Post-Contrast Acute Kidney Injury in Patients with Various Stages of Chronic Kidney Disease—Is Fear Justified?


Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Study Limitations
3.2. Key Findings and Future Directions
4. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zamora, C.A.; Castillo, M. Historical Perspective of Imaging Contrast Agents. Magn. Reason. Imaging Clin. N. Am. 2017, 25, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Bartels, E.D.; Brun, G.C.; Gammeltoft, A.; Gjorup, P.A. Acute anuria following intravenous pyelography in a patient with myelomatosis. Acta Med. Scand. 1954, 150, 297–302. [Google Scholar] [CrossRef]
- van der Molen, A.J.; Reimer, P.; Dekkers, I.A.; Bongartz, G.; Bellin, M.F.; Bertolotto, M.; Clement, O.; Heinz-Peer, G.; Stacul, F.; Webb, J.A.W.; et al. Post-contrast acute kidney injury—Part 1: Definition, clinical features, incidence, role of contrast medium and risk factors: Recommendations for updated ESUR Contrast Medium Safety Committee guidelines. Eur. Radiol. 2018, 28, 2845–2855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davenport, M.S.; Perazella, M.A.; Yee, J.; Dillman, J.R.; Fine, D.; McDonald, R.J.; Rodby, R.A.; Wang, C.L.; Weinreb, J.C. Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation. Radiology 2020, 294, 660–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luk, L.; Steinman, J.; Newhouse, J.H. Intravenous Contrast-Induced Nephropathy-The Rise and Fall of a Threatening Idea. Adv. Chronic Kidney Dis. 2017, 24, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, H.S.; Morcos, S.K. Contrast media and metformin: Guidelines to diminish the risk of lactic acidosis in non-insulin-dependent diabetics after administration of contrast media. ESUR Contrast Media Safety Committee. Eur. Radiol. 1999, 9, 738–740. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, A.J.; Reimer, P.; Dekkers, I.A.; Bongartz, G.; Bellin, M.F.; Bertolotto, M.; Clement, O.; Heinz-Peer, G.; Stacul, F.; Webb, J.A.W.; et al. Post-contrast acute kidney injury. Part 2: Risk stratification, role of hydration and other prophylactic measures, patients taking metformin and chronic dialysis patients: Recommendations for updated ESUR Contrast Medium Safety Committee guidelines. Eur. Radiol. 2018, 28, 2856–2869. [Google Scholar] [CrossRef] [Green Version]
- Elicker, B.M.; Cypel, Y.S.; Weinreb, J.C. IV contrast administration for CT: A survey of practices for the screening and prevention of contrast nephropathy. Am. J. Roentgenol. 2006, 186, 1651–1658. [Google Scholar] [CrossRef] [Green Version]
- Do, C. Intravenous Contrast: Friend or Foe? A Review on Contrast-Induced Nephropathy. Adv. Chronic Kidney Dis. 2017, 24, 147–149. [Google Scholar] [CrossRef]
- Chomicka, I.; Kwiatkowska, M.; Małyszko, J. Post-contrast acute kidney injury following computed tomography: A real or overestimated threat? Pol. Arch. Intern. Med. 2020, 130, 704–707. [Google Scholar]
- Stevens, P.E.; Levin, A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013, 4, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kooiman, J.; Pasha, S.M.; Zondag, W.; Sijpkens, Y.W.; van der Molen, A.J.; Huisman, M.V.; Dekkers, O.M. Meta-analysis: Serum creatinine changes following contrast enhanced CT imaging. Eur. J. Radiol. 2012, 81, 2554–2561. [Google Scholar] [CrossRef]
- Moos, S.I.; van Vemde, D.N.; Stoker, J.; Bipat, S. Contrast induced nephropathy in patients undergoing intravenous (IV) contrast enhanced computed tomography (CECT) and the relationship with risk factors: A meta-analysis. Eur. J. Radiol. 2013, 82, e387–e399. [Google Scholar] [CrossRef] [PubMed]
- From, A.M.; Bartholmai, B.J.; Williams, A.W.; Cha, S.S.; Pflueger, A.; McDonald, F.S. Sodium bicarbonate is associated with an increased incidence of contrast nephropathy: A retrospective cohort study of 7977 patients at mayo clinic. Clin. J. Am. Soc. Nephrol. 2008, 3, 10–18. [Google Scholar] [CrossRef]
- Timal, R.J.; Kooiman, J.; Sijpkens, Y.W.J.; de Vries, J.P.P.M.; Verberk-Jonkers, I.J.A.M.; Brulez, H.F.H.; van Buren, M.; van Der Molen, A.J.; Cannegieter, S.C.; Putter, H.; et al. Effect of No Prehydration vs. Sodium Bicarbonate Prehydration Prior to Contrast-Enhanced Computed Tomography in the Prevention of Postcontrast Acute Kidney Injury in Adults With Chronic Kidney Disease: The Kompas Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Sebastià, C.; Páez-Carpio, A.; Guillen, E.; Paño, B.; Garcia-Cinca, D.; Poch, E.; Oleaga, L.; Nicolau, C. Oral hydration compared to intravenous hydration in the prevention of post-contrast acute kidney injury in patients with chronic kidney disease stage IIIb: A phase III non-inferiority study (NICIR study). Eur. J. Radiol. 2021, 136, 109509. [Google Scholar] [CrossRef]
- Chaudhury, P.; Armanyous, S.; Harb, S.C.; Provenzano, L.F.; Ashour, T.; Jolly, S.E.; Arrigain, S.; Konig, V.; Schold, J.D.; Navaneethan, S.D.; et al. Intra-Arterial versus Intravenous Contrast and Renal Injury in Chronic Kidney Disease: A Propensity-Matched Analysis. Nephron 2019, 141, 31–40. [Google Scholar] [CrossRef]
- Hinson, J.S.; Ehmann, M.R.; Fine, D.M.; Fishman, E.K.; Toerper, M.F.; Rothman, R.E.; Klein, E.Y. Risk of Acute Kidney Injury After Intravenous Contrast Media Administration. Ann. Emerg. Med. 2017, 69, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Hinson, J.S.; Al Jalbout, N.; Ehmann, M.R.; Klein, E.Y. Acute kidney injury following contrast media administration in the septic patient: A retrospective propensity-matched analysis. J. Crit. Care 2019, 51, 111–116. [Google Scholar] [CrossRef]
- Gorelik, Y.; Yaseen, H.; Heyman, S.N.; Khamaisi, M. Negligible Risk of Acute Renal Failure among Hospitalized Patients After Contrast-Enhanced Imaging With Iodinated Versus Gadolinium-Based Agents. Investig. Radiol. 2019, 54, 312–318. [Google Scholar] [CrossRef]
- Gorelik, Y.; Bloch-Isenberg, N.; Yaseen, H.; Heyman, S.N.; Khamaisi, M. Acute Kidney Injury after Radiocontrast-Enhanced Computerized Tomography in Hospitalized Patients with Advanced Renal Failure: A Propensity-Score-Matching Analysis. Investig. Radiol. 2020, 55, 677–687. [Google Scholar] [CrossRef]
- Carlqvist, J.; Nyman, U.; Sterner, G.; Brandberg, J.; Fagman, E.; Hellström, M. Minimal risk of contrast-induced kidney injury in a randomly selected cohort with mildly reduced GFR. Eur. Radiol. 2020, 31, 3248–3257. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, Y.; Miyazawa, H.; Nakamura, J.; Taketomi-Takahashi, A.; Suto, T.; Tsushima, Y. Contrast-induced nephropathy (CIN) of patients with renal dysfunction in CT examination. Jpn. J. Radiol. 2017, 35, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J.H.; Khalatbari, S.; Yosef, M.; Cohan, R.H.; Davenport, M.S. Influence of Clinical Factors on Risk of Contrast-Induced Nephrotoxicity From IV Iodinated Low-Osmolality Contrast Material in Patients With a Low Estimated Glomerular Filtration Rate. AJR Am. J. Roentgenol. 2019, 213, W188–W193. [Google Scholar] [CrossRef]
- McDonald, J.S.; McDonald, R.J.; Williamson, E.E.; Kallmes, D.F. Is Intravenous Administration of Iodixanol Associated with Increased Risk of Acute Kidney Injury, Dialysis, or Mortality? A Propensity Score-adjusted Study. Radiology 2017, 285, 414–424. [Google Scholar] [CrossRef]
- Tao, S.M.; Wichmann, J.L.; Schoepf, U.J.; Fuller, S.R.; Lu, G.M.; Zhang, L.J. Contrast-induced nephropathy in CT: Incidence, risk factors and strategies for prevention. Eur. Radiol. 2016, 26, 3310–3318. [Google Scholar] [CrossRef] [PubMed]
- Aycock, R.D.; Westafer, L.M.; Boxen, J.L.; Majlesi, N.; Schoenfeld, E.; Bannuru, R.R. Acute Kidney Injury After Computed Tomography: A Meta-analysis. Ann. Emerg. Med. 2018, 71, 44–53.e4. [Google Scholar] [CrossRef]
- Räty, P.; Mentula, P.; Lampela, H.; Nykänen, T.; Helanterä, I.; Haapio, M.; Lehtimäki, T.; Skrifvars, M.B.; Vaara, S.T.; Leppäniemi, A.; et al. INtravenous Contrast computed tomography versus native computed tomography in patients with acute Abdomen and impaired Renal functiOn (INCARO): A multicentre, open-label, randomised controlled trial-study protocol. BMJ Open 2020, 10, e037928. [Google Scholar] [CrossRef]
- Hiremath, S.; Kong, J.; Clark, E.G. Contrast and acute kidney injury: What is left to enhance? Nephrol. Dial. Transplant. 2020, 10, gfaa183. [Google Scholar] [CrossRef]
- Nijssen, E.C.; Rennenberg, R.J.; Nelemans, P.J.; Essers, B.A.; Janssen, M.M.; Vermeeren, M.A.; Ommen, V.V.; Wildberger, J.E. Prophylactic hydration to protect renal function from intravascular iodinated contrast material in patients at high risk of contrast-induced nephropathy (AMACING): A prospective, randomised, phase 3, controlled, open-label, non-inferiority trial. Lancet 2017, 389, 1312–1322. [Google Scholar] [CrossRef]
- Cosmai, L.; Porta, C.; Privitera, C.; Gesualdo, L.; Procopio, G.; Gori, S.; Laghi, A. Acute kidney injury from contrast-enhanced CT procedures in patients with cancer: White paper to highlight its clinical relevance and discuss applicable preventive strategies. ESMO Open 2020, 5, e000618. [Google Scholar] [CrossRef] [Green Version]
- Mangus, R.S.; Bajpai, S.; Lutz, A.J.; Powelson, J.A.; Goggins, W.C. Contrast Administration to the Deceased Kidney Donor Has No Impact on Post-Transplant Outcomes. J. Surg. Res. 2020, 254, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Benjamens, S.; Yakar, D.; Slart, R.H.J.A.; Sanders, J.S.F.; Pol, R.A. The fear for contrast-induced nephropathy in kidney transplant recipients: Time for a paradigm shift? Transpl. Int. 2018, 31, 1050–1051. [Google Scholar] [CrossRef] [Green Version]
- Garfinkle, M.A.; Stewart, S.; Basi, R. Incidence of CT Contrast Agent-Induced Nephropathy: Toward a More Accurate Estimation. AJR Am. J. Roentgenol. 2015, 204, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Clec’H, C.; Razafimandimby, D.; Laouisset, M.; Chemouni, F.; Cohen, Y. Incidence and outcome of contrast-associated acute kidney injury in a mixed medical-surgical ICU population: A retrospective study. BMC Nephrol. 2013, 14, 31. [Google Scholar] [CrossRef] [Green Version]
- De Simone, B.; Ansaloni, L.; Sartelli, M.; Gaiani, F.; Leandro, G.; Luigi de’ Angelis, G.; Di Mario, F.; Coccolini, F.; Catena, F. Is the risk of contrast-induced nephropathy a real contraindication to perform intravenous contrast enhanced Computed Tomography for non-traumatic acute abdomen in Emergency Surgery Department? Acta Biomed. 2018, 89, 158–172. [Google Scholar] [PubMed]
- Song, W.; Zhang, T.; Pu, J.; Shen, L.; He, B. Incidence and risk of developing contrast-induced acute kidney injury following intravascular contrast administration in elderly patients. Clin. Interv. Aging 2014, 9, 85–93. [Google Scholar]
- Jeon, J.; Kim, S.; Yoo, H.; Kim, K.; Kim, Y.; Park, S.; Jang, H.R.; Kim, D.K.; Huh, W.; Kim, Y.G.; et al. Risk Prediction for Contrast-Induced Nephropathy in Cancer Patients Undergoing Computed Tomography under Preventive Measures. J. Oncol. 2019, 2019, 8736163. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before CT | 1–7 Days after | 14–28 Days after | >28 Days after | |
|---|---|---|---|---|
| CT without contrast creatinine, mg/dL | 1.16 (1.06; 10.61) | 1.54 (1.12; 7.18) **## | 1.44 (0.49; 12.98) *## | 1.04 (0.21; 7.81) |
| CT without contrast eGFR, mL/min/1.73 m2 | 50 (5; 120) # | 39 (7; 120) ## | 45(4; 102) ## | 72 (7; 120) |
| CT with contrast creatinine, mg/dL | 0.99 (0.48; 8.73) | 1.06 (0.33; 8.07) | 0.96 (0.36; 7.85) | 1.00 (0.49; 5.84) |
| CT with contrast eGFR, mL/min/1.73 m2 | 68 (7; 120) | 66 (7; 120) | 74 (7; 120) | 70 (8; 120) |
| Before CT | 1–7 Days after | 14–28 Days after | >28 Days after | |
|---|---|---|---|---|
| CT without contrast creatinine, mg/dL | 1.22 (0.74; 10.61) | 1.73 (0.70; 6.77) ** | 1.75 (1.00; 9.20) ** | 1.71 (0.93; 7.81) * |
| CT without contrast eGFR, mL/min/1.73m2 | 46 (9; 120) | 31 (7; 86) ** | 34 (4; 69) ** | 31 (7; 116) * |
| CT with contrast creatinine, mg/dL | 1.29 (0.67; 6.17) | 1.46 (0.67; 6.53) **# | 1.56 (0.64; 4.03) **# | 1.77 (0.64; 4.74) * |
| CT with contrast eGFR, mL/min/1.73m2 | 53 (8;20) # | 37 (7; 91) **# | 40 (7; 87) # | 34 (8; 116) |
| Comorbid Disease | Participation in the Population Subjected to Contrast-Enhanced CT | Participation in the Population Subjected to Non-Enhanced CT |
|---|---|---|
| Cancer | 72 (25.4%) | 10 (14.9%) |
| Hypertension | 181 (63.7%) | 50 (74.6%) |
| Diabetes mellitus | 77 (27.1%) | 12 (17.9%) |
| COPD 1/asthma | 39 (13.7%) | 11 (16.4%) |
| Chronic heart failure | 67 (23.6%) | 24 (35.8%) |
| Coronary heart disease | 58 (20.4%) | 13 (19.4%) |
| Cirrhosis | 18 (6.3%) | 3 (4.5%) |
| Thyroid disease | 6 (2.1%) | 1 (1.5%) |
| Sepsis/severe infection | 74 (26%) | 29 (43.3%) |
| Anemia | 169 (59.5%) | 47 (70.1%) |
| Pulmonary embolism | 21 (7.4%) | 3 (4.5%) |
| Indication | Number of Patients (n = 285) |
|---|---|
| Pulmonary embolism | 21 |
| Abscess | 7 |
| Neoplastic disease (diagnosis or stage assessment) | 29 |
| Vascular complications | 3 |
| Other | 7 |
| Indication | Number of Patients (n = 67) |
|---|---|
| Vasculitis | 6 |
| Fracture/bone metastases | 13 |
| Stroke/intracranial bleeding | 14 |
| Sinusitis | 6 |
| Pneumonia/pulmonary fibrosis | 16 |
| Other | 12 |
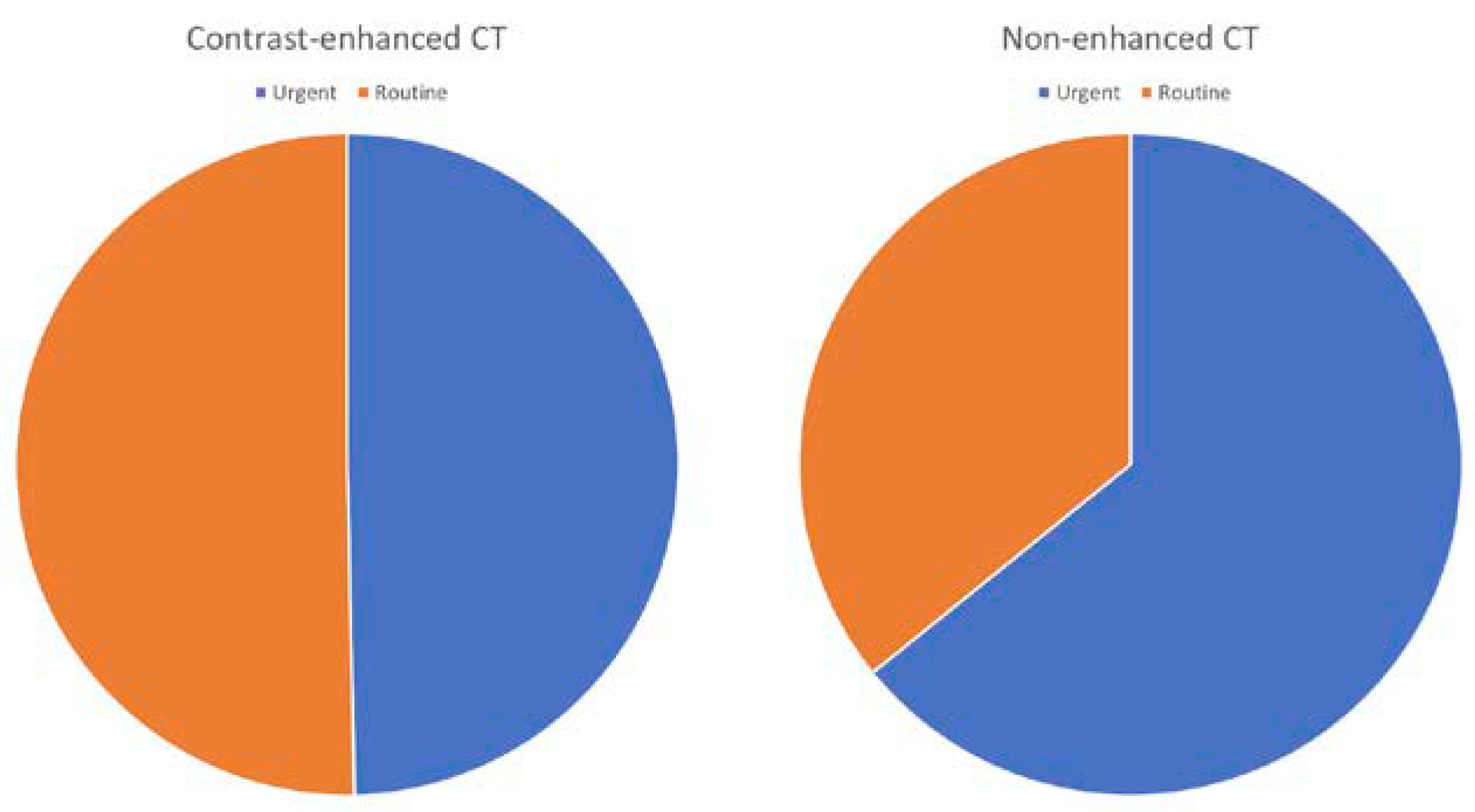
| Type of Examination | Urgent | Routine | |
|---|---|---|---|
| Contrast-enhanced CT | Number of AKI cases | 10 | 2 |
| Total number of CT | 37 | 30 | |
| AKI frequency | 27% | 6.7% | |
| Non-enhanced CT | Number of AKI cases | 12 | 5 |
| Total number of CT | 43 | 24 | |
| AKI frequency | 27.9% | 20.8% |
| Study Group | Study Design | Study Procedures | Central Message | Additional Findings | Study Limitation | Other | Reference |
|---|---|---|---|---|---|---|---|
| NICIR study | Prospective | Serum creatinine within 48–72 h after the procedure | PC-AKI rate was 4.4% (95%CI: 1.4–9.9%) in the oral hydration arm and 5.3% (95%CI: 2.0–11.1%) in the i.v. hydration arm |
|
| [13] | |
| KOMPAS trial | Prospective | CT with contrast in CKD stage 3 | PC-AKI occurred in 11 patients (2.1%), including 7 of 262 (2.7%) in the no prehydration group and 4 of 261 (1.5%) in the prehydration group |
|
No urinary catalytic iron levels | [15] | |
| Cleveland Clinic CKD registry | Registry | Serum creatinine within 48–72 h after the procedure | The incidence of AKI was 27% in the coronary angiography group, 24% in CT with contrast, and 24% in CT without contrast |
| [17] | ||
| 17,934 visits to emergency department with CT (16,801 patients) | Single-center retrospective cohort study | Serum was collected before contrast exposure (baseline) and at 48–72 h following contrast exposure | AKI rate was similar between CT with and without contrast | AKI rate was not dependent on baseline kidney function; no difference with CKD rate, dialysis, and transplantation at sixth month
|
| [18] | |
| 11,516 patients | Meta-analysis | Plasma samples were obtained on days 1 and 8, whereas hepcidin was measured on day 1 only | Higher plasma concentrations of catalytic iron and lower plasma concentrations of hepcidin were associated with a significantly greater risk of death |
|
|
| [19] |
| 4171 visits to ED, 1640 CT with contrast, 976 without contrast, and 1731 no CT at all | Single-center, propensity-matched, retrospective cohort study | Serum creatinine within 48–72 h after the procedure | The incidences of AKI were 7.2%, 9.4%, and 9.7% in those who underwent CECT, unenhanced CT, and no CT, respectively |
|
Heterogeneous group |
| [19] |
| Enhanced MRI = 958, non-enhanced = 491, enhanced CT = 9576, non-enhanced CT = 11,660 | Propensity score matching analysis | 22,321 imaging studies | Patients with impaired kidney function have a greater risk of PC-AKI | Anemia and diabetes are risk factors for PC-AKI |
| Creatinine takes up to 3 days before imaging | [21] |
| 1009 patients form SCAPIS study | Prospective | Creatinine measurement in 2–4 after the angiography | Iohexol is safe in patients with eGFR > 50 mL/min | PC-AKI rate very low (0.2%); no effect of diabetes and NSAIDs use on AKI rate |
| Very homogenous and well-defined group aged 50–65 years | [22] |
| 2583 CT scans in 2277 patients | Retrospective cohort analysis | The incidence of acute kidney injury (Acute Kidney Injury Network stages) and dialysis after acute kidney injury were assessed in the immediate period (24–48 h) and in a delayed period (72–96 h) after the scan. | AKI rate was not dependent on CKD stage | Dialysis after AKI was similar across eGFR subgroups. |
| [34] | |
| 2008 on adult patients who underwent a contrast-enhanced computed tomography for urgent diagnostic purposes. | Single-center retrospective analysis | Creatinine assessment within 48 h | PC-AKI was a frequent complication (16.8%) | Sepsis, nephrotoxic drugs, and hemodynamic failure—risk factors for AKI PC-AKI associated with ICU mortality; need for renal replacement therapy in 29.2% of PC-AKI |
| [35] | |
| 8 articles out of 2500 screened were analyzed | Systemic review (meta-analysis of observational studies) | Incidence of post-contrast acute kidney injury (AKI) following intravenous contrast agent administration | CT with contrast was not significantly associated with AKI. | Risk of contrast induced nephropathy (CIN) was negligible in patients with normal renal function, but the incidence appeared to rise to as high as 25% in patients with pre-existing renal impairment or in the presence of risk factors such as diabetes, advanced age, vascular disease, and use of certain concurrent medications | Systematic review addressed both CIN and PC-AKI because in literature the two terms CIN from PC-AKI were difficult to separate, even if these terms were not interchangeable | The incidence reported of AKI in patients undergoing cCT with contrast was not as high as thought before | [36] |
| 67,831 patients older than 65 years of age (out of 186, 455 patients) | Meta-analysis (22 studies) | Incidence of AKI in elderly (over 65 years) | Incidence of CI-AKI was 13.6% in the elderly | The high incidence of CI-AKI in the elderly was consistent across different administration route subgroups (intracoronary contrast medium group, 15.5%; intravenous contrast medium group, 12.4%) |
| No data regarding the impact of CI-AKI on a patient’s clinical course and prognosis, and no conclusive management strategy for the elderly are available | [37] |
| 2240 cancer patients with eGFR < 45 mL/min undergoing CT with contrast (out of 6463 patients) | Observational retrospective | Creatinine measurement within 48–96 h after CT | AKI rate was 2.5% | eGFR, diabetes mellitus, and serum albumin level were risk factor for AKI |
| Development of the prediction model of AKI | [38] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chomicka, I.; Kwiatkowska, M.; Lesniak, A.; Malyszko, J. Post-Contrast Acute Kidney Injury in Patients with Various Stages of Chronic Kidney Disease—Is Fear Justified? Toxins 2021, 13, 395. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13060395
Chomicka I, Kwiatkowska M, Lesniak A, Malyszko J. Post-Contrast Acute Kidney Injury in Patients with Various Stages of Chronic Kidney Disease—Is Fear Justified? Toxins. 2021; 13(6):395. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13060395
Chicago/Turabian StyleChomicka, Inga, Marlena Kwiatkowska, Alicja Lesniak, and Jolanta Malyszko. 2021. "Post-Contrast Acute Kidney Injury in Patients with Various Stages of Chronic Kidney Disease—Is Fear Justified?" Toxins 13, no. 6: 395. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13060395