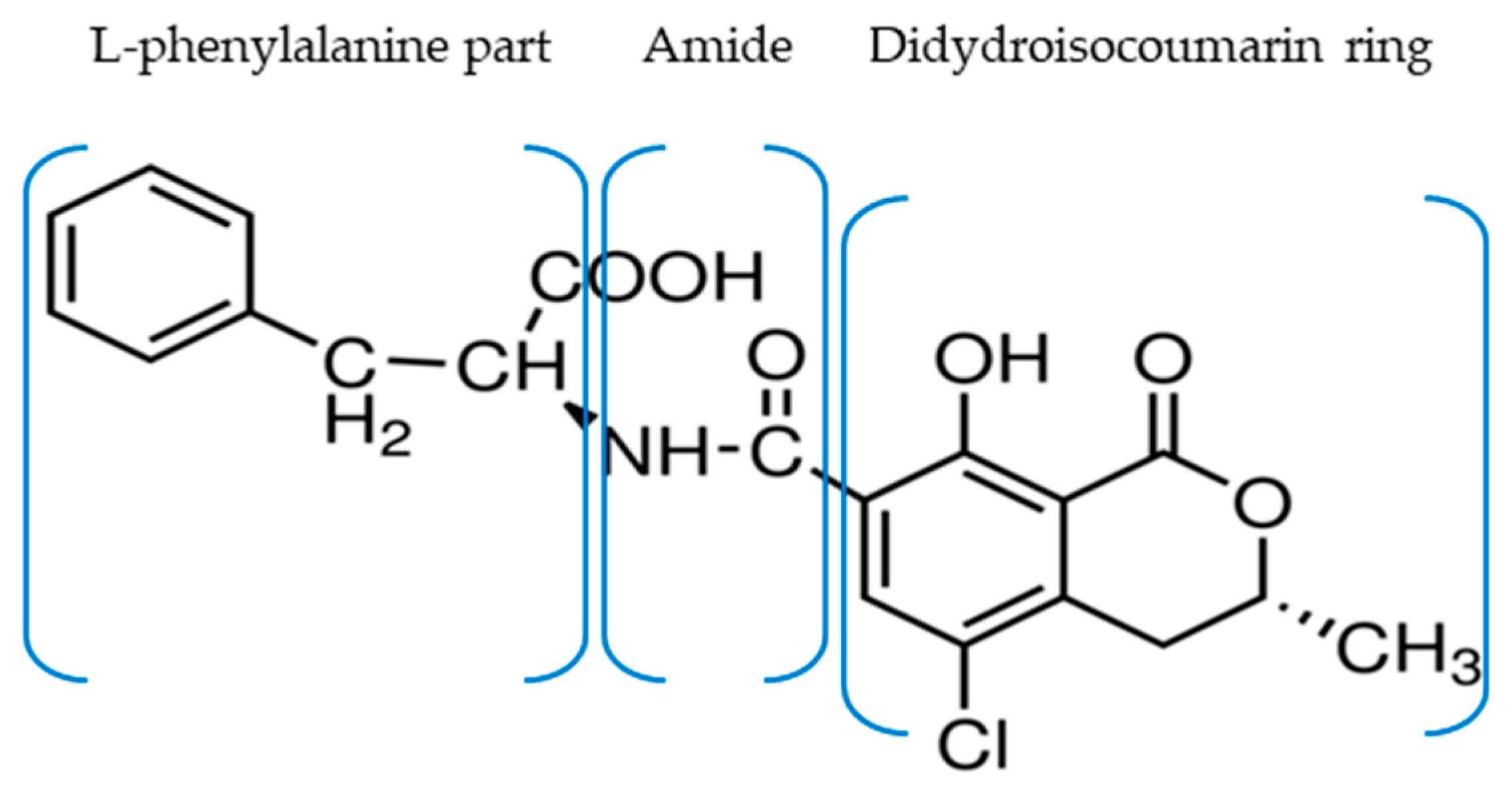
An Immunoenzymatic Method for the Determination of Ochratoxin A in Biological Liquids (Colostrum and Cow’s Milk)

 ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Validation of the Direct, Competitive Immunoenzymatic Method
2.1.1. Performance of the Method
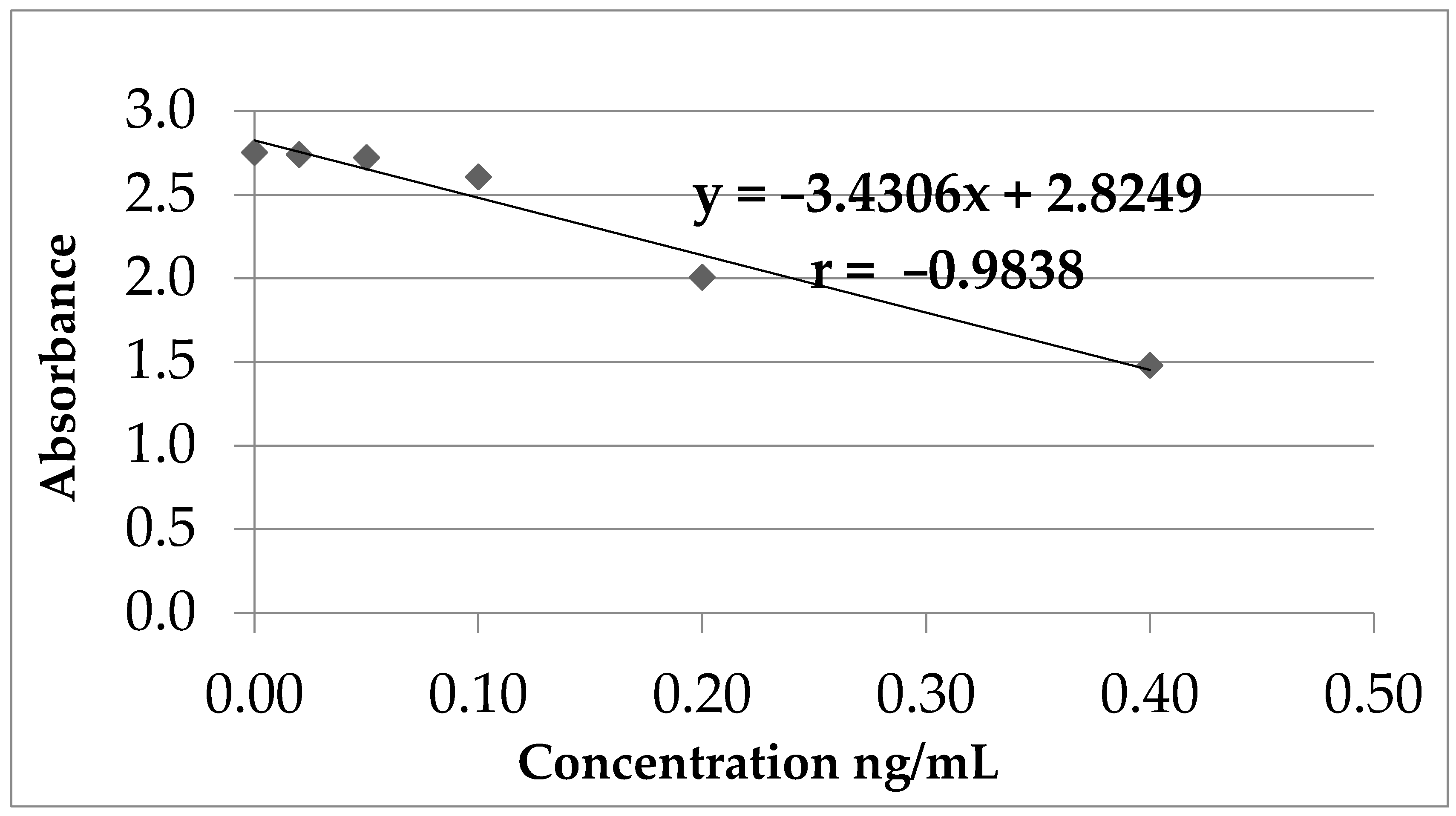
2.1.2. Method Linearity (Calibration Curve)
2.1.3. The Minimum Detection Limit (Milk)
2.1.4. The Minimum Limit of Quantification (Milk)
2.1.5. Recovery (Recovery Percentage)
- -
- equation of calibration line: y = −3.4306x + 2.8249
- -
- standard error of regression line: ES = 0.1052
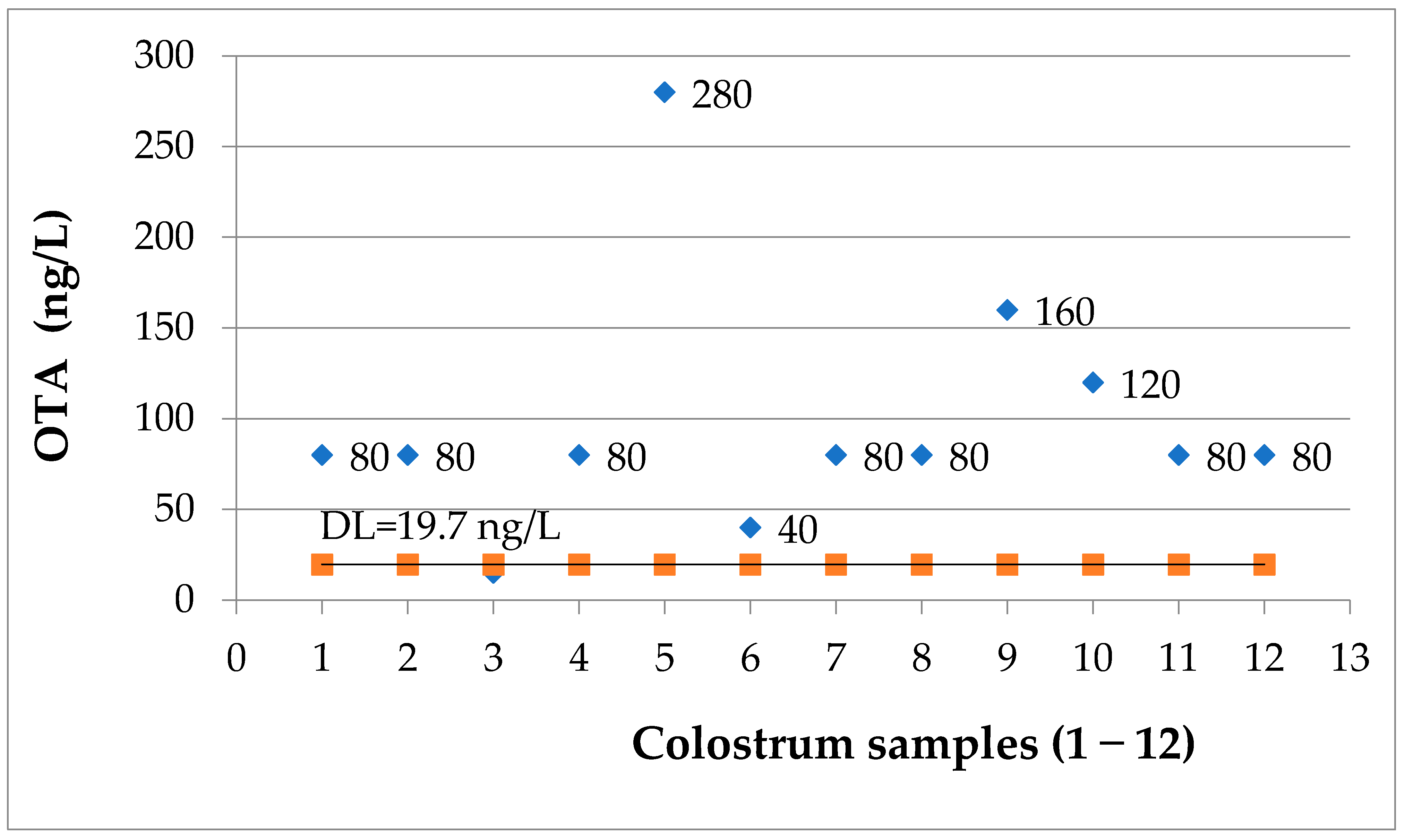
2.2. Determination of OTA in Human Milk Samples
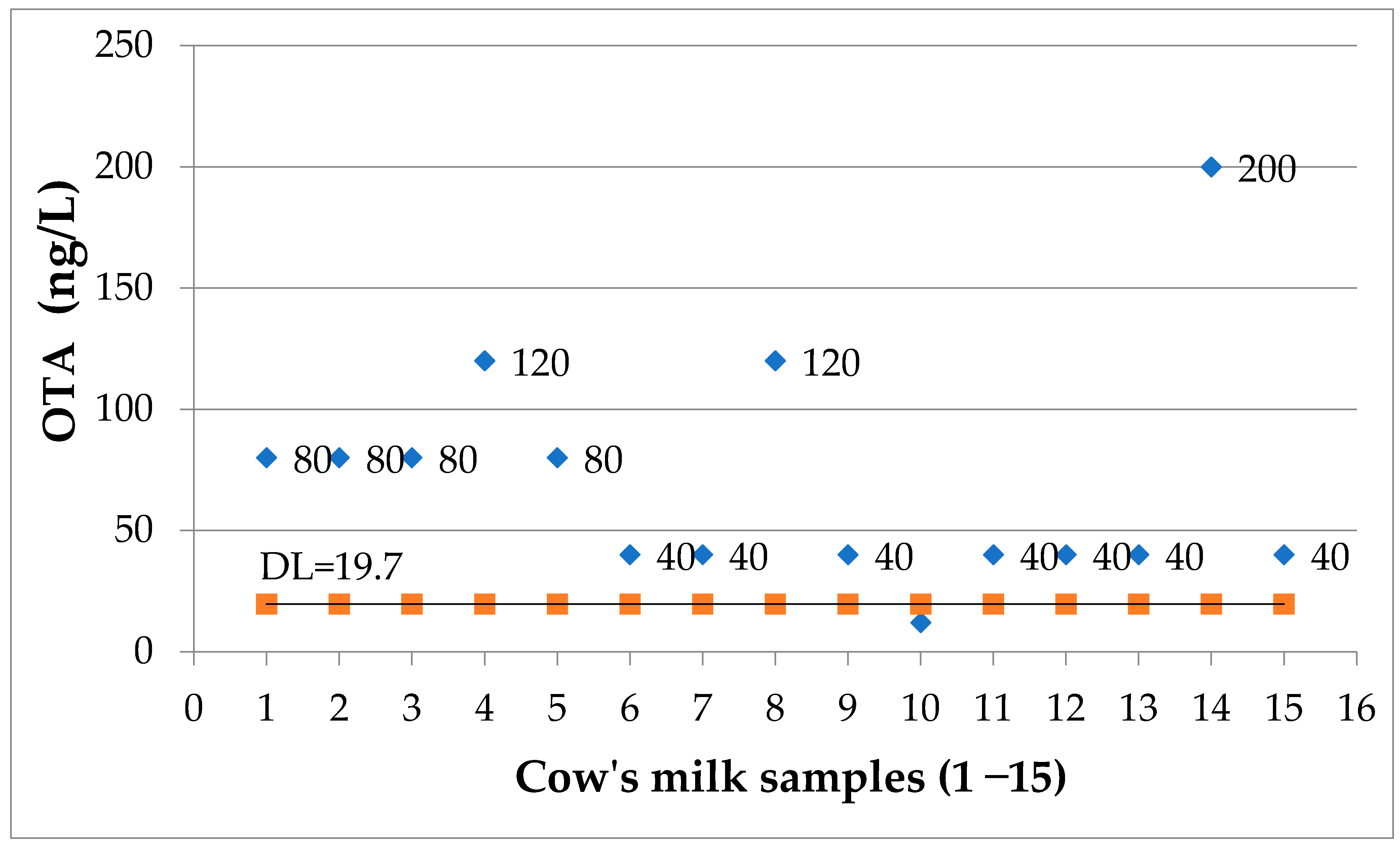
2.3. Determination of OTA in Cow’s Milk Samples
3. Discussions
4. Conclusions
5. Materials and Methods
5.1. Equipment
5.2. Reagents
- Calibrators with OTA concentrations between 0.0–0.40 ng/mL: each kit contains multi-analyte calibrators with values attributed through a referential method that certifies that the values of the said analytes were established in accordance with WHO-certified reference materials for 6 consecutive levels of concentration, in a liquid conditioning medium, which can be used as such (6 bottles, 1.5 mL each, with OTA concentrations of 0.0, 0.02, 0.05, 0.1, 0.2, 0.4 ng/mL diluted in 70% methanol).
- Reagent kit for the quantitative detection of OTA, contained all the necessary items that enable the ELISA reaction for the detection of OTA: reactive diluent, enzyme conjugate containing OTA conjugated with horseradish peroxidase (HRP), an underlayer reagent containing stabilized tetramethylbenzidine (TMB), acid stop solution and washing solution as a lyophilized powder from phosphate-buffered saline (PBS) with Tween®20 (10 mM phosphate, 137 mM NaCl, 2.7 mM KCl, 0.05% Tween®20, pH 7.4); one sachet to be diluted in 1000 mL distilled water. Absolute methanol was purchased from Chemical Company, Romania.
5.3. Statistical Analysis
5.4. Sample Preparation
5.5. Method
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Porter, D. (Ed.) Ochratoxins: Biosynthesis, Detection and Toxicity, 1st ed.; Nova Publishers Inc.: New York, NY, USA, 2016; pp. 33–35. [Google Scholar]
- Malir, F.; Ostry, V.; Pfohl-Leszkowicz, A.; Malir, J.; Toman, J. Ochratoxin A: 50 Years of Research. Toxins 2016, 8, 191. [Google Scholar] [CrossRef] [Green Version]
- Kamali, A.; Mehni, S.; Kamali, M.; Taheri Sarvtin, M. Detection of Ochratoxin A in Human Breast Milk in Jiroft City, South of Iran. Curr. Med. Mycol. 2017, 3, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Paolo, N.; Guarnieri, A.; Loi, F.; Sacchi, G.; Mangiarotti, A.M.; Di Paolo, M. Acute Renal Failure from Inhalation of Mycotoxins. Nephron 1993, 64, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Pitt, J.I. Toxigenic Fungi: Which Are Important? Med. Mycol. 2000, 38, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.V.; Wenndt, A.J.; Girard, A.W.; Taneja, S.; Ranjan, S.; Ramakrishnan, U.; Martorell, R.; Ryan, P.B.; Rangiah, K.; Young, M.F. Risk of Dietary and Breastmilk Exposure to Mycotoxins among Lactating Women and Infants 2–4 Months in Northern India. Matern. Child Nutr. 2021, 17, e13100. [Google Scholar] [CrossRef]
- Pyo, M.C.; Shin, H.S.; Jeon, G.Y.; Lee, K.-W. Synergistic Interaction of Ochratoxin A and Acrylamide Toxins in Human Kidney and Liver Cells. Biol. Pharm. Bull. 2020, 43, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer; Ochratoxin, A. IARC Monographs on The Evaluation of Carcinogenic Risk to Humans: Some Naturally Occurring Substances, Food Items and Constituents, Heterocyclic Aromatic Amines and Mycotoxins; International Agency for Research on Cancer: Geneva, Switzerland, 1993; Volume 56, pp. 26–32.
- Niaz, K.; Shah, S.Z.A.; Khan, F.; Bule, M. Ochratoxin A-Induced Genotoxic and Epigenetic Mechanisms Lead to Alzheimer Disease: Its Modulation with Strategies. Environ. Sci. Pollut. Res. Int. 2020, 27, 44673–44700. [Google Scholar] [CrossRef]
- Heussner, A.H.; Bingle, L.E.H. Comparative Ochratoxin Toxicity: A Review of the Available Data. Toxins 2015, 7, 4253–4282. [Google Scholar] [CrossRef] [Green Version]
- EFSA (Panel on Contaminants in the Food Chain); Schrenk, D.; Bodin, L.; Chipman, J.K.; del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Hoogenboom, L.; Leblanc, J.-C.; Nebbia, C.S.; et al. Risk Assessment of Ochratoxin A in Food. EFSA J. 2020, 18, e06223. [Google Scholar] [CrossRef]
- Huang, S.; Zheng, N.; Fan, C.; Cheng, M.; Wang, S.; Jabar, A.; Wang, J.; Cheng, J. Effects of Aflatoxin B1 Combined with Ochratoxin A and/or Zearalenone on Metabolism, Immune Function, and Antioxidant Status in Lactating Dairy Goats. Asian-Australas. J. Anim. Sci. 2018, 31, 505–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondy, G.S.; Curran, I.H.C.; Coady, L.C.; Armstrong, C.; Bourque, C.; Bugiel, S.; Caldwell, D.; Kwong, K.; Lefebvre, D.E.; Maurice, C.; et al. A One-Generation Reproductive Toxicity Study of the Mycotoxin Ochratoxin A in Fischer Rats. Food Chem. Toxicol. 2021, 153, 112247. [Google Scholar] [CrossRef]
- Frizzell, C.; Verhaegen, S.; Ropstad, E.; Elliott, C.T.; Connolly, L. Endocrine Disrupting Effects of Ochratoxin A at the Level of Nuclear Receptor Activation and Steroidogenesis. Toxicol. Lett. 2013, 217, 243–250. [Google Scholar] [CrossRef]
- Kumar, S.N.; Telang, A.G.; Singh, K.P.; Jain, A.K.; Afroz, M.; Patil, R.D. Experimentally Induced Toxicity of Ochratoxin A and Endosulfan in Male Wistar Rats: A Hormonal Disorder. J. Anim. Vet. Adv. 2011, 10, 1750–1755. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Wang, Y.; Jia, X.; Liu, W.; Zhang, X.; Cui, J. The Effect of Ochratoxin A on Cytotoxicity and Glucose Metabolism in Human Esophageal Epithelium Het-1A Cells. Toxicon 2021, 198, 80–92. [Google Scholar] [CrossRef]
- Song, Y.; Liu, W.; Zhao, Y.; Zang, J.; Gao, H. Ochratoxin A Induces Human Kidney Tubular Epithelial Cell Apoptosis through Regulating Lipid raft/PTEN/AKT Signaling Pathway. Environ. Toxicol. 2021, 36, 1880–1885. [Google Scholar] [CrossRef] [PubMed]
- Izco, M.; Vettorazzi, A.; Forcen, R.; Blesa, J.; de Toro, M.; Alvarez-Herrera, N.; Cooper, J.M.; Gonzalez-Peñas, E.; Lopez de Cerain, A.; Alvarez-Erviti, L. Oral Subchronic Exposure to the Mycotoxin Ochratoxin a Induces Key Pathological Features of Parkinson’s Disease in Mice Six Months after the End of the Treatment. Food Chem. Toxicol. 2021, 152, 112164. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lim, W.; You, S.; Song, G. Ochratoxin A Exerts Neurotoxicity in Human Astrocytes through Mitochondria-Dependent Apoptosis and Intracellular Calcium Overload. Toxicol. Lett. 2019, 313, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Izco, M.; Vettorazzi, A.; de Toro, M.; Sáenz, Y.; Alvarez-Erviti, L. Oral Sub-Chronic Ochratoxin a Exposure Induces Gut Microbiota Alterations in Mice. Toxins 2021, 13, 106. [Google Scholar] [CrossRef]
- Lippolis, V.; Asif, S.; Pascale, M.; Cervellieri, S.; Mancini, E.; Peli, A.; De Amicis, I.; Robbe, D.; Minervini, F. Natural Occurrence of Ochratoxin A in Blood and Milk Samples from Jennies and Their Foals after Delivery. Toxins 2020, 12, 758. [Google Scholar] [CrossRef] [PubMed]
- Taheur, F.B.; Fedhila, K.; Chaieb, K.; Kouidhi, B.; Bakhrouf, A.; Abrunhosa, L. Adsorption of Aflatoxin B1, Zearalenone and Ochratoxin A by Microorganisms Isolated from Kefir Grains. Int. J. Food Microbiol. 2017, 251, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Damiano, S.; Longobardi, C.; Andretta, E.; Prisco, F.; Piegari, G.; Squillacioti, C.; Montagnaro, S.; Pagnini, F.; Badino, P.; Florio, S.; et al. Antioxidative Effects of Curcumin on the Hepatotoxicity Induced by Ochratoxin A in Rats. Antioxidants 2021, 10, 125. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.G.; Terkelli, L.R.; Venancio, E.J.; Justino, L.; dos Santos, B.Q.; Baptista, A.A.S.; Oba, A.; de Oliveira Souza, B.D.; Bracarense, A.P.F.R.; Hirooka, E.Y.; et al. Tryptophan Attenuates the Effects of OTA on Intestinal Morphology and Local IgA/IgY Production in Broiler Chicks. Toxins 2020, 13, 5. [Google Scholar] [CrossRef]
- Jahreis, S.; Kuhn, S.; Madaj, A.-M.; Bauer, M.; Polte, T. Mold Metabolites Drive Rheumatoid Arthritis in Mice via Promotion of IFN-Gamma- and IL-17-Producing T Cells. Food Chem. Toxicol. 2017, 109, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Mor, F.; Sengul, O.; Topsakal, S.; Kilic, M.; Ozmen, O. Diabetogenic Effects of Ochratoxin A in Female Rats. Toxins 2017, 9, 144. [Google Scholar] [CrossRef] [Green Version]
- Petkova-Bocharova, T.; Chernozemsky, I.N.; Castegnaro, M. Ochratoxin A in Human Blood in Relation to Balkan Endemic Nephropathy and Urinary System Tumours in Bulgaria. Food Addit. Contam. 1988, 5, 299–301. [Google Scholar] [CrossRef]
- Abarca, M.L.; Accensi, F.; Bragulat, M.R.; Cabañes, F.J. Current Importance of Ochratoxin A–Producing Aspergillus Spp. J. Food Prot. 2001, 64, 903–906. [Google Scholar] [CrossRef] [PubMed]
- Pfohl-Leszkowicz, A.; Castegnaro, M. L’ochratoxine A. In Les Mycotoxines Dans L’alimentation, Evaluation et Gestion du Risqué, 1st ed.; Tec & Doc. Lavoisier: Paris, France, 1999; pp. 249–277. [Google Scholar]
- Pfohl-Leszkowicz, A.; Petkova-Bocharova, T.; Chernozemsky, I.N.; Castegnaro, M. Balkan Endemic Nephropathy and Associated Urinary Tract Tumours: A Review on Aetiological Causes and the Potential Role of Mycotoxins. Food Addit. Contam. 2002, 19, 282–302. [Google Scholar] [CrossRef]
- Gluhovschi, G.; Margineanu, F.; Velciov, S.; Gluhovschi, C.; Bob, F.; Petrica, L.; Bozdog, G.; Trandafirescu, V.; Modalca, M. Fifty Years of Balkan Endemic Nephropathy in Romania: Some Aspects of the Endemic Focus in the Mehedinti County. Clin. Nephrol. 2011, 75, 34–48. [Google Scholar] [PubMed]
- Gluhovschi, G.; Margineanu, F.; Trandafirescu, V.; Schiller, A.; Petrica, L.; Velciov, S.; Bozdog, G.; Gluhovschi, C.; Bob, F. Balkan Endemic Nephropathy in Romania. Facta Univ. Ser. Med. Biol. 2002, 9, 15–25. [Google Scholar]
- Wafa, E.W.; Yahya, R.S.; Sobh, M.A.; Eraky, I.; el-Baz, M.; el-Gayar, H.A.; Betbeder, A.M.; Creppy, E.E. Human Ochratoxicosis and Nephropathy in Egypt: A Preliminary Study. Hum. Exp. Toxicol. 1998, 17, 124–129. [Google Scholar] [CrossRef]
- Bui-Klimke, T.R.; Wu, F. Ochratoxin A and Human Health Risk: A Review of the Evidence. Crit. Rev. Food Sci. Nutr. 2015, 55, 1860–1869. [Google Scholar] [CrossRef] [Green Version]
- Gromadzka, K.; Pankiewicz, J.; Beszterda, M.; Paczkowska, M.; Nowakowska, B.; Kocyłowski, R. The Presence of Mycotoxins in Human Amniotic Fluid. Toxins 2021, 13, 409. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, K.; Blaszkewicz, M.; Campos, V.; Vega, M.; Degen, G.H. Exposure of Infants to Ochratoxin A with Breast Milk. Arch. Toxicol. 2014, 88, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Biasucci, G.; Calabrese, G.; Di Giuseppe, R.; Carrara, G.; Colombo, F.; Mandelli, B.; Maj, M.; Bertuzzi, T.; Pietri, A.; Rossi, F. The Presence of Ochratoxin A in Cord Serum and in Human Milk and Its Correspondence with Maternal Dietary Habits. Eur. J. Nutr. 2011, 50, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Micco, C.; Ambruzzi, M.A.; Miraglia, M.; Brera, C.; Onori, R.; Benelli, L. Contamination of Human Milk with Ochratoxin A. IARC Sci. Publ. 1991, 115, 105–108. [Google Scholar]
- Turconi, G.; Guarcello, M.; Livieri, C.; Comizzoli, S.; Maccarini, L.; Castellazzi, A.M.; Pietri, A.; Piva, G.; Roggi, C. Evaluation of Xenobiotics in Human Milk and Ingestion by the Newborn--An Epidemiological Survey in Lombardy (Northern Italy). Eur. J. Nutr. 2004, 43, 191–197. [Google Scholar] [CrossRef]
- Valitutti, F.; De Santis, B.; Trovato, C.M.; Montuori, M.; Gatti, S.; Oliva, S.; Brera, C.; Catassi, C. Assessment of Mycotoxin Exposure in Breastfeeding Mothers with Celiac Disease. Nutrients 2018, 10, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breitholtz-Emanuelsson, A.; Olsen, M.; Oskarsson, A.; Palminger, I.; Hult, K. Ochratoxin A in Cow’s Milk and in Human Milk with Corresponding Human Blood Samples. J. AOAC Int. 1993, 76, 842–846. [Google Scholar] [CrossRef] [PubMed]
- Zimmerli, B.; Dick, R. Determination of Ochratoxin A at the Ppt Level in Human Blood, Serum, Milk and Some Foodstuffs by High-Performance Liquid Chromatography with Enhanced Fluorescence Detection and Immunoaffinity Column Cleanup: Methodology and Swiss Data. J. Chromatogr. B Biomed. Sci. Appl. 1995, 666, 85–99. [Google Scholar] [CrossRef]
- Postupolski, J.; Karłowski, K.; Kubik, P. Ochratoxin a in Maternal and Foetal Blood and in Maternal Milk. Rocz. Panstw. Zakl. Hig. 2006, 57, 23–30. [Google Scholar]
- Ferrufino-Guardia, E.; Chavez-Rico, V.; Larondelle, Y. Ochratoxin a in Human Breast Milk, Maternal and Placental Blood from Cochabamba-Bolivia. Rev. Toxicol. 2019, 36, 116–125. [Google Scholar]
- Muñoz, K.; Wollin, K.-M.; Kalhoff, H.; Degen, G.H. Occurrence of the mycotoxin ochratoxin a in breast milk samples from Germany. Gesundheitswesen 2013, 75, 194–197. [Google Scholar] [CrossRef]
- Dostal, A.; Jakusova, L.; Cajdova, J.; Hudeckova, H. Results of the First Studies of Occurence of Ochratoxin A in Human Milk in Slovakia. Bratisl. Lek. Listy 2008, 109, 276–278. [Google Scholar] [PubMed]
- Skaug, M.A.; Helland, I.; Solvoll, K.; Saugstad, O.D. Presence of Ochratoxin A in Human Milk in Relation to Dietary Intake. Food Addit. Contam. 2001, 18, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Kovács, F.; Sándor, G.; Ványi, A.; Domány, S.; Zomborszky-Kovács, M. Detection of Ochratoxin a in Human Blood and Colostrum. Acta Vet. Hung. 1995, 43, 393–400. [Google Scholar]
- Jonsyn, F.E.; Maxwell, S.M.; Hendrickse, R.G. Ochratoxin A and Aflatoxins in Breast Milk Samples from Sierra Leone. Mycopathologia 1995, 131, 121–126. [Google Scholar] [CrossRef]
- Gürbay, A.; Girgin, G.; Sabuncuoğlu, S.A.; Sahin, G.; Yurdakök, M.; Yigit, S.; Tekinalp, G. Ochratoxin A: Is It Present in Breast Milk Samples Obtained from Mothers from Ankara, Turkey? J. Appl. Toxicol. 2010, 30, 329–333. [Google Scholar] [CrossRef]
- Cherkani-Hassani, A.; Ghanname, I.; Zinedine, A.; Sefrioui, H.; Qmichou, Z.; Mouane, N. Ochratoxin a in Breast Milk in Morocco: The Affecting Dietary Habits of the Lactating Mothers and the Degree of Exposure of Newborns “Contamilk Study”. Drug Chem. Toxicol. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Coppa, C.F.S.C.; Cirelli, A.C.; Gonçalves, B.L.; Barnabé, E.M.B.; Petta, T.; Franco, L.T.; Javanmardi, F.; Khaneghah, A.M.; Lee, S.H.I.; Corassin, C.H.; et al. Mycotoxin Occurrence in Breast Milk and Exposure Estimation of Lactating Mothers Using Urinary Biomarkers in São Paulo, Brazil. Environ. Pollut. 2021, 279, 116938. [Google Scholar] [CrossRef] [PubMed]
- Yalçin, S.S.; Güneş, B.; Yalçin, S. Influence of Season and Lactational Stage on Aflatoxin M1 and Ochratoxin A in Human Milk in a Cohort Study from Southeastern Region of Turkey. Int. J. Environ. Health Res. 2020, 1–12. [Google Scholar] [CrossRef]
- Piacentini, K.C.; Ferranti, L.S.; Pinheiro, M.; Bertozzi, B.G.; Rocha, L.O. Mycotoxin Contamination in Cereal-Based Baby Foods. Curr. Opin. Food Sci. 2019, 30, 73–78. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, B.; Dai, Y.; Li, H.; Xu, W. A Review: Epigenetic Mechanism in Ochratoxin a Toxicity Studies. Toxins 2017, 9, 113. [Google Scholar] [CrossRef] [Green Version]
- Kuiper-Goodman, T.; Scott, P.M. Risk Assessment of the Mycotoxin Ochratoxin A. Biomed. Environ. Sci. 1989, 2, 179–248. [Google Scholar] [PubMed]
- Kuiper-Goodman, T.; Hilts, C.; Billiard, S.M.; Kiparissis, Y.; Richard, I.D.K.; Hayward, S. Health Risk Assessment of Ochratoxin A for All Age-Sex Strata in a Market Economy. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2010, 27, 212–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pattono, D.; Gallo, P.F.; Civera, T. Detection and Quantification of Ochratoxin A in Milk Produced in Organic Farms. Food Chem. 2011, 127, 374–377. [Google Scholar] [CrossRef]
- Miraglia, M.; Brera, C. Assessment of Dietary Intake of Ochratoxin A by the Population of EU Member States Reports on Tasks for Scientific Cooperation. Rep. Export. Particip. SCOOP Task 2002, 3, 7. [Google Scholar]
- Weidenbörner, M. Animal Products as Well as Human Breast Milk and Their Mycotoxins. In Mycotoxins Animal Products; Springer: Cham, Switzerland, 2019; pp. 127–134. [Google Scholar]
- Akinyemi, M.O.; Braun, D.; Windisch, P.; Warth, B.; Ezekiel, C.N. Assessment of Multiple Mycotoxins in Raw Milk of Three Different Animal Species in Nigeria. Food Control 2021, 131, 108258. [Google Scholar] [CrossRef]
- Hof, H. Mycotoxins in Milk for Human Nutrition: Cow, Sheep and Human Breast Milk. GMS Infect. Dis. 2016, 4, Doc03. [Google Scholar] [CrossRef]
- Altafini, A.; Roncada, P.; Guerrini, A.; Sonfack, G.M.; Fedrizzi, G.; Caprai, E. Occurrence of Ochratoxin A in Different Types of Cheese Offered for Sale in Italy. Toxins 2021, 13, 540. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tested Sample | %A0 Standard 0.02 ng/mL | %A0 Sample | %A0 Standard < 2 SD | Coefficient of Variation % | ng/mL |
|---|---|---|---|---|---|
| Colostrum | 86.5 | 92.3 | 89.3 | 1.6 | <0.08 |
| Cow’s milk | 85.9 | 91.1 | 88.9 | 1.2 | <0.08 |
| Nr. | Standard | Concentration (ng/mL) | Absorbance | r | Intercept | Slope |
|---|---|---|---|---|---|---|
| 1 | STD 1 | 0.4 | 1.4800 | −0.9838 | 2.824 | −3.3430 |
| 2 | STD 2 | 0.2 | 2.0060 | |||
| 3 | STD 3 | 0.1 | 2.6070 | |||
| 4 | STD 4 | 0.05 | 2.7220 | |||
| 5 | STD 5 | 0.02 | 2.7410 | |||
| 6 | STD 6 | 0 | 2.7520 |
| Regression Statistics | |
|---|---|
| Multiple R | 0.9838 |
| R Square | 0.9681 |
| Adjusted R Square | 0.9601 |
| Standard Error | 0.1052 |
| Observations | 6 |
| ANOVA Statistical Analysis | |||||
|---|---|---|---|---|---|
| df | SS | MS | F | Significance F | |
| Regression | 1 | 1.3426 | 1.3426 | 121.2284 | 0.0004 |
| Residual | 4 | 0.0443 | 0.0111 | ||
| Total | 5 | 1.3869 | |||
| Coefficients | Standard Error | t Stat | p-Value | Lower | Upper | |
|---|---|---|---|---|---|---|
| 95% | 95% | |||||
| Intercept | 2.8249 | 0.0587 | 48.1313 | 1.11 × 10−6 | 2.6620 | 2.9879 |
| Concentration (ng/mL) | −3.4306 | 0.3116 | −11.0104 | 0.0004 | −4.2957 | −2.5655 |
| Sample Type | Mean Concentration (ng/mL, n = 20) | Standard Deviation (SD) | Limit of Detection (ng/mL) | Limit of Quantification (ng/mL) |
|---|---|---|---|---|
| Milk | 0.0079 | 0.0039 | 0.0197 | 0.0474 |
| Tested Sample | Recovery Series I (%) | Recovery Series II (%) | Recovery Series III (%) | Recovery Mean (%) |
|---|---|---|---|---|
| Human milk | 96 | 110 | 95 | 100 |
| Cow’s milk | 114 | 116 | 113 | 114 |
| Procedure: | Blank | STD 1 | STD 2 | STD 3 | STD 4 | STD 5 | STD 6 | Sample |
|---|---|---|---|---|---|---|---|---|
| (0.4 ng/mL) | (0.2 ng/mL) | (0.1 ng/mL) | (0.05 ng/mL) | (0.02 ng/mL) | (0 ng/mL) | |||
| a. Addition | x | 200 μL of reactive diluent was added to each well | ||||||
| b. Addition | x | 100 μL | 100 μL | 100 μL | 100 μL | 100 μL | 100 μL | 100 μL |
| c. Homogenization | x | 2–3 successive pipetting for homogenization were performed. | ||||||
| d. Transfer | x | 100 μL of contents from each mixing well of microtiter plate was transferred. | ||||||
| to corresponding Anti OTA antibody coated well from reaction microplate. | ||||||||
| e. Incubation | x | 30 min at ambient temperature (22 °C). | ||||||
| f. Wash | x | The content of the wells was removed and then wells were washed 3 times | ||||||
| with washing buffer PBS-Tween (pause between washes was 60 s). | ||||||||
| After the last wash the excess moisture was absorbed by blotting on filter paper. | ||||||||
| g. Addition | x | 100 μL OTA-horseradish peroxidase (HRP) conjugate was added to each well. | ||||||
| h. Incubation | x | 30 min at ambient temperature (22 °C). | ||||||
| i. Wash | x | Three successive washes were carried out with washing buffer PBS-Tween. | ||||||
| After the last wash the excess moisture was absorbed by blotting on filter paper. | ||||||||
| j. Addition | x | 100 μL substrate solution TMB was added to each well. Being a chromogenic | ||||||
| substrate for HRP, TMP produced a deep blue color during the enzymatic | ||||||||
| degradation of hydrogen peroxide by HRP. | ||||||||
| k. Incubation | x | 10 min at ambient temperature (22 °C). | ||||||
| l. Homogenization | x | 2–3 successive pipetting for homogenization were performed. | ||||||
| m. Reading | x | Using a spectrophotometer, optical density was read at λ = 450 nm with 630 | ||||||
| nm reference filter. The intensity of the color was directly proportional with the | ||||||||
| quantity of linked conjugate and indirectly proportional to the quantity of OTA | ||||||||
| present in the standard or in the sample. | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuciureanu, M.; Tuchiluș, C.; Vartolomei, A.; Tamba, B.I.; Filip, L. An Immunoenzymatic Method for the Determination of Ochratoxin A in Biological Liquids (Colostrum and Cow’s Milk). Toxins 2021, 13, 673. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13100673
Cuciureanu M, Tuchiluș C, Vartolomei A, Tamba BI, Filip L. An Immunoenzymatic Method for the Determination of Ochratoxin A in Biological Liquids (Colostrum and Cow’s Milk). Toxins. 2021; 13(10):673. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13100673
Chicago/Turabian StyleCuciureanu, Magdalena, Cristina Tuchiluș, Anca Vartolomei, Bogdan Ionel Tamba, and Lorena Filip. 2021. "An Immunoenzymatic Method for the Determination of Ochratoxin A in Biological Liquids (Colostrum and Cow’s Milk)" Toxins 13, no. 10: 673. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13100673