Safety and Stability of Pulmonary Function in Patients with Decreased Respiratory Function Treated for Spasticity with OnabotulinumtoxinA

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Demographics and Baseline Characteristics
2.2. Muscles Injected
2.3. Pulmonary Function Tests
2.3.1. Mean Change from Baseline FVC
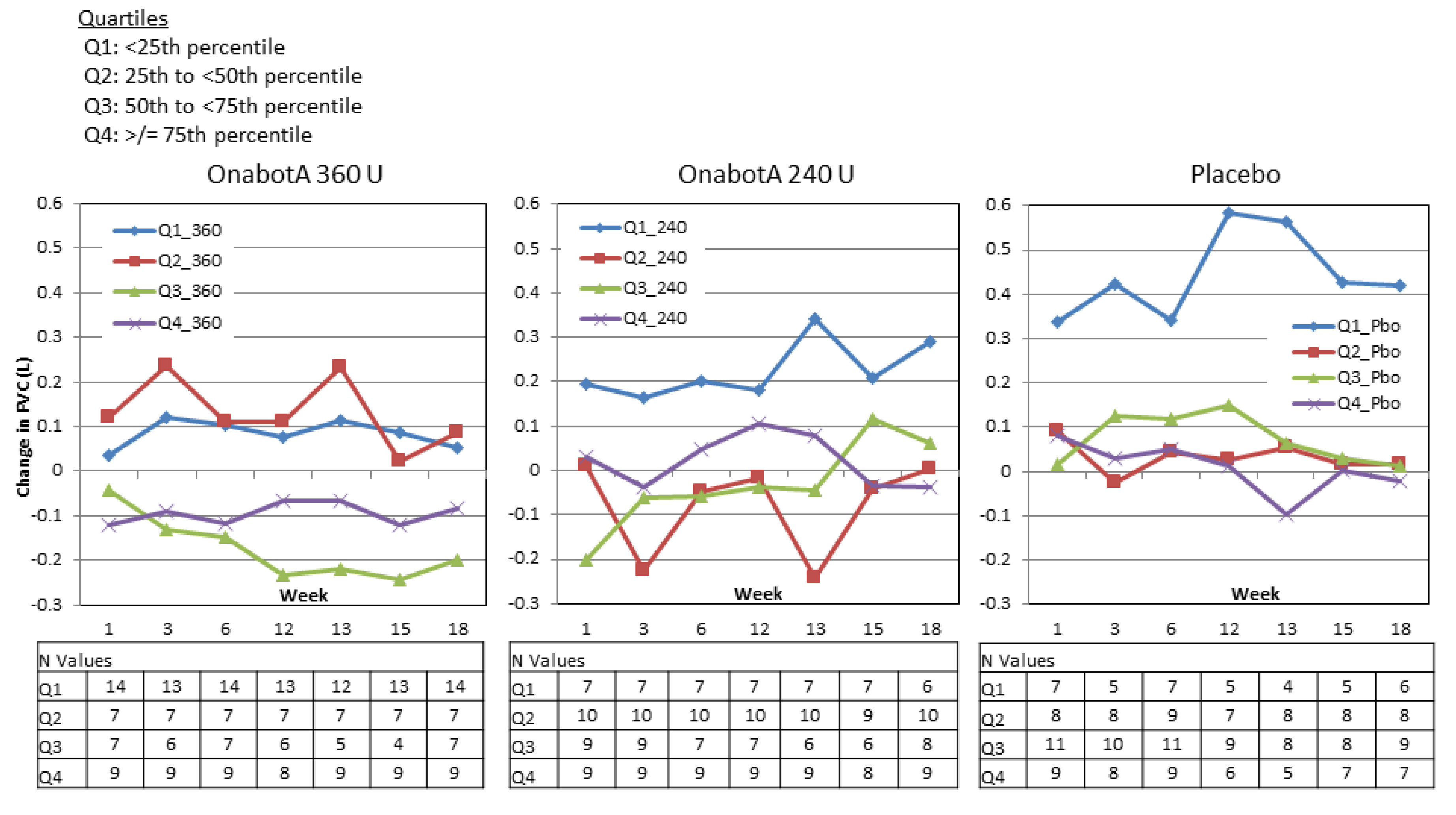
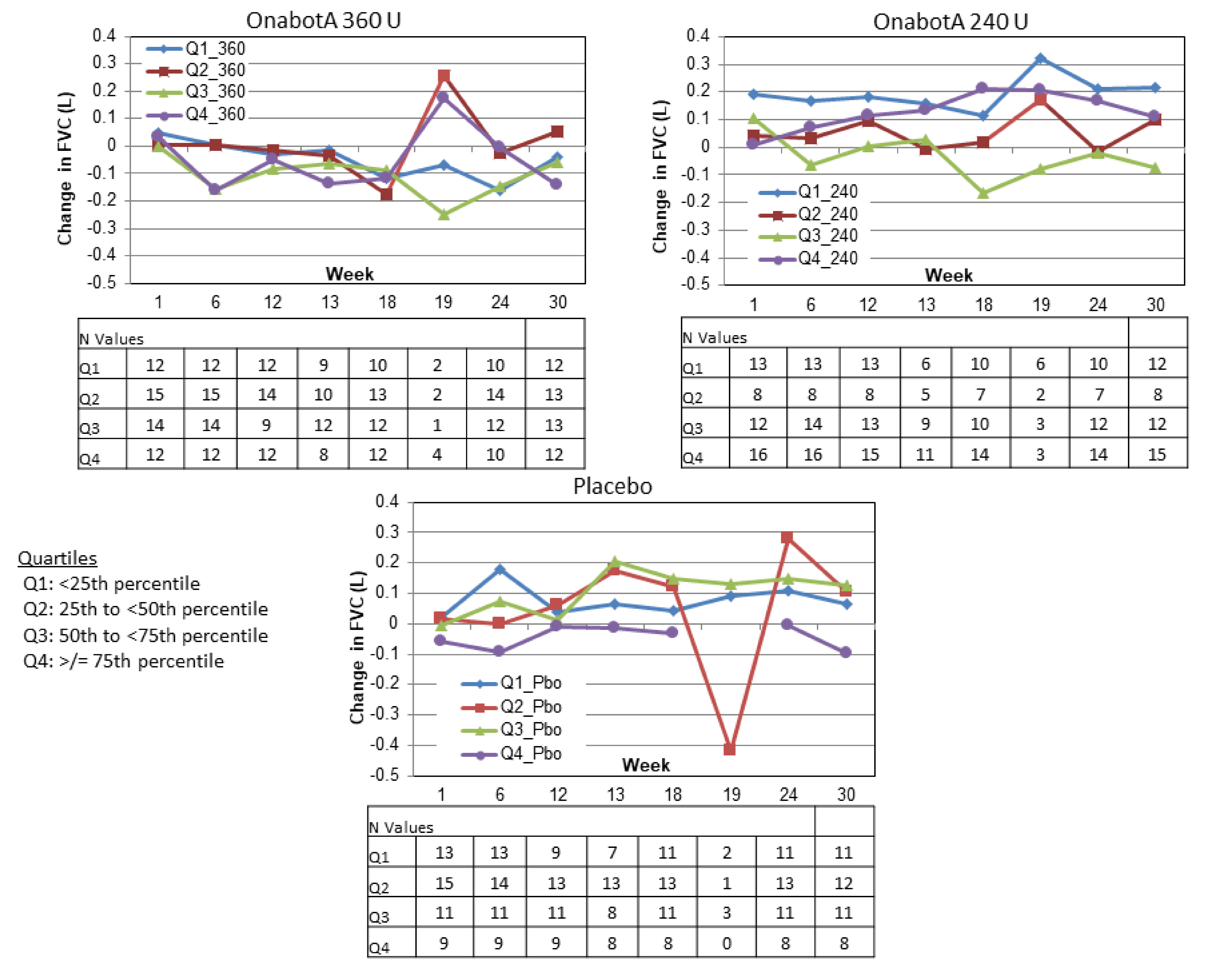
2.3.2. Distribution of Change from Baseline FVC
2.3.3. Percentage of Patients with Decrease of ≥12% and ≥200 mL in FVC or FEV1
2.3.4. Change from Baseline FVC Stratified by Baseline FVC
2.4. Efficacy
2.5. Safety
2.5.1. Adverse Events
2.5.2. Pulmonary Related Adverse Events
2.5.3. Medical Review of Relationship Between PFT and Pulmonary Related Adverse Events
3. Discussion
4. Materials and Methods
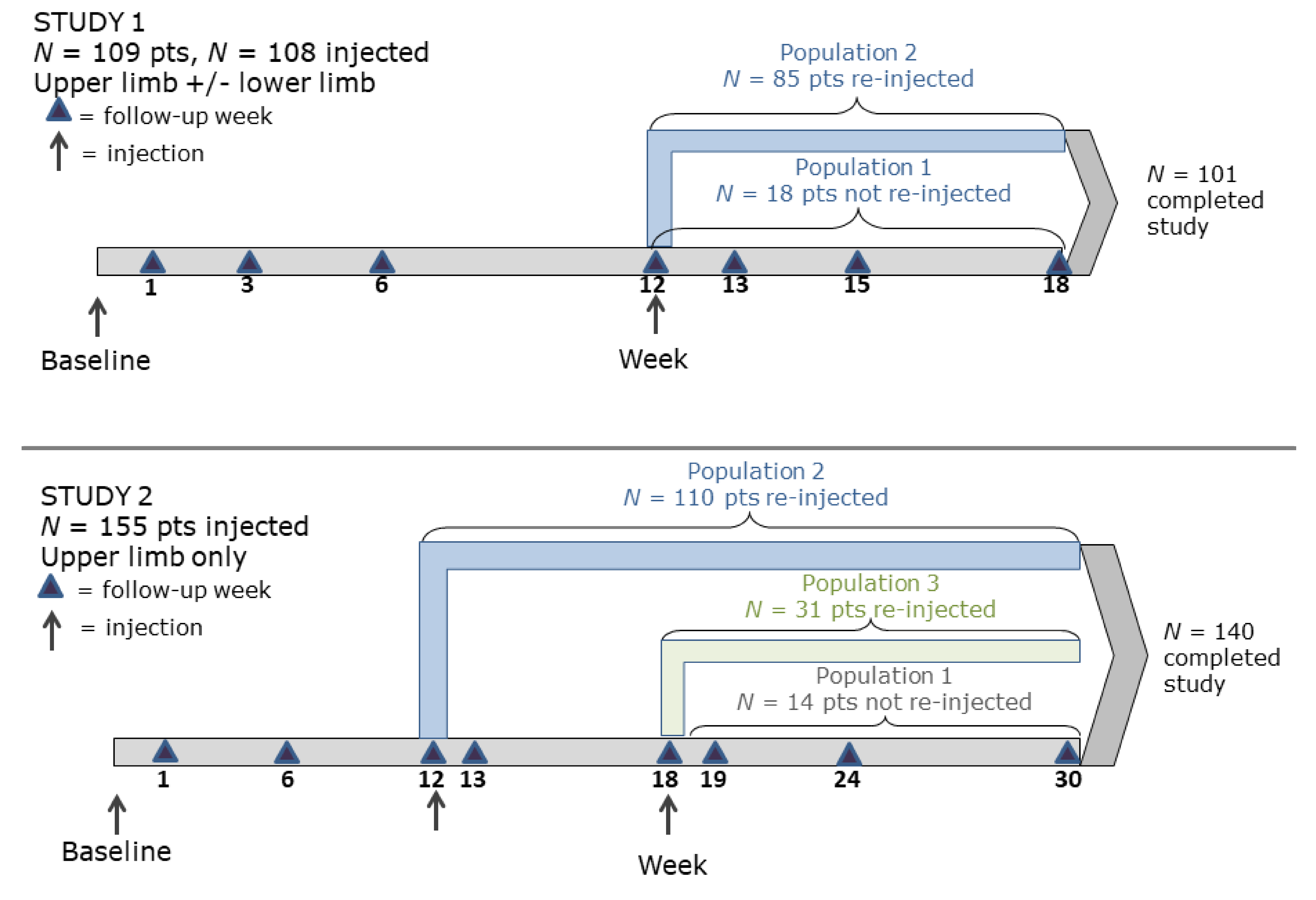
4.1. Study Design and Procedure
4.2. Outcomes
4.3. Sample Size Determination
4.4. Patients
4.5. Data Analysis
4.6. Analysis Populations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 360 U | 240 U | Placebo | p Value | |
|---|---|---|---|---|
| Week 0 total muscles injected (mean) | 5.8 | 4.8 | 4.4 | |
| Flexor digitorum superficialis | 27 (73%) | 23 (64%) | 23 (64%) | 0.625 |
| Flexor carpi radialis | 20 (54%) | 21 (58%) | 16 (44%) | 0.502 |
| Flexor carpi ulnaris | 21 (57%) | 22 (61%) | 21 (58%) | 0.969 |
| Flexor digitorum profundus | 26 (70%) | 18 (50%) | 15 (42%) | 0.042 |
| Biceps | 14 (38%) | 14 (39%) | 13 (36%) | 1.000 |
| Week 12 total muscles injected (mean) | 5.7 | 4.6 | 4.3 | |
| Flexor digitorum superficialis | 22 (59%) | 17 (47%) | 18 (50%) | 0.566 |
| Flexor digitorum profondus | 20 (54%) | 14 (39%) | 13 (36%) | 0.261 |
| Flexor carpi ulnaris | 17 (46%) | 19 (53%) | 15 (42%) | 0.638 |
| Flexor carpi radialis | 16 (43%) | 18 (50%) | 10 (28%) | 0.145 |
| Gastrocnemius lateral | 14 (38%) | 5 (14%) | 7 (19%) | 0.049 |
| 360 U | 240 U | Placebo | p Value | |
|---|---|---|---|---|
| Week 0 total muscles injected | 392 | 386 | 345 | |
| Flexor digitorum superficialis | 51 (92.7%) | 45 (86.5%) | 45 (93.8%) | 0.411 |
| Flexor carpi radialis | 52 (94.5%) | 48 (92.3%) | 40 (83.3%) | 0.152 |
| Flexor carpi ulnaris | 49 (89.1%) | 49 (94.2%) | 40 (83.3%) | 0.220 |
| Biceps | 48 (87.3%) | 48 (92.3%) | 41 (85.4%) | 0.543 |
| Flexor digitorum profundus | 37 (67.3%) | 37 (71.2%) | 34 (70.8%) | 0.905 |
| Week 12 total muscles injected | 361 | 329 | 329 | |
| Flexor digitorum superficialis | 48 (96.0%) | 39 (84.8%) | 42 (95.5%) | 0.100 |
| Biceps | 46 (92.0%) | 40 (87.0%) | 36 (81.8%) | 0.354 |
| Flexor carpi radialis | 43 (86.0%) | 42 (91.3%) | 37 (84.1%) | 0.598 |
| Flexor carpi ulnaris | 43 (86.0%) | 43 (93.5%) | 35 (79.5%) | 0.155 |
| Flexor digitorum profundus | 37 (74.0%) | 30 (65.2%) | 35 (79.5%) | 0.315 |
| Population: | Population 2 a | Population 3 b | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study: | Study 1 | Study 2 | Study 2 | |||||||
| Treatment Group: | 360 U | 240 U | Pbo | 360 U | 240 U | Pbo | 360 U | 240 U | Pbo | |
| Study Baseline | N | 29 | 28 | 28 | 41 | 32 | 37 | 9 | 15 | 7 |
| FVC, mL | 2830 | 3032 | 2981 | 2935 | 3179 | 2955 | 3087 | 2788 | 2574 | |
| Week 1 | N | 29 | 28 | 27 | 41 | 30 | 37 | 9 | 15 | 7 |
| Mean Δ | −3 | 25 | 165 | 35 | 87 | −6 | −22 | 115 | −23 | |
| Week 3 | N | 27 | 28 | 25 | -- | -- | -- | -- | -- | -- |
| Mean Δ | 51 | −20 | 130 | -- | -- | -- | -- | -- | -- | |
| Week 6 | N | 29 | 28 | 28 | 41 | 32 | 37 | 9 | 15 | 7 |
| Mean Δ | −11 ** | 30 | 177 | −69 | 33 | 43 | −122 | 72 | −51 | |
| Week 12 | N | 29 | 28 | 25 | 37 | 31 | 35 | 9 | 15 | 6 |
| Mean Δ | −11 ** | 37 | 170 | −50 | 66 | 80 | −18 | 163 * | −275 | |
| Week 13 | N | 26 | 27 | 23 | 39 | 31 | 36 | -- | -- | -- |
| Mean Δ | 42 | −5 | 103 | −60 ** | 84 | 119 | -- | -- | -- | |
| Week 15 | N | 27 | 24 | 25 | -- | -- | -- | -- | -- | -- |
| Mean Δ | −19 | 14 | 98 | -- | -- | -- | -- | -- | -- | |
| Week 18 | N | 29 | 27 | 27 | 37 | 27 | 36 | 9 | 12 | 7 |
| Mean Δ | −21 | 8 | 89 | −132 *** | 31 | 112 | −127 | 110 | −83 | |
| Week 19 | N | -- | -- | -- | -- | -- | -- | 9 | 14 | 6 |
| Mean Δ | -- | -- | -- | -- | -- | -- | −64 | 189 | 25 | |
| Week 24 | N | -- | -- | -- | 38 | 30 | 36 | 8 | 12 | 7 |
| Mean Δ | -- | -- | -- | −106 *** | 51 | 186 | 36 | 138 | −44 | |
| Week 30 | N | -- | -- | -- | 40 | 31 | 36 | 9 | 15 | 6 |
| Mean Δ | -- | -- | -- | −69 * | 57 | 73 | 31 | 123 | −10 | |
| Treatment Group: | 360 U | 240 U | Placebo | 360 U vs. Placebo Difference b 95% CI c | 240 U vs. Placebo Difference 95% CI | |
|---|---|---|---|---|---|---|
| Study Baseline | N | 37 | 35 | 36 | ||
| FEV1, L | 2.233 | 2.469 | 2.437 | −0.20 (−0.52, 0.11) | 0.03 (−0.29, 0.35) | |
| Week 1 | N | 37 | 35 | 35 | ||
| Mean Δ | −0.044 | −0.045 | 0.073 | −0.12 (−0.25, 0.01) | −0.12 (−0.25, 0.01) | |
| Week 3 | N | 35 | 35 | 31 | ||
| Mean Δ | −0.009 | −0.102 * | 0.059 | −0.07 (−0.22, 0.08) | −0.16 (−0.31, −0.01) | |
| Week 6 | N | 37 | 33 | 36 | ||
| Mean Δ | −0.038 * | −0.041 * | 0.102 | −0.14 (−0.26, −0.02) | −0.14 (−0.27, −0.02) | |
| Week 12 | N | 34 | 33 | 27 | ||
| Mean Δ | −0.029 | −0.066 | 0.033 | −0.06 (−0.20, 0.08) | −0.10 (−0.24, 0.04) | |
| Week 13 | N | 33 | 32 | 25 | ||
| Mean Δ | −0.035 | −0.093 | 0.028 | −0.06 (−0.25, 0.12) | −0.12 (−0.31, 0.06) | |
| Week 15 | N | 33 | 30 | 28 | ||
| Mean Δ | −0.042 | −0.120 | 0.024 | −0.07 (−0.22, 0.09) | −0.14 (−0.30, 0.01) | |
| Week 18 | N | 37 | 33 | 30 | ||
| Mean Δ | −0.059 | −0.137 | 0.018 | −0.08 (−0.23, 0.08) | −0.16 (−0.31, 0.00) | |
| Treatment Group: | 360 U | 240 U | Placebo | 360 U vs. Placebo Difference b 95% CI c | 240 U vs. Placebo Difference 95% CI | |
|---|---|---|---|---|---|---|
| Study Baseline | N | 54 | 53 | 48 | ||
| FEV1, L | 2.183 | 2.206 | 2.111 | 0.07 (−0.18, 0.32) | 0.09 (−0.16, 0.35) | |
| Week 1 | N | 53 | 49 | 48 | ||
| Mean Δ | 0.011 | 0.054 | 0.024 | −0.01 (−0.09, 0.07) | 0.03 (−0.05, 0.11) | |
| Week 6 | N | 52 | 51 | 47 | ||
| Mean Δ | −0.006 | 0.023 | 0.054 | −0.06 (−0.16, 0.04) | −0.03 (−0.13, 0.07) | |
| Week 12 | N | 47 | 49 | 42 | ||
| Mean Δ | −0.035 | 0.072 | 0.060 | −0.09 (−0.20, 0.01) | 0.01 (−0.09, 0.12) | |
| Week 13 | N | 39 | 31 | 36 | ||
| Mean Δ | −0.001 | 0.033 | 0.083 | −0.08 (−0.20, 0.03) | −0.05 (−0.18, 0.08) | |
| Week 18 | N | 47 | 41 | 43 | ||
| Mean Δ | −0.055 ** | 0.059 | 0.139 | −0.19 (−0.32, −0.07) | −0.08 (−0.21, 0.05) | |
| Week 19 | N | 9 | 14 | 6 | ||
| Mean Δ | −0.056 | 0.214 | 0.140 | −0.20 (−0.57, 0.18) | 0.07 (−0.28, 0.42) | |
| Week 24 | N | 46 | 43 | 43 | ||
| Mean Δ | 0.000 | 0.023 | 0.071 | −0.07 (−0.19, 0.05) | −0.05 (−0.17, 0.08) | |
| Week 30 | N | 50 | 47 | 42 | ||
| Mean Δ | 0.007 | 0.035 | 0.048 | −0.04 (−0.16, 0.08) | −0.01 (−0.14, 0.11) | |
| Placebo | OnabotA 240 U | OnabotA 360 U | p-Values OnabotA 240 U vs. Placebo | p-Values OnabotA 360 U vs. Placebo | |
|---|---|---|---|---|---|
| Elbow | (n = 45) | (n = 51) | (n = 51) | ||
| Baseline | 2.76 | 2.47 | 2.57 | 0.131 | 0.301 |
| Week 1 | −0.24 | −0.53 | −0.62 | 0.016 | 0.013 |
| Week 6 | −0.47 | −0.60 | −0.89 | 0.358 | 0.018 |
| Week 12 | −0.26 | −0.40 | −0.51 | 0.474 | 0.100 |
| Week 18 | −0.46 | −0.51 | −0.80 | 0.969 | 0.058 |
| Week 24 | −0.57 | −0.42 | −0.68 | 0.207 | 0.534 |
| Week 30 | −0.24 | −0.40 | −0.56 | 0.608 | 0.112 |
| Wrist | (n = 47) | (n = 52) | (n = 54) | ||
| Baseline | 2.60 | 2.29 | 2.61 | 0.089 | 0.843 |
| Week 1 | −0.21 | −0.60 | −0.80 | 0.008 | <0.001 |
| Week 6 | −0.35 | −0.79 | −1.19 | 0.011 | <0.001 |
| Week 12 | −0.12 | −0.43 | −0.60 | 0.094 | 0.006 |
| Week 18 | −0.35 | −0.54 | −0.96 | 0.181 | <0.001 |
| Week 24 | −0.36 | −0.49 | −0.86 | 0.455 | 0.010 |
| Week 30 | −0.34 | −0.44 | −0.49 | 0.602 | 0.476 |
| Fingers | (n = 46) | (n = 49) | (n = 55) | ||
| Baseline | 2.80 | 2.47 | 2.40 | 0.060 | 0.018 |
| Week 1 | −0.48 | −0.61 | −0.49 | 0.369 | 0.970 |
| Week 6 | −0.44 | −0.80 | −0.81 | 0.062 | 0.029 |
| Week 12 | −0.34 | −0.66 | −0.28 | 0.060 | 0.700 |
| Week 18 | −0.41 | −0.69 | −0.62 | 0.164 | 0.132 |
| Week 24 | −0.48 | −0.56 | −0.29 | 0.818 | 0.200 |
| Week 30 | −0.36 | −0.42 | −0.11 | 0.809 | 0.124 |
| Thumb | (n = 35) | (n = 36) | (n = 35) | ||
| Baseline | 2.37 | 2.00 | 1.94 | 0.102 | 0.096 |
| Week 1 | −0.23 | −0.61 | −0.43 | 0.071 | 0.547 |
| Week 6 | −0.35 | −0.67 | −0.63 | 0.213 | 0.285 |
| Week 12 | −0.29 | −0.49 | −0.30 | 0.249 | 0.897 |
| Week 18 | −0.38 | −0.65 | −0.72 | 0.162 | 0.149 |
| Week 24 | −0.49 | −0.69 | −0.42 | 0.639 | 0.568 |
| Week 30 | −0.29 | −0.54 | −0.10 | 0.246 | 0.559 |
| Placebo (Three Patients, Six Events) |
|---|
| Atrial fibrillation Thrombophlebitis, deep Syncope Accidental injury Bone fracture Joint dislocation |
| OnabotA 240 U (one patient, one event) |
| Asthma |
| OnabotA 360 U (three patients, three events) |
| Pneumonia Bone fracture Arthritis |
| Placebo (Seven Patients, 13 Events) |
|---|
| Convulsion Anemia Hypotension Renal failure Decreased mobility Splenic abscess Cerebral infarction Prostate cancer Syncope Angina pectoris Chronic obstructive pulmonary disease Wound infection Hyponatremia |
| OnabotA 240 U (Nine Patients, 17 Events) |
| Bacteremia Cardiac failure congestive Chronic obstructive pulmonary disease Cellulitis Ischemic stroke Epilepsy Cognitive disorder Hypotension Decreased heart rate Pneumonia (one patient, two events) Abscess Hyperglycemia Meingocele Encephalitis Myocardial infarction Acute coronary syndrome |
| OnabotA 360 U (six patients, 13 events) |
| Appendicitis Convulsion (n = 2 patients, n = 5 events) Hypertension Chest pain Acute endocarditis Cardiac arrest Prostate cancer Gastroenteritis Dyspnea |
| Placebo (n = 36) | OnabotA 240 U (n = 36) | OnabotA 360 U (n = 36) | |
|---|---|---|---|
| Overall | 11 (30.6%) | 8 (22.9%) | 16 (43.2%) |
| Nasopharyngitis | 2 (5.6%) | 3 (8.6%) | 6 (16.2%) |
| Bronchitis | 0 (0.0%) | 1 (2.9%) | 2 (5.4%) |
| Upper respiratory tract infection | 2 (5.6%) | 0 (0.0%) | 2 (5.4%) |
| Oropharyngeal pain | 0 (0.0%) | 2 (5.7%) | 1 (2.7%) |
| Cough | 1 (2.8%) | 1 (2.9%) | 1 (2.7%) |
| Pneumonia | 1 (2.8%) | 0 (0.0%) | 1 (2.7%) |
| COPD | 0 (0.0%) | 0 (0.0%) | 1 (2.7%) |
| Nasal congestion | 0 (0.0%) | 0 (0.0%) | 1 (2.7%) |
| Pleurisy | 0 (0.0%) | 0 (0.0%) | 1 (2.7%) |
| Asthma | 0 (0.0%) | 1 (2.9%) | 0 (0.0%) |
| Rhinitis | 0 (0.0%) | 1 (2.9%) | 0 (0.0%) |
| Influenza | 1 (2.8%) | 0 (0.0%) | 0 (0.0%) |
| Laryngitis | 1 (2.8%) | 0 (0.0%) | 0 (0.0%) |
| Musculoskeletal chest pain | 1 (2.8%) | 0 (0.0%) | 0 (0.0%) |
| Pharyngitis | 1 (2.8%) | 0 (0.0%) | 0 (0.0%) |
| Sinus congestion | 1 (2.8%) | 0 (0.0%) | 0 (0.0%) |
| Sinusitis | 1 (2.8%) | 0 (0.0%) | 0 (0.0%) |
| Wheezing | 1 (2.8%) | 0 (0.0%) | 0 (0.0%) |
| Adverse Event | Placebo (n = 48) | OnabotA 240 U (n = 53) | OnabotA 360 U (n = 54) |
|---|---|---|---|
| Overall | 9 (18.8%) | 14 (26.4%) | 15 (27.8%) |
| Upper respiratory tract infection | 3 (6.3%) | 4 (7.5%) | 6 (11.1%) |
| Nasal congestion | 0 (0.0%) | 2 (3.8%) | 2 (3.7%) |
| Nasopharyngitis | 1 (2.1%) | 1 (1.9%) | 2 (3.7%) |
| Cough | 2 (4.2%) | 3 (5.7%) | 0 (0.0%) |
| COPD | 1 (2.1%) | 1 (1.9%) | 1 (1.9%) |
| Rhinitis | 0 (0.0%) | 2 (3.8%) | 0 (0.0%) |
| Bronchitis | 1 (2.1%) | 0 (0.0%) | 1 (1.9%) |
| Vital capacity decreased | 1 (2.1%) | 0 (0.0%) | 1 (1.9%) |
| Rhinorrhea | 1 (2.1%) | 1 (1.9%) | 0 (0.0%) |
| Forced expiratory volume decreased | 2 (4.2%) | 0 (0.0%) | 0 (0.0%) |
| Chest pain | 0 (0.0%) | 0 (0.0%) | 1 (1.9%) |
| Dyspnea | 0 (0.0%) | 0 (0.0%) | 1 (1.9%) |
| Asthma | 0 (0.0%) | 1 (1.9%) | 0 (0.0%) |
| Oropharyngeal pain | 0 (0.0%) | 1 (1.9%) | 0 (0.0%) |
| Pneumonia | 0 (0.0%) | 1 (1.9%) | 0 (0.0%) |
| Productive cough | 0 (0.0%) | 1 (1.9%) | 0 (0.0%) |
| Sinus congestion | 0 (0.0%) | 1 (1.9%) | 0 (0.0%) |
| Epistaxis | 1 (2.1%) | 0 (0.0%) | 0 (0.0%) |
| Sleep apnea syndrome | 1 (2.1%) | 0 (0.0%) | 0 (0.0%) |
References
- Brashear, A.; Gordon, M.F.; Elovic, E.; Kassicieh, V.D.; Marciniak, C.; Do, M.; Lee, C.H.; Jenkins, S.; Turkel, C. Botox Post-Stroke Spasticity Study, G. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after a stroke. N. Engl. J. Med. 2002, 347, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Fietzek, U.M.; Kossmehl, P.; Schelosky, L.; Ebersbach, G.; Wissel, J. Early botulinum toxin treatment for spastic pes equinovarus--a randomized double-blind placebo-controlled study. Eur. J. Neurol. 2014, 21, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi, A.; Albanese, A.; Chancellor, M.B.; Elovic, E.; Segal, K.R.; Simpson, D.M.; Smith, C.P.; Ward, A.B. Evidence-based review and assessment of botulinum neurotoxin for the treatment of adult spasticity in the upper motor neuron syndrome. Toxicon 2013, 67, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Phadke, C.P.; Balasubramanian, C.K.; Holz, A.; Davidson, C.; Ismail, F.; Boulias, C. Adverse Clinical Effects of Botulinum Toxin Intramuscular Injections for Spasticity. Can. J. Neurol. Sci. 2016, 43, 298–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turkel, C.C.; Bowen, B.; Liu, J.; Brin, M.F. Pooled analysis of the safety of botulinum toxin type A in the treatment of poststroke spasticity. Arch. Phys. Med. Rehabil. 2006, 87, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Bergfeldt, U.; Borg, K.; Kullander, K.; Julin, P. Focal spasticity therapy with botulinum toxin: Effects on function, activities of daily living and pain in 100 adult patients. J. Rehabil. Med. 2006, 38, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Mayer, N.H.; Esquenazi, A. Muscle overactivity and movement dysfunction in the upper motoneuron syndrome. Phys. Med. Rehabil. Clin. 2003, 14, 855–883. [Google Scholar] [CrossRef]
- Santos, R.S.D.; Dall’alba, S.C.F.; Forgiarini, S.G.I.; Rossato, D.; Dias, A.S.; Forgiarini Junior, L.A. Relationship between pulmonary function, functional independence, and trunk control in patients with stroke. Arq. Neuropsiquiatr. 2019, 77, 387–392. [Google Scholar] [CrossRef] [Green Version]
- Roth, E.J.; Noll, S.F. 2. Comorbidities and complications. Arch. Phys. Med. Rehabil. 1994, 75, S42–S46. [Google Scholar] [CrossRef]
- Khedr, E.M.; El Shinawy, O.; Khedr, T.; Abdel Aziz Ali, Y.; Awad, E.M. Assessment of corticodiaphragmatic pathway and pulmonary function in acute ischemic stroke patients. Eur. J. Neurol. 2000, 7, 509–516. [Google Scholar] [CrossRef]
- Schilero, G.J.; Spungen, A.M.; Bauman, W.A.; Radulovic, M.; Lesser, M. Pulmonary function and spinal cord injury. Respir. Physiol. Neurobiol. 2009, 166, 129–141. [Google Scholar] [CrossRef]
- Dong, Y.; Wu, T.; Hu, X.; Wang, T. Efficacy and safety of botulinum toxin type A for upper limb spasticity after stroke or traumatic brain injury: A systematic review with meta-analysis and trial sequential analysis. Eur. J. Phys. Rehabil. Med. 2017, 53, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Schramm, A.; Ndayisaba, J.P.; auf dem Brinke, M.; Hecht, M.; Herrmann, C.; Huber, M.; Lobsien, E.; Mehnert, S.; Reuter, I.; Stenner, A.; et al. Spasticity treatment with onabotulinumtoxin A: Data from a prospective German real-life patient registry. J. Neural. Transm. 2014, 121, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Kaji, R.; Osako, Y.; Suyama, K.; Maeda, T.; Uechi, Y.; Iwasaki, M.; Group, G.S.K.S.S. Botulinum toxin type A in post-stroke upper limb spasticity. Curr. Med. Res. Opin. 2010, 26, 1983–1992. [Google Scholar] [CrossRef]
- Childers, M.K.; Brashear, A.; Jozefczyk, P.; Reding, M.; Alexander, D.; Good, D.; Walcott, J.M.; Jenkins, S.W.; Turkel, C.; Molloy, P.T. Dose-dependent response to intramuscular botulinum toxin type A for upper-limb spasticity in patients after a stroke. Arch. Phys. Med. Rehabil. 2004, 85, 1063–1069. [Google Scholar] [CrossRef]
- Wissel, J.; Bensmail, D.; Ferreira, J.J.; Molteni, F.; Satkunam, L.; Moraleda, S.; Rekand, T.; McGuire, J.; Scheschonka, A.; Flatau-Baque, B.; et al. Safety and efficacy of incobotulinumtoxinA doses up to 800 U in limb spasticity: The TOWER study. Neurology 2017, 88, 1321–1328. [Google Scholar] [CrossRef] [Green Version]
- Sahin, M.; Aydogdu, I.; Akyildiz, S.; Erdinc, M.; Ozturk, K.; Ogut, F. Electromyography-Guided Botulinum Toxin Injection into the Cricothyroid Muscles in Bilateral Vocal Fold Abductor Paralysis. Clin. Exp. Otorhinolaryngol. 2017, 10, 193–202. [Google Scholar] [CrossRef]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [PubMed]
- Urban, P.P.; Morgenstern, M.; Brause, K.; Wicht, S.; Vukurevic, G.; Kessler, S.; Stoeter, P. Distribution and course of cortico-respiratory projections for voluntary activation in man. A transcranial magnetic stimulation study in healthy subjects and patients with cerebral ischemia. J. Neurol. 2002, 249, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Cho, J.E.; Hwang, D.Y.; Lee, W. Decreased Respiratory Muscle Function Is Associated with Impaired Trunk Balance among Chronic Stroke Patients: A Cross-sectional Study. Tohoku J. Exp. Med. 2018, 245, 79–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruhnau, J.; Schulze, K.; Gaida, B.; Langner, S.; Kessler, C.; Broker, B.; Dressel, A.; Vogelgesang, A. Stroke alters respiratory burst in neutrophils and monocytes. Stroke 2014, 45, 794–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winklewski, P.J.; Radkowski, M.; Demkow, U. Cross-talk between the inflammatory response, sympathetic activation and pulmonary infection in the ischemic stroke. J. Neuroinflamm. 2014, 11, 213. [Google Scholar] [CrossRef] [PubMed]
- Brommer, B.; Engel, O.; Kopp, M.A.; Watzlawick, R.; Muller, S.; Pruss, H.; Chen, Y.; DeVivo, M.J.; Finkenstaedt, F.W.; Dirnagl, U.; et al. Spinal cord injury-induced immune deficiency syndrome enhances infection susceptibility dependent on lesion level. Brain 2016, 139, 692–707. [Google Scholar] [CrossRef] [Green Version]
- Crapo, R.O.; Morris, A.H.; Gardner, R.M. Reference spirometric values using techniques and equipment that meet ATS recommendations. Am. Rev. Respir. Dis. 1981, 123, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.A.; Whitelaw, W.A. The assessment of maximal respiratory mouth pressures in adults. Respir. Care 2009, 54, 1348–1359. [Google Scholar]
- Hautmann, H.; Hefele, S.; Schotten, K.; Huber, R.M. Maximal inspiratory mouth pressures (PIMAX) in healthy subjects—What is the lower limit of normal? Respir. Med. 2000, 94, 689–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]







| Study: | Study 1 | Study 2 | ||||
|---|---|---|---|---|---|---|
| Treatment group | 360 U | 240 U | Placebo | 360 U | 240 U | Placebo |
| Total N | 37 | 35 | 36 | 54 | 53 | 48 |
| Mean age (yrs) | 58.8 | 57.7 | 59.1 | 55.5 | 55.9 | 58.0 |
| % Female | 62 | 46 | 42 | 39 | 25 | 40 |
| % Caucasian | 84 | 83 | 58 | 70 | 66 | 71 |
| Mean height (cm) | 166.3 | 169.3 | 168.9 | 171.4 | 171.5 | 171.1 |
| Baseline FVC (L), mean (range) | 2.77 (1.52–4.47) | 3.03 (1.45–6.38) | 2.96 (1.29–4.91) | 2.94 (1.30–4.87) | 3.05 (1.38–5.02) | 2.89 (1.25–4.82) |
| Baseline % predicted FVC, mean (range) | 78 (53–139) | 77 (44–127) | 76 (29–151) | 71 (47–105) | 71 (37–105) | 71 (52–108) |
| Baseline % predicted FVC, number (% of pts) | ||||||
| <40% | 0 (0%) | 0 (0%) | 1 (3%) | 0 (0%) | 1 (2%) | 0 (0%) |
| 40–60% | 5 (14%) | 4 (11%) | 3 (8%) | 10 (19%) | 7 (13%) | 10 (21%) |
| 60–80% | 16 (44%) | 18 (51%) | 20 (56%) | 33 (61%) | 31 (59%) | 27 (56%) |
| >80% | 15 (42%) | 13 (37%) | 12 (33%) | 11 (20%) | 14 (26%) | 11 (23%) |
| Baseline FEV1, mean (range) | 2.23 (1.25–3.63) | 2.47 (1.29–5.18) | 2.44 (1.23–3.94) | 2.18 (1.03–4.34) | 2.21 (0.71–3.37) | 2.11 (0.88–3.66) |
| Baseline % predicted FEV1, mean (range) | 79 (58–137) | 79 (41–130) | 80 (36–152) | 66 (46–80) | 65 (33–84) | 65 (37–100) |
| Baseline % predicted FEV1, number (% of pts) | ||||||
| <40% | 0 (0%) | 0 (0%) | 1 (3%) | 0 (0%) | 1 (2%) | 1 (2%) |
| 40–60% | 4 (11%) | 6 (17%) | 2 (6%) | 17 (32%) | 17 (32%) | 13 (27%) |
| 60–80% | 18 (50%) | 12 (34%) | 15 (42%) | 35 (65%) | 33 (62%) | 31 (65%) |
| >80% | 14 (39%) | 17 (49%) | 18 (50%) | 2 (4%) | 2 (4%) | 3 (6%) |
| FEV1/FVC ratio, mean (range) | 0.81 (0.59–0.97) | 0.82 (0.63–0.98) | 0.83 (0.59–1.20) | 0.74 (0.49–0.95) | 0.73 (0.42–0.97) | 0.74 (0.32–0.98) |
| Treatment Group: | 360 U | 240 U | Placebo | 360 U vs. Placebo Difference b 95% CI c | 240 U vs. Placebo Difference 95% CI | |
|---|---|---|---|---|---|---|
| Study Baseline | N | 37 | 35 | 36 | ||
| FVC, L | 2.772 | 3.032 | 2.958 | −0.19 (−0.58, 0.21) | 0.07 (−0.32, 0.47) | |
| Week 1 | N | 37 | 35 | 35 | ||
| Mean Δ | −0.001 | −0.002 | 0.114 | −0.12 (−0.27, 0.04) | −0.12 (−0.28, 0.04) | |
| Week 3 | N | 35 | 35 | 31 | ||
| Mean Δ | 0.047 | −0.057 * | 0.110 | −0.06 (−0.22, 0.09) | −0.17 (−0.32, −0.01) | |
| Week 6 | N | 37 | 33 | 36 | ||
| Mean Δ | 0.003 | 0.029 | 0.126 | −0.12 (−0.25, 0.01) | −0.10 (−0.23, 0.04) | |
| Week 12 | N | 34 | 33 | 27 | ||
| Mean Δ | −0.006 * | 0.054 | 0.167 | −0.17 (−0.33, −0.02) | −0.11 (−0.27, 0.04) | |
| Week 13 | N | 33 | 32 | 25 | ||
| Mean Δ | 0.039 | 0.112 | 0.109 | −0.07 (−0.24, 0.10) | −0.10 (−0.27, 0.08) | |
| Week 15 | N | 33 | 30 | 28 | ||
| Mean Δ | −0.025 | 0.051 | 0.090 | −0.11 (−0.26, 0.03) | −0.04 (−0.19, 0.11) | |
| Week 18 | N | 37 | 33 | 30 | ||
| Mean Δ | −0.022 | 0.058 | 0.087 | −0.11 (−0.26, 0.05) | −0.03 (−0.19, 0.13) | |
| Treatment Group: | 360 U | 240 U | Placebo | 360 U vs. Placebo Difference b 95% CI c | 240 U vs. Placebo Difference 95% CI | |
|---|---|---|---|---|---|---|
| Study Baseline | N | 54 | 53 | 48 | ||
| FVC, L | 2.935 | 3.053 | 2.889 | 0.05 (−0.27, 0.36) | 0.16 (−0.15, 0.48) | |
| Week 1 | N | 53 | 49 | 48 | ||
| Mean Δ | 0.020 | 0.085 | −0.001 | 0.02 (−0.08, 0.13) | 0.09 (−0.02, 0.19) | |
| Week 6 | N | 52 | 51 | 47 | ||
| Mean Δ | −0.078 * | 0.052 | 0.049 | −0.13 (−0.24, −0.01) | 0.00 (−0.11, 0.12) | |
| Week 12 | N | 47 | 49 | 42 | ||
| Mean Δ | −0.040 | 0.100 | 0.029 | −0.07 (−0.20, 0.06) | 0.07 (−0.06, 0.20) | |
| Week 13 | N | 39 | 31 | 36 | ||
| Mean Δ | −0.060 ** | 0.084 | 0.119 | −0.18 (−0.31, −0.05) | −0.03 (−0.17, 0.11) | |
| Week 18 | N | 47 | 41 | 43 | ||
| Mean Δ | −0.128 *** | 0.064 | 0.080 | −0.21 (−0.33, −0.09) | −0.02 (−0.14, 0.11) | |
| Week 19 | N | 9 | 14 | 6 | ||
| Mean Δ | −0.064 | 0.189 | 0.025 | −0.09 (−0.51, 0.33) | 0.16 (−0.23, 0.56) | |
| Week 24 | N | 46 | 43 | 43 | ||
| Mean Δ | −0.082 *** | 0.094 | 0.149 | −0.23 (−0.37, −0.09) | −0.05 (−0.20, 0.09) | |
| Week 30 | N | 50 | 47 | 42 | ||
| Mean Δ | −0.046 | 0.088 | 0.061 | −0.11 (−0.24, 0.02) | 0.03 (−0.11, 0.16) | |
| Population: | DBPC Population a | Population 2 b | |||||
|---|---|---|---|---|---|---|---|
| Treatment Group: | 360 U | 240 U | Placebo | 360 U | 240 U | Placebo | |
| Week 1 | N | 37 | 35 | 35 | 29 | 28 | 27 |
| n (%) | 6 (16.2%) | 4 (11.4%) | 6 (17.1%) | 5 (17.2%) | 3 (10.7%) | 3 (11.1%) | |
| Week 6 | N | 35 | 35 | 31 | 27 | 28 | 25 |
| n (%) | 5 (14.3%) | 8 (22.9%) | 3 (9.7%) | 4 (14.8%) | 6 (21.4%) | 3 (12.0%) | |
| Week 12 | N | 37 | 33 | 36 | 29 | 28 | 28 |
| n (%) | 4 (10.8%) | 6 (18.2%) | 4 (11.1%) | 4 (13.8%) | 4 (14.3%) | 2 (7.1%) | |
| Week 13 | N | 34 | 33 | 27 | 29 | 28 | 25 |
| n (%) | 6 (17.6%) | 6 (18.2%) | 4 (14.8%) | 6 (20.7%) | 5 (17.9%) | 4 (16.0%) | |
| Week 18 | N | 33 | 32 | 25 | 26 | 27 | 23 |
| n (%) | 6 (18.2%) | 7 (21.9%) | 4 (16.0%) | 4 (15.4%) | 5 (18.5%) | 4 (17.4%) | |
| Week 24 | N | 33 | 30 | 28 | 27 | 24 | 25 |
| n (%) | 5 (15.2%) | 7 (23.3%) | 5 (17.9%) | 4 (14.8%) | 5 (20.8%) | 4 (16.0%) | |
| Week 30 | N | 37 | 33 | 30 | 29 | 27 | 27 |
| n (%) | 6 (16.2%) | 8 (24.2%) | 5 (16.7%) | 4 (13.8%) | 6 (22.2%) | 4 (14.8%) | |
| Population: | DBPC Population a | Population 2 b | Population 3 c | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Treatment Group: | 360 U | 240 U | Placebo | 360 U | 240 U | Placebo | 360 U | 240 U | Placebo | |
| Week 1 | N | 53 | 49 | 48 | 41 | 30 | 37 | 9 | 15 | 7 |
| n (%) | 6 (11.3) | 7 (14.3) | 5 (10.4) | 4 (9.8) | 3 (10.0) | 4 (10.8) | 1 (11.1%) | 2 (13.3%) | 1 (14.3%) | |
| Week 6 | N | 52 | 51 | 47 | 41 | 32 | 37 | 9 | 15 | 7 |
| n (%) | 8 (15.4) | 5 (9.8) | 5 (10.6) | 7 (17.1) | 4 (12.5) | 3 (8.1) | 1 (11.1%) | 1 (6.7%) | 2 (28.6%) | |
| Week 12 | N | 47 | 49 | 42 | 37 | 31 | 35 | 9 | 15 | 6 |
| n (%) | 9 (19.1) | 4 (8.2) | 4 (9.5) | 8 (21.6) * | 1 (3.2) | 1 (2.9) | 1 (11.1%) | 2 (13.3%) | 3 (50.0%) | |
| Week 13 | N | 39 | 31 | 36 | 39 | 31 | 36 | -- | -- | -- |
| n (%) | 9 (23.1) | 3 (9.7) | 3 (8.3) | 9 (23.1) | 3 (9.7) | 3 (8.3) | -- | -- | -- | |
| Week 18 | N | 47 | 41 | 43 | 37 | 27 | 36 | 9 | 12 | 7 |
| n (%) | 11 (23.4) | 6 (14.6) | 4 (9.3) | 8 (21.6) * | 5 (18.5) | 1 (2.8) | 3 (33.3%) | 1 (8.3%) | 3 (42.9%) | |
| Week 19 | N | 9 | 14 | 6 | -- | -- | -- | 9 | 14 | 6 |
| n (%) | 2 (22.2%) | 1 (7.1%) | 1 (16.7%) | -- | -- | -- | 2 (22.2%) | 1 (7.1%) | 1 (16.7%) | |
| Week 24 | N | 46 | 43 | 43 | 38 | 30 | 36 | 8 | 12 | 7 |
| n (%) | 10 (21.7) * | 6 (14.0) | 3 (7.0) | 9 (23.7) * | 5 (16.7) | 2 (5.6) | 1 (12.5%) | 1 (8.3%) | 1 (14.3%) | |
| Week 30 | N | 50 | 47 | 42 | 40 | 31 | 36 | 9 | 15 | 6 |
| n (%) | 9 (18.0) | 8 (17.0) | 5 (11.9) | 7 (17.5) | 7 (22.6) | 5 (13.9) | 2 (22.2%) | 1 (6.7%) | 0 (0.0%) | |
| All Patients (N = 109) | Placebo (n = 36) | OnabotA 240 U (n = 36) | OnabotA 360 U (n = 37) | p-Values OnabotA 240 U vs. Placebo | p-Values OnaboA 360 U vs. Placebo |
|---|---|---|---|---|---|
| Baseline | 3.0 | 2.9 | 2.7 | 0.497 | 0.123 |
| Week 1 | −0.4 | −0.7 * | −0.9 * | 0.007 | 0.001 |
| Week 3 | −0.5 | −0.9 * | −0.9 * | 0.003 | 0.013 |
| Week 6 | −0.2 | −0.8 * | −0.8 * | <0.001 | 0.003 |
| Week 12 | 0.0 | −0.3 | −0.3 | 0.061 | 0.064 |
| Week 13 | −0.3 | −0.7 * | −0.7 * | 0.017 | 0.029 |
| Week 15 | −0.3 | −0.7 * | −0.7 | 0.031 | 0.055 |
| Week 18 | −0.1 | −0.7 * | −0.6 * | 0.001 | 0.013 |
| Placebo (n = 48) | OnabotA 240 U (n = 52) | OnabotA 360 U (n = 55) | p-Values OnabotA 240 U vs. Placebo | p-Values OnabotA 360 U vs. Placebo | |
|---|---|---|---|---|---|
| Baseline | 2.65 | 2.34 * | 2.44 | 0.035 | 0.151 |
| Week 1 | −0.28 | −0.58 * | −0.61 * | 0.005 | 0.011 |
| Week 6 | −0.39 | −0.72 * | −0.93 * | 0.010 | <0.001 |
| Week 12 | −0.23 | −0.50 * | −0.43 | 0.009 | 0.079 |
| Week 18 | −0.37 | −0.60 * | −0.79 * | 0.048 | 0.001 |
| Week 24 | −0.46 | −0.53 | −0.59 | 0.498 | 0.230 |
| Week 30 | −0.30 | −0.45 | −0.35 | 0.151 | 0.645 |
| Placebo | OnabotA 240 U | OnabotA 360 U | |
|---|---|---|---|
| Number (%) of Patients | |||
| Study 1 | |||
| Any AEs | 28/36 (77.8%) | 22/36 (61.1%) | 26/36 (72.2%) |
| Treatment-related AEs | 5/36 (13.9%) | 6/36 (16.7%) | 5/36 (13.9%) |
| Serious AEs | 3/36 (8.3%) | 1/36 (2.8%) | 3/36 (8.3%) |
| Study 2 | |||
| Any AEs | 25/48 (52.1%) | 30/52 (57.7%) | 28/55 (50.9%) |
| Treatment-related AEs | 4/48 (8.3%) | 5/52 (9.6%) | 7/55 (12.7%) |
| Serious AEs | 7/48 (14.6%) | 9/52 (17.3%) | 6/55 (10.9%) |
| Adverse Event | Placebo (n = 36) | OnabotA 240 U (n = 36) | OnabotA 360 U (n = 36) |
|---|---|---|---|
| Overall | 11 (30.6%) | 8 (22.9%) | 16 (43.2%) |
| Nasopharyngitis | 2 (5.6%) | 3 (8.6%) | 6 (16.2%) |
| Bronchitis | 0 (0.0%) | 1 (2.9%) | 2 (5.4%) |
| Upper respiratory tract infection | 2 (5.6%) | 0 (0.0%) | 2 (5.4%) |
| Oropharyngeal pain | 0 (0.0%) | 2 (5.7%) | 1 (2.7%) |
| Adverse Event | Placebo (n = 48) | OnabotA 240 U (n = 53) | OnabotA 360 U (n = 54) |
|---|---|---|---|
| Overall | 9 (18.8%) | 14 (26.4%) | 15 (27.8%) |
| Upper respiratory tract infection | 3 (6.3%) | 4 (7.5%) | 6 (11.1%) |
| Nasal congestion | 0 (0.0%) | 2 (3.8%) | 2 (3.7%) |
| Nasopharyngitis | 1 (2.1%) | 1 (1.9%) | 2 (3.7%) |
| Cough | 2 (4.2%) | 3 (5.7%) | 0 (0.0%) |
| Rhinitis | 0 (0.0%) | 2 (3.8%) | 0 (0.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayyoub, Z.; Brashear, A.; Banach, M.; Schoene, R.; Stringer, W.; Boodhoo, T.; Yushmanova, I.; Dimitrova, R.; Brin, M.F. Safety and Stability of Pulmonary Function in Patients with Decreased Respiratory Function Treated for Spasticity with OnabotulinumtoxinA. Toxins 2020, 12, 661. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12100661
Ayyoub Z, Brashear A, Banach M, Schoene R, Stringer W, Boodhoo T, Yushmanova I, Dimitrova R, Brin MF. Safety and Stability of Pulmonary Function in Patients with Decreased Respiratory Function Treated for Spasticity with OnabotulinumtoxinA. Toxins. 2020; 12(10):661. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12100661
Chicago/Turabian StyleAyyoub, Ziyad, Allison Brashear, Marta Banach, Robert Schoene, William Stringer, Terry Boodhoo, Irina Yushmanova, Rozalina Dimitrova, and Mitchell F. Brin. 2020. "Safety and Stability of Pulmonary Function in Patients with Decreased Respiratory Function Treated for Spasticity with OnabotulinumtoxinA" Toxins 12, no. 10: 661. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12100661