Inhibitory Effects of a Reengineered Anthrax Toxin on Canine Oral Mucosal Melanomas

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Clinical and Histological Characteristics
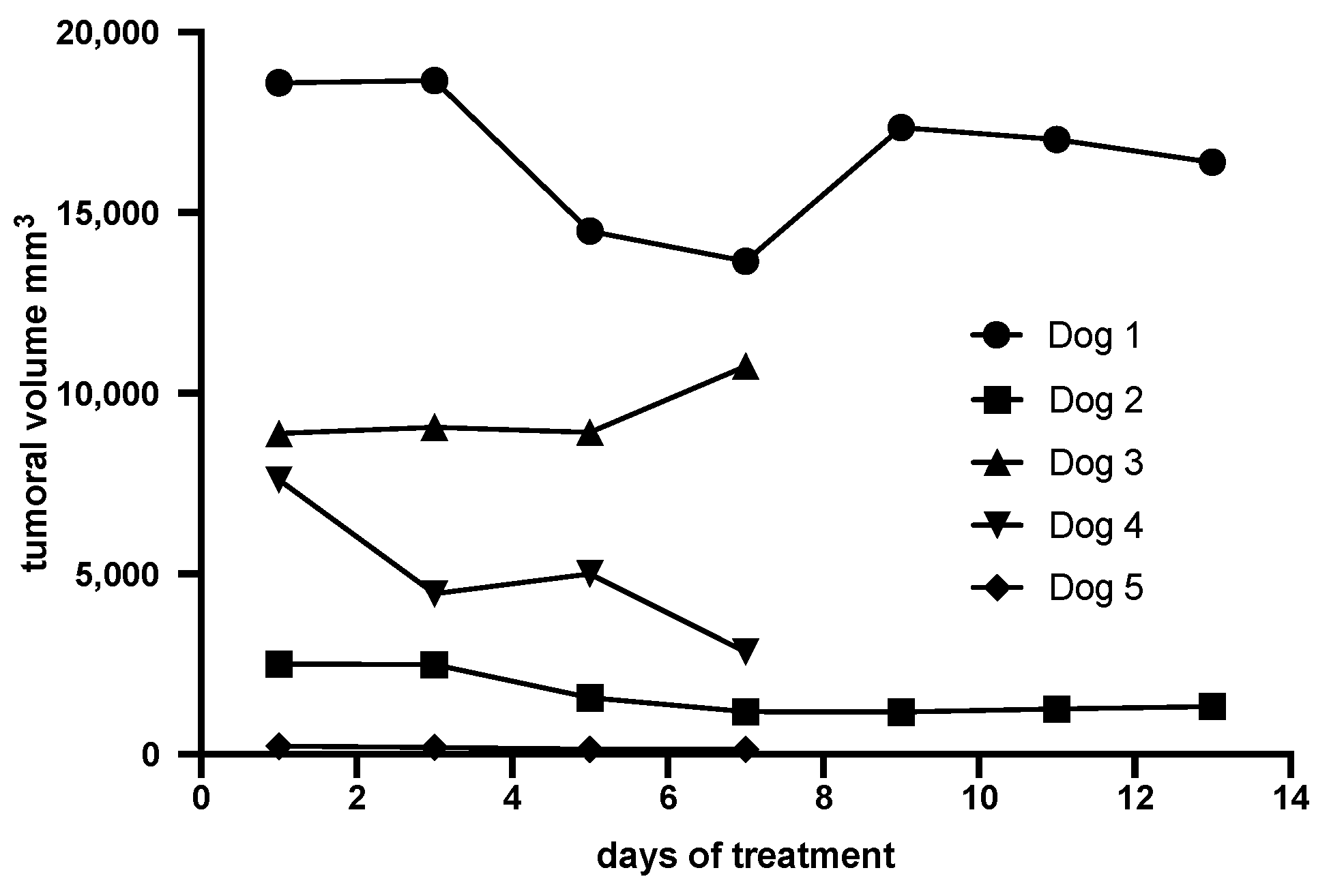
2.2. Evaluation of the Clinical Response of Canine OMM to the Reengineered Anthrax Toxin
2.3. Histopathology, Immunostaining, and Cell Proliferation of Canine OMM Before and After Treatment with the Reengineered Anthrax Toxin
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Animals
5.2. Reengineered Anthrax Toxin
5.3. Clinical Study
5.4. OMM Histopathology and Immunostaining
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bergman, P.J. Canine Oral Melanoma. Clin. Tech. Small Anim. Pract. 2007, 22, 55–60. [Google Scholar] [CrossRef]
- Nishiya, A.T.; Massoco, C.O.; Felizzola, C.R.; Perlmann, E.; Batschinski, K.; Tedardi, M.V.; Garcia, J.S.; Mendonça, P.P.; Teixeira, T.F.; Dagli, M.L.Z. Comparative Aspects of Canine Melanoma. Vet. Sci. 2016, 3, 7. [Google Scholar] [CrossRef]
- Williams, L.E.; Packer, R.A. Association between lymph node size and metastasis in dogs with oral malignant melanoma: 100 cases (1987–2001). J. Am. Vet. Med. Assoc. 2003, 222, 1234–1236. [Google Scholar] [CrossRef] [PubMed]
- Tuohy, J.L.; Milgram, J.; Worley, D.R.; Dernell, W.S. A review of sentinel lymph node evaluation and the need for its incorporation into veterinary oncology. Vet. Comp. Oncol. 2009, 7, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Esplin, D.G. Survival of dogs following surgical excision of histologically well differentiated melanocytic neoplasms of the mucous membranes of the lips and oral cavity. Vet. Pathol. 2008, 45, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Harvey, H.J.; MacEwen, E.G.; Braun, D.; Patnaik, A.K.; Withrow, S.J.; Jongeward, S. Prognostic criteria for dogs with oral melanoma. J. Am. Vet. Med. Assoc. 1981, 178, 580–582. [Google Scholar] [PubMed]
- Boston, S.E.; Lu, X.; Culp, W.T.; Montinaro, V.; Romanelli, G.; Dudley, R.M.; Liptak, J.M.; Mestrinho, L.A.; Buracco, P. Efficacy of systemic adjuvant therapies administered to dogs after excision of oral malignant melanomas: 151 cases (2001–2012). J. Am. Vet. Med. Assoc. 2014, 245, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Bergman, P.J.; Wolchok, J.D. Of mice and men (and dogs): Development of a xenogeneic DNA vaccine for canine oral malignant melanoma. Cancer Ther. 2008, 6, 817–826. [Google Scholar]
- Grosenbaugh, D.A.; Leard, A.T.; Bergman, P.J.; Klein, M.K.; Meleo, K.; Susaneck, S.; Hess, P.R.; Jankowski, M.K.; Jones, P.D.; Leibman, N.; et al. Safety and efficacy of a xenogeneic DNA vaccine encoding for human tyrosinase as adjunctive treatment for oral malignant melanoma in dogs following surgical excision of the primary tumor. Am. J. Vet. Res. 2011, 72, 1631–1638. [Google Scholar] [CrossRef]
- Hoopes, P.J.; Wagner, R.J.; Duval, K.; Kang, K.; Gladstone, D.J.; Moodie, K.L.; Crary-Burney, M.; Ariaspulido, H.; Veliz, F.A.; Steinmetz, N.F.; et al. Treatment of Canine Oral Melanoma with Nanotechnology-Based Immunotherapy and Radiation. Mol. Pharm. 2018, 15, 3717–3722. [Google Scholar] [CrossRef]
- Suzuki, D.O.H.; Berkenbrock, J.A.; Frederico, M.J.S.; Silva, F.R.M.B.; Rangel, M.M.M. Oral Mucosa Model for Electrochemotherapy Treatment of Dog Mouth Cancer: Ex Vivo, In Silico, and In Vivo Experiments. Artif. Organs. 2018, 42, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Wouda, R.M.; Hocker, S.E.; Higginbotham, M.L. Safety evaluation of combination carboplatin and toceranib phosphate (Palladia) in tumour-bearing dogs: A phase I dose finding study. Vet. Comp. Oncol. 2018, 16, E52–E60. [Google Scholar] [CrossRef] [PubMed]
- Bachran, C.; Leppla, S.H. Tumor Targeting and Drug Delivery by Anthrax Toxin. Toxins 2016, 8, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Aaronson, H.; Mitola, D.J.; Leppla, S.H.; Bugge, T.H. Potent antitumor activity of a urokinase-activated engineered Bacillus anthracis toxin. Proc. Natl. Acad. Sci. USA 2003, 100, 657–662. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Bugge, T.H.; Leppla, S.H. Targeting of tumor cells by cell surface urokinase plasminogen activator-dependent Bacillus anthracis toxin. J. Biol. Chem. 2001, 276, 17976–17984. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Bugge, T.H.; Frankel, A.E.; Leppla, S.H. Dissecting the urokinase activation pathway using urokinase-activated Bacillus anthracis toxin. Methods Mol. Biol. 2009, 539, 175–190. [Google Scholar]
- Klimpel, K.R.; Molloy, S.S.; Thomas, G.; Leppla, S.H. Bacillus anthracis toxin protective antigen is activated by a cell-surface protease with the sequence specificity and catalytic properties of furin. Proc. Natl. Acad. Sci. USA 1992, 89, 10277–10281. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Redeye, V.; Kuremsky, J.G.; Kuhnen, M.; Molinolo, A.; Bugge, T.H.; Leppla, S.H. Intermolecular complementation achieves high-specificity tumor targeting by Bacillus anthracis toxin. Nat. Biotechnol. 2005, 23, 725–730. [Google Scholar] [CrossRef] [Green Version]
- Rønø, B.; Rømer, J.; Liu, S.; Bugge, T.H.; Leppla, S.H.; Kristjansen, P.E. Antitumor efficacy of a urokinase activation-dependent Bacillus anthracis toxin. Mol. Cancer Ther. 2006, 5, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Schafer, J.M.; Peters, D.E.; Morley, T.; Liu, S.; Molinolo, A.A.; Leppla, S.H.; Bugge, T.H. Efficient targeting of head and neck squamous cell carcinoma by systemic administration of a dual uPA and MMP-activated engineered Bacillus anthracis toxin. PLoS ONE 2011, 6, e20532. [Google Scholar] [CrossRef] [Green Version]
- Andreasen, P.; Egelund, R.; Petersen, H. CMLS, The plasminogen activation system in tumor growth, invasion, and metastasis. Cell. Mol. Life Sci. 2000, 57, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Nakaichi, M.; Yunuki, T.; Okuda, M.; Une, S.; Taura, Y. Activity of matrix metalloproteinase-2 (MMP-2) in canine oronasal tumors. Res. Vet. Sci. 2007, 82, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Docampo, M.J.; Cabrera, J.; Rabanal, R.M.; Bassols, A. Expression of matrix metalloproteinase-2 and -9 and membrane-type 1 matrix metalloproteinase in melanocytic tumors of dogs and canine melanoma cell lines. Am. J. Vet. Res. 2011, 72, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Bailey, T.R.; Paulsen, D.B.; Sehgal, I.; Hosgood, G. Immunohistochemical staining of urokinase plasminogen activator-like and urokinase plasminogen activator receptor-like proteins in the urinary tract of healthy dogs. Am. J. Vet. Res. 2006, 67, 1628–1634. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.; Lopes, C.; Marques, R.M.; Amorim, I.; Ribeiro, J.; Frias, C.; Vicente, C.; Gärtner, F.; de Matos, A. Immunohistochemical analysis of urokinase plasminogen activator and its prognostic value in canine mammary tumours. Vet. J. 2011, 189, 43–83. [Google Scholar] [CrossRef] [PubMed]
- Spangler, W.L.; Kass, P.H. The histologic and epidemiologic bases for prognostic considerations in canine melanocytic neoplasia. Vet. Pathol. 2006, 43, 136–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Liu, J.; Ma, Q.; Cao, L.; Fattah, R.J.; Yu, Z.; Bugge, T.H.; Finkel, T.; Leppla, S.H. Solid tumor therapy by selectively targeting stromal endothelial cells. Proc. Natl. Acad. Sci. USA 2016, 113, E4079–E4087. [Google Scholar] [CrossRef] [Green Version]
- Sugiura, K.; Chester, S.C.; Sugiura, M. Studies in a tumor spectrum. II. The growth of a variety of mouse and rat tumors. Cancer 1952, 5, 979–991. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, S.M.; Thamm, D.H.; Vail, D.M.; London, C.A. Response evaluation criteria for solid tumours in dogs (v1.0): A Veterinary Cooperative Oncology Group (VCOG) consensus document. Vet. Comp. Oncol. 2015, 13, 176–183. [Google Scholar] [CrossRef]
- Paoloni, M.; Khanna, C. Translation of new cancer treatments from pet dogs to humans. Nat. Rev. Cancer 2008, 8, 147–156. [Google Scholar] [CrossRef]
- Lindblad-Toh, K.; Wade, C.M.; Mikkelsen, T.S.; Karlsson, E.K.; Jaffe, D.B.; Kamal, M.; Clamp, M.; Chang, J.L.; Kulbokas, E.J.; Zody, M.C.; et al. Genome sequence, comparative analysis and haplotype structure of the domestic dog. Nature 2005, 438, 803–819. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.M.; Bastian, B.C.; Michael, H.T.; Webster, J.D.; Prasad, M.L.; Conway, C.M.; Prieto, V.M.; Gary, J.M.; Goldschmidt, M.H.; Esplin, D.G.; et al. Sporadic naturally occurring melanoma in dogs as a preclinical model for human melanoma. Pigment Cell Melanoma Res. 2014, 27, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Gillard, M.; Cadieu, E.; De Brito, C.; Abadie, J.; Vergier, B.; Devauchelle, P.; Degorce, F.; Dréano, S.; Primot, A.; Dorso, L.; et al. Naturally occurring melanomas in dogs as models for non-UV pathways of human melanomas. Pigment Cell Melanoma Res. 2014, 27, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Ezzell, J.W.; Ivins, B.E.; Leppla, S.H. Immunoelectrophoretic analysis, toxicity, and kinetics of in vitro production of the protective antigen and lethal factor components of Bacillus anthracis toxin. Infect. Immun. 1984, 45, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wein, A.N.; Peters, D.E.; Valivullah, Z.; Hoover, B.J.; Tatineni, A.; Ma, Q.; Fattah, R.; Bugge, T.H.; Leppla, S.H.; Liu, S. An anthrax toxin variant with an improved activity in tumor targeting. Sci Rep. 2015, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Wang, H.; Currie, B.M.; Molinolo, A.; Leung, H.J.; Moayeri, M.; Basile, J.R.; Alfano, R.W.; Gutkind, J.S.; Frankel, A.E.; et al. Matrix metalloproteinase-activated anthrax lethal toxin demonstrates high potency in targeting tumor vasculature. J. Biol. Chem. 2008, 283, 529–540. [Google Scholar] [CrossRef] [Green Version]
- Duesbery, N.S.; Webb, C.P.; Leppla, S.H.; Gordon, V.M.; Klimpel, K.R.; Copeland, T.D.; Ahn, N.G.; Oskarsson, M.K.; Fukasawa, K.; Paull, K.D.; et al. Proteolytic inactivation of MAP-kinase-kinase by anthrax lethal factor. Science 1998, 280, 734–737. [Google Scholar] [CrossRef]
- Moayeri, M.; Leppla, S.H.; Vrentas, C.; Pomerantsev, A.P.; Liu, S. Anthrax Pathogenesis. Annu. Rev. Microbiol. 2015, 69, 185–208. [Google Scholar] [CrossRef]
- Abi-Habib, R.J.; Singh, R.; Leppla, S.H.; Greene, J.J.; Ding, Y.; Berghuis, B.; Duesbery, N.S.; Frankel, A.E. Systemic Anthrax Lethal Toxin Therapy Produces Regressions of Subcutaneous Human Melanoma Tumors in Athymic Nude Mice. Clin. Cancer Res. 2006, 12, 7437–7443. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.; Ortiz, J.; Liu, S.; Bugge, T.H.; Singh, R.; Leppla, S.H.; Frankel, A.E. Systematic urokinase-activated anthrax toxin therapy produces regressions of subcutaneous human non-small cell lung tumor in athymic nude mice. Cancer Res. 2007, 67, 3329–3336. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Netzel-Arnett, S.; Birkedal-Hansen, H.; Leppla, S.H. Tumor cell-selective cytotoxicity of matrix metalloproteinase-activated anthrax toxin. Cancer Res. 2000, 60, 6061–6067. [Google Scholar] [PubMed]
- Abi-Habib, R.J.; Singh, R.; Liu, S.; Bugge, T.H.; Leppla, S.H.; Frankel, A.E. A urokinase-activated recombinant anthrax toxin is selectively cytotoxic to many human tumor cell types. Mol. Cancer Ther. 2006, 5, 2556–2562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, D.E.; Hoover, B.; Cloud, L.G.; Liu, S.; Molinolo, A.A.; Leppla, S.H.; Bugge, T.H. Comparative toxicity and efficacy of engineered Bacillus anthracis lethal toxin variants with broad anti-tumor activities. Toxicol. Appl. Pharmacol. 2014, 279, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brossier, F.; Le, M.; Landier, A.; Lafaye, P. Functional Analysis of Bacillus anthracis Protective Antigen by Using Neutralizing Monoclonal Antibodies. Society 2004, 72, 6313–6317. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Dog | Breed; Gender; Age; Weight (Kg) | Staging A (I-IV) | Histological Type B | Initial Volume C (mm3) | Main Diameter (mm) | Localization |
|---|---|---|---|---|---|---|
| 1 | Yorkshire; Male; 11; 5,4 | III (T2N1bM0) | Amelanotic, epithelioid | 18602 | 50,6 | Left mandible |
| 2 | Daschund; Male; 14; 7,3 | III (T2N1bM0) | Melanotic, spindle | 2509 | 36,5 | Left maxilla |
| 3 | Mongrel; Female; 16; 5,7 | III (T2N1bM0) | Melanotic balloon cells | 8875 | 35,4 | Right maxilla |
| 4 | Labrador; Male; 14; 33,3 | III (T2N1bM0) | Melanotic, desmoplastic | 7613 | 37,5 | Pre maxilla |
| 5 | Lhasa Apso; Male; 12; 5,0 | I (T1aN0M0) | Melanotic, spindle | 228,3 | 7,7 | Hard palate |
| Dog/Breed | Tumor Volume Day 0 (mm3) A | Tumor Volume Day 7 or 14 (mm3) A | % of Tumor Reduction |
|---|---|---|---|
| 1 Yorkshire terrier | 18602 | 16402 (day 14) | 12% |
| 2 Daschund | 2509 | 1341 (day 14) | 47% |
| 3 Mongrel | 8895 | 10754 (day 7) | 20% (+) |
| 4 Labrador retriever | 7613 | 2847 (day 7) | 63% |
| 5 Lhasa apso | 228,3 | 148 (day 7) | 34% |
| Dog | PCV (%) (b/a) | Leukocytes (×1000cels/μL) (b/a) | Alanine transferase (U/L) (b/a) | Alkaline Phosphatase (U/L) (b/a) | Urea (mg/dl) (b/a) | Creatinin (mg/dl) (b/a) | Platelet (×1000/mL) (b/a) | Weeks after Treatments |
|---|---|---|---|---|---|---|---|---|
| 1 | 46/40 | 19,9/28,4 | 43/12 | 29/69 | 43/47 | 1,0/0,8 | 366/285 | 5 |
| 2 | 50/43 | 34/12,9 | 31/56 | 248/655 | 58/34 | 0,7/0,9 | 569/407 | 9 |
| 3 | 34/25 | 29,6/14,1 | 99/264 | 395/691 | 64/94 | 1,3/1,3 | 678/474 | 14 |
| 4 | 43/41 | 13,7/6,1 | 57/60 | 110/92 | 25/35 | 0,8/0,8 | 392/312 | 21 |
| 5 | 47/44 | 6,3/8,69 | 56/52 | 131/138 | 43/155 | 1,2/1,0 | 438/553 | 22 |
| Dog | Breed; Gender; Age; Weight (Kg) | Histological Type A | Main Diameter (mm) before Toxin Inoculation B | Main Diameter (mm) after Toxin InoculationB | cRECISTB |
|---|---|---|---|---|---|
| 1 | Yorkshire terrier; Male; 11; 5,4 | Amelanotic, epithelioid | 50,6 | 45 | Stable disease |
| 2 | Daschund; Male; 14, 7,3 | Melanotic, spindle | 36,5 | 32,1 | Stable disease |
| 3 | Mongrel; Female; 16; 5,7 | Melanotic balloon cells | 35,4 | 35,1 | Stable disease |
| 4 | Labrador; Male; 14; 33,3 | Melanotic, desmoplasic | 37,5 | 32,3 | Stable disease |
| 5 | Lhasa Apso; Male; 12; 5,0 | Melanotic, spindle | 7,7 | 6,7 | Stable disease |
| Dog | Necrosis/ Endothelial Cells Necrosis after Treatment | Ki67 Positive Cells Quantification (%) before Treatment | Ki67 Positive Cells Quantification (%) after Treatment |
|---|---|---|---|
| 1 | Yes/no | ≥19 | ≥19 |
| 2 | Yes/no | ≥19 | 12,2 |
| 3 | Yes/yes | ≥19 | 7 |
| 4 | Yes/yes | 8,2 | 4,6 |
| 5 | Yes/yes | 3,6 | 16 |
| Dog | uPA | uPAr | MMP-2 | MT1-MMP | TIMP-2 |
|---|---|---|---|---|---|
| 1 | + | + | - | + | + |
| 2 | + | + | + | + | + |
| 3 | + | + | + | + | + |
| 4 | + | + | + | + | + |
| 5 | + | + | + | + | + |
| Criteria | Ideal Condition |
|---|---|
| Histopathological or cytological diagnosis | Melanoma |
| Localization of the tumor | Oral cavity (mandible or maxila), and measurable with a pachimeter |
| Radiographic exam of the thorax | No metastasis in lungs |
| Ultrasound examination of abdomen | No metastasis in liver and spleen |
| Complete blood examination, serum biochemistry for liver and kidney function | Good general condition. |
| Antibody | Code | Mono/ Polyclonal | Mouse or Rabbit | Dilution | Subcellular Localization |
|---|---|---|---|---|---|
| uPA H140–Santa Cruz | Sc14019 | Polyclonal | rabbit | 1:200 | Cytoplasm |
| uPAR–Dako | M7294 | Monoclonal | mouse | 1:200 | Membrane |
| MMP-2– Abcam | Ab86607 | Monoclonal | mouse | 1:200 | Membrane |
| MT1-MMP–Abcam | Ab53712 | Polyclonal | rabbit | 1:200 | Membrane |
| TIMP-2–Abcam | b1828 | Monoclonal | mouse | 1:200 | Membrane |
| Ki67–Dako | M7240 | Monoclonal | Mouse | 1:50 | Nucleus |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishiya, A.T.; Nagamine, M.K.; Fonseca, I.I.M.d.; Miraldo, A.C.; Villar Scattone, N.; Guerra, J.L.; Xavier, J.G.; Santos, M.; Massoco de Salles Gomes, C.O.; Ward, J.M.; et al. Inhibitory Effects of a Reengineered Anthrax Toxin on Canine Oral Mucosal Melanomas. Toxins 2020, 12, 157. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030157
Nishiya AT, Nagamine MK, Fonseca IIMd, Miraldo AC, Villar Scattone N, Guerra JL, Xavier JG, Santos M, Massoco de Salles Gomes CO, Ward JM, et al. Inhibitory Effects of a Reengineered Anthrax Toxin on Canine Oral Mucosal Melanomas. Toxins. 2020; 12(3):157. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030157
Chicago/Turabian StyleNishiya, Adriana Tomoko, Marcia Kazumi Nagamine, Ivone Izabel Mackowiak da Fonseca, Andrea Caringi Miraldo, Nayra Villar Scattone, José Luiz Guerra, José Guilherme Xavier, Mário Santos, Cristina Oliveira Massoco de Salles Gomes, Jerrold Michael Ward, and et al. 2020. "Inhibitory Effects of a Reengineered Anthrax Toxin on Canine Oral Mucosal Melanomas" Toxins 12, no. 3: 157. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030157