A Prospective Observational Cohort Study on Pharmacological Habitus, Headache-Related Disability and Psychological Profile in Patients with Chronic Migraine Undergoing OnabotulinumtoxinA Prophylactic Treatment

 , , and
, , and
Abstract
:
1. Introduction
2. Results
2.1. Demographic and Clinical Carachteristics of Patients with CM
2.2. Headache Index (HI) and Headache-Related Disability Scores during Treatment Phases
2.3. Psychological Characteristics of Patients with CM
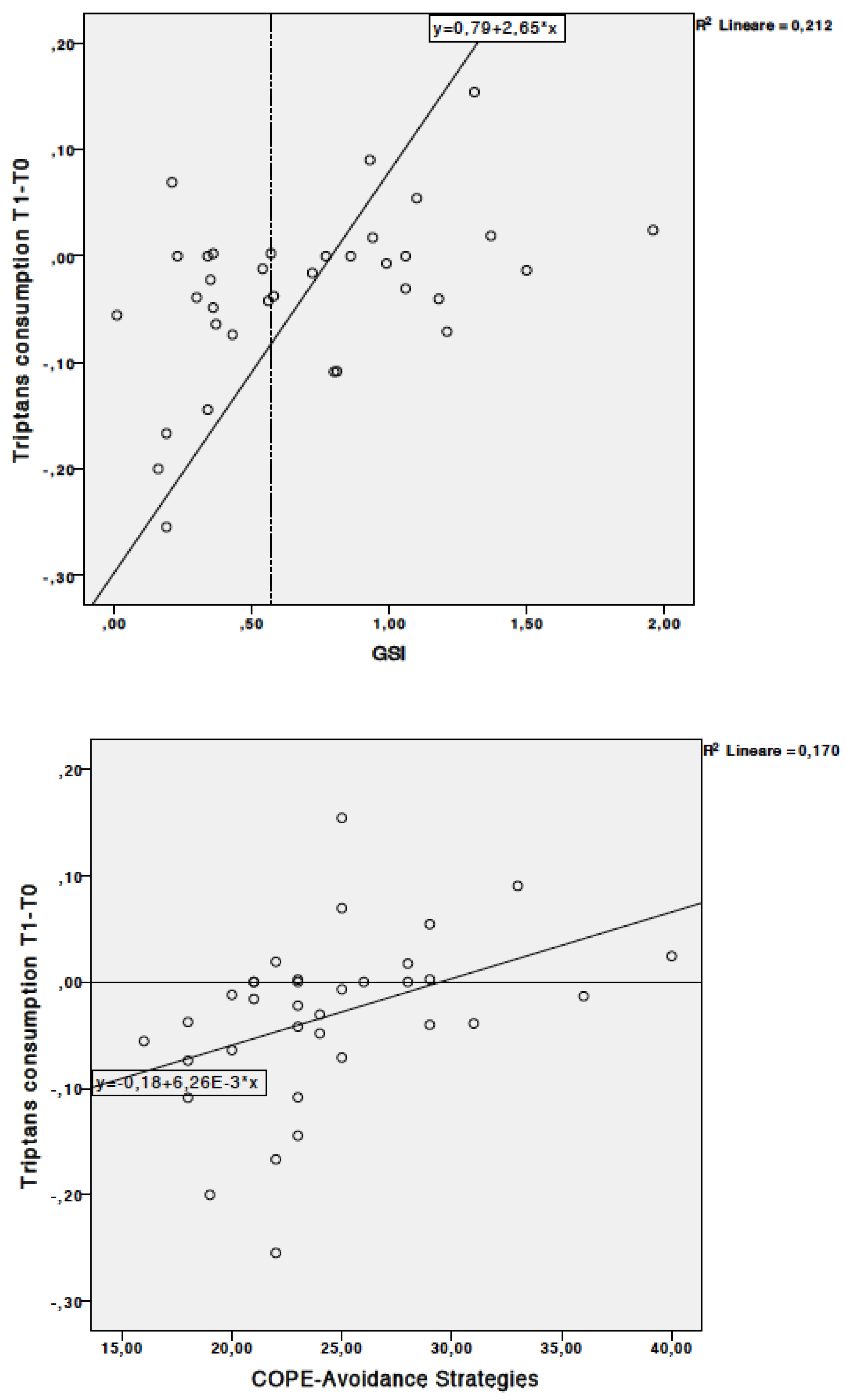
2.4. Correlation between Clinical Outcomes and Psychological Profile
3. Discussion
4. Conclusions
5. Materials and Methods
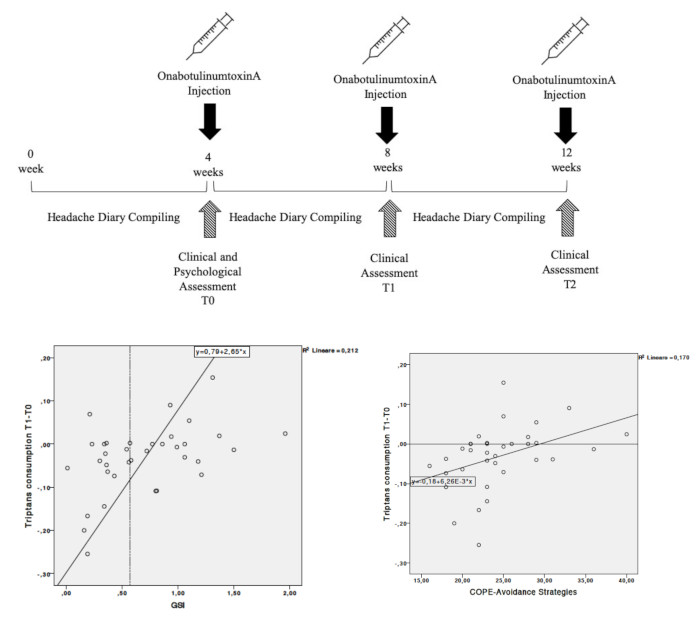
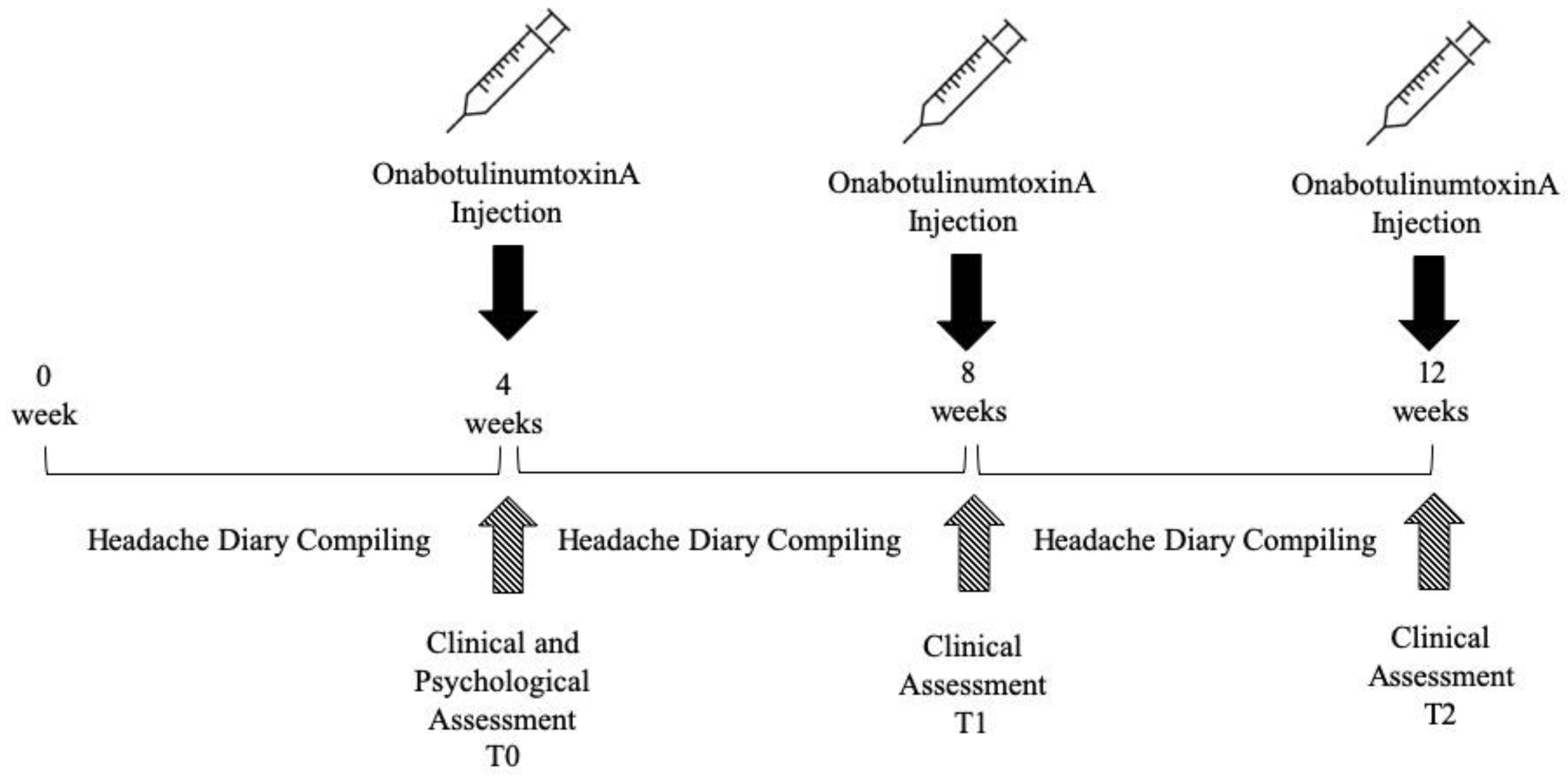
5.1. Study Design and Setting
5.2. Participants
5.3. Measures
5.3.1. Clinical and Demographic Characteristics
5.3.2. Headache-Related Disability
5.3.3. Psychological Outcomes
5.4. OnabotulinumtoxinA Treatment
5.5. Study Size
5.6. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- May, A.; Schulte, L.H. Chronic migraine: Risk factors, mechanisms and treatment. Nat. Rev. Neurol. 2016, 12, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Pomes, L.M.; Guglielmetti, M.; Bertamino, E.; Simmaco, M.; Borro, M.; Martelletti, P. Optimising migraine treatment: From drug-drug interactions to personalized medicine. J. Headache Pain 2019, 20, 56. [Google Scholar] [CrossRef] [PubMed]
- Seybold, V.S. The role of peptides in central sensitization. Handb. Exp. Pharmacol. 2009, 194, 451–491. [Google Scholar] [CrossRef]
- Aurora, S.K.; Brin, M.F. Chronic Migraine: An Update on Physiology, Imaging, and the Mechanism of Action of Two Available Pharmacologic Therapies. Headache 2017, 57, 109–125. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.J. The Diagnosis and Management of Chronic Migraine in Primary Care. Headache 2017, 57, 1471–1481. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Dodick, D.; Aurora, S.; Turkel, C.; Degryse, R.; Lipton, R.; Silberstein, S.; Brin, M. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef]
- Dodick, D.W.; Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef]
- Bendtsen, L.; Sacco, S.; Ashina, M.; Mitsikostas, D.; Ahmed, F.; Pozo-Rosich, P.; Martelletti, P. Guideline on the use of onabotulinumtoxinA in chronic migraine: A consensus statement from the European Headache Federation. J. Headache Pain 2018, 19, 91. [Google Scholar] [CrossRef]
- Park, J.; Chung, M.E. Botulinum Toxin for Central Neuropathic Pain. Toxins (Basel) 2018, 10, 224. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.R.; Francis, J. Updates on the antinociceptive mechanism hypothesis of botulinum toxin A. Park. Relat. Disord. 2011, 17 (Suppl. 1), S28–S33. [Google Scholar] [CrossRef] [PubMed]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, S.; Brigo, F.; Trinka, E.; Vernieri, F.; Corradetti, T.; Dobran, M.; Silvestrini, M. Erenumab for Preventive Treatment of Migraine: A Systematic Review and Meta-Analysis of Efficacy and Safety. Drugs 2019, 79, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Negro, A.; Martelletti, P. Patient selection for migraine preventive treatment with anti-CGRP(r) monoclonal antibodies. Expert Rev. Neurother. 2019, 19, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Piechal, A.; Domitrz, I.; Kurkowska-Jastrzębska, I.; Mirowska-Guzel, D. Are antimigraine drugs that influence CGRP levels justified? Pharmacol. Rep. 2019, 71, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, H.; Wei, Y.; Lian, Y.; Chen, Y.; Zheng, Y. Treatment of chronic daily headache with comorbid anxiety and depression using botulinum toxin A: A prospective pilot study. Int. J. Neurosci. 2017, 127, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Guerzoni, S.; Pellesi, L.; Baraldi, C.; Pini, L.A. Increased efficacy of regularly repeated cycles with OnabotulinumtoxinA in MOH patients beyond the first year of treatment. J. Headache Pain 2015, 17, 48. [Google Scholar] [CrossRef]
- Aydinlar, E.I.; Dikmen, P.Y.; Kosak, S.; Kocaman, A.S. OnabotulinumtoxinA effectiveness on chronic migraine, negative emotional states and sleep quality: A single-center prospective cohort study. J. Headache Pain 2017, 18, 23. [Google Scholar] [CrossRef]
- Demiryurek, B.E.; Ertem, D.H.; Tekin, A.; Ceylan, M.; Aras, Y.G.; Gungen, B.D. Effects of onabotulinumtoxinA treatment on efficacy, depression, anxiety, and disability in Turkish patients with chronic migraine. Neurol. Sci. 2016, 37, 1779–1784. [Google Scholar] [CrossRef]
- Boudreau, G.P.; Grosberg, B.M.; McAllister, P.J.; Lipton, R.B.; Buse, D.C. Prophylactic onabotulinumtoxinA in patients with chronic migraine and comorbid depression: An open-label, multicenter, pilot study of efficacy, safety and effect on headache-related disability, depression, and anxiety. Int. J. Gen. Med. 2015, 18, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Tepper, S.J.; Robbins, L.D.; Manack Adams, A.; Buse, D.C.; Orejudos, A.; Silberstein, S.D. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J. Neurol. Neurosurg. Psychiatry 2019, 90, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarchielli, P.; Corbelli, I.; Messina, P.; Cupini, L.M.; Bernardi, G.; Bono, G.; Di Piero, V.; Petolicchio, B.; Livrea, P.; Prudenzano, M.P.; et al. SAMOHA Study Group. Psychopathological comorbidities in medication-overuse headache: A multicenter clinical study. Eur. J. Neurol. 2016, 23, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Santangelo, G.; Tessitore, A.; Silvestro, M.; Trojsi, F.; De Mase, A.; Garramone, F.; Trojano, L.; Tedeschi, G. Coping Strategies in Migraine without Aura: A Cross-Sectional Study. Behav. Neurol. 2019, 5, 5808610. [Google Scholar] [CrossRef] [PubMed]
- Gunel, M.K.; Akkaya, F.Y. Are migraineur women really more vulnerable to stress and less able to cope? BMC Health Serv. Res. 2008, 8, 211. [Google Scholar] [CrossRef]
- Biagianti, B.; Grazzi, L.; Usai, S.; Gambini, O. Dependency-like behaviors and pain coping styles in subjects with chronic migraine and medication overuse: Results from a 1-year follow-up study. BMC Neurol. 2014, 14, 181. [Google Scholar] [CrossRef]
- D’Amico, D.; Grazzi, L.; Bussone, G.; Curone, M.; Di Fiore, P.; Usai, S.; Leonardi, M.; Giovannetti, A.M.; Schiavolin, S.; Raggi, A. Are depressive symptomatology, self-efficacy, and perceived social support related to disability and quality of life in patients with chronic migraine associated to medication overuse? Data from a cross-sectional study. Headache 2015, 55, 636–645. [Google Scholar] [CrossRef]
- Sica, C.; Magni, C.; Ghisi, M.; Altoè, G.; Sighinolfi, C.; Chiri, L.R.; Franceschini, S. Coping Orientation to Problems Experienced-Nuova Versione Italiana (COPE-NVI): Uno strumento per la misura degli stili di coping. [Coping Orientation or Problems Experienced Italian—New Version (COPE-NVI): An instrument for the measurement of coping styles]. Psicoter. Cogn. Comport. 2008, 14, 27–53. [Google Scholar]
- Schauenburg, H.; Strack, M. Measuring psychotherapeutic change with the symptom checklist SCL 90 R. Psychother. Psychosom. 1999, 68, 199–206. [Google Scholar] [CrossRef]
- Piacentino, D.; Cesarini, M.; Badiali, D.; Pallotta, N.; Biondi, M.; Corazziari, E.S. The central role of psychopathology and its association with disease severity in inflammatory bowel disease and irritable bowel syndrome. Riv. Psichiatr. 2019, 54, 75–83. [Google Scholar] [CrossRef]
- BOTOX. ([OnabotulinumtoxinA]) for Injection, Intramuscular, Intradetrusor, or Intradermal Use; Summary of Product Characteristics; Allergan Ltd.: Marlow, UK, 2015. [Google Scholar]
- Blumenfeld, A.M.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Brin, M.F.; Binder, W.J. Insights into the Functional Anatomy Behind the PREEMPT Injection Paradigm: Guidance on Achieving Optimal Outcomes. Headache 2017, 57, 766–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenfeld, A.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; Binder, W.J. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache 2010, 50, 1406–1418. [Google Scholar] [CrossRef] [PubMed]
- Frampton, J.E.; Silberstein, S. OnabotulinumtoxinA: A Review in the Prevention of Chronic Migraine. Drugs 2018, 78, 589–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matharu, M.; Halker, R.; Pozo-Rosich, P.; DeGryse, R.; Manack Adams, A.; Aurora, S.K. The impact of onabotulinumtoxinA on severe headache days: PREEMPT 56-week pooled analysis. J. Headache Pain 2018, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Baskin, S.M.; Smitherman, T.A. Migraine and psychiatric disorders: Comorbidities, mechanisms, and clinical applications. Neurol. Sci. 2009, 30 (Suppl. 1), S61–S65. [Google Scholar] [CrossRef]
- Seng, E.K.; Buse, D.C.; Klepper, J.E.; J. Mayson, S.; Grinberg, A.S.; Grosberg, B.M.; Pavlovic, J.M.; Robbins, M.S.; Vollbracht, S.E.; Lipton, R.B. Psychological Factors Associated with Chronic Migraine and Severe Migraine-Related Disability: An Observational Study in a Tertiary Headache Center. Headache 2017, 57, 593–604. [Google Scholar] [CrossRef]
- Buse, D.C.; Manack, A.; Serrano, D.; Turkel, C.; Lipton, R.B. Sociodemographic and comorbidity profiles of chronic migraine and episodic migraine sufferers. J. Neurol. Neurosurg. Psychiatry 2010, 81, 428–432. [Google Scholar] [CrossRef]
- Cupini, L.M.; De Murtas, M.; Costa, C.; Mancini, M.; Eusebi, P.; Sarchielli, P.; Calabresi, P. Obsessive-compulsive disorder and migraine with medication-overuse headache. Headache 2009, 49, 1005–1013. [Google Scholar] [CrossRef]
- Curone, M.; Tullo, V.; Lovati, C.; Proietti-Cecchini, A.; D’Amico, D. Prevalence and profile of obsessive-compulsive trait in patients with chronic migraine and medication overuse. Neurol. Sci. 2014, 35 (Suppl. 1), 185–187. [Google Scholar] [CrossRef]
- Hamelsky, S.W.; Lipton, R.B. Psychiatric comorbidity of migraine. Headache 2006, 46, 1327–1333. [Google Scholar] [CrossRef]
- Korkmaz, S.; Kazgan, A.; Korucu, T.; Gönen, M.; Yilmaz, M.Z.; Atmaca, M. Psychiatric symptoms in migraine patients and their attitudes towards psychological support on stigmatization. J. Clin. Neurosci. 2019, 62, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Raggi, A.; Grignani, E.; Leonardi, M.; Andrasik, F.; Sansone, E.; Grazzi, L.; D’Amico, D. Behavioral Approaches for Primary Headaches: Recent Advances. Headache 2018, 58, 913–925. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, A.; Cousins, S.; Ridsdale, L. Psychological interventions for migraine: A systematic review. J. Neurol. 2016, 263, 2369–2377. [Google Scholar] [CrossRef] [PubMed]
- Castelnuovo, G.; Giusti, E.M.; Manzoni, G.M.; Saviola, D.; Gatti, A.; Gabrielli, S.; Lacerenza, M.; Pietrabissa, G.; Cattivelli, R.; Spatola, C.A.; et al. Psychological Treatments and Psychotherapies in the Neurorehabilitation of Pain: Evidences and Recommendations from the Italian Consensus Conference on Pain in Neurorehabilitation. Front. Psychol. 2016, 7, 115. [Google Scholar] [CrossRef] [PubMed]
- Afzal, A.; Ahmad, S.; Agha, F.; Batool, Z.; Tabassum, S.; Liaquat, L.; Sadir, S.; Nawaz, A.; Haider, S. Administration of 5-HT-1B agonist ameliorates pseudodementia induced by depression in rats. Pak. J. Pharm. Sci. 2018, 31, 2179–2184. [Google Scholar] [PubMed]
- Scholz, U.; Gutiérrez-Doña, B.; Sud, S.; Schwarzer, R. Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur. J. Psychol. Assess. 2002, 18, 242–251. [Google Scholar] [CrossRef]
- Matsuzawa, Y.; Lee, Y.S.C.; Fraser, F.; Langenbahn, D.; Shallcross, A.; Powers, S.; Lipton, R.; Simon, N.; Minen, M. Barriers to Behavioral Treatment Adherence for Headache: An Examination of Attitudes, Beliefs, and Psychiatric Factors. Headache 2019, 59, 19–31. [Google Scholar] [CrossRef]
- Probyn, K.; Bowers, H.; Caldwell, F.; Mistry, D.; Underwood, M.; Matharu, M.; Pincus, T. CHESS Team. Prognostic factors for chronic headache: A systematic review. Neurology 2017, 89, 291–301. [Google Scholar] [CrossRef]
- French, D.J.; Holroyd, K.A.; Pinell, C.; Malinoski, P.T.; O’Donnell, F.; Hill, K.R. Perceived self-efficacy and headache-related disability. Headache 2000, 40, 647–656. [Google Scholar] [CrossRef]
- Rains, J.C.; Penzien, D.B.; Lipchik, G.L. Behavioral facilitation of medical treatment of headache: Implications of noncompliance and strategies for improving adherence. Headache 2006, 46 (Suppl. 3), S142–S143. [Google Scholar] [CrossRef]
- Wieser, T.; Walliser, U.; Womastek, I.; Kress, H.G. Dysfunctional coping in headache: Avoidance and endurance is not associated with chronic forms of headache. Eur. J. Pain 2012, 16, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Kosinski, M.; Bayliss, M.S.; Bjorner, J.B.; Ware, J.E., Jr.; Garber, W.H.; Batenhorst, A.; Cady, R.; Dahlöf, C.G.; Dowson, A.; Tepper, S. A six-item short-form survey for measuring headache impact: The HIT-6. Qual. Life Res. 2003, 12, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Rendas-Baum, R.; Yang, M.; Varon, S.F.; Bloudek, L.M.; DeGryse, R.E.; Kosinski, M. Validation of the Headache Impact Test (HIT-6) in patients with chronic migraine. Health Qual. Life Outcomes 2014, 12, 117. [Google Scholar] [CrossRef] [PubMed]
- Smelt, A.F.; Assendelft, W.J.; Terwee, C.B.; Ferrari, M.D.; Blom, J.W. What is a clinically relevant change on the HIT-6 questionnaire? An estimation in a primary-care population of migraine patients. Cephalalgia 2014, 34, 29–36. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, D.; Mosconi, P.; Genco, S.; Usai, S.; Prudenzano, A.M.; Grazzi, L.; Leone, M.; Puca, F.M.; Bussone, G. The Migraine Disability Assessment (MIDAS) Questionnaire: Translation and Reliability of the Italian Version’. Cephalalgia 2001, 21, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R. The SCL-90-R administration, scoring, and procedures manual II for the R(evised) version. Clin. Psychom. Res. 1983. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy scale. In measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. Available online: http://userpage.fu-berling.de/~health/selfscal.htm (accessed on 24 July 2019).



{kind=link}
{kind=link}
{kind=link}
| Demographic and Clinical Features | N (%) |
|---|---|
| Age (years) (Mean, SD) | 46.73 (13.75) |
| Sex (female) | 37 (92.5%) |
| Body Mass Index | 23.62 |
| Sleep regular irregular regular with drugs | 17 (42.5%) 15 (37.5%) 8 (20%) |
| Familiarity with the headache (yes) | 25 (62.5%) |
| Onset pre-adolescence adolescence adult age | 11 (27.5%) 13 (32.5%) 16 (40%) |
| Type of Pain constrictive pulsating both | 17 (42,5%) 17(42.5%) 4 (10%) |
| Presence of aura (yes) | 10 (25%) |
| Pre-study Headache Prophylaxis therapy (non-use) | 16 (40%) |
| Sport Activity (yes) | 18 (45%) |
| Smoker (yes) | 34 (85%) |
| Alcohol consumer (yes) | 35 (87.5%) |
| Contraceptive consumer (yes) | 33 (89.2%) |
| Menopause (yes) | 22 (59.5%) |
| Medical comorbidities (present) | 24 (60%) |
| Acute Headache medicine responsiveness (yes) | 14 (35%) |
| Antidepressants or Anxiolytics consumer (yes) | 14 (35%) |
| On a controlled diet | 7 (17.5%) |
| Number of Detoxification Treatments None One two | 19 (47.5%) 18 (45%) 3 (7.5%) |
| Outcomes | T0 Mean (SD) n = 40 | T1 Mean (SD) n = 35 | T2 Mean (SD) n = 30 | Friedman Test p-Value |
|---|---|---|---|---|
| Wilcoxon Test for Paired Data | ||||
| HI | 0.44 (0.25) | 0.37 (0.24) ** | 0.36 (0.24) ** | <0.001 |
| HI Severe Intensity | 0.92 (1.41) | 0.59 (1.09) | 0.56 (1.11) * | 0.009 |
| HI Moderate Intensity | 0.98 (1.39) | 0.95 (1.48) | 0.78 (1.05) | 0.20 |
| HI Mild intensity | 1.22 (2.39) | 1.36 (2.08) | 0.97 (2.20) | 0.75 |
| HIT-6 | 61.62 (8.42) | 61.48 (7.57) | 58.67 (10.35) | 0.06 |
| Total Analgesics Consumption | 0.41 (0.45) | 0.33 (0.35) | 0.24 (0.21) ** | 0.003 |
| NSAIDs Consumption | 0.22 (0.39) | 0.17 (0.35) | 0.11 (0.21) | 0.09 |
| Triptans Consumption | 0.18 (0.17) | 0.16 (0.17) | 0.12 (0.11) | 0.10 |
| Outcomes | T0 * Mean (SD) |
|---|---|
| General Symptoms Intensity (GSI) | 0.71 (0.48) |
| General self-efficacy scale (GSE) | 28.45 (4.9) |
| Coping style: Social support (COPE-SS) | 29.98 (6.77) |
| Coping style: Avoidance Strategies (COPE-AS) | 23.97 (5.15) |
| Coping style: Positive Attitude (COPE-PA) | 29.65 (6.30) |
| Coping style: Problem Oriented (COPE-PO) | 30.60 (5.72) |
| Coping style: Turning to Religion (COPE-TR) | 22.07 (5.01) |
| MIDAS total score | 65.67 (61.12) |
| MIDAS item C headache frequency | 39.37 (24.91) |
| MIDAS item D pain intensity | 6.37 (1.61) |
| MIDAS Disability Categories | n, % |
| Low to Moderate Disability (score < 21) | 8 (20) |
| Severe Disability (score ≥ 21) | 32 (80) |
| Outcomes | Total AC | NSAIDs C | Triptans C | HI | HI Severe | HI Mod | HI Mild | HIT-6 |
|---|---|---|---|---|---|---|---|---|
| GSI | 0.262 (0.10) | 0.410 (0.009) ** | −0.151 (0.351) | 0.23 (0.159) | 0.438 (0.007) ** | 0.170 (0.315) | 0.027 (0.875) | 0.394 (0.012) * |
| GSE | −0.09 (0.581) | −0.245 (0.128) | 0.111 (0.494) | 0.072 (0.661) | −0.170 (0.313) | 0.028 (0.87) | 0.037 (0.826) | −0.118 (0.469) |
| COPE-SS | 0.03 (0.856) | −0.106 (0.515) | 0.107 (0.509) | −0.175 (0.279) | 0.187 (0.268) | −0.246 (0.142) | −0.43 (0.008) ** | 0.049 (0.764) |
| COPE-AS | −0.027 (0.871) | 0.244 (0.129) | −0.189 (0.242) | 0.240 (0.135) | 0.257 (0.124) | 0.042 (0.804) | 0.020 (0.908) | 0.174 (0.282) |
| COPE-PA | 0.356 (0.024) * | 0.008 (0.961) | −0.260 (0.105) | 0.092 (0.572) | −0.230 (0.127) | −0.166 (0.325) | −0.244 (0.146) | −0.041 (0.80) |
| COPE-PO | 0.354 (0.025) * | −0.04 (0.807) | 0.329 (0.038) * | −0.018 (0.913) | −0.257 (0.125) | −0.283 (0.09) | −0.306 (0.066) | −0.287 (0.073) |
| COPE-TR | −0.130 (0.422) | −0.173 (0.285) | 0.181 (0.265) | 0.109 (0.504) | 0.076 (0.657) | 0.022 (0.899) | −0.219 (0.193) | 0.183 (0.258) |
| Outcomes | Total AC T1-T0 | Total AC T2-T0 | NSAID C T1-T0 | NSAID C T2-T0 | Triptans C T1-T0 | Triptans C T2-T0 | HI T1-T0 | HI T2-T0 |
|---|---|---|---|---|---|---|---|---|
| GSI | 0.204 (0.239) | 0.198 (0.303) | −0.042 (0.811) | −0.030 (0.878) | 0.448 ** (0.007) | 0.515 ** (0.004) | 0.039 (0.826) | −0.032 (0.869) |
| GSE | −0.191 (0.271) | −0.287 (0.131) | −0.287 (0.094) | −0.157 (0.417) | −0.089 (0.609) | −0.328 (0.083) | 0.070 (0.690) | −0.016 (0.936) |
| COPE-SS | −0.058 (0.740) | −0.074 (0.701) | 0.250 (0.148) | 0.006 (0.974) | −0.031 (0.862) | −0.015 (0.939) | 0.033 (0.849) | −0.081 (0.675) |
| COPE-AS | 0.347 * (0.041) | 0.343 (0.069) | −0.064 (0.717) | 0.021 (0.913) | 0.519 ** (0.001) | 0.576 ** (0.001) | 0.204 (0.241) | 0.100 (0.605) |
| COPE-PA | −0.075 (0.669) | −0.128 (0.510) | −0.051 (0.771) | −0.107 (0.579) | −0.018 (0.917) | −0.041 (0.833) | −0.104 (0.553) | −0.242 (0.205) |
| COPE-PO | −0.288 (0.094) | −0.553 ** (0.002) | −0.096 (0.583) | −0.387 * (0.038) | −0.089 (0.612) | −0.295 (0.120) | 0.036 (0.839) | −0.102 (0.599) |
| COPE-TR | 0.241 (0.162) | 0.441 * (0.017) | −0.170 (0.328) | 0.280 (0.141) | −0.035 (0.841) | 0.202 (0.294) | −0.227 (0.190) | 0.263 (0.168) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gandolfi, M.; Donisi, V.; Marchioretto, F.; Battista, S.; Smania, N.; Del Piccolo, L. A Prospective Observational Cohort Study on Pharmacological Habitus, Headache-Related Disability and Psychological Profile in Patients with Chronic Migraine Undergoing OnabotulinumtoxinA Prophylactic Treatment. Toxins 2019, 11, 504. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11090504
Gandolfi M, Donisi V, Marchioretto F, Battista S, Smania N, Del Piccolo L. A Prospective Observational Cohort Study on Pharmacological Habitus, Headache-Related Disability and Psychological Profile in Patients with Chronic Migraine Undergoing OnabotulinumtoxinA Prophylactic Treatment. Toxins. 2019; 11(9):504. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11090504
Chicago/Turabian StyleGandolfi, Marialuisa, Valeria Donisi, Fabio Marchioretto, Simone Battista, Nicola Smania, and Lidia Del Piccolo. 2019. "A Prospective Observational Cohort Study on Pharmacological Habitus, Headache-Related Disability and Psychological Profile in Patients with Chronic Migraine Undergoing OnabotulinumtoxinA Prophylactic Treatment" Toxins 11, no. 9: 504. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11090504