Aflatoxin Exposure from Milk in Rural Kenya and the Contribution to the Risk of Liver Cancer

 ,
,
Abstract
:1. Introduction
2. Results
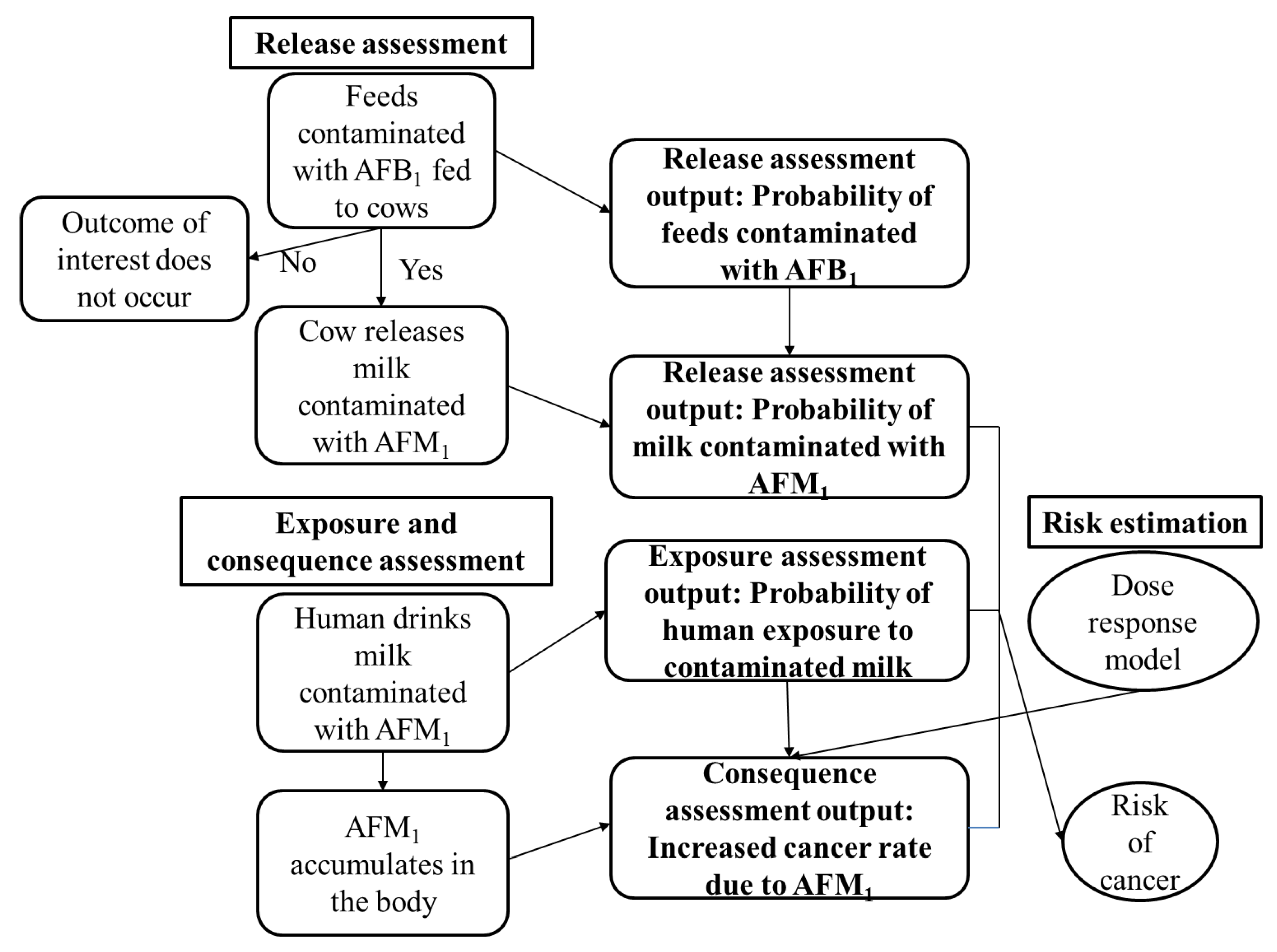
2.1. Release Assessment
2.2. Exposure Assessment
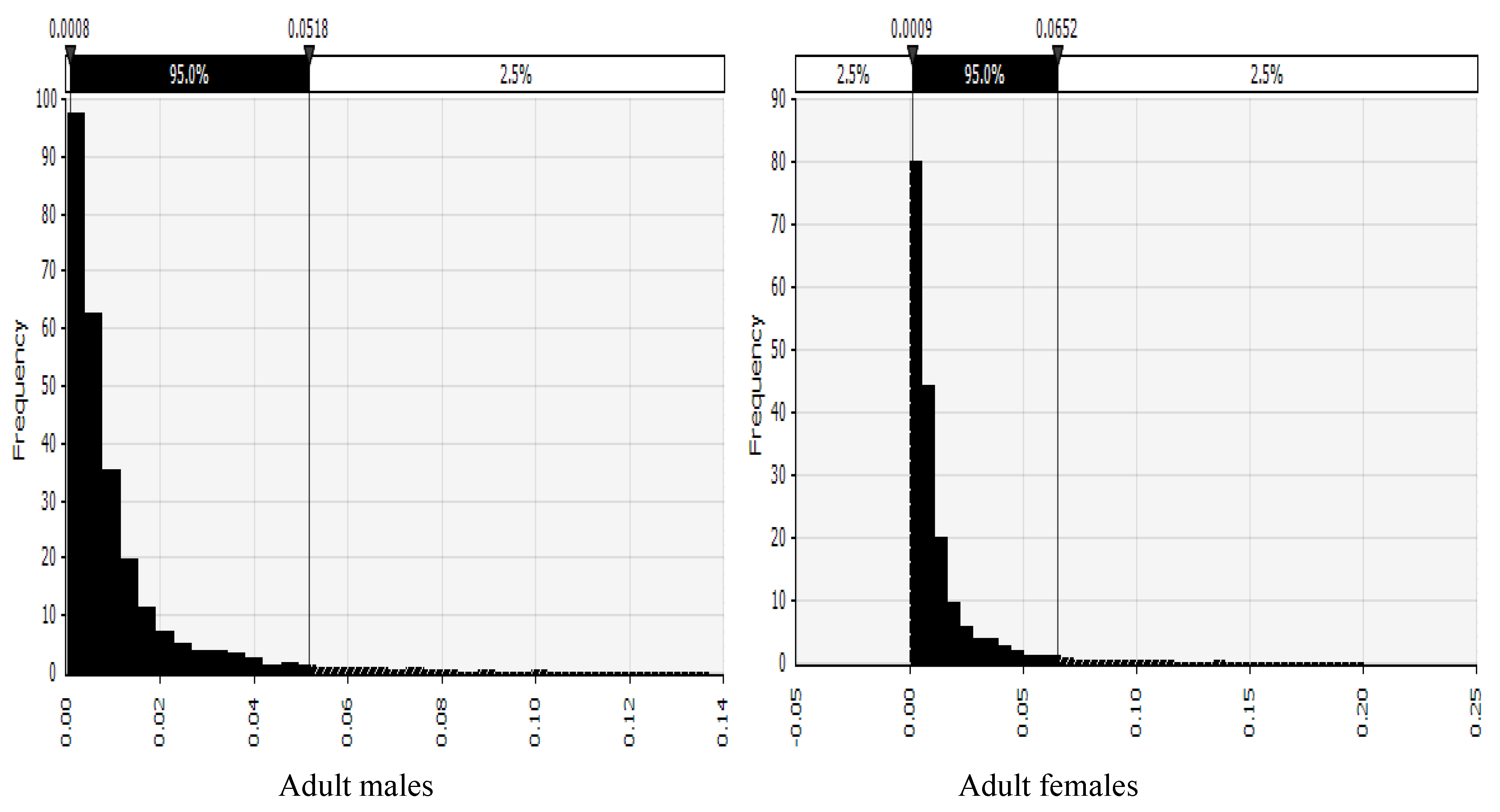
2.3. Consequence Assessment and Risk Estimation
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Site and Household Selection
5.2. Aflatoxin Determination and Validation Of Method
5.3. Quantitative Risk Assessment
5.3.1. Release Assessment
5.3.2. Exposure Assessment
5.3.3. Consequence Assessment
5.3.4. Risk Estimation
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nyikal, J.; Misore, A.; Nzioka, C.; Njuguna, C.; Muchiri, E.; Njau, J.; Maingi, S.; Njoroge, J.; Mutiso, J.; Onteri, J.; et al. Outbreak of aflatoxin poisoning Eastern and Central Provinces, Kenya, January-July 2004. Morb. Mortal. Wkly. Rep. 2004, 53, 790–793. [Google Scholar]
- IARC IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Some Traditional Herbal Medicines, Some Mycotoxins, Naphthalene and Styrene. Int. Agency Res. Cancer Lyon 2002, 82, 1–556. [Google Scholar]
- Kiarie, G.; Dominguez-Salas, P.; Kang’ethe, S.; Grace, D.; Lindahl, J.; Kang’ethe, S.; Grace, D.; Lindahl, J. Aflatoxin exposure among young children in urban low-income areas of Nairobi and association with child growth. Afr. J. Food Agric. Nutr. Dev. 2016, 16, 10967–10990. [Google Scholar] [CrossRef]
- Mutegi, C.K.; Ngugi, H.K.; Hendriks, S.L.; Jones, R.B. Prevalence and factors associated with aflatoxin contamination of peanuts from Western Kenya. Int. J. Food Microbiol. 2009, 130, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutiga, S.K.; Hoffmann, V.; Harvey, J.; Milgroom, M.G.; Nelson, R. Assessment of aflatoxin and fumonisin contamination of maize in western Kenya. Phytopathology 2015, 105, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Senerwa, D.M.; Sirma, A.J.; Mtimet, N.; Kang’ethe, E.K.; Grace, D.; Lindahl, J.F. Prevalence of aflatoxin in feeds and cow milk from five counties in Kenya. Afr. J. Food Agric. Nutr. Dev. 2016, 16, 11004–11021. [Google Scholar] [CrossRef]
- Sirma, A.J.; Senerwa, D.M.; Grace, D.; Makita, K.; Mtimet, N.; Kang’ethe, E.K.; Lindahl, J.F. Aflatoxin B1 occurrence in millet, sorghum and maize from four agro-ecological zones in Kenya. Afr. J. Food Agric. Nutr. Dev. 2016, 16, 10991–11003. [Google Scholar] [CrossRef]
- Pitt, J.I.I.; Wild, C.P.; Baan, R.A.; Gelderblom, W.C.A.; Miller, J.D.; Riley, R.T.; Wu, F. Improving Public Health Through Mycotoxin Control; IARC WHO: Lyon, France, 2012; pp. 225–248. ISBN 978-92-832-2158-6. [Google Scholar]
- IARC Chemical agents and related occupations. 100F. In A Review Of Human Carcinogens; International Agency for Research on Cancer: Lyon, France, 2012; ISBN 9789283213239. [Google Scholar]
- Thomas, A. IARC Mycotoxin Control in Low- and Middle- Income Countries; Wild, C.P., Miller, J.D., Groopman, J.D., Eds.; International Agency for Research on Cancer: Lyon, France, 2016; ISBN 9789283225102. [Google Scholar]
- Guo, C.; Zhang, M. Liver Tumors in Infancy and Children. In Hepatic Surgery; Abdeldayem, H., Ed.; In Tech Open: London, UK, 2013. [Google Scholar] [Green Version]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 359–386. [Google Scholar] [CrossRef]
- Mutuma, G.; Mbuchi, M.; Zeyhle, E.; Fasana, R. Prevalence of Hepatitis B Virus (HBV) surface antigen and HBV-associated hepatocellular carcinoma in Kenyans of various ages. Afr. J. Health Sci. 2011, 18, 53–61. [Google Scholar]
- Liu, Y.; Chang, C.C.H.; Marsh, G.M.; Wu, F. Population attributable risk of aflatoxin-related liver cancer: Systematic review and meta-analysis. Eur. J. Cancer 2012, 48, 2125–2136. [Google Scholar] [CrossRef] [Green Version]
- Vose, D. Risk Analysis: A Quantitative Guide, 3rd ed.; Wiley: Chichester, UK, 2008; ISBN 9780470512845. [Google Scholar]
- Alimentarius, C. Principles and Guidelines for the Conduct Of Microbiological Risk Assessment; FAO/WHO Joint Publications: Rome, Italy, 1999. [Google Scholar]
- OIE Import Risk Analysis. Terrestial Animal Health Code; World Organisation for Animal Health: Paris, France, 2010. [Google Scholar]
- Shephard, G. Risk assessment of aflatoxins in food in Africa. Food Addit. Contam. Part A Chem. Anal. Control. Expo. Risk Assess. 2008, 25, 1246–1256. [Google Scholar] [CrossRef]
- Shephard, G. Impact of mycotoxins on human health in developing countries. Food Addit. Contam. Part A Chem. Anal. Control. Expo. Risk Assess. 2008, 25, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Sirma, A.J.; Lindahl, J.F.; Makita, K.; Senerwa, D.; Mtimet, N.; Kang’ethe, E.K.; Grace, D. The impacts of aflatoxin standards on health and nutrition in sub-Saharan Africa: The case of Kenya. Glob. Food Sec. 2018, 18, 57–61. [Google Scholar] [CrossRef]
- EU Commission Regulation (EC) No 1881/2006 Setting maximum levels for certain contaminants in foodstuffs. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32006R1881&from=EN (accessed on 11 June 2018).
- Cullen, J.M.; Ruebner, B.H.; Hsieh, L.S.; Hyde, D.M.; Hsieh, D.P. Carcinogenicity of Dietary Aflatoxin M1 in Male Fischer Rats Compared to Aflatoxin B1. Cancer Res. 1987, 47, 1913–1917. [Google Scholar]
- Lindahl, J.F.; Kagera, I.N.; Grace, D. Aflatoxin M1 levels in different marketed milk products in Nairobi, Kenya. Mycotoxin Res. 2018, 34, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Wu, F. Global burden of aflatoxin-induced hepatocellular carcinoma: A risk assessment. Environ. Health Perspect. 2010, 118, 818–824. [Google Scholar] [CrossRef]
- Kiama, T.N.; Lindahl, J.F.; Sirma, A.J.; Senerwa, D.; Waithanji, E.M.; Ochungo, P.A.; Poole, E.J.; Kang’ethe, E.K.; Grace, D. Kenya dairy farmer perception of moulds and mycotoxins and implications for exposure to aflatoxins: A gendered analysis. Afr. J. Food, Agric. Nutr. Dev. 2016, 16, 11106–11125. [Google Scholar] [CrossRef]
- Kuboka, M.M.; Imungi, J.K.; Njue, L.; Mutua, F.; Grace, D.; Lindahl, J.F. Occurrence of aflatoxin M1 in raw milk traded in peri-urban Nairobi, and the effect of boiling and fermentation. Infect. Ecol. Epidemiol. 2019, 9, 1625703. [Google Scholar] [CrossRef] [Green Version]
- Fink-Gremmels, J. Mycotoxins in cattle feeds and carry-over to dairy milk: A review. Food Addit. Contam. 2008, 2, 172–180. [Google Scholar] [CrossRef]
- Masoero, F.; Gallo, A.; Moschini, M.; Piva, G.; Diaz, D. Carryover of aflatoxin from feed to milk in dairy cows with low or high somatic cell counts. Animal 2007, 1, 1344–1350. [Google Scholar] [CrossRef] [Green Version]
- Kang’ethe, E.K.; Lang’a, K.A. Aflatoxin B1 and M1 contamination of animal feeds and milk from urban centers in Kenya. Afr. Health Sci. 2009, 9, 218–226. [Google Scholar]
- Lanyasunya, T.P.; Wamae, L.W.; Musa, H.H.; Olowofeso, O.; Lokwaleput, I.K. The risk of mycotoxins contamination of dairy feed and milk on smallholder dairy farms in Kenya. Pakistan J. Nutr. 2005, 4, 162–169. [Google Scholar]
- Signorini, M.L.; Gaggiotti, M.; Molineri, A.; Chiericatti, C.A.; Basílico, M.L.; Basílico, J.C.; Pisani, M. Exposure assessment of mycotoxins in cow’s milk in Argentina. Food Chem. Toxicol. 2012, 50, 250–257. [Google Scholar] [CrossRef]
- Wambui, J.M.; Karuri, E.G.; Ojiambo, J.A.; Njage, P.M.K.K. Application of Probabilistic Modeling to Quantify the Reduction Levels of Hepatocellular Carcinoma Risk Attributable to Chronic Aflatoxins Exposure. Nutr. Cancer 2017, 69, 1–13. [Google Scholar] [CrossRef]
- Lachenmeier, D.W.; Rehm, J. Comparative risk assessment of alcohol, tobacco, cannabis and other illicit drugs using the margin of exposure approach. Sci. Rep. 2015, 5, 8126. [Google Scholar] [CrossRef] [Green Version]
- Lachenmeier, D.W.; Przybylski, M.C.; Rehm, J. Comparative risk assessment of carcinogens in alcoholic beverages using the margin of exposure approach. Int. J. Cancer 2012, 131, E995–E1003. [Google Scholar] [CrossRef]
- Ahlberg, S.; Grace, D.; Kiarie, G.; Kirino, Y.; Lindahl, J.; Ahlberg, S.; Grace, D.; Kiarie, G.; Kirino, Y.; Lindahl, J. A Risk Assessment of Aflatoxin M1 Exposure in Low and Mid-Income Dairy Consumers in Kenya. Toxins 2018, 10, 348. [Google Scholar] [CrossRef]
- Dohoo, I.R.I.; Martin, S.W.S.; Stryhn, H. Methods in Epidemiologic Research; VER Inc.: Charlottetown, Canada, 2012; ISBN 9780919013735. [Google Scholar]
- Imtiaz, N.; Yunus, A.W. Comparison of Some ELISA Kits for Aflatoxin M Quantification. J. AOAC Int. 2019, 102, 677–679. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Agro-Ecological Zone | Mean AFMI Levels in Milk from Cows Fed with Concentrates or Maize Based Feeds | Probability of Samples Exceeding EU Limits (50 ng/kg) | Mean AFMI Levels in Milk from Cows Not Fed Concentrates or Maize Based Feeds | Probability of Samples Exceeding 50 ng/kg |
|---|---|---|---|---|
| Semi-Arid | n/a | - | 8.3 (n = 53) | 0.04 |
| Sub-Humid | 370.7 (n = 2) | * | 4.7 (n = 30) | ** |
| Humid | 52.9 (n = 67) | 0.46 | 10 (n = 21) | ** |
| Temperate | 34.6 (n = 47) | 0.13 | 21.3 (n = 41) | 0.08 |
| AEZ | Mean | Median |
|---|---|---|
| Semi-Arid (n = 200) | 0.2 | 0.2 |
| Sub-Humid (n = 112) | 0.3 | 0.2 |
| Humid (n = 192) | 0.3 | 0.3 |
| Temperate (n = 416) | 0.5 | 0.4 |
| Total (n = 920) | 0.4 | 0.3 |
| Agro-Ecological Zone | Adult Male | Adult Female | Child 6–18 Years | Child <5 Years |
|---|---|---|---|---|
| Semi-arid | 4 × 10−5 (3 × 10−5–5 × 10−5) | 5.9 × 10−3 (4.2 × 10−3–7.5 × 10−3) | 2 × 10−5 (2 × 10−5–3 × 10−5) | 1 × 10−4 (8 × 10−5–1 × 10−4) |
| Sub-humid | 3.2 × 10−3 (2.3 × 10−3–4 × 10−3) | 1.7 × 10−3 (1.2 × 10−3–2.1 × 10−3) | 5 × 10−6 (4 × 10−6–6 × 10−6) | 1.3 × 10−2 (9.2 × 10−3–1.7 × 10−2) |
| Humid | 3.3 × 10−3 (2.3 × 10−3–4.2 × 10−3) | 2 × 10−4 (1 × 10−4–3 × 10−4) | 2.7 × 10−3 (1.9 × 10−3–3.4 × 10−3) | 2.3 × 10−3 (1.6 × 10−4–2.9 × 10−3) |
| Temperate | 1.3 × 10−3 (9 × 10−4–1.7 × 10−3) | 3 × 10−4(2 × 10−4–4 × 10−4) | 7 × 10−4 (5 × 10−4–9 × 10−4) | 2.4 × 10−3 (1.7 × 10−3–3 × 10−3) |
| All | 2.9 × 10−3 (95% CI: 2.5 × 10−3–3.3 × 10−3) | 3.5 × 10−3 (95% CI: 3 × 10−3–3.9 × 10−3) | 1.4 × 10−3 (95% CI: 1.2 × 10−3–1.5 × 10−3) | 2.7 × 10−3 (95% CI: 2.3 × 10−3–3 × 10−3) |
| Risk Assessment Step | Name | Distributions |
|---|---|---|
| Release assessment | AFM1 occurrence in milk in extensive rearing without concentrates | Risk Beta (Number of positive + 1, Number of sample–Number positive + 1) |
| Release assessment | AFM1 occurrence in milk in intensive rearing without concentrates | Risk Beta (Number of positive + 1, Number of sample–Number positive + 1) |
| Release assessment | AFB1 occurrence in feed in extensive rearing with concentrates | Risk Beta (Number of positive + 1, Number of sample–Number positive + 1) |
| Release assessment | AFB1 occurrence in feed in intensive rearing with concentrates | Risk Beta (Number of positive + 1, Number of sample–Number positive + 1) |
| Release assessment | AFM1 occurrence in milk in extensive rearing with concentrates | Risk Beta (Number of positive + 1, Number of sample–Number positive + 1) |
| Release assessment | AFM1 occurrence in milk in intensive rearing with concentrates | Risk Beta (Number of positive + 1, Number of sample–Number positive + 1) |
| Exposure assessment | Frequency of milk consumption (rate) | Risk Duniform (bootstrap of raw data) |
| Exposure assessment | Whether milk was consumed that day | Risk Binomial (1, rate) |
| Exposure assessment | Volume of milk consumed, if consumed | Risk Duniform (bootstrap of raw data) |
| Exposure assessment | AFM1 status in milk | Risk Binomial (1, occurrence of AFM1) |
| Exposure assessment | AFM1 levels in milk | Risk Duniform (bootstrap of raw data) |
| Exposure assessment | Body weight | Risk Normal |
| Exposure assessment | Hepatitis B prevalence | Risk Binomial (1, hepatitis B prevalence) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sirma, A.J.; Makita, K.; Grace Randolph, D.; Senerwa, D.; Lindahl, J.F. Aflatoxin Exposure from Milk in Rural Kenya and the Contribution to the Risk of Liver Cancer. Toxins 2019, 11, 469. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080469
Sirma AJ, Makita K, Grace Randolph D, Senerwa D, Lindahl JF. Aflatoxin Exposure from Milk in Rural Kenya and the Contribution to the Risk of Liver Cancer. Toxins. 2019; 11(8):469. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080469
Chicago/Turabian StyleSirma, Anima J., Kohei Makita, Delia Grace Randolph, Daniel Senerwa, and Johanna F. Lindahl. 2019. "Aflatoxin Exposure from Milk in Rural Kenya and the Contribution to the Risk of Liver Cancer" Toxins 11, no. 8: 469. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080469