Botulinum Toxin Therapy Combined with Rehabilitation for Stroke: A Systematic Review of Effect on Motor Function

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
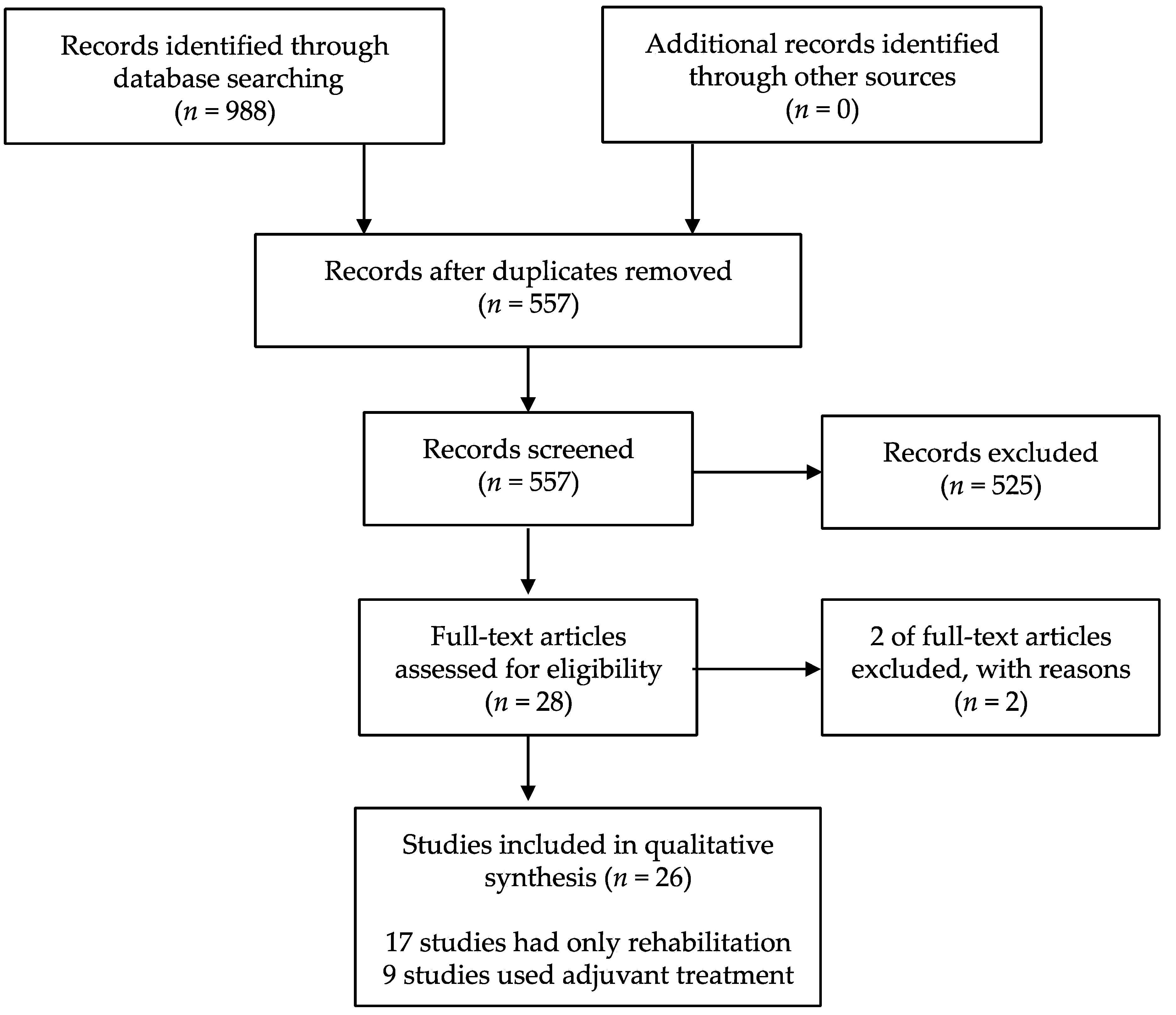
2.1. Study Selection
2.2. Description of Studies
2.3. Risk of Bias Assessment
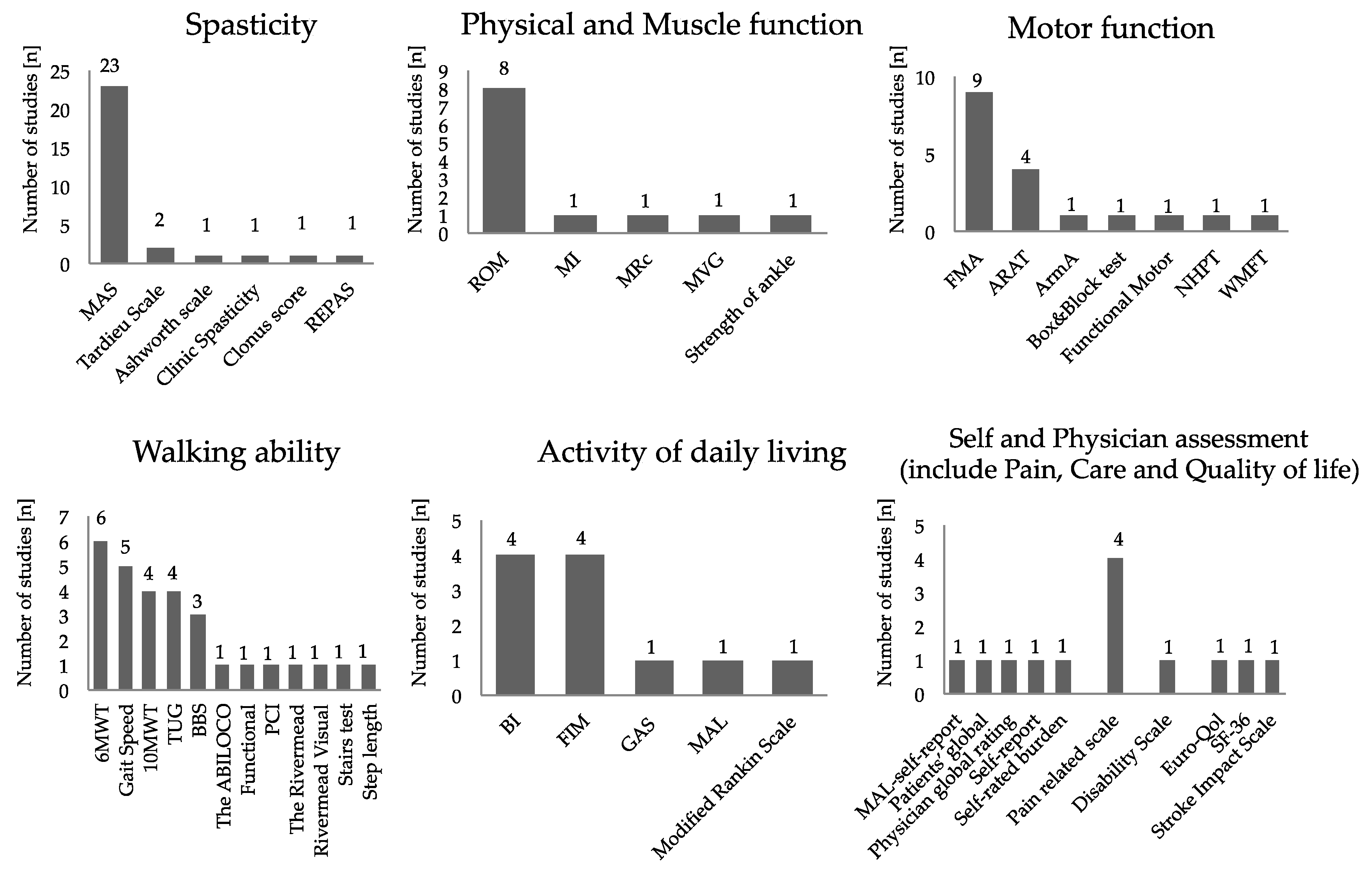
2.4. Outcome Measure
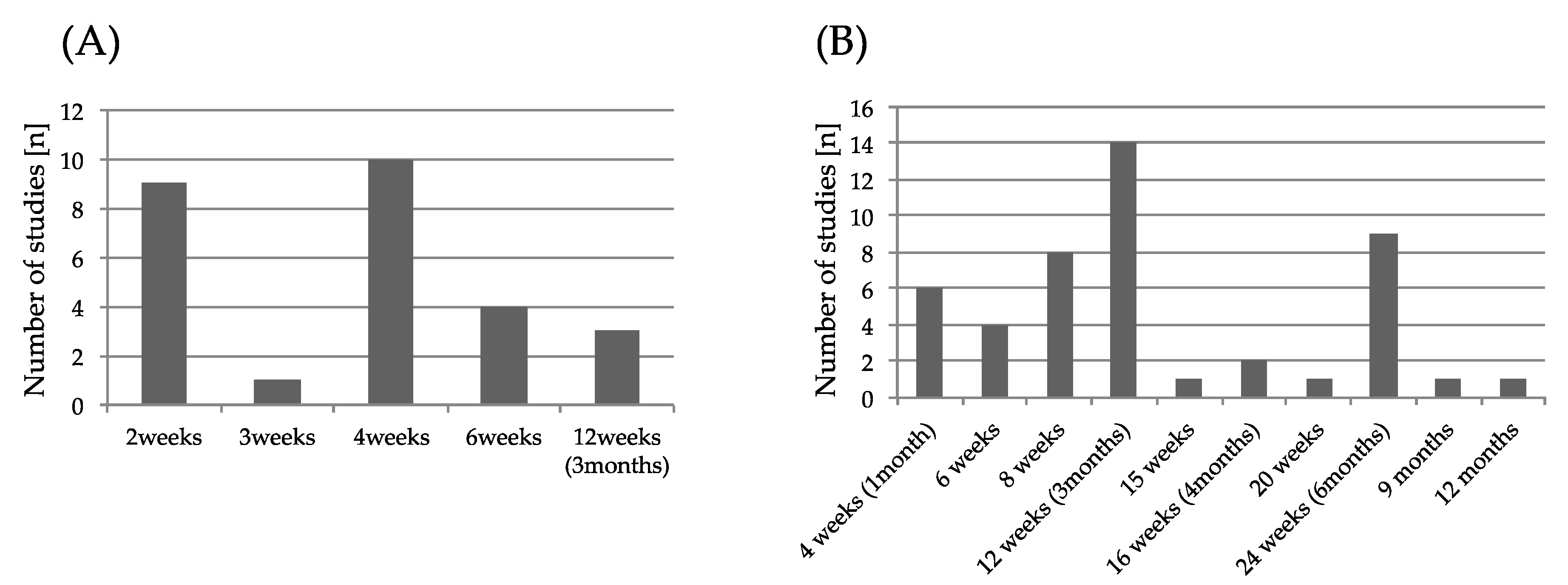
2.5. Intervention in BoNT-A Therapy
2.6. Rehabilitation
2.7. Effect of BoNT-A and Rehabilitation of Motor Function
3. Discussion
4. Conclusions and Future Perspective
5. Methods
5.1. Criteria for Considering Studies for Review
5.1.1. Type of Studies
5.1.2. Type of Participants
5.1.3. Type of Interventions and Comparisons
5.1.4. Search Strategy
5.2. Date Collection and Analysis
5.2.1. Selection of Studies
5.2.2. Date Extraction
5.2.3. Assessment of Risk of Bias in the Included Studies
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Mayer, N.H. Clinicophysiologic concepts of spasticity and motor dysfunction in adults with an upper motoneuron lesion. Muscle Nerve Suppl. 1997, 6, S1–S13. [Google Scholar] [CrossRef]
- Sommerfeld, D.K.; Eek, E.U.; Svensson, A.K.; Holmqvist, L.W.; von Arbin, M.H. Spasticity after stroke: Its occurrence and association with motor impairments and activity limitations. Stroke 2004, 35, 134–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watkins, C.L.; Leathley, M.J.; Gregson, J.M.; Moore, A.P.; Smith, T.L.; Sharma, A.K. Prevalence of spasticity post stroke. Clin. Rehabil. 2002, 16, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Schinwelsk, M.; Sławek, J. Prevalence of spasticity following stroke and its impact on quality of life with emphasis on disability in activities of daily living. Systematic review. Neurol. Neurochir. 2010, 44, 404–411. [Google Scholar] [CrossRef]
- Kimura, A.; Abo, M.; Kawate, N.; Osako, Y.; Suyama, K.; Maeda, T.; Uechi, Y.; Iwasaki, M. Efficacy and Safety of Botulinum Toxin Type A in treating Lower Limb Spasticity in Post-stroke Patients: A Multicenter, Double-blind, Placebo-controlled Trial followed by an Open-label Trial. Jpn. J. Rehabil. Med. 2010, 47, 626–636. [Google Scholar] [CrossRef] [Green Version]
- Tanikawa, H.; Kagaya, H.; Saitoh, E.; Ozaki, K.; Hirano, S.; Itoh, N.; Yamada, J.; Kanada, Y. Efficacy of Botulinum Toxin A Treatment for Pes Varus during Gait. J. Stroke Cerebrovasc. Dis. 2015, 24, 2416–2422. [Google Scholar] [CrossRef]
- Brin, M.F. Botulinum toxin: Chemistry, pharmacology, toxicity and immunology. Muscle Nerve Suppl. 1997, 6, 146–168. [Google Scholar] [CrossRef]
- Boyd, R.N.; Pliatsios, V.; Starr, R.; Wolfe, R.; Graham, H.K. Biomechanical transformation of the gastroc-soleus muscle with botulinum toxin A in children with cerebral palsy. Dev. Med. Child Neurol. 2000, 42, 32–41. [Google Scholar] [CrossRef]
- Elia, A.E.; Filippini, G.; Calandrella, D.; Albanese, A. Botulinum Neurotoxin for Post-Stroke Spasticity in Adults: A Systematic Review. Mov. Disord. Soc. 2009, 24, 801–812. [Google Scholar] [CrossRef]
- Rosales, R.L.; Chua-Yap, A.S. Evidence-based systematic review on the efficacy and safety of botulinum toxin-A therapy in post-stroke spasticity. J. Neural Transm. 2008, 115, 617–623. [Google Scholar] [CrossRef]
- Naumann, M.; Albanese, A.; Heinen, F.; Molenaers, G.; Relja, M. Safety and efficacy of botulinum toxin type A following long-term use. Eur. J. Neurol. 2006, 13, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.F.; Brashear, A.; Elovic, E.; Kassicieh, D.; Marciniak, C.; Liu, J.; Turkel, C. Repeated dosing of botulinum toxin type A for upper limb spasticity following stroke. Neurology 2004, 63, 1971–1973. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Gracies, J.M.; Graham, H.K.; Miyasaki, J.M.; Naumann, M.; Russman, B.; Simpson, L.L.; So, Y. Assessment: Botulinum neurotoxin for the treatment of spasticity (an evidence-based review) Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2008, 70, 1691–1698. [Google Scholar] [PubMed] [Green Version]
- Bakheit, A.M.; Zakine, B.; Maisonobe, P.; Aymard, C.; Fhedoroff, K.; Hefter, H.; Jacinto, J.; Jost, W.H.; Molteni, F.; Stam, H.; et al. The profile of patients and current practice of treatment of upper limb muscle spasticity with botulinum toxin type A: An international survey. Int. J. Rehabil. Res. 2010, 33, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Hara, T.; Abo, M.; Hara, H.; Kobayashi, K.; Shimamoto, Y.; Samizo, Y.; Sasaki, N.; Yamada, N.; Niimi, M. Effects of botulinum toxin A therapy and multidisciplinary rehabilitation on upper and lower limb spasticity in post-stroke patients. Int. J. Neurosci. 2017, 127, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Hara, T.; Abo, M.; Hara, H.; Kobayashi, K.; Shimamoto, Y.; Shibata, Y.; Sasaki, N.; Yamada, N.; Niimi, M. Effects of botulinum toxin A therapy and multidisciplinary rehabilitation on lower limb spasticity classified by spastic muscle echo intensity in post-stroke patients. Int. J. Neurosci. 2018, 128, 412–420. [Google Scholar] [CrossRef]
- Hara, T.; Abo, M.; Hara, H.; Sasaki, N.; Yamada, N.; Niimi, M.; Shimamoto, Y. The Effect of Repeated Botulinum Toxin A Therapy Combined with Intensive Rehabilitation on Lower Limb Spasticity in Post-Stroke Patients. Toxins (Basel) 2018, 31, 10. [Google Scholar] [CrossRef] [Green Version]
- Uchiyama, Y.; Koyama, T.; Wada, Y.; Katsutani, M.; Kodama, N.; Domen, K. Botulinum Toxin Type A Treatment Combined with Intensive Rehabilitation for Gait Poststroke: A Preliminary. Study. J. Stroke Cerebrovasc. Dis. 2018, 27, 1975–1986. [Google Scholar] [CrossRef]
- Prazeres, A.; Lira, M.; Aguiar, P.; Monteiro, L.; Vilasbôas, Í.; Melo, A. Efficacy of physical therapy associated with botulinum toxin type A on functional performance in post-stroke spasticity: A randomized, double-blinded, placebo-controlled trial. Neurol. Int. 2018, 10, 7385. [Google Scholar] [CrossRef]
- Umar, M.; Masood, T.; Badshah, M. Effect of botulinum toxin A&task-specific training on upper limb function in post-stroke focaldystonia. J. Pak. Med. Assoc. 2018, 68, 526–531. [Google Scholar]
- Devier, D.; Harnar, J.; Lopez, L.; Brashesr, A.; Graham, G. Rehabilitation plus OnabotulinumtoxinA Improves Motor Function over OnabotulinumtoxinA Alone in Post-Stroke Upper Limb Spasticity: A Single-Blind, Randomized Trial. Toxins (Basel) 2017, 11, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roche, N.; Zory, R.; Sauthier, A.; Bonnyaud, C.; Pradon, D.; Bensmail, D. Effect of rehabilitation and botulinum toxin injection on gait in chronic stroke patients: A randomized controlled study. J. Rehabil. Med. 2015, 47, 31–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, X.D.; Zhang, G.B.; Chen, H.X.; Wang, W.; Song, J.H.; Fu, D.G. Color Doppler ultrasound-guided botulinum toxin type A injection combined with an ankle footbrace for treating lower limb spasticity after a stroke. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 406–411. [Google Scholar] [PubMed]
- Tao, W.; Yan, D.; Li, J.H.; Shi, Z.H. Gait improvement by low-dose botulinum toxin A injection treatment of the lower limbs in subacute stroke patients. J. Phys. Ther. Sci. 2015, 27, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Demetrios, M.; Gorelik, A.; Louie, J.; Brand, C.; Baguley, I.J.; Khan, F. Outcomes of ambulatory rehabilitation programmes following botulinum toxin for spasticity in adults with stroke. J. Rehabil. Med. 2014, 46, 730–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimentel, L.H.; Alencar, F.J.; Rodrigues, L.R.; Sousa, F.C.; Teles, J.B. Effects of botulinum toxin type A for spastic foot in post-stroke patients enrolled in a rehabilitationprogram. Arq. Neuropsiquiatr. 2014, 72, 28–32. [Google Scholar] [CrossRef]
- Rosales, R.L.; Kong, K.H.; Goh, K.J.; Kumthornthip, W.; Mok, V.C.; Delgado-De Los Santos, M.M.; Chua, K.S.; Abdullah, S.J.; Zakine, B.; Maisonobe, P.; et al. Botulinum toxin injection for hypertonicity of the upper extremity within 12 weeks after stroke: A randomized controlled trial. Neurorehabil. Neural Repair 2012, 26, 812–821. [Google Scholar] [CrossRef]
- Hesse, S.; Mach, H.; Fröhlich, S.; Behrend, S.; Werner, C.; Melzer, I. An early botulinum toxin A treatment in subacute stroke patients may prevent a disabling fingerflexor stiffness six months later: A randomized controlled trial. Clin. Rehabil. 2012, 26, 237–245. [Google Scholar] [CrossRef]
- Wolf, S.L.; Milton, S.B.; Reiss, A.; Easley, K.A.; Shenvi, N.V.; Clark, P.C. Further assessment to determine the additive effect of botulinum toxin type A on an upperextremity exercise program to enhance function among individuals with chronic stroke but extensor capability. Arch. Phys. Med. Rehabil. 2012, 93, 578–587. [Google Scholar] [CrossRef]
- Shaw, L.C.; Price, C.I.; van Wijck, F.M.; Shackley, P.; Steen, N.; Barnes, M.P.; Ford, G.A.; Graham, L.A.; Rodgers, H. BoTULS Investigators. Botulinum Toxin for the Upper Limb after Stroke (BoTULS) Trial: Effect on impairment, activitylimitation, and pain. Stroke 2011, 42, 1371–1379. [Google Scholar] [CrossRef] [Green Version]
- Shaw, L.; Rodgers, H.; Price, C.; van Wijck, F.; Shackley, P.; Steen, N.; Barnes, M.; Ford, G.; Graham, L. BoTULS investigators. BoTULS: A multicentre randomised controlled trial to evaluate the clinical effectiveness and cost-effectiveness of treating upper limb spasticity due to stroke with botulinum toxin type A. Health Technol. Assess. 2010, 14, 1–113. [Google Scholar] [CrossRef] [PubMed]
- Meythaler, J.M.; Vogtle, L.; Brunner, R.C. A preliminary assessment of the benefits of the addition of botulinum toxin a to a conventionaltherapy program on the function of people with longstanding stroke. Arch. Phys. Med. Rehabil. 2009, 90, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.Y.; Koh, J.H.; Paik, N.J. Intramuscular botulinum toxin-A reduces hemiplegic shoulder pain: A randomized, double-blind, comparative study versus intraarticular triamcinolone acetonide. Stroke 2008, 39, 126–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suputtitada, A.; Suwanwela, N.C. The lowest effective dose of botulinum A toxin in adult patients with upper limb spasticity. Disabil. Rehabil. 2005, 27, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Burbaud, P.; Wiart, L.; Dubos, J.L.; Gaujard, E.; Debelleix, X.; Joseph, P.A.; Mazaux, J.M.; Bioulac, B.; Barat, M.; Lagueny, A. A randomised, double blind, placebo controlled trial of botulinum toxin in the treatment of spasticfoot in hemiparetic patients. J. Neurol. Neurosurg. Psychiatry 1996, 61, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, K.; Miaki, H.; Hori, H.; Kobayashi, Y.; Nakagawa, T. How effective is physicaltherapy for gait muscle activity in hemiparetic patients who receive botulinum toxin injections? Eur. J. Phys. Rehabil. Med. 2019, 55, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.J.; Skidmore, E.R.; Niyonkuru, C.; Chang, C.L.; Huber, L.M.; Munin, M.C. Cyclic functional electrical stimulation does not enhance gains in hand grasp function when used as an adjunct to onabotulinumtoxinA and task practice therapy: A single-blind, randomized controlled pilot study. Arch. Phys. Med. Rehabil. 2010, 91, 679–686. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.A.; Wood, D.E.; Swain, I.D.; Tromans, A.M.; Strike, P.; Burridge, J.H. A pilot study to investigate the combined use of botulinum neurotoxin type a and functionalelectrical stimulation, with physiotherapy, in the treatment of spastic dropped foot in subacutestroke. Artif. Organs 2002, 26, 263–266. [Google Scholar] [CrossRef]
- Johnson, C.A.; Burridge, J.H.; Strike, P.W.; Wood, D.E.; Swain, I.D. The effect of combined use of botulinum toxin type A and functional electric stimulation in the treatment of spastic drop foot after stroke: A preliminary investigation. Arch. Phys. Med. Rehabil. 2004, 85, 902–909. [Google Scholar] [CrossRef]
- Erbil, D.; Tugba, G.; Murat, T.H.; Melike, A.; Merve, A.; Cagla, K.; Mehmetali, Ç.C.; Akay, Ö.; Nigar, D. Effects of robot-assisted gait training in chronic stroke patients treated by botulinum toxin-a: A pivotal study. Physiother. Res. Int. 2018, 23, e1718. [Google Scholar] [CrossRef]
- Picelli, A.; Bacciga, M.; Melotti, C.L.A.; Marchina, E.; Verzini, E.; Ferrari, F.; Pontillo, A.; Corradi, J.; Tamburin, S.; Saltuari, L.; et al. Combined effects of robot-assisted gait training and botulinum toxin type A on spastic equinus foot in patients with chronic stroke: A pilot, single blind, randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2016, 52, 759–766. [Google Scholar] [PubMed]
- Pennati, G.V.; Da Re, C.; Messineo, I.; Bonaiuti, D. How could robotic training and botolinum toxin be combined in chronic post stroke upper limbspasticity? A pilot study. Eur. J. Phys. Rehabil. Med. 2015, 51, 381–387. [Google Scholar] [PubMed]
- Carda, S.; Invernizzi, M.; Baricich, A.; Cisari, C. Casting, taping or stretching after botulinum toxin type A for spastic equinus foot: A single-blindrandomized trial on adult stroke patients. Clin. Rehabil. 2011, 25, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Karadag-Saygi, E.; Cubukcu-Aydoseli, K.; Kablan, N.; Ofluoglu, D. The role of kinesiotaping combined with botulinum toxin to reduce plantar flexors spasticity afterstroke. Top. Stroke Rehabil. 2010, 17, 318–322. [Google Scholar] [CrossRef]
- Sun, S.F.; Hsu, C.W.; Sun, H.P.; Hwang, C.W.; Yang, C.L.; Wang, J.L. Combined botulinum toxin type A with modified constraint-induced movement therapy for chronicstroke patients with upper extremity spasticity: A randomized controlled study. Neurorehabil. Neural Repair 2010, 24, 34–41. [Google Scholar] [CrossRef]
- Takekawa, T.; Abo, M.; Ebihara, K.; Taguchi, K.; Sase, Y.; Kakuda, W. Long-term effects of injection of botulinum toxin type A combined with home-based functional training for post-stroke patients with spastic upper limb hemiparesis. Acta Neurol. Belg. 2013, 113, 469–475. [Google Scholar] [CrossRef]
- Phadke, C.P.; Ismail, F.; Boulias, C.; Gage, W.; Mochizuki, G. The impact of post-stroke spasticity and botulinum toxin on standing balance: A systematic review. Expert Rev. Neurother. 2014, 14, 319–327. [Google Scholar] [CrossRef]
- Foley, N.; Murie-Fernandez, M.; Speechley, M.; Salter, K.; Sequeira, K.; Teasell, R. Does the treatment of spastic equinovarus deformity following stroke with botulinum toxin increase gait velocity? A systematic review and meta-analysis. Eur. J. Neurol. 2010, 17, 1419–1427. [Google Scholar] [CrossRef]
- Picelli, A.; Lobba, D.; Midiri, A.; Prandi, P.; Melotti, C.; Baldessarelli, S.; Smania, N. Botulinum toxin injection into the forearm muscles for wrist and fingers spastic overactivity in adults with chronic stroke: A randomized controlled trial comparing three injection techniques. Clin. Rehabil. 2014, 28, 232–242. [Google Scholar] [CrossRef]
- Kaji, R.; Osako, Y.; Suyama, K.; Maeda, T.; Uechi, Y.; Iwasaki, M. GSK1358820 Spasticity Study Group. Botulinum toxin type A in post-stroke lower limb spasticity: A multicenter, double-blind, placebo-controlled trial. J. Neurol. 2010, 257, 1330–1337. [Google Scholar] [CrossRef] [Green Version]
- Kaji, R.; Osako, Y.; Suyama, K.; Maeda, T.; Uechi, Y.; Iwasaki, M. GSK1358820 Spasticity Study Group. Botulinum toxin type A in post-stroke upper limb spasticity. Curr. Med. Res. Opin. 2010, 26, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Kinnear, B.Z.; Lannin, N.A.; Cusick, A.; Harvey, L.A.; Rawicki, B. Rehabilitation therapies after botulinum toxin-A injection to manage limb spasticity: A systematic review. Phys. Ther. 2014, 94, 1569–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundh, A.; Gøtzsche, P.C. Recommendations by Cochrane Review Groups for assessment of the risk of bias in studies. BMC Med. Res. Methodol. 2008, 8, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | Limb | Design | Sample | Sex(M:F) | Age | Time Between Onset and Treatment |
|---|---|---|---|---|---|---|---|
| Combined Rehabilitation | |||||||
| Uchiyama Y et al. 2018 [18] | Japan | Lower | Comparative study | Group1:9(BoNT-A combined PT and OT) Group2:10(Group2:First Phase: PT, OT Second Phase BoNT-A combined PT and OT) | 15:4 | Group1 57.0 (51.0–65.5), Group2:58.5 (47.0–65.6) | Group1 17.0 (11.5–39.0), Group2:35.5 (18.5–105.3) month |
| Prazeres A et al. 2018 [19] | Brazil | Both | RCT (vs Placebo injection) | I:20 C:20 | 24:16 | I:52.5(11.0) C:52.5(12.5) | I:34.1(21.4) C:32.1(14.9) months |
| Umar et al. 2018 [20] | Pakistan | Upper for focal dystonia | RCT (vs rehabilitation only) | I:23 C:23 | 26:17 | I:43.6(10.9) C:48.8(10.8) | NR |
| Devier et al. 2017 [21] | USA | Upper | RCT (vs BoNT-A only) | I:15 C:16 | 21:10 | I:58.0(6.6) C:60.9(11.0) | 6(0.5–16.5) years |
| Roche et al. 2015 [22] | France | Lower | RCT (vs BoNT-A only) | I:19 C:16 | 25:10 | I:47.8(14.4) C:51.5(13.5) | I:15.7(6.9) C:7.3(3.6) years |
| Ding et al. 2015 [23] | China | Lower | RCT (vs rehabilitation only) | I:33(BoNT-A, AFO, Conventional therapy(Co), rehabilitation) Observation:35(BoNT-A, Co, rehabilitation) C:35(Co, rehabilitation) | 49:54 | I:63.4(10.2) Observation:62.8(11.5) C:64.2(12.4) | I:17.0(1.1) Observation:16.4(1.2) C:15.4(1.8) ? |
| Tao et al. 2015 [24] | China | Lower | RCT (vs Placebo injection) | I:11 C:12 | 15:8 | I:55(12) C:58(14) | I:24.2(12.2) C:23.2(17.2) days |
| Demetrios et al. 2014 [25] | Australia | Both (Upper 40 Lower 37) | Comparative study (vs rehabilitation only) | I:28(BoNT-A, Standard Care) C:31 (Placebo, Standard Care) | 42:17 | I:60.6(48.6–65.9) C:61.4(47.8–68.6) | I:2.3(1.1–5.5) C:2.5(1.1–5.0) years |
| Pimentel et al. 2014 [26] | Brazil | Lower | RCT (300U vs 100U) | First group(300U):11 Second group(100U):12 | 10:11 | First group:50.5(6.8) Second group:47.9(3.8) | First group:41.6(63.4) Second group:34.5(33.8) months |
| Rosales et al. 2012 [27] | Philippines | Upper | RCT (vs Placebo injection) | I:83 C:80 | 109:54 | I:55.7(23–79) C:54.5(17–79) | I:7.7(3.1) C:7(2.9) weeks |
| Hesse et al. 2012 [28] | Germany | Upper | RCT (vs rehabilitation only) | I:9 C:9 | 6:12 | I:57(11) C:66(11) | I:5.8(1.3) C:5.6(1.1) weeks |
| Wolf et al. 2012 [29] | USA | Upper | RCT (vs Placebo injection) | I:13 C:12 | 15:10 | I:48.8(15.6) C:49.8(13.7) | NR |
| Shaw et al. 2011, 2010 [30,31] | UK | Upper | RCT (vs rehabilitation only) | I:170 C:162 | 225:107 | I:67(58.8–74) C:66(59.8–72.3) | I:324(128.5–1387.5) C:280(148.8–1145.8) days |
| Meythaler et al. 2009 [32] | USA | Upper | RCT with cross-over trial (12 weeks) (vs Placebo injection) | 21 | 15:6 | 53.3(14.8) | more than 6 months |
| Lim et al. 2008 [33] | Korea | Upper | RCT (vs Triamcinolone acetonide) | I:16 C:13 | 15:14 | I:64.8(2.1) C:57.1(3.6) | I:230.4(53.8) C:299.5(73.9) days |
| Suputtitada et al. 2005 [34] | Thailand | Upper | RCT (vs Placebo injection) | I:45(350U:15,500U:15,1000U:5) C:15 | 26:24 | 350U:46.5(8.5),500U:53(18.7),1000U:59.9(9.2) C:55.2(8.9) | 350U:7.9(0.9),500U:8.4(0.7),1000U:8.7(0.4) C:8.5(0.8) months |
| Burbaud et al. 1996 [35] | France | Lower | RCT with cross-over trial(90days) (vs Placebo injection) | I:10 C:13 | 16:7 | I:50.7(11) C:53.9(16) | I:23.2(36) C:23.8(33) months |
| Combined ES, FES and rehabilitation | |||||||
| Fujita et al. 2018 [36] | Japan | Lower | Non-RCT (vs BoNT-A only) | I:17(ES) C:17 | 25:9 | I:58.6(10.5) C:57.2(10.5) | I:39.8(37.7) C:75.2(51.2) months |
| Weber et al. 2010 [37] | USA | Upper | RCT (vs BoNT-A + rehabilitation) | I:10(BoNT-A FES Rehabilitation) C:13(Rehabilitation) | 8:15 | I:54.0(10.3) C:41.2(14.2) | I:9.7(8.6) C:4.3(2.5) years |
| Johnson et al. 2002, 2004 [38,39] | UK | Lower | RCT (vs rehabilitation only) | I:10(BoNT-A FES Rehabilitation) C:8(Rehabilitation) | 12:6 | I:59.3(12.5) C:58.2(12.7) | 0–6 months:9, 6–12 months:9 |
| Combined Robot and rehabilitation | |||||||
| Erbil et al. 2018 [40] | Turkey | Lower | RCT (vs BoNT-A + rehabilitation) | I:32(BoNT-A, RAT and physical therapy) C:16(BoNT-A, physical therapy) | 27:16 | I:50.1(11.8) C:48.7(10.4) | I:39(34.3) C:25.9(24.6) months |
| Picelli et al. 2016 [41] | Italy | Lower | RCT (vs BoNT-A only) | I:11(BoNT-A, RAGT) C:11(BoNT-A) | 16:6 | I:62.4(9.5) C:65.1(3.4) | I:6.2(4.2) C:6.1(3.8) years |
| Pennati et al. 2015 [42] | Italy | Upper | RCT (vs rehabilitation only) | I:7(BoNT-A, robotic training) C:8(robotic training alone) | 9:6 | 53.66(38–69) | 10 months–20 years |
| Combined Taping, Casting and rehabilitation | |||||||
| Carda S et al. 2011 [43] | Italy | Lower | RCT (vs rehabilitation only) | Taping:24, Casting:27, Stretching: 18 | 35: 34 | Taping:62.2(11.7), Casting:64.5(12.5), Stretching:59.6(14.3) | Taping:46.9(41.3), Casting:52.3(43.8), Stretching:43.9(39.6) months |
| Karadag-Saygi E et al. 2010 [44] | Turkey | Lower | RCT (vs rehabilitation only) | I:10(BoNT-A, kinesiotaping) C:10 | 12:8 | I:63.8(9) C:57.3(12) | I:35.2(29) C:39.4(30) months |
| Combined CIMT | |||||||
| Sun et al. 2010 [45] | Taiwan | Upper | RCT (vs BoNT-A + rehabilitation) | I:15(BoNT-A, CIMT) C:14(BoNT-A, convention rehabilitation) | 24:5 | I:58.7(9.9) C:61.5(9.4) | I:2.9(1.5) C:2.9(1.3) years |
| Study | BoNT-A-Dosage-Location | Rehabilitation Protocol | Assessments | Follow-up | Results |
|---|---|---|---|---|---|
| Combined Rehabilitation | |||||
| Uchiyama Y et al. 2018 [18] | BotoxⓇ 300U -Gastrocnemius, Soleus, TP, FDL | 1-h physical therapy and a 1-h occupational therapy for a total of 2 h/d and 5 d/wk.Total 4 weeks, ROM, Stretch, Gait training, Endurance training | MAS, ROM, Gait Speed, 6MWT, TUG, BBS | Group1: 4 week Group2: 4,8 week | Gait speed, 6MD, and TUG scores improved in group II. Intergroup comparisons at week 4 showed significantly greater improvements in the MAS score of ankle plantar flexor, ROM of ankle dorsiflexion, and 6MD in group I than in group II |
| Prazeres A et al. 2018 [19] | DysportⓇ -Dosage and location had no data. | 30minutes twice/week, Stretch, mobilization, flexibility, endurance and functional training. | MAS, FMA, 6MWT, TUG | 3, 6, 9 months | MAS was a significant tonus decrease in elbow flexors and wrist flexors in BoNT-A group. Motor function was significantly improved after 6 months in both group. TUG and 6MWT was improved after third month in the both groups. But, there was no difference between groups during follow-up. |
| Umar et al. 2018 [20] | DysportⓇ by EMG 350-500U - B, BB, TB, FDS, FDP, FCU, FCR, EPL, FPL | The task-specific training at one week after administration of the injections, the duration of one hour, at a frequency of three times a week for a total of 8 weeks | MAS, FMA | 4,8 weeks | Both groups showed significant improvements on MAS and FMA. no significant differences were observed between the groups at baseline, after 4 and 8 weeks of intervention. |
| Devier et al. 2017 [21] | OnabotulinumtoxinA by EMG. -Dosage and location had no data. | 24 weekly rehabilitation program. 1.5 h PT and OT included techniques such as electrical stimulation and 1h daily home exercise program between visits. | MAS, FMA, FIM, Self-report | 6, 12, 15, 18–21, 24–27 weeks | Both groups had a reduction in spasticity following injection. Intervention group was significantly improved on the Fugl–Meyer upper extremity score |
| Roche et al. 2015 [22] | BotoxⓇ by ES - Gluteus magnus, RF, Crurails, Ham, Soleus, Calf muscles, FDB, FDL -Dosage had no data. | a standardized home-based self-rehabilitation program that consisted of 3 parts (10 min each). 4 weeks. Stretch, task-oriented exercise. | MAS, the ABILOCO Scale, 10MWT, 6MWT, TUG, MRc, Stairs test | 1 month | Intervention group was significantly improved in gait speed, 6MWT, Stairs test |
| Ding et al. 2015 [23] | BoNT-A by US -Dosage and location had no data. | Bobath concept, ROM, walking, massage, ADL training. Duration and frequency was not reported | CSI, FMA, BBS, FIM | 1, 3, 6 months | Intervention and Observation group was significantly improved after 1 month in CSI, BBS, FMA, FIM. Intervention group was significantly improved after 3 and 6 months compared other groups in CSI, BBS, FMA, FIM. |
| Tao et al. 2015 [24] | BoNT-A by ES 200U-Gastrocnemius, Soleus, TP | Gait training, the neurodevelopmental technique and motor relearning program physiotherapy (45 min every workday) and occupational therapy (30 min every workday). | MAS, FMA, 6MWT, modifiedBI | 4,8 weeks | The gait analysis, FMA, and MBI results in Intervention group were better than those in control group. |
| Demetrios et al. 2014 [25] | DysportⓇ:54 patients, BotoxⓇ:5 patients mean dose I:766(244), C:673(314), -pectoralis, latissimus dorsi, corachobrachialis, B, BB, BR, PrT, pronator quadratus, FCU, FCR, FDS, FDP, FPL, adductor pollicus, flexor pollicus brevis, opponens pollicus, vastus intermedius, RF, gastrocnemius medial, gastrocnemius lateral, soleus, TP, tibialis anterior, flexor hallicus longus, flexor hallicus brevis, FDB, FDL | I: 3 or more 1-h sessions per week for approximately 10 weeks C: ≤2 × 1-h sessions per week. All participants received goal-directed, individualized rehabilitation programs, consistent with ‘real-life’ rehabilitation practices. motor learning, strengthening, postural awareness, balance training, aerobic/ conditioning exercises, range of movement, stretching, adaptive/ com- pensatory strategies (environmental adaptation, one handed skills), task specific practice and sensory training. | MAS, ArmA, 10MWT, GAS, Self-rated burden | 6, 12, 24 weeks | Intervention group showed greater reduction in MAS score compared with control group at 6 and 12 weeks. Upper limb function and Gait speed was not significantly changed after Intervention and between group.Both groups showed significant improvement in goal attainment and participant satisfaction up to 24 weeks. |
| Combined Rehabilitation | |||||
| Rosales et al. 2012 [27] | DysportⓇ 500U -BB, BR, FCU, FCR, FDS, FDP, FPL | All patients continued with their standard rehabilitation programs throughout the study, as deemed suitable by the attending physician. These generally consisted of a 30- to 60-min program of range of motion plus stretching exercises, strengthening and endurance exercises, and electrical stimulation in some cases. | MAS, ROM, Modified Rankin Scale scores, Functional Motor Assessment Scale, VAS-pain, BI | 2, 4, 8, 12, 24 weeks | Intervention group was significantly improved in MAS. Motor function was not significantly improved. |
| Hesse et al. 2012 [28] | XeominⓇ by US 150U - FDP, FDS, FCR, FCU | Comprehensive rehabilitation in both groups. The multiprofessional motor rehabilitation program was identical in both groups. It included physiotherapy (45 min every workday) and occupational therapy (30 min every workday); speech therapy, neuropsychology and spa therapy | MAS, REPAS, FMA, Disability Scale | 4, 6 weeks | MAS, REPAS and Disability Scale was improved after4 weeks, FMA was not improved. |
| Wolf et al. 2012 [29] | BotoxⓇ MAX300U -wrist and finger muscles | One-hour session divided into 3 sessions. That sessions were scheduled per week beginning approximately 1 month after injections and continued until 12 to 16 treatment sessions were completed | MAS, ROM, WMFT, Stroke Impact Scale | 1, 2, 3 months | MAS scores improved for the BTX-A group and worsened for the control group after injection. There were no group-by-time interactions for changes in the WMFT and no treatment difference, although the Intervention group could complete more tasks governing proximal joint motions. |
| Shaw et al. 2011, 2010 [30,31] | DysportⓇ 100 U or 200 U.Repeat botulinum toxin type A injections and/or therapy were available at 3, 6, and 9 months if considered necessary after reassessment. location had no date. | 4-week therapy program. The therapy program was provided by trained study therapists and each participant received 1 h per day, 2 times per week for 4 weeks. Stretch, positioning, passive/active, assisted upper limb activity, task-oriented practice | MAS, MI, MVG, NHPT, ARAT, pain, BI | 3, 12 months | There was no significant difference in achievement of improved arm function (ARAT) at 1 month. Significant differences in favor of the intervention group were seen in muscle tone at 1 month; upper limb strength at 3 months; basic arm functional tasks (hand hygiene, facilitation of dressing) at 1, 3, and 12 months; and pain at 12 months. |
| Meythaler et al. 2009 [32] | BoNT-A 300U to 400U -location had no date. | Twice weekly 1-h sessions for each 12-week arm of the study (24 weeks total). Subjects did not begin treatment until 10 days from the injection. | Ashworth Scale, ROM, deep tendon reflex score, Grip strength, Pain, MAL, KB-ADL, BI, MOS-36 | 12, 24 weeks | Intervention group only improved the functional status of the subjects on the MAL Quality of Movement subscale and showed a trend toward significance in the Amount of Use subscale. |
| Lim et al. 2008 [33] | BotoxⓇ 100U by EMG -infraspinatus, subscapularis and pectoralis muscles | Physiotherapy during the 6-week period, a minimum of 2 visits per week | MAS, ROM, FMA, Pain, Physician global rating scale | 2, 6, 12 weeks | No significant differences were observed between the 2 groups in terms of improvement in MAS, FMA or physician global rating. |
| Suputtitada et al. 2005 [34] | DysportⓇ by EMG 350 or 500 or1000 U - BB, FCU, FCR, FDP, FDS | Stretching, 3 days per week throughout the 6-month studied period | MAS, ARAT, VAS, BI | 2, 4, 6, 8, 16, 24 weeks | The effect of functional disability was best at a dose of 500 U and the peak improvement was at week 8 after injection. A dose of 1000 U Dysport produced such an excess degree of muscle weakening that the number of randomized patients was reduced to five. BI and ARAT of all patients were decrease after injection. |
| Burbaud et al. 1996 [35] | DysportⓇ by EMG 1000U-Gastrocnemius, Soleus, TP, FDL | Active physiotherapy | MAS, FMA, Gait speed | 30, 90, 120 days | Gait velocity was slightly but not significantly improved after BoNT-A injections. |
| Combined ES, FES and rehabilitation | |||||
| Fujita et al. 2018 [36] | BotoxⓇ by US 300U -Gastro Soleus TP FDL FPL | Physical therapy was performed for 2 weeks (two 1-h sessions per day). Stretch, leg resistance exercises, low-frequency electrical stimulation, electromyographic feedback, walking exercises | MAS, Clonus score, ROM, Gait speed | 2 weeks | Intervention group was significantly changed in gait speed. For those who received BoNT-A+PT, biceps femoris activity and knee co-activation index during the loading response and tibialis anterior activity during the pre-swing phases increased, whereas soleus and rectus femoris activities during the swing phase decreased 2 weeks after the intervention. |
| Weber et al. 2010 [37] | OnabotulinumtoxinA -PrT, FCR, FCU, FDS, FDP, FPL | FES(1hour) and task practice therapy(1hour) included instructions for the home exercise program, and instruction on how to complete a daily patient exercise diary. 12 weeks | MAL, ARAT, MAL-Self-Report | 6, 12 weeks | MAL-Observation mean item scores improved significantly from baseline to week-6, but did not remain significant at week-12. ARAT total scores also improved significantly from baseline to week-6 and were sustained at week-12. However, there were no significant differences between the FES and No-FES groups for any outcome variable over time. |
| Johnson et al. 2002, 2004 [38,39] | DysportⓇ 800U byEMG -Gastrocnemius, TP | A minimum of 3 sessions per week and outpatients 2 sessions per week | Walking speed, PCI, The Rivermead Motor Assessment, SF-36 | 2, 4, 6, 8, 12 weeks | Comparison of median walking speed (nonstimulated) in the control group with median stimulated walking speed shows a significant upward trend, the trend lines being significantly different in location. |
| Combined Robot and rehabilitation | |||||
| Erbil et al. 2018 [40] | BoNT-A by ES -Dosage and location had no data. | 30 min of RAT plus 60 min of physical therapy, whereas controls received 90 min of physical therapy for 3 weeks during weekdays | MAS, Tardieu Scale, TUG, BBS, Rivermead Visual Gait Assessment | 6, 12 weeks | Significant improvements were determined in both RAT and control groups regarding spasticity, balance, and gait functions after treatment. However, at post-treatment Weeks 6 and 12, change from baseline TUG, BBS, and Rivermead Visual Gait Assessment were significantly higher in RAT group than those of the control group. |
| Picelli et al. 2016 [41] | AbobotulinumtoxinA by US 750U -Gastrocnemius, Soleus | RAGT (30 min a day for five consecutive days) Immediately after BoNT‑A administration, all patients included in this study received a 60-min session of electrical stimulation of the injected muscles. | MAS, Tardieu Scale, 6MWT | 1 month | No difference was found between groups as to MAS and the Tardieu scale measured at the affected ankle one month after BoNT-A. A significant difference in 6MWT was noted between groups at the post‑treatment evaluation. |
| Pennati et al. 2015 [42] | DysportⓇ by ES -pectoral, BB, TB, flexor carpi, FDS, FDP, FPL -Dosage had no data. | ReoGo system (10 sessions lasting 60 min each, 2 or 3 days a week) | MAS, FMA, Box&Block test, FIM, Euro-Qol | The end of robotic training | Both groups showed improvement in FMA. Higher improvement in Box&Block test was detected in Control group. MAS was improved more in Intervention group. In both groups, sEMG showed a reduction of co-contractions and an increase of agonist muscles recruitment during the reaching movement and the robotic exercises. |
| Combined Taping, Casting and rehabilitation | |||||
| Carda S et al. 2011 [43] | XeominⓇ by ES -each muscle 50-140U -Gastrocnemius, Soleus | After the first week all patients, irrespective of the allocation arm, underwent 30 min of gait training and 20 min of plantar flexor muscle stretching each day for one week under the guidance of a senior physical therapist. | MAS, ROM, Strength of ankle dorsal flexor muscles, 6MWT, 10MWT, Functional Ambulation Categories | 20,90 days | Intervention group showed better and longer lasting results than with Control group |
| Karadag-Saygi E et al. 2010 [44] | BotoxⓇ by ES 150U-200U -Gastrocnemius | Active-assistive range of motion and stretching exercises were given as a home exercise program to both groups. Exercises were assigned twice daily for 20 min for 4 weeks | MAS, ROM, Gait velocity, Step length | 2 weeks, 1, 3, 6 months | Improvement was recorded in both groups for all outcome variables. No significant difference was found between groups other than ROM, which was found to have increased more in control group at 2 weeks. |
| Combined CIMT | |||||
| Sun et al. 2010 [45] | DysportⓇ 1000U -BB, FDS, FDP, FCU, FCR | 2 h/day, 3 days/week for 3 months | MAS, ARAT, MAL, Patients’ global satisfaction | 4 weeks, 3, 6 months | Spasticity significantly improved in all subjects at 4 weeks and 3 months postinjection without between-group differences. Intervention group showed significantly greater improvements in elbow, wrist, and finger spasticity, affected upper extremity real-world arm function and laboratory motor activity than the control group at 6-month postinjection. |
| Control Group | Study |
|---|---|
| BoNT-A only | Devier et al. 2017 [21], Roche et al. 2015 [22], Fujita et al. 2018 [36], Picelli et al. 2016 [41] |
| Placebo injection | Prazeres A et al. 2018 [19], Tao et al. 2015 [24], Rosales et al. 2012 [27], Wolf et al. 2012 [29], Meythaler et al. 2009 [32] |
| Suputtitada et al. 2005 [34], Burbaud et al. 1996 [35] | |
| Rehabilitation only | Umar et al. 2018 [20], Ding et al. 2015 [23], Demetrios et al. 2014 [25], Hesse et al. 2012 [28], Shaw et al. 2011, 2010 [30,31] |
| Johnson et al. 2002, 2004 [38,39], Pennati et al. 2015 [42], Carda S et al. 2011 [43], Karadag-Saygi E et al. 2010 [44] | |
| BoNT-A + Rehabilitation | Weber et al. 2010 [37], Erbil et al. 2018 [40], Sun et al. 2010 [45] |
| Other | Uchiyama Y et al. 2018 [18], Pimentel et al. 2014 [26], Lim et al. 2008 [33] |
| Risk of Bias | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Uchiyama Y et al. 2018 [18] | High | High | High | High | Low | Low | High |
| Prazeres A et al. 2018 [19] | Low | Low | Low | Low | Low | Unclear | High |
| Umar et al. 2018 [20] | Low | Low | High | Low | Low | Low | Low |
| Devier D et al. 2017 [21] | Low | Low | High | Low | Low | High | High |
| Roche N et al. 2015 [22] | High | Unclear | High | High | Unclear | Low | Low |
| Ding XD et al. 2015 [23] | High | Unclear | High | High | Unclear | Low | High |
| Tao et al. 2015 [24] | Unclear | Unclear | Low | Low | Low | Low | Low |
| Demetrios M et al. 2014 [25] | High | High | High | Low | Low | High | High |
| Pimentel LH et al. 2014 [26] | Unclear | Unclear | Low | Low | Low | Low | Unclear |
| Rosales RL et al. 2012 [27] | Low | Low | Low | Low | Low | High | High |
| Hesse S et al. 2012 [28] | Low | High | High | High | Low | Low | Low |
| Wolf SL et al. 2012 [29] | Low | Low | Low | Low | Low | High | Low |
| Shaw LC et al. 2011, 2010 [30,31] | Low | Low | High | High | Low | Low | High |
| Meythaler JM et al. 2009 [32] | Unclear | Low | Low | Low | Low | High | High |
| Lim JY et al. 2008 [33] | Low | Low | Low | Low | High | High | Low |
| Suputtitada et al. 2005 [34] | Low | High | Low | Low | Low | High | High |
| Burbaud et al. 1996 [35] | Unclear | Unclear | Low | Unclear | Low | High | High |
| Fujita K 2018 [36] | High | High | High | High | Low | Low | High |
| Weber D.J. et al. 2010 [37] | Low | High | High | Low | Low | Low | High |
| Johnson CA et al. 2002, 2004 [38,39] | Low | High | High | High | Low | High | High |
| Erbil D et al. 2018 [40] | Unclear | High | High | High | Low | Low | High |
| Picelli A et al. 2016 [41] | Low | Low | High | Low | Low | Low | Low |
| Pennati G.V. et al. 2015 [42] | Low | Low | High | Low | Low | High | High |
| Carda S et al. 2011 [43] | Low | High | High | Low | Low | Low | Low |
| Karadag-Saygi E et al. 2010 [44] | Unclear | High | High | Low | Low | Low | Low |
| Sun SF et al. 2010 [45] | Low | High | High | Low | Low | Low | Low |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hara, T.; Momosaki, R.; Niimi, M.; Yamada, N.; Hara, H.; Abo, M. Botulinum Toxin Therapy Combined with Rehabilitation for Stroke: A Systematic Review of Effect on Motor Function. Toxins 2019, 11, 707. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11120707
Hara T, Momosaki R, Niimi M, Yamada N, Hara H, Abo M. Botulinum Toxin Therapy Combined with Rehabilitation for Stroke: A Systematic Review of Effect on Motor Function. Toxins. 2019; 11(12):707. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11120707
Chicago/Turabian StyleHara, Takatoshi, Ryo Momosaki, Masachika Niimi, Naoki Yamada, Hiroyoshi Hara, and Masahiro Abo. 2019. "Botulinum Toxin Therapy Combined with Rehabilitation for Stroke: A Systematic Review of Effect on Motor Function" Toxins 11, no. 12: 707. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11120707