The Effects of Botulinum Toxin Injections on Spasticity and Motor Performance in Chronic Stroke with Spastic Hemiplegia

Abstract
:1. Introduction
2. Results
2.1. Elbow Flexor Spasticity
2.2. Maximum Voluntary Contraction (MVC) Tasks
2.3. Force Control Performance
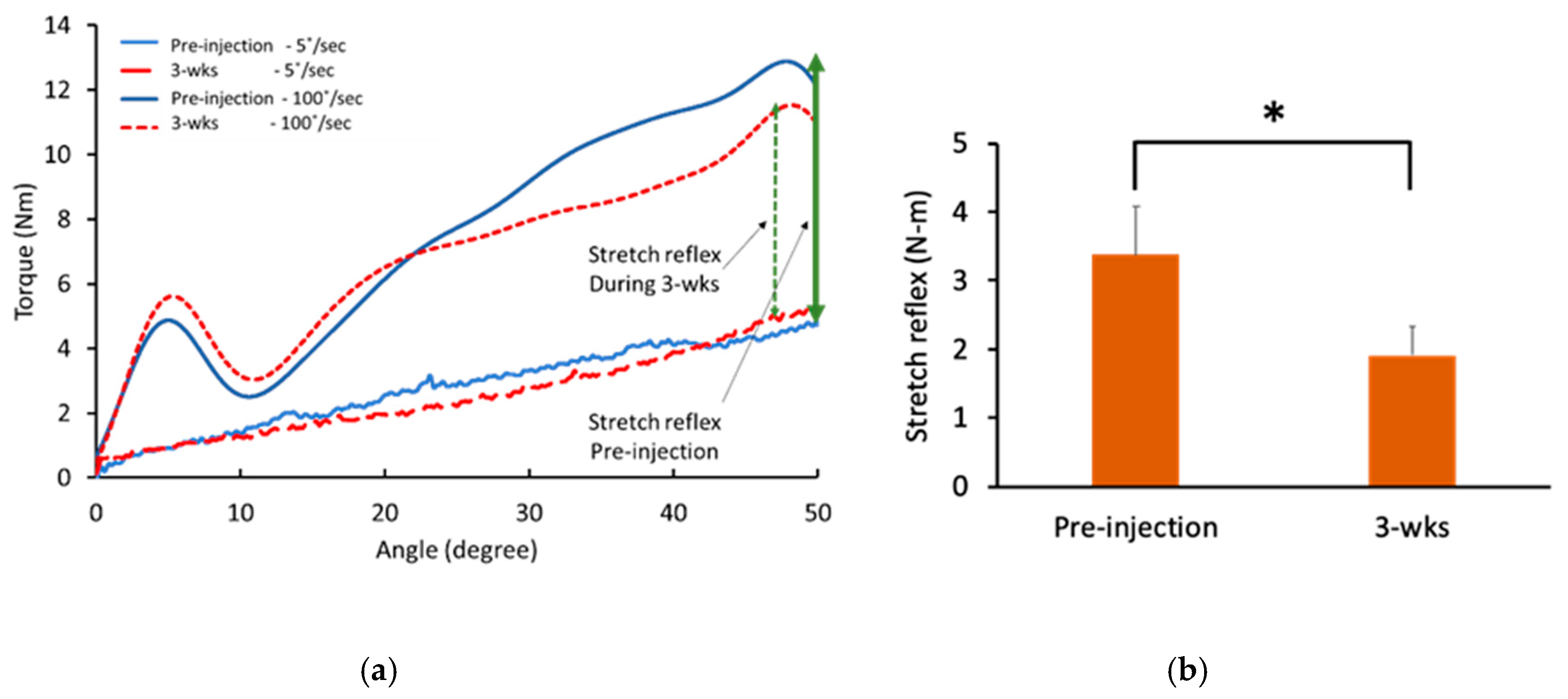
2.4. Reflex Torque
3. Discussion
3.1. Effects of BoNT on and Quantification of Spasticity
3.2. Motor Performance after BoNT
4. Conclusions
5. Materials and Methods
5.1. Participants
5.2. Experimental Protocol
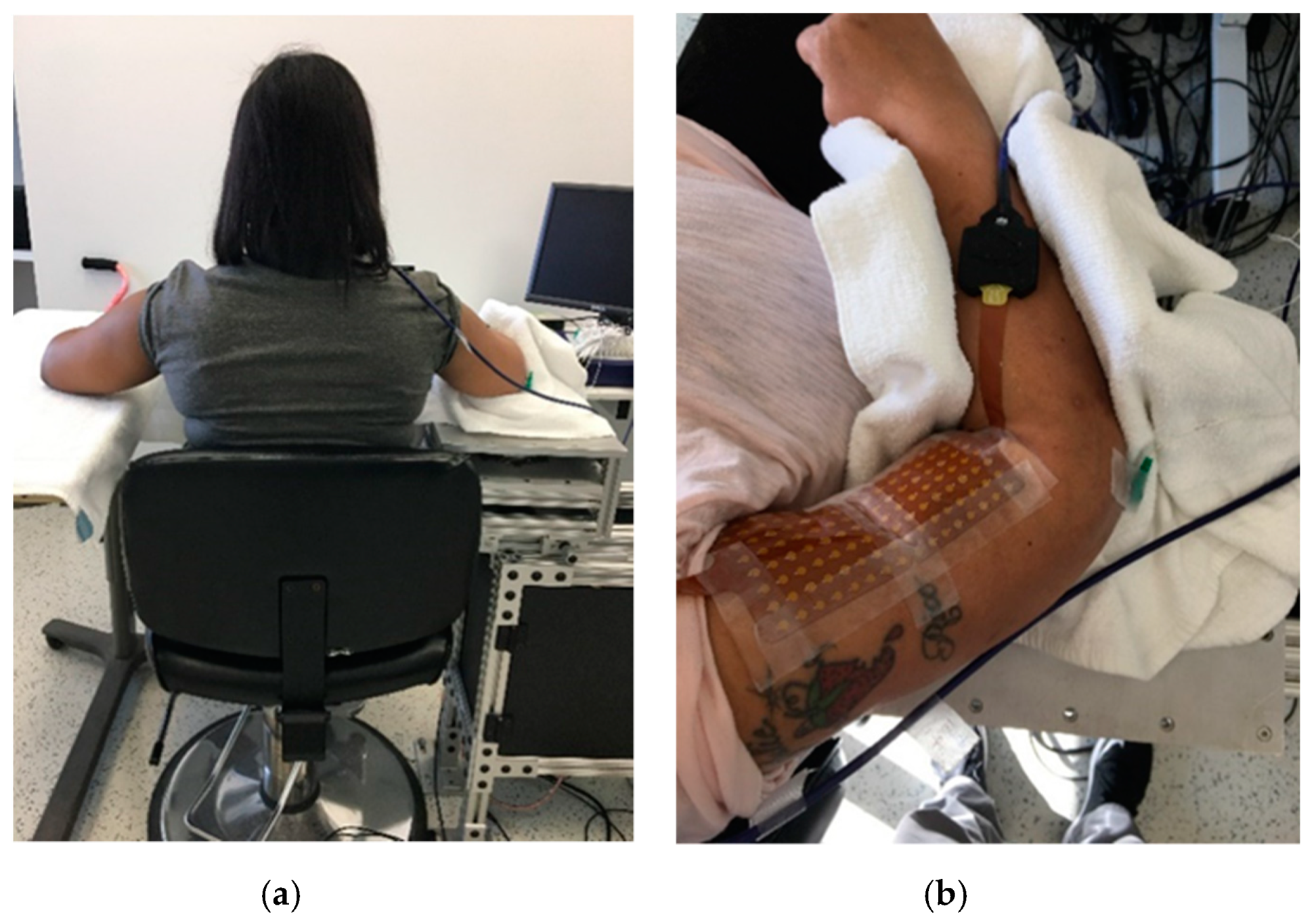
5.3. Experimental Set-Up
5.4. Data Analysis
5.4.1. Force Control Performance
5.4.2. Reflex Torque
5.5. Statictical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Li, S.; Liu, J.; Bhadane, M.; Zhou, P.; Rymer, W.Z. Activation deficit correlates with weakness in chronic stroke: Evidence from evoked and voluntary EMG recordings. Clin. Neurophysiol. 2014, 125, 2413–2417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamper, D.G.; Fischer, H.C.; Cruz, E.G.; Rymer, W.Z. Weakness is the primary contributor to finger impairment in chronic stroke. Arch. Phys. Med. Rehabil. 2006, 87, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Zorowitz, R.D.; Gillard, P.J.; Brainin, M. Poststroke spasticity: Sequelae and burden on stroke survivors and caregivers. Neurology 2013, 80, S45–S52. [Google Scholar] [CrossRef]
- Pundik, S.; McCabe, J.; Skelly, M.; Tatsuoka, C.; Daly, J.J. Association of spasticity and motor dysfunction in chronic stroke. Ann. Phys. Rehabil. Med. 2019, 62, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Lance, J.W. Symposium synopsis. In Spasticity: Disordered motor control; Feldman, R.G., Young, R.R., Koella, W.P., Eds.; Year Book Medical Publishers: Chicago, IL, USA, 1980; pp. 485–494. [Google Scholar]
- Gracies, J.M.; Bayle, N.; Vinti, M.; Alkandari, S.; Vu, P.; Loche, C.M.; Colas, C. Five-step clinical assessment in spastic paresis. Eur. J. Phys. Rehabil. Med. 2010, 46, 411–421. [Google Scholar] [PubMed]
- O’Dwyer, N.; Ada, L.; Neilson, P. Spasticity and muscle contracture following stroke. Brain 1996, 119, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Schmit, B.D.; Dhaher, Y.; Dewald, J.P.; Rymer, W.Z. Reflex torque response to movement of the spastic elbow: Theoretical analyses and implications for quantification of spasticity. Ann. Biomed. Eng. 1999, 27, 815–829. [Google Scholar] [CrossRef]
- Kamper, D.G.; Rymer, W.Z. Quantitative features of the stretch response of extrinsic finger muscles in hemiparetic stroke. Muscle Nerve 2000, 23, 954–961. [Google Scholar] [CrossRef]
- Li, S.; Shin, H.; Zhou, P.; Li, X. Different Effects of Cold Stimulation on Reflex and Non-Reflex Components of Poststroke Spastic Hypertonia. Front. Neurol. 2017, 8, 169. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-T.; Li, S.; Magat, E.; Zhou, P.; Li, S. Motor Overflow and Spasticity in Chronic Stroke Share a Common Pathophysiological Process: Analysis of Within-Limb and Between-Limb EMG-EMG Coherence. Front. Neurol. 2018, 9, 795. [Google Scholar] [CrossRef] [Green Version]
- Mayer, N.H.; Esquenazi, A. Muscle overactivity and movement dysfunction in the upper motoneuron syndrome. Phys. Med. Rehabil. Clin. N. Am. 2003, 14, 855–883. [Google Scholar] [CrossRef]
- Chang, S.H.; Francisco, G.E.; Li, S. Botulinum Toxin (BT) injection improves voluntary motor control in selected patients with post-stroke spasticity. Neural Regen. Res. 2012, 7, 1436–1439. [Google Scholar] [PubMed]
- Seo, N.J.; Rymer, W.Z.; Kamper, D.G. Delays in grip initiation and termination in persons with stroke: Effects of arm support and active muscle stretch exercise. J. Neurophysiol. 2009, 101, 3108–3115. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.H.; Francisco, G.E.; Zhou, P.; Rymer, W.Z.; Li, S. Spasticity, weakness, force variability, and sustained spontaneous motor unit discharges of resting spastic-paretic biceps brachii muscles in chronic stroke. Muscle Nerve 2013, 48, 85–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlyle, J.K.; Mochizuki, G. Influence of post-stroke spasticity on EMG-force coupling and force steadiness in biceps brachii. J. Electromyogr. Kinesiol. 2018, 38, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Lodha, N.; Naik, S.K.; Coombes, S.A.; Cauraugh, J.H. Force control and degree of motor impairments in chronic stroke. Clin. Neurophysiol. 2010, 121, 1952–1961. [Google Scholar] [CrossRef]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [Green Version]
- de Paiva, A.; Meunier, F.A.; Molgó, J.; Aoki, K.R.; Dolly, J.O. Functional repair of motor endplates after botulinum neurotoxin type A poisoning: Biphasic switch of synaptic activity between nerve sprouts and their parent terminals. Proc. Natl. Acad. Sci. USA 1999, 96, 3200–3205. [Google Scholar] [CrossRef] [Green Version]
- Francisco, G.E.; Li, S. Spasticity. In Braddom’s Physical Medicine and Rehabilitation, 5th ed.; Elsevier: Philadelphia, PA, USA, 2015. [Google Scholar]
- Moeini-Naghani, I.; Hashemi-Zonouz, T.; Jabbari, B. Botulinum Toxin Treatment of Spasticity in Adults and Children. Semin. Neurol. 2016, 36, 64–72. [Google Scholar] [CrossRef]
- Rosales, R.L.; Chua-Yap, A.S. Evidence-based systematic review on the efficacy and safety of botulinum toxin-A therapy in post-stroke spasticity. J. Neural Transm. 2008, 115, 617–623. [Google Scholar] [CrossRef]
- Rosales, R.L.; Kong, K.H.; Goh, K.J.; Kumthornthip, W.; Mok, V.C.; Delgado-De Los Santos, M.M.; Chua, K.S.; Abdullah, S.J.; Zakine, B.; Maisonobe, P.; et al. Botulinum Toxin Injection for Hypertonicity of the Upper Extremity Within 12 Weeks After Stroke A Randomized Controlled Trial. Neurorehabilit. Neural Repair 2012, 26, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Wissel, J.; Ward, A.B.; Erztgaard, P.; Bensmail, D.; Hecht, M.J.; Lejeune, T.M.; Schnider, P. European consensus table on the use of botulinum toxin type A in adult spasticity. J. Rehabil. Med. 2009, 41, 13–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheean, G.; Lannin, N.A.; Turner-Stokes, L.; Rawicki, B.; Snow, B.J. Botulinum toxin assessment, intervention and after-care for upper limb hypertonicity in adults: International consensus statement. Eur. J. Neurol. 2010, 17, 74–93. [Google Scholar] [CrossRef] [PubMed]
- Bakheit, A.M.; Thilmann, A.F.; Ward, A.B.; Poewe, W.; Wissel, J.; Muller, J.; Benecke, R.; Collin, C.; Muller, F.; Ward, C.D.; et al. A randomized, double-blind, placebo-controlled, dose-ranging study to compare the efficacy and safety of three doses of botulinum toxin type A (Dysport) with placebo in upper limb spasticity after stroke. Stroke 2000, 31, 2402–2406. [Google Scholar] [CrossRef]
- Burridge, J.H.; Wood, D.E.; Hermens, H.J.; Voerman, G.E.; Johnson, G.R.; Wijck, F.V.; Platz, T.; Gregoric, M.; Hitchcock, R.; Pandyan, A.D. Theoretical and methodological considerations in the measurement of spasticity. Disabil. Rehabil. 2005, 27, 69–80. [Google Scholar] [CrossRef]
- Shaw, L.C.; Price, C.I.; van Wijck, F.M.; Shackley, P.; Steen, N.; Barnes, M.P.; Ford, G.A.; Graham, L.A.; Rodgers, H. Botulinum Toxin for the Upper Limb after Stroke (BoTULS) Trial: Effect on impairment, activity limitation, and pain. Stroke 2011, 42, 1371–1379. [Google Scholar] [CrossRef] [Green Version]
- Lampire, N.; Roche, N.; Carne, P.; Cheze, L.; Pradon, D. Effect of botulinum toxin injection on length and lengthening velocity of rectus femoris during gait in hemiparetic patients. Clin. Biomech. 2013, 28, 164–170. [Google Scholar] [CrossRef]
- Tenniglo, M.J.; Nederhand, M.J.; Prinsen, E.C.; Nene, A.V.; Rietman, J.S.; Buurke, J.H. Efefct of Chemodenervation of the Rectus Femoris Muscle in Adults With a Stiff Knee Gait Due to Spastic Paresis: A Systematic Review With a Meta-Analysis in Patients With Stroke. Arch. Phys. Med. Rehabil. 2014, 95, 576–587. [Google Scholar] [CrossRef]
- Holman Barden, H.L.; Baguley, I.J.; Nott, M.T.; Chapparo, C. Measuring spasticity and fine motor control (pinch) change in the hand following botulinum toxin-A injection using dynamic computerised hand dynamometry. Arch. Phys. Med. Rehabil. 2014, 5, 412–414. [Google Scholar]
- Simpson, D.M.; Gracies, J.M.; Graham, H.K.; Miyasaki, J.M.; Naumann, M.; Russman, B.; Simpson, L.L.; So, Y. Assessment: Botulinum neurotoxin for the treatment of spasticity (an evidence-based review) Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2008, 70, 1691–1698. [Google Scholar] [CrossRef] [Green Version]
- Bensmail, D.; Robertson, J.V.; Fermanian, C.; Roby-Brami, A. Botulinum toxin to treat upper-limb spasticity in hemiparetic patients: Analysis of function and kinematics of reaching movements. Neurorehabil. Neural Repair 2010, 24, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Andringa, A.; van de Port, I.; van Wegen, E.; Ket, J.; Meskers, C.; Kwakkel, G. Effectiveness of botulinum toxin treatment for upper limb spasticity after stroke over different ICF domains: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 1703–1725. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, A.; Smith, H.S. Botulinum toxins: Mechanisms of action, antinociception and clinical applications. Toxicology 2013, 306, 124–146. [Google Scholar] [CrossRef]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum neurotoxins: Biology, pharmacology, and toxicology. Pharmacol. Rev. 2017, 9, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Botulinum toxin: State of the art. Mov. Disord. 2017, 32, 1131–1138. [Google Scholar] [CrossRef]
- Phadke, C.P.; Balasubramanian, C.K.; Holz, A.; Davidson, C.; Ismail, F.; Boulias, C. Adverse Clinical Effects of Botulinum Toxin Intramuscular Injections for Spasticity. Can. J. Neurol. Sci. J. Can. Des Sci. Neurol. 2015, 43, 298–310. [Google Scholar] [CrossRef] [Green Version]
- Mas, M.F.; Li, S.; Francisco, G.E. Centrally mediated late motor recovery after botulinum toxin injection: Case reports and a review of current evidence. J. Rehabil. Med. 2017, 49, 609–619. [Google Scholar] [CrossRef] [Green Version]
- Fridman, E.A.; Crespo, M.; Argüello, S.G.; Degue, L.; Villarreal, M.; Bohlhalter, S.; Wheaton, L.; Hallett, M. Kinematic improvement following Botulinum Toxin-A injection in upper-limb spasticity due to stroke. J. Neurol. Neurosurg. Psychiatry 2010, 81, 423–427. [Google Scholar] [CrossRef]
- Patrick, E.; Ada, L. The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it. Clin. Rehabil. 2006, 20, 173–182. [Google Scholar] [CrossRef]
- Pandyan, A.D.; Vuadens, P.; van Wijck, F.M.J.; Stark, S.; Johnson, G.R.; Barnes, M.P. Are we underestimating the clinical efficacy of botulinum toxin (type A)? Quantifying changes in spasticity, strength and upper limb function after injections of Botox® to the elbow flexors in a unilateral stroke population. Clin. Rehabil. 2002, 16, 654–660. [Google Scholar] [CrossRef]
- Malhotra, S.; Cousins, E.; Ward, A.; Day, C.; Jones, P.; Roffe, C.; Pandyan, A. An investigation into the agreement between clinical, biomechanical and neurophysiological measures of spasticity. Clin. Rehabil. 2008, 22, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Kamper, D.G.; Rymer, W.Z. Effects of changing wrist positions on finger flexor hypertonia in stroke survivors. Muscle Nerve 2006, 33, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.F.; Jones, K.E.; Wolpert, D.M. The scaling of motor noise with muscle strength and motor unit number in humans. Exp. Brain Res. 2004, 157, 417–430. [Google Scholar] [CrossRef]
- Mottram, C.J.; Suresh, N.L.; Heckman, C.J.; Gorassini, M.A.; Rymer, W.Z. Origins of abnormal excitability in biceps brachii motoneurons of spastic-paretic stroke survivors. J. Neurophysiol. 2009, 102, 2026–2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottram, C.J.; Wallace, C.L.; Chikando, C.N.; Rymer, W.Z. Origins of spontaneous firing of motor units in the spastic-paretic biceps brachii muscle of stroke survivors. J. Neurophysiol. 2010, 104, 3168–3179. [Google Scholar] [CrossRef] [Green Version]
- Kallenberg, L.A.; Hermens, H.J. Motor unit properties of biceps brachii in chronic stroke patients assessed with high-density surface EMG. Muscle Nerve 2009, 39, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Chen, Y.T.; Francisco, G.E.; Zhou, P.; Rymer, W.Z. A Unifying Pathophysiological Account for Post-stroke Spasticity and Disordered Motor Control. Front. Neurol. 2019, 10, 468. [Google Scholar] [CrossRef]
- Pandyan, A.; Gregoric, M.; Barnes, M.P.; Wood, D.; Wijck, F.V.; Burridge, J.; Hermens, H.; Johnson, G.R. Spasticity: Clinical perceptions, neurological realities and meaningful measurement. Disabil. Rehabil. 2005, 27, 2–6. [Google Scholar] [CrossRef]
- Li, S. Spasticity, Motor Recovery, and Neural Plasticity after Stroke. Front. Neurol. 2017, 8, 120. [Google Scholar] [CrossRef] [Green Version]
- Seo, N.J.; Fischer, H.W.; Bogey, R.A.; Rymer, W.Z.; Kamper, D.G. Effect of a serotonin antagonist on delay in grip muscle relaxation for persons with chronic hemiparetic stroke. Clin. Neurophysiol. 2011, 122, 796–802. [Google Scholar] [CrossRef]
- Levy, J.; Molteni, F.; Cannaviello, G.; Lansaman, T.; Roche, N.; Bensmail, D. Does botulinum toxin treatment improve upper limb active function? Ann. Phys. Rehabil. Med. 2019, 62, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Hara, T.; Momosaki, R.; Niimi, M.; Yamada, N.; Hara, H.; Abo, M. Botulinum Toxin Therapy Combined with Rehabilitation for Stroke: A Systematic Review of Effect on Motor Function. Toxins 2019, 11, 707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhadane, M.Y.; Gao, F.; Francisco, G.E.; Zhou, P.; Li, S. Correlation of resting elbow angle with spasticity in chronic stroke survivors. Front. Neurol. 2015, 6, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, A.; Ando, R.; Akima, H. Effects of prolonged vibration to vastus intermedius muscle on force steadiness of knee extensor muscles during isometric force-matching task. J. Electromyogr. Kinesiol. 2016, 31, 48–54. [Google Scholar] [CrossRef]
- Limonta, E.; Rampichini, S.; Cè, E.; Esposito, F. Effects of visual feedback absence on force control during isometric contraction. Eur. J. Appl. Physiol. 2015, 115, 507–519. [Google Scholar] [CrossRef] [Green Version]
- Lodha, N.; Misra, G.; Coombes, S.A.; Christou, E.A.; Cauraugh, J.H. Increased force variability in chronic stroke: Contributions of force modulation below 1 Hz. PLoS ONE 2013, 8, e83468. [Google Scholar] [CrossRef]
- Skinner, J.W.; Christou, E.A.; Hass, C.J. Lower Extremity Muscle Strength and Force Variability in Persons With Parkinson Disease. J. Neurol. Phys. Ther. JNPT 2019, 43, 56–62. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ID | Age | Gender | History of Stroke (Months) | Paretic Side | Dominant Side | Elbow Flexor MAS (1st) | Elbow Flexor MAS (2nd) | Lesion Type |
|---|---|---|---|---|---|---|---|---|
| 1 | 60 | M | 23 | Left | Right | 2 | 2 | Hemorrhagic |
| 2 | 52 | F | 104 | Left | Right | 2 | 1+ | Ischemic |
| 3 | 63 | M | 137 | Left | Right | 2 | 1+ | Ischemic |
| 4 | 40 | F | 77 | Right | Right | 2 | 1+ | Ischemic |
| 5 | 49 | M | 7 | Right | Right | 2 | 1+ | Ischemic |
| 6 | 40 | M | 39 | Right | Right | 2 | 1+ | Hemorrhagic |
| 7 | 68 | F | 7 | Left | Right | 2 | 2 | Ischemic |
| 8 | 65 | M | 29 | Left | Right | 2 | 1+ | Hemorrhagic |
| 9 | 39 | F | 76 | Right | Right | 2 | 1 | Hemorrhagic |
| 10 | 46 | F | 117 | Right | Right | 3 | 2 | Ischemic |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-T.; Zhang, C.; Liu, Y.; Magat, E.; Verduzco-Gutierrez, M.; Francisco, G.E.; Zhou, P.; Zhang, Y.; Li, S. The Effects of Botulinum Toxin Injections on Spasticity and Motor Performance in Chronic Stroke with Spastic Hemiplegia. Toxins 2020, 12, 492. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12080492
Chen Y-T, Zhang C, Liu Y, Magat E, Verduzco-Gutierrez M, Francisco GE, Zhou P, Zhang Y, Li S. The Effects of Botulinum Toxin Injections on Spasticity and Motor Performance in Chronic Stroke with Spastic Hemiplegia. Toxins. 2020; 12(8):492. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12080492
Chicago/Turabian StyleChen, Yen-Ting, Chuan Zhang, Yang Liu, Elaine Magat, Monica Verduzco-Gutierrez, Gerard E. Francisco, Ping Zhou, Yingchun Zhang, and Sheng Li. 2020. "The Effects of Botulinum Toxin Injections on Spasticity and Motor Performance in Chronic Stroke with Spastic Hemiplegia" Toxins 12, no. 8: 492. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12080492