Rectus Femoris Characteristics in Post Stroke Spasticity: Clinical Implications from Ultrasonographic Evaluation

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Conclusions
5. Materials and Methods
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
| RF | rectus femoris |
| SKG | stiff knee gait |
| BoNT-A | botulinum toxin type A |
| MD | Muscle depth |
| MT | Muscle Thickness |
| CSA | Cross-sectional Area |
| MEI | Mean Echo Intensity |
| MAS | Modified Ashworth Scale |
| ES | electrical stimulation |
| JCP | juvenile cerebral palsy |
References
- Lance, J. Symposium. In Spasticity: Disordered Motor Control; Year Book Medical Pubs.: Chicago, IL, USA, 1980; pp. 485–495. [Google Scholar]
- Perry, J. Gait analysis: Normal and pathological function. J. Pediatr. Orthop. 1992, 12, 815. [Google Scholar] [CrossRef]
- Riley, P.O.; Kerrigan, D.C. Torque action of two-joint muscles in the swing period of stiff-legged gait: A forward dynamic model analysis. J. Biomech. 1998, 31, 835–840. [Google Scholar] [CrossRef]
- Stoquart, G.G.; Detrembleur, C.; Palumbo, S.; Deltombe, T.; Lejeune, T. Effect of botulinum toxin injection in the rectus femoris on stiff-knee gait in people with stroke: A prospective observational study. Arch. Phys. Med. Rehabil. 2008, 89, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.C.; Goldberg, S.R.; Pandy, M.G.; Delp, S.L. Contributions of muscle forces and toe-off kinematics to peak knee flexion during the swing phase of normal gait: An induced position analysis. J. Biomech. 2004, 37, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Sung, D.H.; Bang, H.J. Motor branch block of the rectus femoris: Its effectiveness in stiff-legged gait in spastic paresis. Arch. Phys. Med. Rehabil. 2000, 81, 910–915. [Google Scholar] [CrossRef]
- Zakin, E.; Simpson, D. Evidence on botulinum toxin in selected disorders. Toxicon 2018, 147, 134–140. [Google Scholar] [CrossRef]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [Green Version]
- Baskaran, P.; Thyagarajan, B. Acute and chronic effects of botulinum neurotoxin A on the mammalian neuromuscular junction. Muscle Nerve 2014, 50, 206–215. [Google Scholar] [CrossRef]
- Wissel, J.; Ward, A.B.; Erztgaard, P.; Bensmail, D.; Hecht, M.J.; Lejeune, T.M.; Schnider, L. European consensus table on the use of botulinum toxin type A in adult spasticity. J. Rehabil. Med. 2009, 41, 13–25. [Google Scholar] [CrossRef] [Green Version]
- Charles, D.; Gill, C.E. Neurotoxin injection for movement disorders. Contin. Lifelong Learn. Neurol. 2010, 16, 131–157. [Google Scholar] [CrossRef]
- Hutin, É.; Pradon, D.; Barbier, F.; Gracies, J.-M.; Bussel, B.; Roche, N. Lower limb coordination in hemiparetic subjects: Impact of botulinum toxin injections into rectus femoris. Neurorehabil. Neural Repair 2010, 24, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Schnitzler, A.; Roche, N.; Denormandie, P.; Lautridou, C.; Parratte, B.; Genêt, F. Manual needle placement: Accuracy of botulinum toxin a injections. Muscle Nerve 2012, 46, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Kaymak, B.; Kara, M.; Yağiz-On, A.; Soylu, A.R.; Özçakar, L. Innervation zone targeted botulinum toxin injections. Eur J. Phys Rehabil Med. 2017, 54, 100–109. [Google Scholar] [PubMed]
- Santamato, A.; Micello, M.F.; Panza, F.; Fortunato, F.; Baricich, A.; Cisari, C.; Pilotto, A.; Logroscino, G.; Fiore, P.; Ranieri, M. Can botulinum toxin type A injection technique influence the clinical outcome of patients with post-stroke upper limb spasticity? A randomized controlled trial comparing manual needle placement and ultrasound-guided injection techniques. J. Neurol. Sci. 2014, 347, 39–43. [Google Scholar] [CrossRef]
- Smania, N.; Colosimo, C.; Bentivoglio, A.R.; Sandrini, G.; Picelli, A. Use of botulinum toxin type A in the management of patients with neurological disorders: A national survey. Diet. Exerc. Cogn. Funct. Neurol. Dis. 2014, 28, 253–258. [Google Scholar]
- Behan, F.P.; Maden-Wilkinson, T.M.; Pain, M.T.G.; Folland, J.P. Sex differences in muscle morphology of the knee flexors and knee extensors. PLoS ONE 2018, 13, e0190903. [Google Scholar] [CrossRef]
- Evans, W.J.; Lexell, J. Human Aging, Muscle Mass, and Fiber Type Composition. J. Gerontol Ser. A Boil. Sci. Med. Sci. 1995, 50, 11–16. [Google Scholar] [CrossRef]
- Picelli, A.; Bonetti, P.; Fontana, C.; Barausse, M.; Dambruoso, F.; Gajofatto, F.; Tamburin, S.; Girardi, P.; Gimigliano, R.; Smania, N. Accuracy of botulinum toxin type A injection into the gastrocnemius muscle of adults with spastic equinus: Manual needle placement and electrical stimulation guidance compared using ultrasonography. J. Rehabil. Med. 2012, 44, 450–452. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, S.; Gormley, M.E.; Carey, J.R. Muscle fiber orientation in muscles commonly injected with botulinum toxin: An anatomical pilot study. Neurotox Res. 2006, 9, 115–120. [Google Scholar] [CrossRef]
- Picelli, A.; Tamburin, S.; Bonetti, P.; Fontana, C.; Barausse, M.; Dambruoso, F.; Gajofatto, F.; Santilli, V.; Smania, N. Botulinum Toxin Type A Injection into the Gastrocnemius Muscle for Spastic Equinus in Adults With Stroke. Am. J. Phys. Med. Rehabil. 2012, 91, 957–964. [Google Scholar] [CrossRef]
- Py, A.G.; ZeinAddeen, G.; Perrier, Y.; Carlier, R.Y.; Picard, A. Evaluation of the effectiveness of botulinum toxin injections in the lower limb muscles of children with cerebral palsy. Preliminary prospective study of the advantages of ultrasound guidance. Ann Phys. Rehabil. Med. 2009, 52, 215–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picelli, A.; Lobba, D.; Midiri, A.; Prandi, P.; Melotti, C.; Baldessarelli, S.; Smania, N. Botulinum toxin injection into the forearm muscles for wrist and fingers spastic overactivity in adults with chronic stroke: A randomized controlled trial comparing three injection techniques. Clin. Rehabil. 2013, 28, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Grigoriu, A.I.; Dinomais, M.; Rémy-Néris, O.; Brochard, S. Impact of injection-guiding techniques on the effectiveness of botulinum toxin for the treatment of focal spasticity and dystonia: A systematic review. Ann. Phys. Rehabil. Med. 2015, 58, e79. [Google Scholar] [CrossRef] [Green Version]
- Warnink-Kavelaars, J.; Vermeulen, R.J.; I Buizer, A.; Becher, J. Botulinum neurotoxin treatment in children with cerebral palsy: Validation of a needle placement protocol using passive muscle stretching and relaxing. Dev. Med. Child. Neurol. 2016, 58, 1281–1287. [Google Scholar] [CrossRef] [Green Version]
- Picelli, A.; Baricich, A.; Cisari, C.; Paolucci, S.; Smania, N.; Rossi, P. The Italian real-life post-stroke spasticity survey: Unmet needs in the management of spasticity with botulinum toxin type A. Funct. Neurol. 2017, 32, 89–96. [Google Scholar] [CrossRef]
- Picelli, A.; Bonetti, P.; Fontana, C.; Barausse, M.; Dambruoso, F.; Gajofatto, F.; Girardi, P.; Manca, M.; Gimigliano, R.; Smania, N. Is spastic muscle echo intensity related to the response to botulinum toxin type a in patients with stroke? A cohort study. Arch. Phys. Med. Rehabil. 2012, 93, 1253–1258. [Google Scholar] [CrossRef]
- Nijholt, W.; Scafoglieri, A.; Jager-Wittenaar, H.; Hobbelen, J.S.; Van Der Schans, C.P. The reliability and validity of ultrasound to quantify muscles in older adults: A systematic review. J. Cachex. Sarcopenia Muscle 2017, 8, 702–712. [Google Scholar] [CrossRef]
- Fukumoto, Y.; Ikezoe, T.; Yamada, Y.; Tsukagoshi, R.; Nakamura, M.; Mori, N.; Kimura, M.; Ichihashi, N. Skeletal muscle quality assessed from echo intensity is associated with muscle strength of middle-aged and elderly persons. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 112, 1519–1525. [Google Scholar] [CrossRef] [Green Version]
- Scherbakov, N.; Von Haehling, S.; Anker, S.D.; Dirnagl, U.; Doehner, W. Stroke induced Sarcopenia: Muscle wasting and disability after stroke. Int. J. Cardiol. 2013, 170, 89–94. [Google Scholar] [CrossRef]
- Park, E.S.; Sim, E.; Rha, D.-W.; Jung, S. Architectural changes of the gastrocnemius muscle after botulinum toxin type A injection in children with cerebral palsy. Yonsei Med. J. 2014, 55, 1406–1412. [Google Scholar] [CrossRef] [Green Version]
- Alexander, C.; Elliott, C.; Valentine, J.; Stannage, K.; Bear, N.; Donnelly, C.J.; Shipman, P.; Reid, S.L. Muscle volume alterations after first botulinum neurotoxin A treatment in children with cerebral palsy: A 6-month prospective cohort study. Dev. Med. Child. Neurol. 2018, 60, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Kawano, A.; Yanagizono, T.; Kadouchi, I.; Umezaki, T.; Chosa, E. Ultrasonographic evaluation of changes in the muscle architecture of the gastrocnemius with botulinum toxin treatment for lower extremity spasticity in children with cerebral palsy. J. Orthop. Sci. 2017, 23, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Park, G.-Y.; Kwon, D.R. Sonoelastographic evaluation of medial gastrocnemius muscles intrinsic stiffness after rehabilitation therapy with botulinum toxin a injection in spastic cerebral palsy. Arch. Phys. Med. Rehabil. 2012, 93, 2085–2089. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, A.S.; Ertl-Wagner, B.; Britsch, S.; Shroder, J.M.; Nikolin, S.; Weis, J.; Muller-Felber, W.; Koerte, I.; Stehr, M.; Berweck, S.; et al. Muscle biopsy substantiates long-term MRI alterations one year after a single dose of botulinum toxin injected into the lateral gastrocnemius muscle of healthy volunteers. Mov. Disord. 2009, 24, 1494–1503. [Google Scholar] [CrossRef]
- Harris, C.P.; Alderson, K.; Nebeker, J.; Holds, J.B.; Anderson, R.L. Histologic Features of Human Orbicularis Oculi Treated With Botulinum A Toxin. Arch. Ophthalmol. 1991, 109, 393–395. [Google Scholar] [CrossRef]
- Huang, L. Benefcial effect of botulinum toxin A on secondary ischaemic injury of skin flaps in rats. Br. J. Oral Maxillofac. Surg. 2018, 56, 144–147. [Google Scholar] [CrossRef]
- Negosanti, L.; Sanguinetti, G.; Gaiani, L.; Battilana, M.; Capirossi, R.; Landi, S.; Sgarzani, R. Spinal cord injury patients with spasticity and pressure sores: Preliminary report on reconstruction with botulinum toxin treated muscle flaps. Integr. Mol. Med. 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.L.; Jobling, P.; Gibbins, I.L. Botulinum neurotoxin A attenuates release of norepinephrine but not NPY from vasoconstrictor neurons. Am. J. Physiol. Circ. Physiol. 2002, 283, H2627–H2635. [Google Scholar] [CrossRef] [Green Version]
- Kaymak, B.; Kara, M.; Tok, F.; Ulasli, A.M.; Öztürk, G.T.; Chang, K.V.; Hsiao, M.Y.; Hung, C.Y.; Yağiz On, A.; Özçakar, L. Sonographic guide for botulinum toxin injections of the lower limb: Euro-musculus/USPRM spasticity approach. Eur. J. Phys. Rehabil. Med. 2018, 54, 469–485. [Google Scholar]
- Narici, M.V.; Roi, G.S.; Landoni, L.; Minetti, A.E.; Cerretelli, P. Changes in force, cross-sectional area and neural activation during strength training and detraining of the human quadriceps. Graefe’s Arch. Clin. Exp. Ophthalmol. 1989, 59, 310–319. [Google Scholar] [CrossRef]
- Strasser, E.-M.; Draskovits, T.; Praschak, M.; Quittan, M.; Graf, A. Association between ultrasound measurements of muscle thickness, pennation angle, echogenicity and skeletal muscle strength in the elderly. Age 2013, 35, 2377–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, P.J. The Behavior of Maximum Likelihood Estimates under Non Standard Conditions; University of California Press: Berkeley, CA, USA, 1967; pp. 221–233. [Google Scholar]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Harrell, F. Regression Modeling Strategies; Springer International Publishing; Springer Nature Switzerland AG: Springer, Switzerland, 2015. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age (years) Mean (SD) 25th–75th percentile | 64 (10.87) 55/72 |
| Gender (male/female) | 28/19 |
| Time Stroke/1st Treatment (years) 25th–75th percentile | 2.7 0.22/2.26 |
| Time 1st Treatment/Acquisition(years) 25th–75th percentile | 3.4 0.22/6.31 |
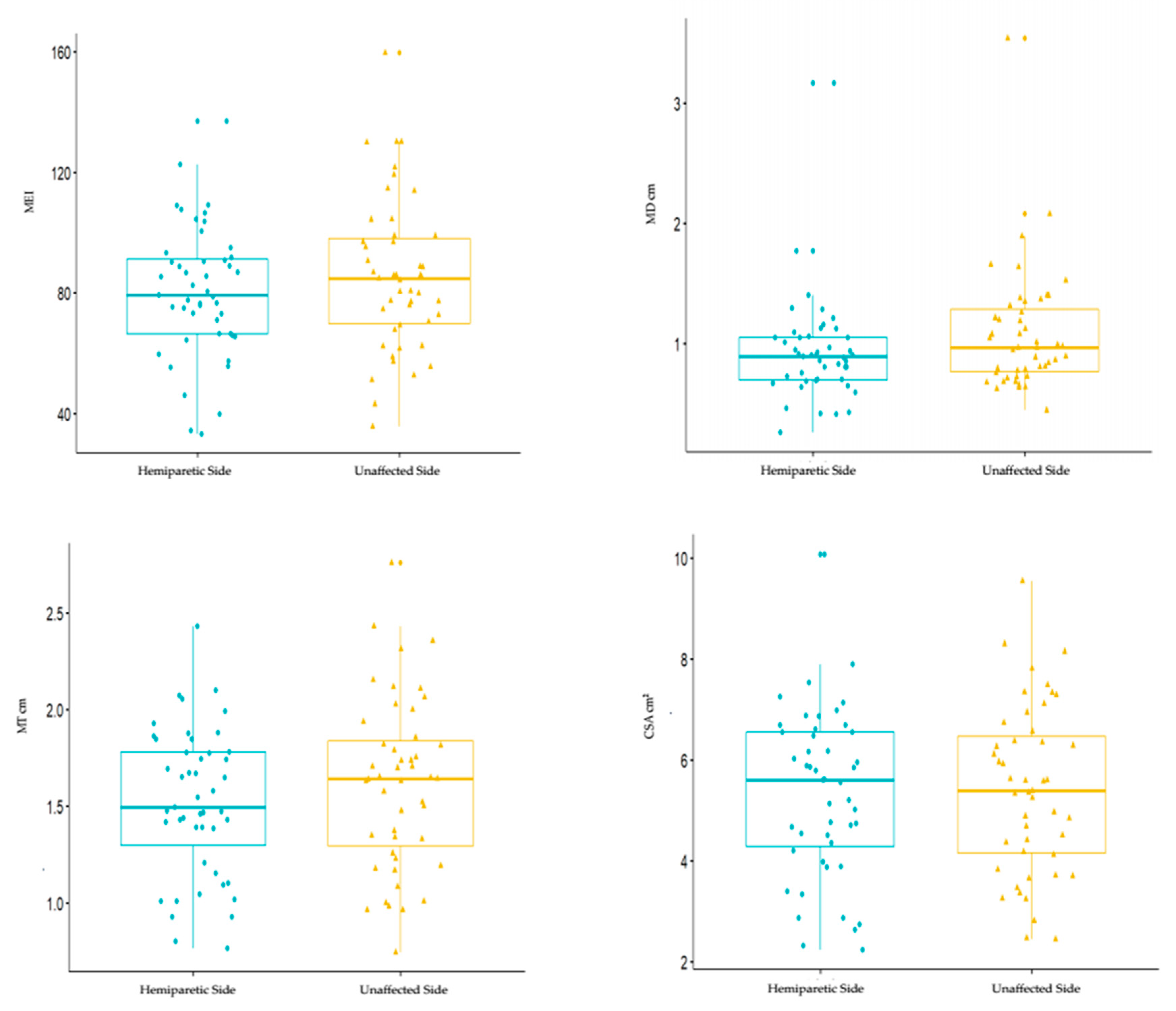
| Hemiparetic Side (N = 47) | Unaffected Side (N = 47) | Test | |
|---|---|---|---|
| 25th–75th percentile Median | 25th–75th percentile Median | Statistics | |
| MD (cm) | 0.76/1.28 1.08 | 0.69/1.05 0.92 | P = 0.09 |
| MT (cm) | 1.29/1.84 1.62 | 1.30/1.78 1.52 | P = 0.4 |
| CSA (cm2) | 4.15/6.47 5.41 | 4.28/6.55 5.33 | P = 0.89 |
| MEI | 69.8/98.0 85.7 | 66.5/91.3 80.4 | P = 0.46 |
| Hemiparetic Side Treated RF (N = 37) | Hemiparetic Side Untreated RF (N = 10) | Test | |
|---|---|---|---|
| 25th–75th percentile Median | 25th–75th percentile Median | Statistics | |
| MD (cm) | 0.79/1.35 1.11 | 0.69/1.17 0.97 | P = 0.36 |
| MT (cm) | 1.34/1.82 1.63 | 1.18/2.00 1.56 | P = 0.6 |
| CSA (cm2) | 4.18/6.37 5.45 | 3.70/6.46 5.26 | P = 0.76 |
| MEI | 72.6/97.0 84.5 | 61.4/115. 4 89.8 | P = 0.90 |
| Coefficient MD (cm) | S.E. | p-Value MD | Coefficient MT (cm) | S.E. | p-Value MT | Coefficient CSA (cm2) | S.E. | p-Value CSA | |
|---|---|---|---|---|---|---|---|---|---|
| Age | 0.0015 | 0.004 | 0.7281 | -0.0139 | 0.003 | <0.0001 * | −0.0493 | 0.013 | 0.0003 * |
| Gender (male) | −0.4313 | 0.132 | 0.0016 * | 0.3109 | 0.087 | 0.0006 * | 1.4918 | 0.386 | 0.0002 * |
| Age/side effect (unaffected) | −0.0035 | 0.003 | 0.1810 | 0.0105 | 0.056 | 0.0632 | 0.0184 | 0.88 | 0.3812 |
| Gender/side effect (unaffected) | −0.0878 | 0.054 | 0.1071 | 0.0616 | 0.113 | 0.5865 | −0.1085 | −0.24 | 0.8083 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosenza, L.; Picelli, A.; Azzolina, D.; Minetto, M.A.; Invernizzi, M.; Bertoni, M.; Santamato, A.; Baricich, A. Rectus Femoris Characteristics in Post Stroke Spasticity: Clinical Implications from Ultrasonographic Evaluation. Toxins 2020, 12, 490. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12080490
Cosenza L, Picelli A, Azzolina D, Minetto MA, Invernizzi M, Bertoni M, Santamato A, Baricich A. Rectus Femoris Characteristics in Post Stroke Spasticity: Clinical Implications from Ultrasonographic Evaluation. Toxins. 2020; 12(8):490. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12080490
Chicago/Turabian StyleCosenza, Lucia, Alessandro Picelli, Danila Azzolina, Marco Alessandro Minetto, Marco Invernizzi, Michele Bertoni, Andrea Santamato, and Alessio Baricich. 2020. "Rectus Femoris Characteristics in Post Stroke Spasticity: Clinical Implications from Ultrasonographic Evaluation" Toxins 12, no. 8: 490. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12080490