Association of Long-Term Treatment by Botulinum Neurotoxins and Occupational Therapy with Subjective Physical Status in Patients with Post-Stroke Hemiplegia

 , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Subjects
5.2. BoNT-A Injections
5.3. Functional Assessment of Upper Extremity
5.4. Items of the Subjective Physical Questionnaire
5.5. Data Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lin, J.P.; Brown, J.K.; Walsh, E.G. Continuum of reflex excitability in hemiplegia: Influence of muscle length and muscular transformation after heel-cord lengthening and immobilization on the pathophysiology of spasticity and clonus. Dev. Med. Child. Neurol. 1999, 41, 534–548. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Huang, P.; Li, X.; Samuel, O.W.; Xiang, Y.; Li, G. Spasticity assessment based on the maximum isometrics voluntary contraction of upper limb muscles in post-stroke hemiplegia. Front. Neurol. 2019, 10, 465. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jaasko, L. Post-stroke hemiplegia and adl-performance. Scand. J. Rehabil. Med. Suppl. 1980, 7, 140–152. [Google Scholar] [PubMed]
- Mikolajewska, E. Associations between results of post-stroke ndt-bobath rehabilitation in gait parameters, adl and hand functions. Adv. Clin. Exp. Med. 2013, 22, 731–738. [Google Scholar] [PubMed]
- Marco, E.; Duarte, E.; Vila, J.; Tejero, M.; Guillen, A.; Boza, R.; Escalada, F.; Espadaler, J.M. Is botulinum toxin type A effective in the treatment of spastic shoulder pain in patients after stroke? A double-blind randomized clinical trial. J. Rehabil. Med. 2007, 39, 440–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marciniak, C.M.; Harvey, R.L.; Gagnon, C.M.; Duraski, S.A.; Denby, F.A.; McCarty, S.; Bravi, L.A.; Polo, K.M.; Fierstein, K.M. Does botulinum toxin type a decrease pain and lessen disability in hemiplegic survivors of stroke with shoulder pain and spasticity? A randomized, double-blind, placebo-controlled trial. Am. J. Phys. Med. Rehabil. 2012, 91, 1007–1019. [Google Scholar] [CrossRef] [PubMed]
- Society, T.J.S. Japanese Guidelines for the Management of Stroke 2015; Kyowa Planning Co., Ltd.: Tokyo, Japan, 2017; p. 360. [Google Scholar]
- Jankovic, J. Botulinum toxin in clinical practice. J. Neurol. Neurosurg. Psychiatry 2004, 75, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Scheps, D.; Lopez de la Paz, M.; Jurk, M.; Hofmann, F.; Frevert, J. Design of modified botulinum neurotoxin a1 variants with a shorter persistence of paralysis and duration of action. Toxicon 2017, 139, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Veverka, T.; Hlustik, P.; Tomasova, Z.; Hok, P.; Otruba, P.; Kral, M.; Tudos, Z.; Zapletalova, J.; Herzig, R.; Krobot, A.; et al. Bont-a related changes of cortical activity in patients suffering from severe hand paralysis with arm spasticity following ischemic stroke. J. Neurol. Sci. 2012, 319, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Bhakta, B.B.; Cozens, J.A.; Bamford, J.M.; Chamberlain, M.A. Use of botulinum toxin in stroke patients with severe upper limb spasticity. J. Neurol. Neurosurg. Psychiatry 1996, 61, 30–35. [Google Scholar] [CrossRef]
- Holmes, R.J.; Connell, L.A. A survey of the current practice of intramuscular Botulinum toxin injections for hemiplegic shoulder pain in the UK. Disabil. Rehabil. 2019, 41, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, E.; Alt Murphy, M.; Persson, H.C.; Lundgren-Nilsson, A.; Sunnerhagen, K.S. Which clinical and sociodemographic determinants are associated with self-perceived manual ability at one year after stroke? Disabil. Rehabil. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bonnyaud, C.; Gallien, P.; Decavel, P.; Marque, P.; Aymard, C.; Pellas, F.; Isner, M.E.; Boyer, F.C.; Muller, F.; Daviet, J.C.; et al. Effects of a 6-month self-rehabilitation programme in addition to botulinum toxin injections and conventional physiotherapy on limitations of patients with spastic hemiparesis following stroke (adju-tox): Protocol study for a randomised controlled, investigator blinded study. BMJ Open 2018, 8, e020915. [Google Scholar] [CrossRef] [PubMed]
- Field, M.; Splevins, A.; Picaut, P.; van der Schans, M.; Langenberg, J.; Noort, D.; Foster, K. AbobotulinumtoxinA (Dysport®), OnabotulinumtoxinA (Botox®), and IncobotulinumtoxinA (Xeomin®) neurotoxin content and potential implications for duration of response in patients. Toxins 2018, 10, 535. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, C.; Munin, M.C.; Brashear, A.; Rubin, B.S.; Patel, A.T.; Slawek, J.; Hanschmann, A.; Hiersemenzel, R.; Elovic, E.P. Incobotulinumtoxina efficacy and safety in adults with upper-limb spasticity following stroke: Results from the open-label extension period of a phase 3 study. Adv. Ther. 2019, 36, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Serlin, R.C.; Mendoza, T.R.; Nakamura, Y.; Edwards, K.R.; Cleeland, C.S. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain 1995, 61, 277–284. [Google Scholar] [CrossRef]
- Given, B.; Given, C.W.; Sikorskii, A.; Jeon, S.; McCorkle, R.; Champion, V.; Decker, D. Establishing mild, moderate, and severe scores for cancer-related symptoms: How consistent and clinically meaningful are interference-based severity cut-points? J. Pain Symptom Manag. 2008, 35, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Foucault, P.; Meklat, H.; Vial, D. Botulinum toxin and medical liability: Is the patient sufficiently informed? Ann. Readapt. Med. Phys. 2005, 48, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Sheean, G.; Lannin, N.A.; Turner-Stokes, L.; Rawicki, B.; Snow, B.J.; Cerebral Palsy, I. Botulinum toxin assessment, intervention and after-care for upper limb hypertonicity in adults: International consensus statement. Eur. J. Neurol. 2010, 17 (Suppl. 2), 74–93. [Google Scholar] [CrossRef]
- Jandhyala, R. Improving consent procedures and evaluation of treatment success in cosmetic use of incobotulinumtoxina: An assessment of the treat-to-goal approach. J. Drugs Dermatol. 2013, 12, 72–78. [Google Scholar]
- Rousseaux, M.; Daveluy, W. The risk-benefit of high doses of botulinum toxin injections for muscle spasticity. Ann. Readapt. Med. Phys. 2007, 50 (Suppl. 1), S1–S3. [Google Scholar] [CrossRef]
- Esquenazi, A.; Albanese, A.; Chancellor, M.B.; Elovic, E.; Segal, K.R.; Simpson, D.M.; Smith, C.P.; Ward, A.B. Evidence-based review and assessment of botulinum neurotoxin for the treatment of adult spasticity in the upper motor neuron syndrome. Toxicon 2013, 67, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the guideline development subcommittee of the american academy of neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [PubMed]
- Devier, D.; Harnar, J.; Lopez, L.; Brashear, A.; Graham, G. Rehabilitation plus onabotulinumtoxina improves motor function over onabotulinumtoxina alone in post-stroke upper limb spasticity: A single-blind, randomized trial. Toxins 2017, 9, 216. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G *power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, N.; Suzuki, M.; Hamaguchi, T. Relationship between knee extension strength and gait styles in patients with dementia. Medicine 2019, 98, e14958. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Treatment | Value |
| Sex (female:male) | 23:24 |
| Type of Stroke (%) | |
| infarction | 15 (32) |
| hemorrhage | 32 (68) |
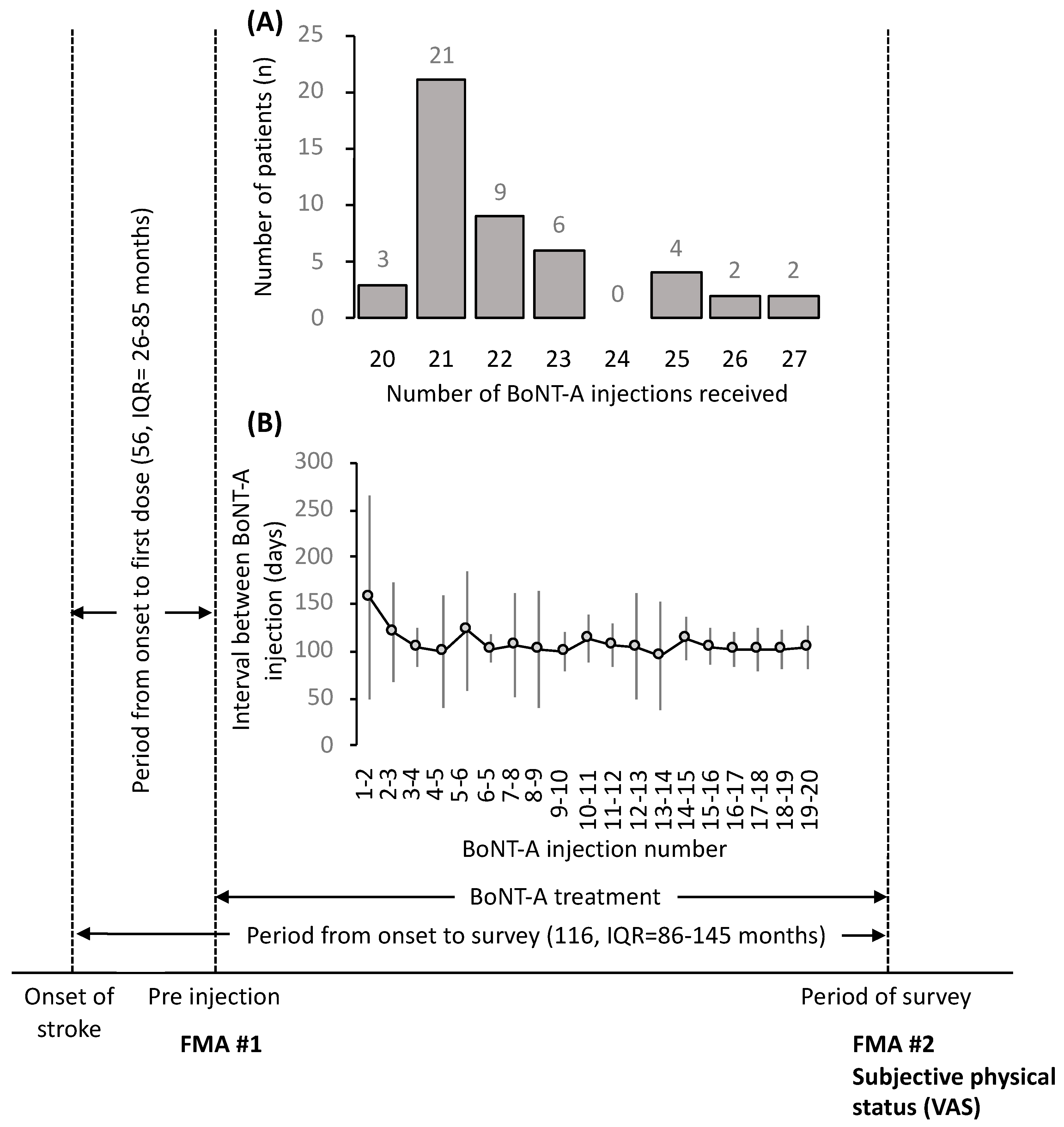
| Period from onset to first dose (months) | 56 (26–85) |
| Post-Treatment | Value |
| Age | 61 ± 16 |
| Period since onset (months) | 116 (86–145) |
| Paralysis side (Right:Left) | 21:26 |
| Number of BoNT-A injections (median (min-max)) | 21 (20–27) |
| BoNT-A dose (Units/patient) | 268 ± 77 |
| Interval between doses (days) | 108 ± 39 |
| How do you feel the efficacy and side effects of BoNT-A treatment given for sequelae of stroke as subjective symptoms? |
| Q1. Pain in my limbs is relieved when I receive an injection. |
| Q2. I will sleep better when injected. |
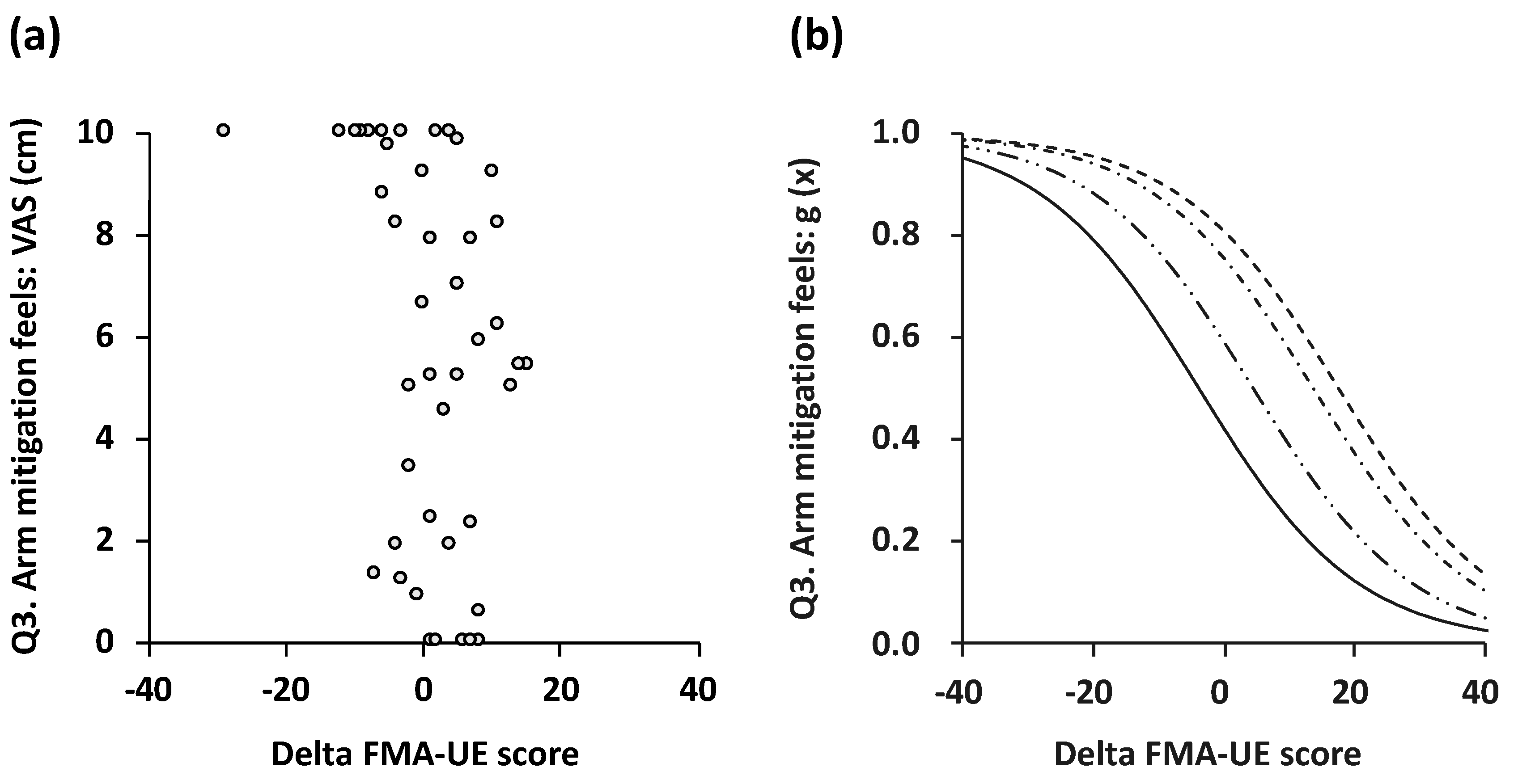
| Q3. My arm feels mitigation when I am injected. |
| Q4. Injections are painful for me. |
| Q5. I feel that the injection has side effects. |
| Do you expect BoNT-A treatment and occupational therapy to be a motivation to continue treatment? Furthermore, is the response of doctors and therapists encouraging for you? |
| Q6. I think it is important to me to continue injection and rehab. |
| Q7. I am encouraged by the response of doctors and therapists. |
| Q8. I think it is important to accept sequelae of stroke. |
| 1: 0–<2 cm | n | 2: 2–<4 cm | n | 3: 4–<6 cm | n | 4: 6–<8 cm | n | 5: 8–10 cm | n | |
|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | 32 (27–37) | 18 | 30 (28–42) | 3 | 41 (39–43) | 5 | 30 (28–39) | 4 | 26 (21–32) | 17 |
| Q2 | 30 (23–37) | 21 | 37 (33–41) | 4 | 40 (37–46) | 8 | 28 (28–29) | 2 | 26 (24–28) | 12 |
| Q3 | 30 (26–28) | 11 | 28 (27–37) | 3 | 40 (37–42) | 8 | 32 (30–39) | 7 | 27 (24–32) | 18 |
| Q4 | 29 (26–34) | 21 | 23 (20–26) | 2 | 32 (26–42) | 7 | 39 (39–40) | 2 | 32 (26–38) | 15 |
| Q5 | 29 (25–38) | 41 | 36 (34–37) | 2 | 34 (33–36) | 2 | - | 0 | 30 (29–31) | 2 |
| Q6 | 43 | 1 | - | 0 | 41 | 1 | 24 | 1 | 31 (26–38) | 44 |
| Q7 | - | 0 | - | 0 | 39 (34–47) | 3 | 30 (24–32) | 5 | 32 (26–38) | 39 |
| Q8 | 32 (32–43) | 3 | - | 0 | 32 (24–38) | 5 | 41 (39–45) | 4 | 28 (25–36) | 35 |
| Question Item | β | SEM | Z | p |
|---|---|---|---|---|
| Q1 | −0.07 | 0.04 | −1.81 | 0.07 |
| Q2 | −0.09 | 0.04 | −2.27 | 0.02 |
| Q3 | −0.08 | 0.04 | −2.07 | 0.04 |
| Q4 | 0.00 | 0.04 | 0.01 | 0.99 |
| Q5 | 0.04 | 0.06 | 0.66 | 0.51 |
| Q6 | −0.07 | 0.09 | −0.74 | 0.46 |
| Q7 | −0.06 | 0.06 | −1.03 | 0.30 |
| Q8 | −0.08 | 0.05 | −1.54 | 0.12 |
| How do you feel your symptoms due to stroke’s sequelae? |
| Q1. Are you suffering from pain in your arm? |
| Q2. Do the symptoms of your arm interfere with your sleep? |
| Q3. Do you feel that your arms are dull? |
| What are your thoughts about BoNT-A treatment and occupational therapy? |
| Q4. Do you think it is important to you to continue rehabilitation? |
| Q5. Do you think that doctors and therapists will be encouraging for you? |
| Q6. Do you think it is important to accept your stroke’s sequelae? |
| Clinical Anatomical Position | Treatment Muscle | Dosage (Units/Injection) |
|---|---|---|
| Adducted upper arm | Pectoralis major | 34.3 ± 14.7 |
| Latissimus dorsi | 21.3 ± 16.8 | |
| Teres major | 2.5 ± 6.3 | |
| Extended elbow | Triceps brachii | 2.4 ± 7.0 |
| Flexed elbow | Biceps brachii | 37.4 ± 16.9 |
| Brachialis | 3.1 ± 7.1 | |
| Brachioradialis | 1.0 ± 2.6 | |
| Pronated forearm | Pronator teres | 12.0 ± 13.0 |
| Pronator quadratus | 0.3 ± 1.1 | |
| Flexed wrist | Flexor carpi radialis | 29.3 ± 16.5 |
| Flexor carpi ulnaris | 7.1 ± 8.5 | |
| Palmaris Iongus | 0.2 ± 0.6 | |
| Clenched fist | Flexor digitorum superficialis | 33.9 ± 16.4 |
| Flexor digitorum profundus | 6.0 ± 9.0 | |
| Thumb-in-palm | Adductor pollicis | 14.0 ± 11.7 |
| Flexor pollicis longus | 4.6 ± 6.8 | |
| Flexor pollicis brevis | 2.1 ± 5.3 | |
| Lumbricals | 1.3 ± 3.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamaguchi, T.; Abo, M.; Murata, K.; Kenmoku, M.; Yoshizawa, I.; Ishikawa, A.; Suzuki, M.; Nakaya, N.; Taguchi, K. Association of Long-Term Treatment by Botulinum Neurotoxins and Occupational Therapy with Subjective Physical Status in Patients with Post-Stroke Hemiplegia. Toxins 2019, 11, 453. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080453
Hamaguchi T, Abo M, Murata K, Kenmoku M, Yoshizawa I, Ishikawa A, Suzuki M, Nakaya N, Taguchi K. Association of Long-Term Treatment by Botulinum Neurotoxins and Occupational Therapy with Subjective Physical Status in Patients with Post-Stroke Hemiplegia. Toxins. 2019; 11(8):453. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080453
Chicago/Turabian StyleHamaguchi, Toyohiro, Masahiro Abo, Kai Murata, Mari Kenmoku, Izumi Yoshizawa, Atsushi Ishikawa, Makoto Suzuki, Naoki Nakaya, and Kensuke Taguchi. 2019. "Association of Long-Term Treatment by Botulinum Neurotoxins and Occupational Therapy with Subjective Physical Status in Patients with Post-Stroke Hemiplegia" Toxins 11, no. 8: 453. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080453