± 0.47 a | 0.79 ± 0.34 a |
| 1,000,000–1,999,999 | 698.20 ± 10.88 b | 69.43 ± 9.15 b | 59.39 ± 1.65 b | 135.02 ± 6.56 b | 69.41 ± 0.31 a | 1.32 ± 0.43 a | 0.76 ± 0.42 a |
| ≥2,000,000 | 743.9447 ± 15.53 c | 48.09 ± 9.49 b,c | 59.72 ± 1.92 a,b | 116.72 ± 11.21 b,c | 69.48 ± 0.52 a | 2.04 ± 0.87 a | 1.86 ± 1.20 a |
| Crowding index (person/room) | |||||||
| <2 | 696.62 ± 8.40 a | 85.66 ± 7.30 a | 58.71 ± 1.09 a | 137.07 ± 5.79 a | 69.52 ± 0.24 a | 1.55 ± 0.42 a | 0.87 ± 0.37 a |
| ≥2 | 657.64 ± 12.49 b | 123.56 ± 14.89 b | 54.91 ± 1.55 a | 156.28 ± 8.56 a | 68.20 ± 0.35 b | 0.56 ± 0.23 b | 1.29 ± 0.63 a |
| Level of physical activity | |||||||
| Active | 691.14 ± 9.42 a | 99.56 ± 8.82 a | 58.13 ± 1.21 a | 155.08 ± 6.43 a | 69.85 ± 0.25 a | 1.41 ± 0.46 a | 1.44 ± 0.53 a |
| Inactive | 677.91 ± 10.37 a | 91.98 ± 10.48 a | 57.16 ± 1.35 a | 125.72 ± 7.14 b | 68.15 ± 0.32 b | 1.10 ± 0.36 a | 0.37 ± 0.23 a |
| Total | 4–8 Years 183 (46.1%) | 9–13 Years 214 (53.9%) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Number of Consumers n (%) | Mean ± SE | % of Total EI | Mean ± SE | % of Total EI | Mean ± SE | % of Total EI † | ||
| Total energy intake from all foods and beverages | 752 (100) | 1924.66 ± 7.45 | 100 | 1899.34 ± 8.80 a | 100 | 1947.67 ± 11.66 b | 100 | 0.001 |
| Energy intake from foods only | 752 (100) | 1741.56 ± 6.34 | 90.54 | 1720.68 ± 7.71 a | 90.62 | 1760.54 ± 9.77 b | 90.47 | 0.001 |
| Energy intake from caloric beverages | 752 (100) | 181.16 ± 1.49 | 9.36 | 176.76 ± 1.76 a | 9.27 | 185.17 ± 2.33 b | 9.44 | 0.004 |
| Milk and milk alternatives | 752 (100) | 56.15 ± 1.24 | 2.92 | 58.28 ± 1.94 a | 3.07 | 54.20 ± 1.57 a | 2.79 * | 0.080 |
| Milk | 752 (100) | 32.25 ± 1.18 | 1.67 | 34.45 ± 1.88 a | 1.80 | 30.25 ± 1.46 a | 1.55 * | 0.079 |
| Milk alternatives | 752 (100) | 23.90 ± 0.23 | 1.25 | 23.84 ± 0.29 a | 1.26 | 23.95 ± 0.35 a | 1.24 | 0.972 |
| Sodas | 752 (100) | 60.22 ± 1.98 | 3.06 | 48.54 ± 2.12 a | 2.51 | 70.83 ± 3.16 b | 3.56 ** | <0.001 |
| Regular | 752 (100) | 59.96 ± 1.98 | 3.05 | 48.18 ± 2.13 a | 2.49 | 70.67 ± 3.16 b | 3.55 ** | <0.001 |
| Diet | 68 (9.04) | 0.26 ± 0.06 | 0.01 | 0.36 ± 0.11 a | 0.02 | 0.17 ± 0.04 a | 0.01 | 0.098 |
| Fruit Juice | 752 (100) | 71.34 ± 0.82 | 3.71 | 73.01 ± 1.30 a | 3.85 | 69.82 ± 1.02 a | 3.58 ** | 0.052 |
| Fresh fruit juice (100% natural) | 752 (100) | 15.24 ± 0.14 | 0.80 | 15.48 ± 0.22 a | 0.82 | 15.02 ± 0.18 a | 0.78 * | 0.096 |
| Bottled fruit juice (with sugar)/fruit drink | 752 (100) | 52.51 ± 0.48 | 2.72 | 52.92 ± 0.68 a | 2.78 | 52.13 ± 0.67 a | 2.67 * | 0.406 |
| Bottled fruit juice (without sugar) | 41 (5.45) | 3.59 ± 0.66 | 0.18 | 4.61 ± 1.15 a | 0.24 | 2.67 ± 0.69 a | 0.13 | 0.152 |
| Vegetable juice | 50 (6.65) | 0.56 ± 0.18 | 0.03 | 0.84 ± 0.36 a | 0.05 | 0.30 ± 0.12 a | 0.02 | 0.157 |
| Fresh vegetable juice | 42 (5.59) | 0.23 ± 0.06 | 0.01 | 0.30 ± 0.09 a | 0.02 | 0.16 ± 0.06 a | 0.01 | 0.232 |
| Bottled vegetable juice | 8 (1.06) | 0.33 ± 0.18 | 0.02 | 0.54 ± 0.35 a | 0.03 | 0.14 ± 0.10 a | 0.01 | 0.268 |
| Hot Beverages | 752 (100) | 0.70 ± 0.01 | 0.037 | 0.67 ± 0.01 a | 0.03 | 0.72 ± 0.01 b | 0.04 * | 0.001 |
| Sports and energy drinks | 21 (2.79) | 0.75 ± 0.23 | 0.04 | 0.31 ± 0.18 a | 0.02 | 1.15 ± 0.40 a | 0.06 | 0.059 |
| Sports drinks | 6 (0.80) | 0.25 ± 0.14 | 0.01 | 0.14 ± 0.14 a | 0.01 | 0.35 ± 0.24 a | 0.02 | 0.463 |
| Energy drinks | 18 (2.39) | 0.50 ± 0.16 | 0.02 | 0.17 ± 0.12 a | 0.01 | 0.80 ± 0.29 b | 0.04 * | 0.047 |
| Alcoholic beverages | 13 (1.73) | 0.48 ± 0.25 | 0.02 | 0.01 ± 0.01 a | 0.00 | 0.90 ± 0.48 a | 0.04 * | 0.064 |
| Present Study (Lebanon) | France a | USA b | Mexico c | Present Study (Lebanon) | ||||
|---|---|---|---|---|---|---|---|---|
| 4–8 years | 9–13 years | 4–8 years | 9–13 years | 4–8 years | 9–13 years | 4–8 years | 9–13 years | |
| Total water intake (TWI) (mL/day) | 1233 | 1416 | 1447 | 1711 | 1426.8 | 1658.4 | 1600.63 | 1697.68 |
| Plain water intake (mL/day) | 407.6 | 498.2 | 364.9 | 496.1 | 350.2 | 426.9 | 767.32 | 840.49 |
| Contribution of plain water to TWI (%) | 33 | 35 | 25.2 | 29 | 24.5 | 25.7 | 47.61 | 49.05 |
| Water intake from foods (mL/day) | 492.3 | 555.5 | 431.4 | 457.5 | 504.8 | 597.2 | 450.69 | 460.41 |
| Contribution of foods to TWI (%) | 40 | 39.2% | 29.8 | 26.7 | 35.4 | 36.0 | 28.5 | 27.7 |
| Water intake from all beverages (mL/day) | 740.7 | 860.6 | 1015.4 | 1254 | 922.1 | 1061.2 | 1143.53 | 1241.62 |
| Contribution of all beverages to TWI (%) | 60.1 | 60.7 | 70.2 | 73.3 | 64.6 | 64.0 | 70.85 | 72.28 |
| Water intake from all beverages (excluding plain water) (mL/day) | 333.3 | 362.4 | M: 678 d | M: 814 d | 571.9 d | 634.3 d | 376.2 | 401.1 |
| F: 621 d | F: 702 d | |||||||
| Contribution of all beverages (excluding plain water) to TWI (%) | 27.0 | 25.6 | M: 46.9 | M: 47.6 | 40.1 | 38.2 | 23.5 | 23.6 |
| F: 43.0 | F: 41.0 | |||||||
| Beverages with the highest contribution to TWI | 4–13 years: Plain water (33%–35%) | Plain Water: 25.2% | Plain Water (29%) | Plain water: (24.5%) | Plain water (25.7%) | Plain water (47.6%) | Plain water (49.05%) | |
| Milk (13.2%) | Milk (20.4%) | Milk (15.7%) | Fruit water (8.8%) | Fruit water (8.6%) | Fruit juice (10.3%) | Soda: 10.3% | ||
| Fruit juice (5.5%) | Fruit drink (7.9%) | Soda (12%) | Milk (5.5%) | Soda (7%) | Soda (8.1%) | Fruit juice (9.5%) | ||
| Proportion of children not meeting AI * | 89 | Boys: 90 | 75 | Boys: 85 | 71 | Boys: 83 | 74.0 | Boys: 92.1 |
| Girls: 93 | Girls: 83 | Girls: 81 | Girls: 97.8 | |||||
| Shortfall compared to AI (mL/day) * | 367 | Boys: 594 | 253 | Boys: 633 | 273 | Boys: 668 | 99 | Boys: 592 |
| Girls: 587 | Girls: 444 | Girls: 516 | Girls: 533 | |||||
| Water to energy ratio | 4–13 years: Boys: 0.75; | 0.85 | Boys: 0.88 | 0.84 | Boys: 0.82 | 0.84 | 0.87 | |
| Girls: 0.77 | Girls: 0.95 | Girls: 0.84 | ||||||
| Contribution of caloric beverages to total EI (%) | 11.5 | 10.1 | 19.5 | 18 | 19.8 | 17.5 | 9.27 | 9.44 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jomaa, L.; Hwalla, N.; Constant, F.; Naja, F.; Nasreddine, L. Water and Beverage Consumption among Children Aged 4–13 Years in Lebanon: Findings from a National Cross-Sectional Study. Nutrients 2016, 8, 554. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090554
Jomaa L, Hwalla N, Constant F, Naja F, Nasreddine L. Water and Beverage Consumption among Children Aged 4–13 Years in Lebanon: Findings from a National Cross-Sectional Study. Nutrients. 2016; 8(9):554. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090554
Chicago/Turabian StyleJomaa, Lamis, Nahla Hwalla, Florence Constant, Farah Naja, and Lara Nasreddine. 2016. "Water and Beverage Consumption among Children Aged 4–13 Years in Lebanon: Findings from a National Cross-Sectional Study" Nutrients 8, no. 9: 554. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090554