Uremic Toxins and Atrial Fibrillation: Mechanisms and Therapeutic Implications


1
Department of Cardiology, Faculty of Medicine, University of Tsukuba, Tsukuba, Ibaraki 305-8575, Japan
2
YUMINO Heart Clinic, Toshima-ku, Tokyo 171-0033, Japan
*
Author to whom correspondence should be addressed.
Toxins 2019, 11(10), 597; https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11100597
Submission received: 23 September 2019
/
Revised: 7 October 2019
/
Accepted: 10 October 2019
/
Published: 13 October 2019
(This article belongs to the Special Issue The Endothelial Effects of Uremic Toxins)
{kind=link}
{kind=link}
Abstract
:Atrial fibrillation (AF) is the most prevalent arrhythmia in the general population. There is a close association between chronic kidney disease (CKD) and AF. In recent years, attention has been focused on the relationship between AF and uremic toxins, including indoxyl sulfate (IS). Several animal studies have shown that IS promotes the development and progression of AF. IS has been shown to cause fibrosis and inflammation in the myocardium and exacerbate AF by causing oxidative stress and reducing antioxidative defense. Administration of AST-120, an absorbent of uremic toxins, decreases uremic toxin-induced AF in rodents. We have recently reported that patients with a higher serum IS level exhibit a higher rate of AF recurrence after catheter ablation, with serum IS being a significant predictor of AF recurrence. In this review, we discuss the possible mechanisms behind the AF-promoting effects of uremic toxins and summarize the reported clinical studies of uremic toxin-induced AF.
Key Contribution: We discuss the atrial fibrillation-promoting effects of uremic toxins by summarizing both basic research and clinical studies.
1. Introduction
Atrial fibrillation (AF) is a common and chronic cardiovascular condition. AF requires expensive health monitoring and treatment because AF patients have an increased risk of stroke, sudden death, heart failure, unplanned hospital admissions, and other complications [1,2,3,4]. Although the management of AF has substantially advanced, with significant developments in the past few decades, the contributing factors and mechanisms promoting AF are still unclear.
An association between chronic kidney disease (CKD) and AF has been described, and several studies have revealed the complex relationship between CKD and AF. In this review, we focused on the causative association between uremic toxins and AF.
2. Epidemiology of AF
AF is the most prevalent arrhythmia in the general population [1] and is associated with an increased risk of stroke [2], heart failure [3], and mortality [4]. The number of people with AF has been increasing worldwide because of an aging general population, and an increased incidence of AF is expected with the increasing life expectancy of society [1,5]. The Global Burden of Disease Study in 2010 [6] stated that the age-adjusted mortality rate (per 100,000 population) for AF patients in 1990 was 0.8 for men and 0.9 for women. The age-adjusted mortality rate had increased to 1.6 and 1.7 by 2010, representing a 2-fold and 1.9-fold increase for men and women, respectively. In 1990, the overall incidence rates of AF in the world population were 60.7 per 100,000 person-years in men and 43.8 in women. In 2010, the estimated incidence rates had increased to 77.5 per 100,000 persons-years in men and 59.5 in women. It is predicted that AF will affect 5–16 million people in the United States and more than 1 million people in Japan by 2050 [5]. Therefore, AF is one of the most important cardiovascular diseases that needs to be effectively managed in aging populations.
3. Pathophysiological Mechanisms of AF
3.1. Triggers and Substrate of AF
AF is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation with the subsequent deterioration of atrial mechanical function. It is well accepted that AF development needs both a trigger and a susceptible substrate. AF is produced by triggered activity from pulmonary vein ectopic foci or the genesis of re-entry circuits in atrial substrates [7], and sustained high frequency reentrant AF drivers (rotors) can be produced by a focal trigger. The electrical waves emerge from the rotors and undergo spatially distributed fragmentation and give rise to fibrillatory conduction [8].
3.2. Cardiac Autonomic Nervous System and Triggered Spontaneous Pulmonary Vein Firing
Autonomic nerve input to the atria originate from both the central autonomic (preganglionic) nervous system and the intrinsic cardiac autonomic nervous system. The intrinsic cardiac autonomic nervous system contains autonomic ganglionated plexi, or clusters of ganglia. The autonomic ganglionated plexi receive input from the central extrinsic autonomic nervous system and numerous interconnecting neurons that provide communication within and between the ganglionated plexi. Focal firing in the pulmonary veins by ganglionated plexi stimulation requires both sympathetic and parasympathetic activity. Parasympathetic stimulation shortens the action potential duration and effective refractory period in atrial and pulmonary vein myocytes, and sympathetic stimulation increases calcium loading and automaticity. Ganglionated plexi may promote AF by activating triggered spontaneous pulmonary vein firing [8].
4. Treatment of AF
The three domains of AF management are (1) the stabilization of underlying and accompanying cardiovascular conditions, (2) stroke risk assessment and oral anticoagulation for stroke prevention, and (3) heart rate and rhythm control therapy [9].
4.1. Stabilization of Underlying and Accompanying Cardiovascular Conditions
The presence of AF strongly indicates that other cardiovascular comorbidities are present, such as hypertension, heart failure, valvular heart disease, obesity, and coronary artery disease. Focusing on heart failure, it is well known that AF increases the risk of stroke, hospitalization, and death in heart failure patients. The treatment of AF can substantially alter long-term outcomes in patients with heart failure. In addition, heart failure may promote AF by creating an AF-promoting atrial substrate via left atrial dilatation, activating the cardiac autonomic nervous system and inducing a focus of inflammation [10].
4.2. Stroke Risk Assessment and Oral Anticoagulation for Stroke Prevention
AF patients have a hypercoagulable state, and AF is one of the most important causes of thromboembolism. The presence of AF is an independent risk factor for stroke and thromboembolism, and stroke associated with AF increases mortality and morbidity [11]. Patients with one or more stroke risk factors (CHA2DS2-VASc score of ≥1) should be treated with oral anticoagulants such as well-controlled warfarin or a direct oral anticoagulant.
4.3. Rate and Rhythm Control Therapy
In AF, each part of the atrial myocardium is stimulated at a rate of 300–400 activations per minute. The rapid reactivation of atrial myocardium leads to a cessation of atrial contractility and results in rapid and irregular ventricular rates. Heart rate control is achieved pharmacologically by slowing the atrioventricular nodal conduction using the β-blockers digoxin or digitoxin, as well as verapamil or diltiazem. Rhythm control with antiarrhythmic drugs are not superior to heart rate control in patients with coexisting heart failure and AF [12]. Another way to maintain sinus rhythm is through catheter ablation, which is a well-established option for drug resistant symptomatic AF in patients with otherwise normal cardiac function [13,14,15,16,17] and in patients with heart failure [18,19,20,21,22]. Moreover, a recent study has shown that catheter ablation is superior to drug therapy for AF patients with heart failure, resulting in an improvement in left ventricular ejection fraction, quality of life, functional status, and mortality [23,24,25,26]. Although catheter ablation has become an established treatment option as implemented in the current guidelines for the treatment of AF [17,27], post-procedure AF recurrence remains a major clinical problem. Unfortunately, the mechanisms of AF recurrence after ablation are unknown. Patient selection seems to play an important role in the procedural success and risk stratification for the prevention of AF recurrence. This is based on pre-existing clinical patient characteristics, such as age, the pattern and duration of AF, and the degree of atrial enlargement. However, these indicators are insufficient to predict AF recurrence [28]. Therefore, new AF biomarkers are needed to predict treatment response after catheter ablation and better understand the mechanisms that promote AF development and recurrence.
5. AF and CKD
Several clinical trials have shown that AF and CKD are closely related [2,29,30,31,32]. It has been reported that the prevalence of AF in CKD patients is 2–3 times higher than that in the general population [33,34]. Moreover, the prevalence of AF in dialysis patients is as high as 27% [35,36,37,38], compared to 1.0% in the general population [16], indicating that dialysis cannot reduce the risk of AF. Therefore, non-dialysis uremic factors are thought to be factors that promote atrial fibrillation. Uremic cardiomyopathy is a distinctive type of heart failure associated with CKD. Uremic cardiomyopathy is caused by an impairment of microvascular function, low-grade inflammation, oxidative stress, and enhanced cardiac fibrosis. In addition, hypertension, anemia, and activation of the renin–angiotensin–aldosterone system and sympathetic nervous may contribute to the occurrence of uremic cardiomyopathy in CKD. The pathophysiological effects of CKD contribute multiple arrhythmogenic factors to the development of AF [39,40,41].
In addition, the relationship between AF recurrence after catheter ablation for AF and CKD has been addressed in recent reports [42,43,44]. Patients with CKD were at high risk of AF recurrence after catheter ablation. Although atrial remodeling associated with renal dysfunction was thought to be responsible for the poor prognosis after AF ablation in CKD patients, the exact mechanism has not been fully elucidated.
6. Uremic Toxins and Cardiovascular Diseases
Protein-bound uremic toxins, such as indoxyl sulfate (IS), indole-3 acetic acid (IAA), p-cresol, and p-cresyl sulfate, which originate from protein fermentation, can increase oxidative stress, inflammation, and activate the neurohormonal system that results in cardiovascular fibrosis and oxidative injury [45,46]. Furthermore, uremic toxins produce pro-hypertrophic, pro-inflammatory, pro-fibrotic conditions in cardiomyocytes [47,48,49].
IS is a uremic toxin that has high protein-binding ability and is poorly dialyzable. Even after hemodialysis, the serum IS level remains high [50]. IS is one of the most common uremic toxins derived from dietary protein metabolism by the gut microbiota and is involved in the pathogenesis of cardiovascular diseases including AF [51,52,53,54]. Recently, the relationship between IS and cardiovascular diseases among CKD patients is attracting increasing attention. Barreto et al. reported that an elevated serum IS level was associated with an increased overall death and cardiovascular-related death among CKD patients [55]. Furthermore, Lin et al. [56] indicated that a serum IS level was a useful biomarker in predicting cardiovascular events in advanced CKD patients [56]. Other researchers have reported an association between elevated IS levels and an increased risk of left ventricular diastolic dysfunction [57,58].
Although IAA has not been studied as much as IS, a recent study suggests that IAA has a cardiovascular toxic effect and is associated with the progress of cardiovascular disease [53]. Dou et al. [53] studied patients with CKD and found that mortality and cardiovascular events were significantly higher in the higher IAA group (IAA > 3.73 mM) than in the lower IAA group (IAA < 3.73 mM). The IAA concentration positively correlated with malondialdehyde and C-reactive protein (CRP) was used to evaluate oxidative stress and inflammation. In multivariate Cox regression analysis, serum IAA was a significant predictor of mortality and cardiovascular events even after adjustments for CKD stage [53]. They also demonstrated direct effects of IAA on endothelial cells. In culture experiments with human endothelial cells, IAA activated an inflammatory nongenomic aryl hydrocarbon receptor (AhR)/p38 MAPK/NF-kB pathway involved in the pro-inflammatory enzyme cyclooxygenase-2 upregulation. Moreover, IAA increased production of reactive oxygen species from the endothelial cells. Thus, IAA has prooxidant and pro-inflammatory effects in human endothelial cells, which may explain the association between IAA concentration and the increased risk of mortality and cardiovascular events in CKD patients [53].
7. IS and AF
In recent years, attention has been focused on the relationship between AF and uremic toxins, especially IS. Several animal studies have revealed that IS has a causative role in exacerbating AF. IS has been shown to promote AF via its effect on cardiac fibrosis and inflammation by increasing oxidative stress; the administration of AST-120, an absorbent of uremic toxins, decreased AF inducibility in rodents [62,63]. In the clinic, we have recently reported that patients with elevated serum IS levels showed a higher AF recurrence rate after successful catheter ablation, with serum IS being a significant predictor of AF recurrence [64].
7.1. Experimental Studies in Animal Models
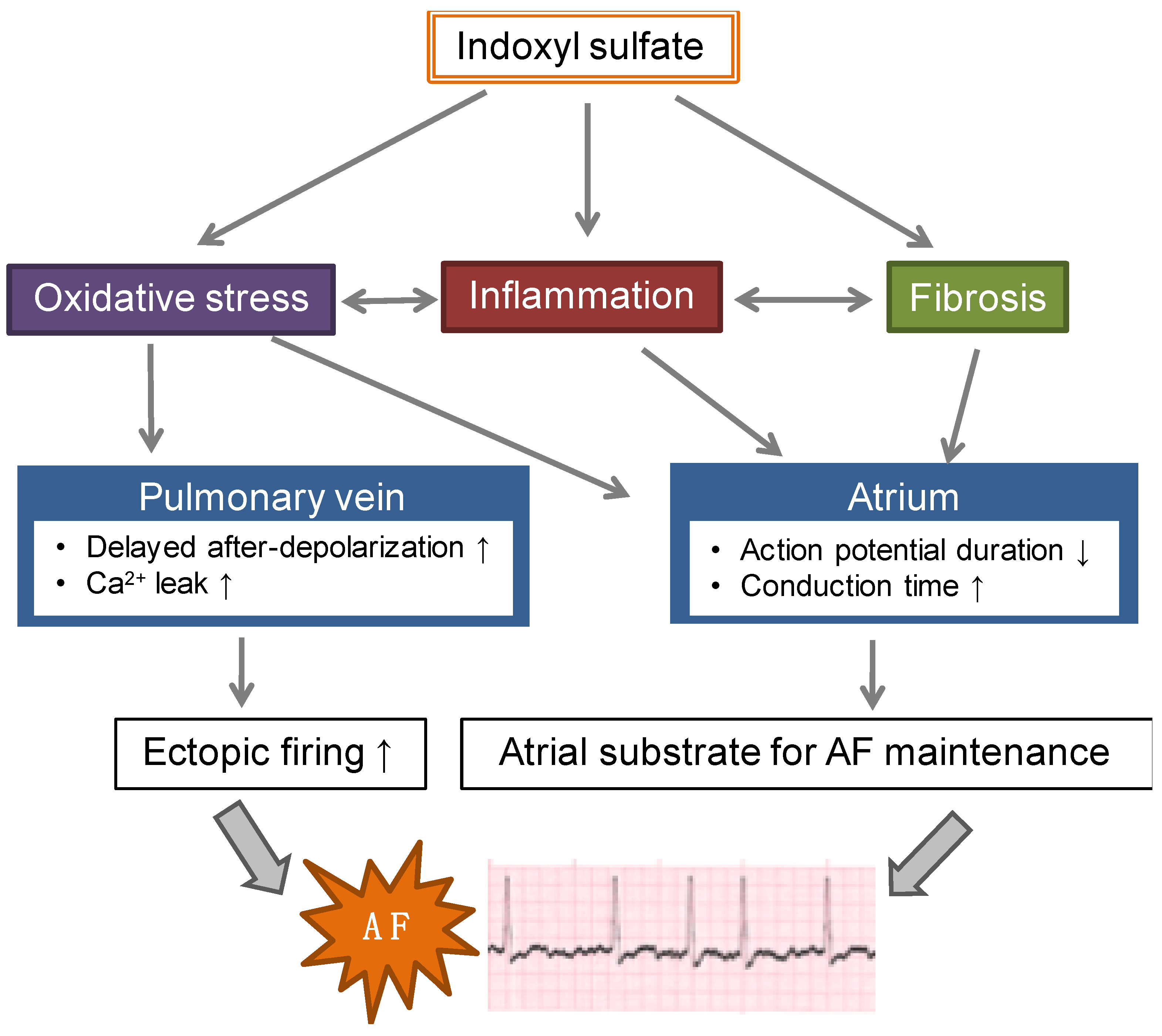
The arrhythmogenic effects of IS have been demonstrated in in vitro, ex vivo, and in vivo experiments (Figure 1). Chen et al. [63] showed that IS induced an increased occurrence of delayed after-depolarizations, burst firing, and increased calcium leakage in isolated pulmonary veins, and decreased spontaneous beating of the sinoatrial nodes and shortened the action potential durations in left atria isolated from rabbits. Stimulation with burst pacing and isoproterenol (a β-agonist) induced an increased occurrence of AF and a longer AF duration in the left atrial tissue with IS than without IS. This IS-induced arrhythmogenesis was attenuated by the antioxidant ascorbic acid. These data suggested that IS increases pulmonary vein and atrial arrhythmogenesis through an oxidative stress-dependent mechanism.
Lekawanvijit et al. demonstrated direct effects of IS on cardiac fibroblasts and myocytes [47]. Stimulation with IS in neonatal rat fibroblasts and cardiomyocytes increased collagen synthesis and myocyte hypertrophy, respectively. They also showed that proinflammatory effects of IS in cultured THP-1 cells, a human monocytic cell line, determined by a significant increase in inflammatory cytokines tumor necrosis factor-alpha, interleukin-6 (IL-6), and IL-1β. Thus, IS may have pro-fibrotic, pro-hypertrophic, and pro-inflammatory effects on cardiac cells.
In a rat model of CKD induced by 5/6 nephrectomy, Aoki et al. demonstrated that IS increases the occurrence of AF in vivo [62]. Serum IS level was significantly increased after 5/6 nephrectomy. In electrophysiological experiments, AF was induced by atrial extrastimuli at almost 100% of the induction rate. They showed that administration of AST-120—that is commonly used in clinical settings in Japan as an absorbent of uremic toxins to delay incident renal replacement therapy—decreased the serum level of IS, resulting in decreased oxidative stress, reduced inflammation, reduced fibrosis in the left atrium, and decreased occurrence of AF. Incubation of cultured atrial fibroblasts with IS upregulated the expression of NADPH oxidase 2 and 4 and malondialdehyde (oxidative stress markers), along with an increase in profibrotic and inflammatory molecules, such as α-smooth muscle actin, transforming growth factor β1, collagen type 1, and monocyte chemoattractant protein 1 (MCP-1), [62]. These data suggested that IS could have a pathogenetic factor for AF in renal dysfunction mediated by the progression of atrial remodeling by oxidative stress, fibrosis, and inflammation.
7.2. IS and AF Recurrence after Catheter Ablation
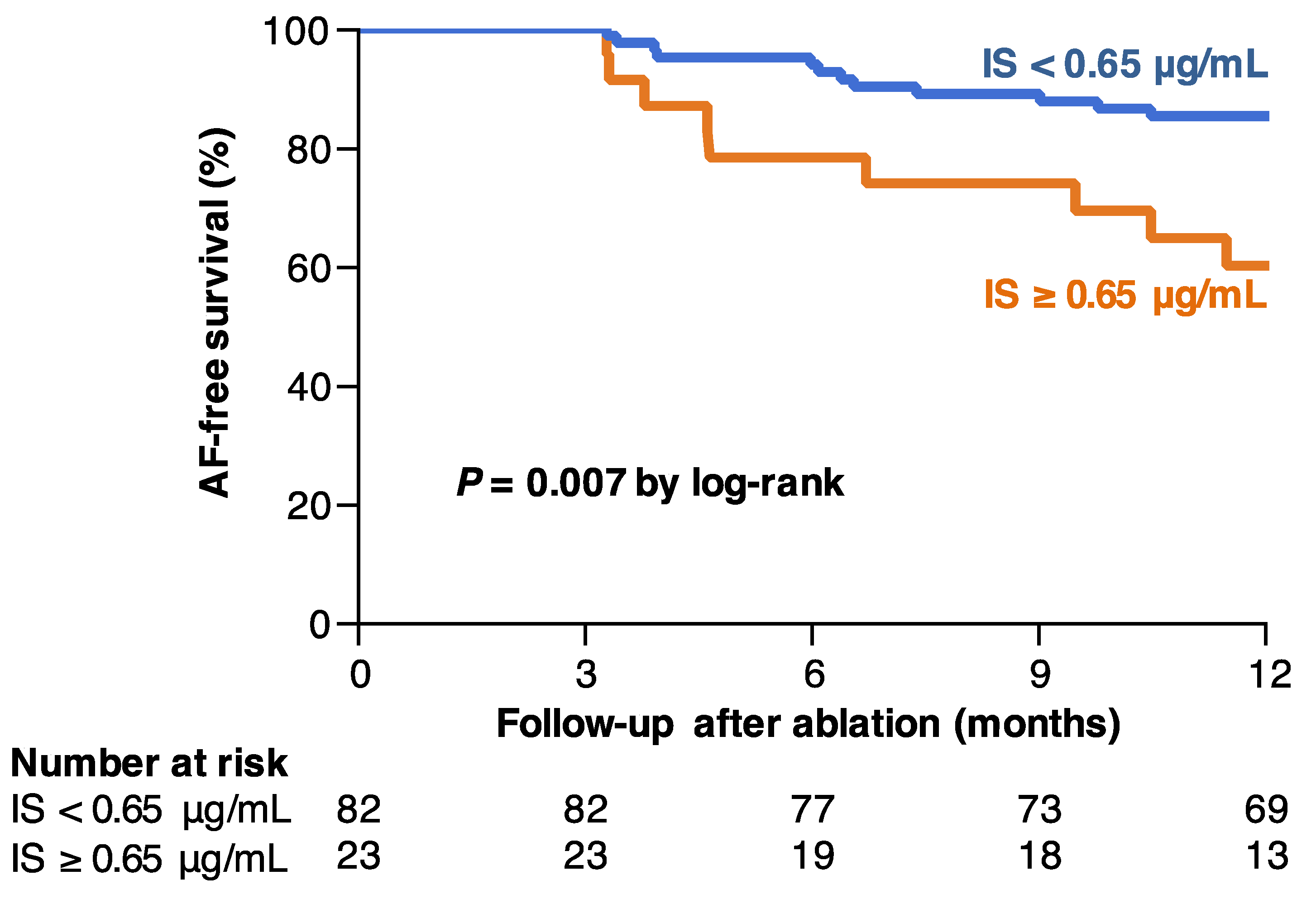
The high AF recurrence rate after ablation in CKD patients suggests that uremic toxins may be involved in the development of AF. Although several studies have investigated the association between IS and cardiovascular disease as we described above, limited clinical data support the association between IS and AF. Therefore, we investigated the association between IS levels and AF recurrence after radiofrequency catheter ablation [64]. The study investigated 125 consecutive patients with nonvalvular AF scheduled for catheter ablation for AF. This cohort included patients with normal or mild-to-moderate reduced renal function (CKD 1–3). Serum levels of IS and IAA were measured by reversed-phase high-performance liquid chromatography before catheter ablation [65]. After catheter ablation, follow-ups were performed at 1, 3, 6, and 12 months. In this cohort, serum IS levels were significantly increased in patients with CKD stage 3 compared to CKD stage 1 and 2. On the other hand, IAA levels were not statistically different among patients with CKD stage 1, 2, and 3. The correlations of serum IS levels with estimated glomerular filtration rate (eGFR) (r = −0.295, p = 0.002) and creatinine clearance (CrCl) (r = −0.263, p = 0.007) were weak. IAA levels were also weakly correlated with eGFR (r = −0.255, p = 0.009), but not with CrCl (r = −0.102, p = 0.30). Patients were divided into two groups based on serum IS levels, the high (≥ 0.65 μg/mL) and low (< 0.65 μg/mL) IS group, which was set as the optimal cutoff value determined by the maximum Youden index (sensitivity + specificity − 1), on the basis of receiver operating characteristic curve analysis. The 1-year AF-free survival was markedly lower in patients with high serum IS levels than in those with low IS levels (60.1 ± 10.4% versus 85.2 ± 3.9%, p = 0.007) (Figure 2). In the univariate analysis, a serum IS level ≥ 0.65 μg/mL was associated with the recurrence of AF (hazard ratio = 3.10 [1.26–7.32], p = 0.015), and this association was maintained in multivariate Cox proportional hazard model (hazard ratio = 3.67 [1.13–11.7], p = 0.031) [64]. Thus, in patients undergoing successful catheter ablation, we identified that baseline IS levels independently predict AF recurrence.
8. Therapeutic Potential of AST-120 for AF
AST-120 (KREMEZIN) is approved in Japan, Korea, and the Philippines for progressive CKD patients as an absorbent of uremic toxins to delay incident renal replacement therapy in clinical settings [66]. AST-120 inhibits the absorption of indoles from the intestines and thus effectively reduces circulating and renal IS levels independent of renal dysfunction [52,67,68] AST-120 decreases serum IS levels in a dose-dependent fashion [69]. In uremic animal models, AST-120 has been shown to improve renal function and structure [68,70]. In humans, several prospective clinical trials have demonstrated the protective effects of AST-120 against the progression of renal dysfunction [71,72,73,74]. However, recent large-scale randomized controlled trials in humans have not observed any beneficial effects of AST-120 on impeding CKD progression [75,76]. There are several ongoing or unpublished clinical studies registered in ClinicalTrials.gov, which will reveal the role of AST-120 in CKD.
On the other hand, many animal studies and small human studies have suggested that AST-120 may have protective effects in cardiovascular disease. Endothelial dysfunction induced by the acute and chronic inflammatory status in CKD patients contributes towards overt cardiovascular disease [77]. There are several reports regarding the beneficial role of AST-120 on vascular function in CKD animals and patients. Treatment with AST-120 has been shown to ameliorate the following: endothelial dysfunction in CKD rats [78]; the extent and instability of atherosclerosis induced by kidney disease in apolipoprotein E-deficient mice [79]; flow-mediated vasodilation in pre-dialysis CKD patients [80]; and microvascular endothelial dysfunction and carotid arterial intima-media thickness in patients receiving hemodialysis [81]. There are also several reports supporting the beneficial effects of AST-120 in the prevention of left ventricular hypertrophy in CKD rats [82,83] and pre-dialysis patients [84]. More recently, Asanuma et al. [85] demonstrated that AST-120 treatment inhibits cardiac remodeling, attenuates apoptosis, and prevents the progression of heart failure in a dog model of heart failure induced by rapid right ventricular pacing.
There has been only one study that has examined the protective effects of AST-120 on AF [62]. Aoki et al. [62] examined the effect of AST-120 treatment in a rat model of CKD induced by 5/6 nephrectomy. AF induced by atrial extra stimuli in perfused hearts extracted from CKD rats was attenuated by AST-120 treatment. Left atrial enlargement and ventricular concentric hypertrophy were significantly prevented by AST-120 treatment, without significant improvement in systolic blood pressure and renal function [62]. AST-120 treatment suppressed expression of MCP-1 and vascular cell adhesion molecule 1 and infiltration of CD68-positive inflammatory cells in the atrium, suggesting that AST-120 attenuated monocyte-mediated inflammation in the atrium [62]. Overall, AST-120 appears to have protective effects against cardiovascular diseases including AF; however, additional randomized controlled trials are required to determine whether AST-120 reduces the risk of cardiovascular diseases in CKD patients.
9. Conclusions
In this review, we investigated the effects of protein-bound uremic toxins, especially IS, on the pathogenesis of AF. Using animal models, several studies have demonstrated that IS can exacerbate AF directly and indirectly by promoting enhanced oxidative stress and reduced antioxidative defense via its effect on cardiac fibrosis and inflammation. Clinical studies have supported the association between IS and AF by identifying elevated IS levels as a strong and independent predictor of AF recurrence in patients undergoing successful catheter ablation.
Methods to remove uremic toxins in the body are limited due to their high protein-binding capacity. AST-120 might be a new therapeutic compound to prevent AF and reduce AF recurrence in patients after catheter ablation.
Author Contributions
Writing—original draft preparation, F.Y.; writing—review and editing, K.T.; supervision, D.Y. and M.I.
Funding
This research received no external funding.
Acknowledgments
We would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fuster, V.; Rydén, L.E.; Cannom, D.S.; Crijns, H.J.; Curtis, A.B.; Ellenbogen, K.A.; Halperin, J.L.; Kay, G.N.; Le Huezey, J.-Y.; Lowe, J.E.; et al. 2011 ACCF/AHA/HRS Focused Updates Incorporated Into the ACC/AHA/ESC 2006 Guidelines for the Management of Patients With Atrial Fibrillation. J. Am. Coll. Cardiol. 2011, 57, e101–e198. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J.B.; Lip, G.Y.H.; Kamper, A.-L.; Hommel, K.; Køber, L.; Lane, D.A.; Lindhardsen, J.; Gislason, G.H.; Torp-Pedersen, C. Stroke and Bleeding in Atrial Fibrillation with Chronic Kidney Disease. N. Engl. J. Med. 2012, 367, 625–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, S.J.; Fonarow, G.C.; Solomon, S.D.; Subacius, H.P.; Ambrosy, A.P.; Vaduganathan, M.; Maggioni, A.P.; Böhm, M.; Lewis, E.F.; Zannad, F.; et al. Influence of atrial fibrillation on post-discharge natriuretic peptide trajectory and clinical outcomes among patients hospitalized for heart failure: insights from the ASTRONAUT trial. Eur. J. Heart Fail. 2017, 19, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Jabre, P.; Roger, V.L.; Murad, M.H.; Chamberlain, A.M.; Prokop, L.; Adnet, F.; Jouven, X. Mortality Associated With Atrial Fibrillation in Patients With Myocardial Infarction. Circulation 2011, 123, 1587–1593. [Google Scholar] [CrossRef]
- Bai, Y.; Wang, Y.-L.; Shantsila, A.; Lip, G.Y.H. The Global Burden of Atrial Fibrillation and Stroke: A Systematic Review of the Clinical Epidemiology of Atrial Fibrillation in Asia. Chest 2017, 152, 810–820. [Google Scholar] [CrossRef]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.-H.; McAnulty, J.H.; Zheng, Z.-J.; et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef]
- Chen, S.-A.; Hsieh, M.-H.; Tai, C.-T.; Tsai, C.-F.; Prakash, V.S.; Yu, W.-C.; Hsu, T.-L.; Ding, Y.-A.; Chang, M.-S. Initiation of Atrial Fibrillation by Ectopic Beats Originating From the Pulmonary Veins. Circulation 1999, 100, 1879–1886. [Google Scholar] [CrossRef] [Green Version]
- Calkins, H.; Kuck, K.H.; Cappato, R.; Brugada, J.; Camm, A.J.; Chen, S.-A.; Crijns, H.J.G.; Damiano, R.J.; Davies, D.W.; DiMarco, J.; et al. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendations for Patient Selection, Procedural Techniques, Patient Management and Follow-up, Definitions, Endpoints, and Research Trial Design. Hear. Rhythm 2012, 9, 632–696.e21. [Google Scholar] [CrossRef]
- Kirchhof, P. The future of atrial fibrillation management: integrated care and stratified therapy. Lancet (London, England) 2017, 390, 1873–1887. [Google Scholar] [CrossRef]
- Ferrari, R.; Bertini, M.; Blomstrom-Lundqvist, C.; Dobrev, D.; Kirchhof, P.; Pappone, C.; Ravens, U.; Tamargo, J.; Tavazzi, L.; Vicedomini, G.G. An update on atrial fibrillation in 2014: From pathophysiology to treatment. Int. J. Cardiol. 2016, 203, 22–29. [Google Scholar] [CrossRef]
- Lip, G.Y.; Tse, H.F.; Lane, D.A. Atrial fibrillation. Lancet 2012, 379, 648–661. [Google Scholar] [CrossRef]
- Knecht, S.; O’Neill, M.D.; Verbeet, T. Rhythm Control versus Rate Control for Atrial Fibrillation. N. Engl. J. Med. 2008, 359, 1522. [Google Scholar] [PubMed]
- Wazni, O.M.; Marrouche, N.F.; Martin, D.O.; Verma, A.; Bhargava, M.; Saliba, W.; Bash, D.; Schweikert, R.; Brachmann, J.; Gunther, J.; et al. Radiofrequency Ablation vs Antiarrhythmic Drugs as First-line Treatment of Symptomatic Atrial Fibrillation. JAMA 2005, 293, 2634. [Google Scholar] [CrossRef] [PubMed]
- Morillo, C.A.; Verma, A.; Connolly, S.J.; Kuck, K.H.; Nair, G.M.; Champagne, J.; Sterns, L.D.; Beresh, H.; Healey, J.S.; Natale, A.; et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of paroxysmal atrial fibrillation (RAAFT-2): a randomized trial. JAMA 2014, 311, 692–700. [Google Scholar] [CrossRef]
- Cosedis Nielsen, J.; Johannessen, A.; Raatikainen, P.; Hindricks, G.; Walfridsson, H.; Kongstad, O.; Pehrson, S.; Englund, A.; Hartikainen, J.; Mortensen, L.S.; et al. Radiofrequency Ablation as Initial Therapy in Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2012, 367, 1587–1595. [Google Scholar] [CrossRef] [Green Version]
- Fuster, V.; Rydén, L.E.; Cannom, D.S.; Crijns, H.J.; Curtis, A.B.; Ellenbogen, K.A.; Halperin, J.L.; Le Heuzey, J.-Y.; Kay, G.N.; Lowe, J.E.; et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation–executive summary. Eur. Heart J. 2006, 27, 1979–2030. [Google Scholar]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation 2014, 130, 2071–2104. [Google Scholar] [CrossRef]
- Khan, M.N.; Jaïs, P.; Cummings, J.; Di Biase, L.; Sanders, P.; Martin, D.O.; Kautzner, J.; Hao, S.; Themistoclakis, S.; Fanelli, R.; et al. Pulmonary-vein isolation for atrial fibrillation in patients with heart failure. N. Engl. J. Med. 2008, 359, 1778–1785. [Google Scholar] [CrossRef]
- MacDonald, M.R.; Connelly, D.T.; Hawkins, N.M.; Steedman, T.; Payne, J.; Shaw, M.; Denvir, M.; Bhagra, S.; Small, S.; Martin, W.; et al. Radiofrequency ablation for persistent atrial fibrillation in patients with advanced heart failure and severe left ventricular systolic dysfunction: a randomised controlled trial. Heart 2011, 97, 740–747. [Google Scholar] [CrossRef]
- Jones, D.G.; Haldar, S.K.; Hussain, W.; Sharma, R.; Francis, D.P.; Rahman-Haley, S.L.; McDonagh, T.A.; Underwood, S.R.; Markides, V.; Wong, T. A randomized trial to assess catheter ablation versus rate control in the management of persistent atrial fibrillation in heart failure. J. Am. Coll. Cardiol. 2013, 61, 1894–1903. [Google Scholar] [CrossRef]
- Chen, M.S.; Marrouche, N.F.; Khaykin, Y.; Gillinov, A.M.; Wazni, O.; Martin, D.O.; Rossillo, A.; Verma, A.; Cummings, J.; Erciyes, D.; et al. Pulmonary vein isolation for the treatment of atrial fibrillation in patients with impaired systolic function. J. Am. Coll. Cardiol. 2004, 43, 1004–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Biase, L.; Mohanty, P.; Mohanty, S.; Santangeli, P.; Trivedi, C.; Lakkireddy, D.; Reddy, M.; Jais, P.; Themistoclakis, S.; Dello Russo, A.; et al. Ablation Versus Amiodarone for Treatment of Persistent Atrial Fibrillation in Patients With Congestive Heart Failure and an Implanted Device. Circulation 2016, 133, 1637–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Virk, S.A.; Bennett, R.G.; Chow, C.; Sanders, P.; Kalman, J.M.; Thomas, S.; Kumar, S. Catheter Ablation Versus Medical Therapy for Atrial Fibrillation in Patients With Heart Failure: A Meta-Analysis of Randomised Controlled Trials. Hear. Lung Circ. 2019, 28, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Blomström-Lundqvist, C.; Gizurarson, S.; Schwieler, J.; Jensen, S.M.; Bergfeldt, L.; Kennebäck, G.; Rubulis, A.; Malmborg, H.; Raatikainen, P.; Lönnerholm, S.; et al. Effect of Catheter Ablation vs Antiarrhythmic Medication on Quality of Life in Patients With Atrial Fibrillation: The CAPTAF Randomized Clinical Trial. JAMA 2019, 321, 1059–1068. [Google Scholar] [CrossRef]
- Elgendy, A.Y.; Mahmoud, A.N.; Khan, M.S.; Sheikh, M.R.; Mojadidi, M.K.; Omer, M.; Elgendy, I.Y.; Bavry, A.A.; Ellenbogen, K.A.; Miles, W.M.; et al. Meta-Analysis Comparing Catheter-Guided Ablation Versus Conventional Medical Therapy for Patients With Atrial Fibrillation and Heart Failure With Reduced Ejection Fraction. Am. J. Cardiol. 2018, 122, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [Green Version]
- Kornej, J.; Hindricks, G.; Kosiuk, J.; Arya, A.; Sommer, P.; Husser, D.; Rolf, S.; Richter, S.; Huo, Y.; Piorkowski, C.; et al. Comparison of CHADS2, R2CHADS2, and CHA2DS2-VASc scores for the prediction of rhythm outcomes after catheter ablation of atrial fibrillation: the Leipzig Heart Center AF Ablation Registry. Circ. Arrhythm. Electrophysiol. 2014, 7, 281–287. [Google Scholar] [CrossRef]
- Watanabe, H.; Watanabe, T.; Sasaki, S.; Nagai, K.; Roden, D.M.; Aizawa, Y. Close bidirectional relationship between chronic kidney disease and atrial fibrillation: the Niigata preventive medicine study. Am. Heart J. 2009, 158, 629–636. [Google Scholar] [CrossRef]
- Alonso, A.; Lopez, F.L.; Matsushita, K.; Loehr, L.R.; Agarwal, S.K.; Chen, L.Y.; Soliman, E.Z.; Astor, B.C.; Coresh, J. Chronic Kidney Disease Is Associated With the Incidence of Atrial Fibrillation: The Atherosclerosis Risk in Communities (ARIC) Study. Circulation 2011, 123, 2946–2953. [Google Scholar] [CrossRef]
- Bansal, N.; Fan, D.; Hsu, C.-Y.; Ordonez, J.D.; Marcus, G.M.; Go, A.S. Incident Atrial Fibrillation and Risk of End-Stage Renal Disease in Adults With Chronic Kidney Disease. Circulation 2013, 127, 569–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, Y.C.; Proietti, M.; Guiducci, E.; Blann, A.D.; Lip, G.Y.H. Atrial Fibrillation and Thromboembolism in Patients With Chronic Kidney Disease. J. Am. Coll. Cardiol. 2016, 68, 1452–1464. [Google Scholar] [CrossRef] [PubMed]
- Wetmore, J.B.; Mahnken, J.D.; Rigler, S.K.; Ellerbeck, E.F.; Mukhopadhyay, P.; Spertus, J.A.; Hou, Q.; Shireman, T.I. The prevalence of and factors associated with chronic atrial fibrillation in Medicare/Medicaid-eligible dialysis patients. Kidney Int. 2012, 81, 469–476. [Google Scholar] [CrossRef] [Green Version]
- Herzog, C.A.; Asinger, R.W.; Berger, A.K.; Charytan, D.M.; Díez, J.; Hart, R.G.; Eckardt, K.-U.; Kasiske, B.L.; McCullough, P.A.; Passman, R.S.; et al. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011, 80, 572–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wizemann, V.; Tong, L.; Satayathum, S.; Disney, A.; Akiba, T.; Fissell, R.B.; Kerr, P.G.; Young, E.W.; Robinson, B.M. Atrial fibrillation in hemodialysis patients: clinical features and associations with anticoagulant therapy. Kidney Int. 2010, 77, 1098–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovesi, S.; Pogliani, D.; Faini, A.; Valsecchi, M.G.; Riva, A.; Stefani, F.; Acquistapace, I.; Stella, A.; Bonforte, G.; DeVecchi, A.; et al. Prevalence of atrial fibrillation and associated factors in a population of long-term hemodialysis patients. Am. J. Kidney Dis. 2005, 46, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Fujii, H.; Kim, J.-I.; Yoshiya, K.; Nishi, S.; Fukagawa, M. Clinical Characteristics and Cardiovascular Outcomes of Hemodialysis Patients with Atrial Fibrillation: A Prospective Follow-Up Study. Am. J. Nephrol. 2011, 34, 126–134. [Google Scholar] [CrossRef]
- Winkelmayer, W.C.; Patrick, A.R.; Liu, J.; Brookhart, M.A.; Setoguchi, S. The Increasing Prevalence of Atrial Fibrillation among Hemodialysis Patients. J. Am. Soc. Nephrol. 2011, 22, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.-T.; Lai, L.-P.; Lin, J.-L.; Chiang, F.-T.; Hwang, J.-J.; Ritchie, M.D.; Moore, J.H.; Hsu, K.-L.; Tseng, C.-D.; Liau, C.-S.; et al. Renin-angiotensin system gene polymorphisms and atrial fibrillation. Circulation 2004, 109, 1640–1646. [Google Scholar] [CrossRef]
- Chang, S.-L.; Chen, Y.-C.; Yeh, Y.-H.; Lai, Y.-J.; Yeh, H.-I.; Lin, C.-I.; Lin, Y.-K.; Lin, Y.-J.; Wu, T.-J.; Huang, Y.-K.; et al. Heart failure enhances arrhythmogenesis in pulmonary veins. Clin. Exp. Pharmacol. Physiol. 2011, 38, 666–674. [Google Scholar] [CrossRef]
- Chen, S.-C.; Chang, J.-M.; Liu, W.-C.; Huang, J.-C.; Tsai, J.-C.; Lin, M.-Y.; Su, H.-M.; Hwang, S.-J.; Chen, H.-C. Echocardiographic parameters are independently associated with increased cardiovascular events in patients with chronic kidney disease. Nephrol. Dial. Transplant 2012, 27, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Naruse, Y.; Tada, H.; Sekiguchi, Y.; Machino, T.; Ozawa, M.; Yamasaki, H.; Igarashi, M.; Kuroki, K.; Itoh, Y.; Murakoshi, N.; et al. Concomitant chronic kidney disease increases the recurrence of atrial fibrillation after catheter ablation of atrial fibrillation: a mid-term follow-up. Hear. Rhythm 2011, 8, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, M.; Yamane, T.; Matsuo, S.; Ito, K.; Narui, R.; Hioki, M.; Tanigawa, S. -i.; Nakane, T.; Yamashita, S.; Inada, K.; et al. Relationship between renal function and the risk of recurrent atrial fibrillation following catheter ablation. Heart 2011, 97, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, S.; Inden, Y.; Kato, H.; Fujii, A.; Mizutani, Y.; Ito, T.; Kamikubo, Y.; Kanzaki, Y.; Ando, M.; Hirai, M.; et al. Impaired renal function is associated with recurrence after cryoballoon catheter ablation for paroxysmal atrial fibrillation: A potential effect of non-pulmonary vein foci. J. Cardiol. 2017, 69, 3–10. [Google Scholar] [CrossRef]
- Raff, A.C.; Meyer, T.W.; Hostetter, T.H. New insights into uremic toxicity. Curr. Opin. Nephrol. Hypertens. 2008, 17, 560–565. [Google Scholar] [CrossRef]
- Sun, C.-Y.; Chang, S.-C.; Wu, M.-S. Uremic toxins induce kidney fibrosis by activating intrarenal renin-angiotensin-aldosterone system associated epithelial-to-mesenchymal transition. PLoS One 2012, 7, e34026. [Google Scholar] [CrossRef]
- Lekawanvijit, S.; Adrahtas, A.; Kelly, D.J.; Kompa, A.R.; Wang, B.H.; Krum, H. Does indoxyl sulfate, a uraemic toxin, have direct effects on cardiac fibroblasts and myocytes? Eur. Heart J. 2010, 31. [Google Scholar] [CrossRef]
- Peng, Y.-S.; Lin, Y.-T.; Wang, S.-D.; Hung, K.-Y.; Chen, Y.; Wang, S.-M. P-cresol induces disruption of cardiomyocyte adherens junctions. Toxicology 2013, 306, 176–184. [Google Scholar] [CrossRef]
- Lekawanvijit, S.; Kompa, A.R.; Manabe, M.; Wang, B.H.; Langham, R.G.; Nishijima, F.; Kelly, D.J.; Krum, H. Chronic kidney disease-induced cardiac fibrosis is ameliorated by reducing circulating levels of a non-dialysable uremic toxin, indoxyl sulfate. PLoS One 2012, 7, e41281. [Google Scholar] [CrossRef]
- Miyazaki, T.; Ise, M.; Hirata, M.; Endo, K.; Ito, Y.; Seo, H.; Niwa, T. Indoxyl sulfate stimulates renal synthesis of transforming growth factor-beta 1 and progression of renal failure. Kidney Int. Suppl. 1997, 63, S211–S214. [Google Scholar]
- Ito, S.; Yoshida, M. Protein-Bound Uremic Toxins: New Culprits of Cardiovascular Events in Chronic Kidney Disease Patients. Toxins (Basel) 2014, 6, 665–678. [Google Scholar] [CrossRef] [PubMed]
- Lekawanvijit, S.; Kompa, A.R.; Wang, B.H.; Kelly, D.J.; Krum, H. Cardiorenal syndrome: the emerging role of protein-bound uremic toxins. Circ. Res. 2012, 111, 1470–1483. [Google Scholar] [CrossRef] [PubMed]
- Dou, L.; Sallée, M.; Cerini, C.; Poitevin, S.; Gondouin, B.; Jourde-Chiche, N.; Fallague, K.; Brunet, P.; Calaf, R.; Dussol, B.; et al. The cardiovascular effect of the uremic solute indole-3 acetic acid. J. Am. Soc. Nephrol. 2015, 26, 876–887. [Google Scholar] [CrossRef] [PubMed]
- Lekawanvijit, S. Cardiotoxicity of Uremic Toxins: A Driver of Cardiorenal Syndrome. Toxins (Basel) 2018, 10, 352. [Google Scholar] [CrossRef]
- Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A. European Uremic Toxin Work Group (EUTox) Serum Indoxyl Sulfate Is Associated with Vascular Disease and Mortality in Chronic Kidney Disease Patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef]
- Lin, C.-J.; Liu, H.-L.; Pan, C.-F.; Chuang, C.-K.; Jayakumar, T.; Wang, T.-J.; Chen, H.-H.; Wu, C.-J. Indoxyl sulfate predicts cardiovascular disease and renal function deterioration in advanced chronic kidney disease. Arch. Med. Res. 2012, 43, 451–456. [Google Scholar] [CrossRef]
- Shimazu, S.; Hirashiki, A.; Okumura, T.; Yamada, T.; Okamoto, R.; Shinoda, N.; Takeshita, K.; Kondo, T.; Niwa, T.; Murohara, T. Association between indoxyl sulfate and cardiac dysfunction and prognosis in patients with dilated cardiomyopathy. Circ. J. 2013, 77, 390–396. [Google Scholar] [CrossRef]
- Sato, B.; Yoshikawa, D.; Ishii, H.; Suzuki, S.; Inoue, Y.; Takeshita, K.; Tanaka, M.; Kumagai, S.; Matsumoto, M.; Okumura, S.; et al. Relation of plasma indoxyl sulfate levels and estimated glomerular filtration rate to left ventricular diastolic dysfunction. Am. J. Cardiol. 2013, 111, 712–716. [Google Scholar] [CrossRef]
- Ng, R.R.G.; Tan, G.H.J.; Liu, W.; Ti, L.K.; Chew, S.T.H. The Association of Acute Kidney Injury and Atrial Fibrillation after Cardiac Surgery in an Asian Prospective Cohort Study. Medicine (Baltimore). 2016, 95, e3005. [Google Scholar] [CrossRef]
- Wang, W.; Hao, G.; Pan, Y.; Ma, S.; Yang, T.; Shi, P.; Zhu, Q.; Xie, Y.; Ma, S.; Zhang, Q.; et al. Serum indoxyl sulfate is associated with mortality in hospital-acquired acute kidney injury: a prospective cohort study. BMC Nephrol. 2019, 20, 57. [Google Scholar] [CrossRef]
- Chen, Y.; Harty, G.J.; Zheng, Y.; Iyer, S.R.; Sugihara, S.; Sangaralingham, S.J.; Ichiki, T.; Grande, J.P.; Lee, H.-C.; Wang, X.; et al. CRRL269. Circ. Res. 2019, 124, 1462–1472. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.; Teshima, Y.; Kondo, H.; Saito, S.; Fukui, A.; Fukunaga, N.; Nawata, T.; Shimada, T.; Takahashi, N.; Shibata, H. Role of Indoxyl Sulfate as a Predisposing Factor for Atrial Fibrillation in Renal Dysfunction. J. Am. Heart Assoc. 2015, 4, e002023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CHEN, W.-T.; CHEN, Y.-C.; HSIEH, M.-H.; HUANG, S.-Y.; KAO, Y.-H.; CHEN, Y.-A.; LIN, Y.-K.; CHEN, S.-A.; CHEN, Y.-J. The Uremic Toxin Indoxyl Sulfate Increases Pulmonary Vein and Atrial Arrhythmogenesis. J. Cardiovasc. Electrophysiol. 2015, 26, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Yamagami, F.; Tajiri, K.; Doki, K.; Hattori, M.; Honda, J.; Aita, S.; Harunari, T.; Yamasaki, H.; Murakoshi, N.; Sekiguchi, Y.; et al. Indoxyl Sulphate is Associated with Atrial Fibrillation Recurrence after Catheter Ablation. Sci. Rep. 2018, 8, 17276. [Google Scholar] [CrossRef]
- Al Za’abi, M.; Ali, B.; Al Toubi, M. HPLC-fluorescence method for measurement of the uremic toxin indoxyl sulfate in plasma. J. Chromatogr. Sci. 2013, 51, 40–43. [Google Scholar] [CrossRef]
- Asai, M.; Kumakura, S.; Kikuchi, M. Review of the efficacy of AST-120 (KREMEZIN®) on renal function in chronic kidney disease patients. Ren. Fail. 2019, 41, 47–56. [Google Scholar] [CrossRef]
- Miyazaki, T.; Aoyama, I.; Ise, M.; Seo, H.; Niwa, T. An oral sorbent reduces overload of indoxyl sulphate and gene expression of TGF-β1 in uraemic rat kidneys. Nephrol. Dial. Transplant. 2000, 15, 1773–1781. [Google Scholar] [CrossRef]
- Aoyama, I.; Shimokata, K.; Niwa, T. An oral adsorbent downregulates renal expression of genes that promote interstitial inflammation and fibrosis in diabetic rats. Nephron 2002, 92, 635–651. [Google Scholar] [CrossRef]
- Schulman, G.; Agarwal, R.; Acharya, M.; Berl, T.; Blumenthal, S.; Kopyt, N. A multicenter, randomized, double-blind, placebo-controlled, dose-ranging study of AST-120 (Kremezin) in patients with moderate to severe CKD. Am. J. Kidney Dis. 2006, 47, 565–577. [Google Scholar] [CrossRef]
- Aoyama, I.; Niwa, T. An oral adsorbent ameliorates renal overload of indoxyl sulfate and progression of renal failure in diabetic rats. Am. J. Kidney Dis. 2001, 37, S7–S12. [Google Scholar] [CrossRef]
- Konishi, K.; Nakano, S.; Tsuda, S.; Nakagawa, A.; Kigoshi, T.; Koya, D. AST-120 (Kremezin®) initiated in early stage chronic kidney disease stunts the progression of renal dysfunction in type 2 diabetic subjects. Diabetes Res. Clin. Pract. 2008, 81, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Kawagoe, Y.; Matsuda, T.; Ueda, Y.; Shimada, N.; Ebihara, I.; Koide, H. Oral ADSORBENT AST-120 decreases carotid intima-media thickness and arterial stiffness in patients with chronic renal failure. Kidney Blood Press. Res. 2004, 27, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Shoji, T.; Wada, A.; Inoue, K.; Hayashi, D.; Tomida, K.; Furumatsu, Y.; Kaneko, T.; Okada, N.; Fukuhara, Y.; Imai, E.; et al. Prospective randomized study evaluating the efficacy of the spherical adsorptive carbon AST-120 in chronic kidney disease patients with moderate decrease in renal function. Nephron. Clin. Pract. 2007, 105, c99–107. [Google Scholar] [CrossRef] [PubMed]
- Akizawa, T.; Asano, Y.; Morita, S.; Wakita, T.; Onishi, Y.; Fukuhara, S.; Gejyo, F.; Matsuo, S.; Yorioka, N.; Kurokawa, K.; et al. Effect of a carbonaceous oral adsorbent on the progression of CKD: a multicenter, randomized, controlled trial. Am. J. Kidney Dis. 2009, 54, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Schulman, G.; Berl, T.; Beck, G.J.; Remuzzi, G.; Ritz, E.; Arita, K.; Kato, A.; Shimizu, M. Randomized Placebo-Controlled EPPIC Trials of AST-120 in CKD. J. Am. Soc. Nephrol. 2015, 26, 1732–1746. [Google Scholar] [CrossRef]
- Cha, R.-H.; Kang, S.W.; Park, C.W.; Cha, D.R.; Na, K.Y.; Kim, S.G.; Yoon, S.A.; Han, S.Y.; Chang, J.H.; Park, S.K.; et al. A Randomized, Controlled Trial of Oral Intestinal Sorbent AST-120 on Renal Function Deterioration in Patients with Advanced Renal Dysfunction. Clin. J. Am. Soc. Nephrol. 2016, 11, 559–567. [Google Scholar] [CrossRef] [Green Version]
- Hogas, S.M.; Voroneanu, L.; Serban, D.N.; Segall, L.; Hogas, M.M.; Serban, I.L.; Covic, A. Methods and potential biomarkers for the evaluation of endothelial dysfunction in chronic kidney disease: a critical approach. J. Am. Soc. Hypertens. 2010, 4, 116–127. [Google Scholar] [CrossRef]
- Namikoshi, T.; Tomita, N.; Satoh, M.; Sakuta, T.; Kuwabara, A.; Kobayashi, S.; Higuchi, Y.; Nishijima, F.; Kashihara, N. Oral adsorbent AST-120 ameliorates endothelial dysfunction independent of renal function in rats with subtotal nephrectomy. Hypertens. Res. 2009, 32, 194–200. [Google Scholar] [CrossRef]
- Yamamoto, S.; Zuo, Y.; Ma, J.; Yancey, P.G.; Hunley, T.E.; Motojima, M.; Fogo, A.B.; Linton, M.F.; Fazio, S.; Ichikawa, I.; et al. Oral activated charcoal adsorbent (AST-120) ameliorates extent and instability of atherosclerosis accelerated by kidney disease in apolipoprotein E-deficient mice. Nephrol. Dial. Transplant 2011, 26, 2491–2497. [Google Scholar] [CrossRef] [Green Version]
- Niwayama, J.; Sanaka, T. Development of a new method for monitoring blood purification: the blood flow analysis of the head and foot by laser Doppler blood flowmeter during hemodialysis. Hemodial. Int. 2005, 9, 56–62. [Google Scholar] [CrossRef]
- Ryu, J.-H.; Yu, M.; Lee, S.; Ryu, D.-R.; Kim, S.-J.; Kang, D.-H.; Choi, K.B. AST-120 Improves Microvascular Endothelial Dysfunction in End-Stage Renal Disease Patients Receiving Hemodialysis. Yonsei Med. J. 2016, 57, 942. [Google Scholar] [CrossRef] [PubMed]
- Fujii, H.; Nishijima, F.; Goto, S.; Sugano, M.; Yamato, H.; Kitazawa, R.; Kitazawa, S.; Fukagawa, M. Oral charcoal adsorbent (AST-120) prevents progression of cardiac damage in chronic kidney disease through suppression of oxidative stress. Nephrol. Dial. Transplant. 2009, 24, 2089–2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwahara, M.; Bannai, K.; Segawa, H.; Miyamoto, K.; Yamato, H. Cardiac remodeling associated with protein increase and lipid accumulation in early-stage chronic kidney disease in rats. Biochim. Biophys. Acta - Mol. Basis Dis. 2014, 1842, 1433–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakai, K.; Fujii, H.; Kono, K.; Goto, S.; Fukagawa, M.; Nishi, S. Effects of AST-120 on left ventricular mass in predialysis patients. Am. J. Nephrol. 2011, 33, 218–223. [Google Scholar] [CrossRef]
- Asanuma, H.; Chung, H.; Ito, S.; Min, K.-D.; Ihara, M.; Takahama, H.; Funayama, M.; Imazu, M.; Fukuda, H.; Ogai, A.; et al. AST-120, an Adsorbent of Uremic Toxins, Improves the Pathophysiology of Heart Failure in Conscious Dogs. Cardiovasc. Drugs Ther. 2019, 33, 277–286. [Google Scholar] [CrossRef]
Figure 1.
Role of indoxyl sulfate (IS) in the progression of atrial fibrillation (AF). IS induces oxidative stress and promotes arrhythmogenesis in the pulmonary vein and atrium. In the pulmonary vein, IS induces an increased occurrence of delayed after-depolarizations, burst firing, and increased calcium leakage. In the atrium, IS shortens the action potential duration. IS also induces inflammation and fibrosis in the atrium, which leads to conduction time prolongation. These IS effects on the pulmonary vein and atrium exacerbates the development of AF substrates through increased ectopic firing and re-entry circuits in atrial substrates.
Figure 1.
Role of indoxyl sulfate (IS) in the progression of atrial fibrillation (AF). IS induces oxidative stress and promotes arrhythmogenesis in the pulmonary vein and atrium. In the pulmonary vein, IS induces an increased occurrence of delayed after-depolarizations, burst firing, and increased calcium leakage. In the atrium, IS shortens the action potential duration. IS also induces inflammation and fibrosis in the atrium, which leads to conduction time prolongation. These IS effects on the pulmonary vein and atrium exacerbates the development of AF substrates through increased ectopic firing and re-entry circuits in atrial substrates.

Figure 2.
Impact of indoxyl sulfate (IS) levels on the atrial fibrillation (AF) recurrence in patients undergoing radiofrequency catheter ablation. The 1-year AF-free survival is shown according to IS levels. The numbers at the bottom of the graph shows the number of ‘at risk’ patients in each follow-up month. Reproduced from [64], 2018, Springer Nature.
Figure 2.
Impact of indoxyl sulfate (IS) levels on the atrial fibrillation (AF) recurrence in patients undergoing radiofrequency catheter ablation. The 1-year AF-free survival is shown according to IS levels. The numbers at the bottom of the graph shows the number of ‘at risk’ patients in each follow-up month. Reproduced from [64], 2018, Springer Nature.

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yamagami, F.; Tajiri, K.; Yumino, D.; Ieda, M. Uremic Toxins and Atrial Fibrillation: Mechanisms and Therapeutic Implications. Toxins 2019, 11, 597. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11100597
AMA Style
Yamagami F, Tajiri K, Yumino D, Ieda M. Uremic Toxins and Atrial Fibrillation: Mechanisms and Therapeutic Implications. Toxins. 2019; 11(10):597. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11100597
Chicago/Turabian StyleYamagami, Fumi, Kazuko Tajiri, Dai Yumino, and Masaki Ieda. 2019. "Uremic Toxins and Atrial Fibrillation: Mechanisms and Therapeutic Implications" Toxins 11, no. 10: 597. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11100597
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.