Effects of Ultrasound-Guided Administration of Botulinum Toxin (IncobotulinumtoxinA) in Patients with Lateral Epicondylitis

Abstract
:1. Introduction
2. Results
2.1. Demographics and Baseline Characteristics
2.2. Treatment
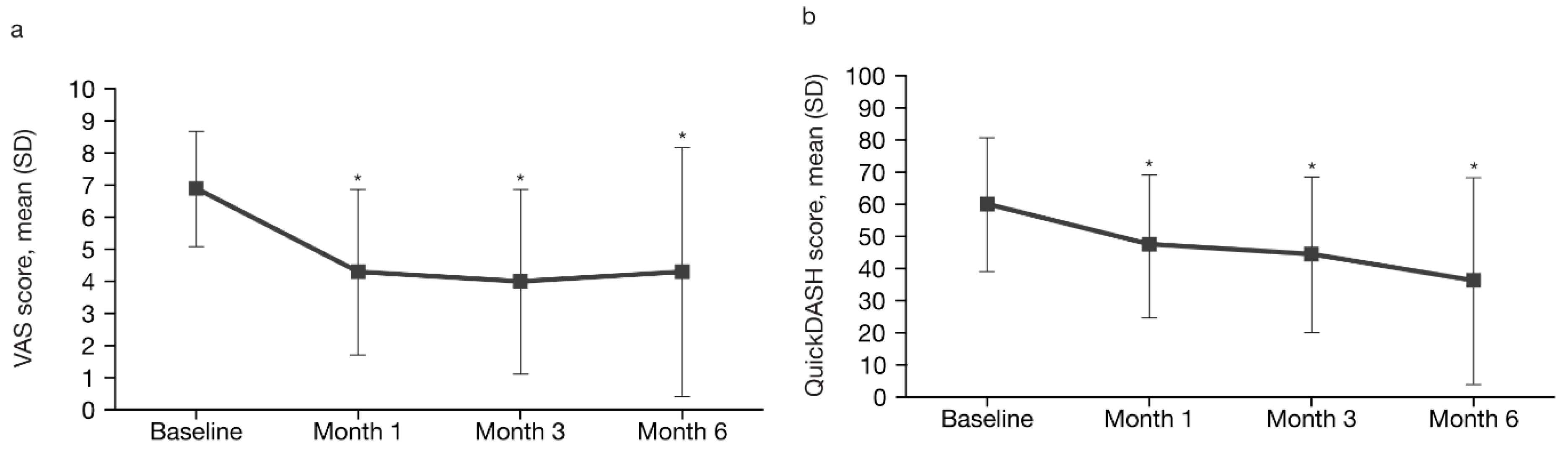
2.3. Efficacy
2.4. Analysis in Different Patient Groups
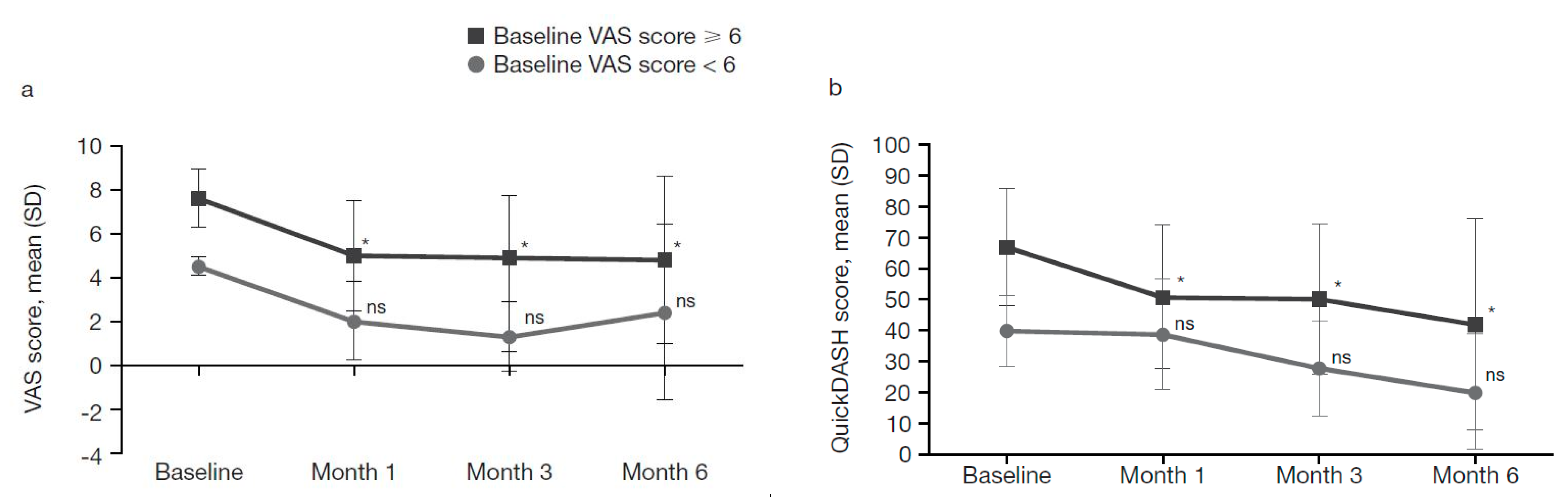
2.4.1. Patients Grouped by Baseline VAS Score
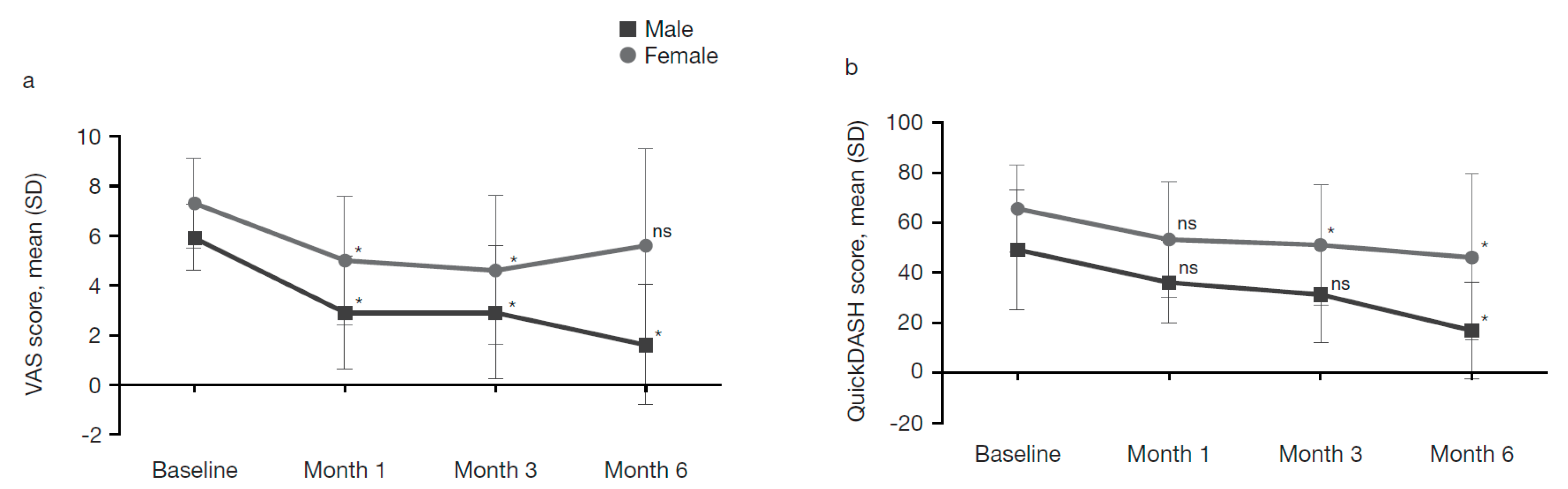
2.4.2. Patients Grouped by Sex
2.5. Safety
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Design
5.2. Patients
5.3. Study Treatment
5.4. Assessed Variables
5.5. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cohen, M.S.; Romeo, A.A.; Hennigan, S.P.; Gordon, M. Lateral epicondylitis: Anatomic relationships of the extensor tendon origins and implications for arthroscopic treatment. J. Shoulder Elbow Surg. 2008, 17, 954–960. [Google Scholar] [CrossRef]
- Bisset, L.; Coombes, B.; Vicenzino, B. Tennis elbow. BMJ Clin. Évid. 2011, 2011, 1117. [Google Scholar]
- Bunata, R.E.; Brown, D.S.; Capelo, R. Anatomic factors related to the cause of tennis elbow. J. Bone Joint Surg. Am. 2007, 89, 1955–1963. [Google Scholar] [CrossRef]
- Hume, P.A.; Reid, D.; Edwards, T. Epicondylar injury in sport: Epidemiology, type, mechanisms, assessment, management and prevention. Sports Med. 2006, 36, 151–170. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Dhaliwal, H.P.; Kukreja, R.V.; Singh, B.R. The botulinum toxin as a therapeutic agent: Molecular structure and mechanism of action in motor and sensory systems. Semin. Neurol. 2016, 36, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity and headache: Report of the guideline development subcommittee of the american academy of neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [PubMed]
- Galvin, R.; Callaghan, C.; Chan, W.-S.; Dimitrov, B.D.; Fahey, T. Injection of botulinum toxin for treatment of chronic lateral epicondylitis: Systematic review and meta-analysis. Semin. Arthritis Rheum. 2011, 40, 585–587. [Google Scholar] [CrossRef]
- Jabbari, B.; Machado, D. Treatment of refractory pain with botulinum toxins—An evidence-based review. Pain Med. 2011, 12, 1594–1606. [Google Scholar] [CrossRef]
- Krogh, T.P.; Bartels, E.M.; Ellingsen, T.; Stengaard-Pedersen, K.; Buchbinder, R.; Fredberg, U.; Bliddal, H.; Christensen, R. Comparative effectiveness of injection therapies in lateral epicondylitis: A systematic review and network meta-analysis of randomized controlled trials. Am. J. Sports Med. 2013, 41, 1435–1446. [Google Scholar] [CrossRef]
- Vicenzino, B.; Coombes, B.K. A single botulinum toxin injection at a precise anatomic point on the forearm reduces pain at rest, compared to placebo injection in patients with chronic refractory lateral epicondylitis. Évid.-Based Med. 2010, 15, 149–150. [Google Scholar] [CrossRef]
- Placzek, R.; Drescher, W.; Deuretzbacher, G.; Hempfing, A.; Meiss, A.L. Treatment of chronic radial epicondylitis with botulinum toxin a. A double-blind, placebo-controlled, randomized multicenter study. J. Bone Joint Surg. Am. 2007, 89, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.M.; Hui, A.C.; Tong, P.Y.; Poon, D.W.; Yu, E.; Wong, L.K. Treatment of lateral epicondylitis with botulinum toxin: A randomized, double-blind, placebo-controlled trial. Ann. Intern. Med. 2005, 143, 793–797. [Google Scholar] [CrossRef]
- Climent, J.M.; Fenollosa, P.; Martín del Rosario, F.M. Rehabilitacion Intervencionista, 1st ed.; Ergon: Madrid, Spain, 2012; pp. 1–592. ISBN 978-8415351-19-1. [Google Scholar]
- Espandar, R.; Heidari, P.; Rasouli, M.R.; Saadat, S.; Farzan, M.; Rostami, M.; Yazdanian, S.; Mortazavi, S.M. Use of anatomic measurement to guide injection of botulinum toxin for the management of chronic lateral epicondylitis: A randomized controlled trial. Can. Med. Assoc. J. 2010, 182, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Villamayor-Blanco, B.; Misa-Agustiño, M.J.; Jorge-Mora, M.T.; López-Castro, A.; López-Pesado, I.; Jorge-Barreiro, Y.F.J. Resultados terapéuticos a corto plazo de la infiltración con toxina botulínica ante el fracaso del tratamiento convencional de 7 pacientes con epicondylitis. Rehabilitación 2008, 42, 122–126. [Google Scholar] [CrossRef]
- Santos, B.; Calderón, E.; Ordóñez, P.; García-Hernández, R.; Torres, L.M. Tratamiento de epicondilitis refractaria con neurotoxina botulínica tipo a libre de complejo proteínico. Rev. Soc. Esp. Dolor 2013, 20, 8–10. [Google Scholar] [CrossRef]
- Kalichman, L.; Bannuru, R.R.; Severin, M.; Harvey, W. Injection of botulinum toxin for treatment of chronic lateral epicondylitis: Systematic review and meta-analysis. Semin. Arthritis Rheum. 2011, 40, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Oskarsson, E.; Piehl Aulin, K.; Gustafsson, B.E.; Pettersson, K. Improved intramuscular blood flow and normalized metabolism in lateral epicondylitis after botulinum toxin treatment. Scand. J. Med. Sci. Sports 2009, 19, 323–328. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Ortega-Santiago, R.; Ambite-Quesada, S.; Jiménez-García, R.; Arroyo-Morales, M.; Cleland, J.A. Specific mechanical pain hypersensitivity over peripheral nerve trunks in women with either unilateral epicondylalgia or carpal tunnel syndrome. J. Orthop. Sports Phys. Ther. 2010, 40, 751–760. [Google Scholar] [CrossRef]
- Ahmad, Z.; Siddiqui, N.; Malik, S.S.; Abdus-Samee, M.; Tytherleigh-Strong, G.; Rushton, N. Lateral epicondylitis: A review of pathology and management. Bone Joint J. 2013, 95-b, 1158–1164. [Google Scholar] [CrossRef]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L., 3rd. Sex, gender and pain: A review of recent clinical and experimental findings. J. Pain 2009, 10, 447–485. [Google Scholar] [CrossRef]
- Ho, K.; Spence, J.; Murphy, M.F. Review of pain-measurement tools. Ann. Emerg. Med. 1996, 27, 427–432. [Google Scholar] [CrossRef]
- Beaton, D.E.; Wright, J.G.; Katz, J.N.; Upper Extremity Collaborative Group. Development of the quickdash: Comparison of three item-reduction approaches. J. Bone Joint Surg. Am. 2005, 87, 1038–1046. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients | n = 24 |
|---|---|
| Sex | n (%) |
| Male | 8 (33.3) |
| Female | 16 (66.7) |
| Age years | |
| Mean (SD) | 46.8 (9) |
| Median (interquartile range) | 48.5 (43.0 to 52.8) |
| Patients with right dominance, n (%) | 24 (100) |
| Injured side | n (%) |
| Left | 5 (20.8) |
| Right | 19 (79.2) |
| Symptom progression time, months | |
| Mean (SD) | 20.0 (19.8) |
| Median (interquartile range) | 12 (9.3 to 24.0) |
| Pain, baseline VAS score | |
| Mean (SD) | 6.85 (1.8) |
| Median (interquartile range) | 7 (5.3 to 8.4) |
| Upper limb functionality, baseline QuickDASH score | |
| Mean (SD) | 60.12 (20.9) |
| Median (interquartile range) | 60 (45.0 to 79.5) |
| Previous ineffective treatments | n (%) |
| Analgesics/NSAIDs | 24 (100) |
| Physiotherapy | 17 (70.8) |
| Electrotherapy | 13 (54.2) |
| Peritendinous injections | 20 (83.3) |
| Positive resisted manoeuvres at baseline | n (%) |
| Extensor carpi ulnaris | 7 (29.2) |
| Extensor digiti minimi | 10 (41.7) |
| Extensor digitorum longus | 21 (87.5) |
| Extensor carpi radialis brevis | 20 (83.3) |
| Muscle Treated | IncobotulinumtoxinA Dose, U | Number of Patients Treated, n (%) |
|---|---|---|
| Extensor carpi ulnaris | 20 | 7 (29.2) |
| Extensor digiti minimi | 10 | 9 (37.5) |
| Extensor digitorum longus | 30 | 21 (87.5) |
| Extensor carpi radialis brevis | 20 | 20 (83.3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galván Ruiz, A.; Vergara Díaz, G.; Rendón Fernández, B.; Echevarría Ruiz De Vargas, C. Effects of Ultrasound-Guided Administration of Botulinum Toxin (IncobotulinumtoxinA) in Patients with Lateral Epicondylitis. Toxins 2019, 11, 46. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11010046
Galván Ruiz A, Vergara Díaz G, Rendón Fernández B, Echevarría Ruiz De Vargas C. Effects of Ultrasound-Guided Administration of Botulinum Toxin (IncobotulinumtoxinA) in Patients with Lateral Epicondylitis. Toxins. 2019; 11(1):46. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11010046
Chicago/Turabian StyleGalván Ruiz, Antonio, Gloria Vergara Díaz, Beatriz Rendón Fernández, and Carmen Echevarría Ruiz De Vargas. 2019. "Effects of Ultrasound-Guided Administration of Botulinum Toxin (IncobotulinumtoxinA) in Patients with Lateral Epicondylitis" Toxins 11, no. 1: 46. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11010046