Effect of Combined Bee Venom Acupuncture and NSAID Treatment for Non-Specific Chronic Neck Pain: A Randomized, Assessor-Blinded, Pilot Clinical Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
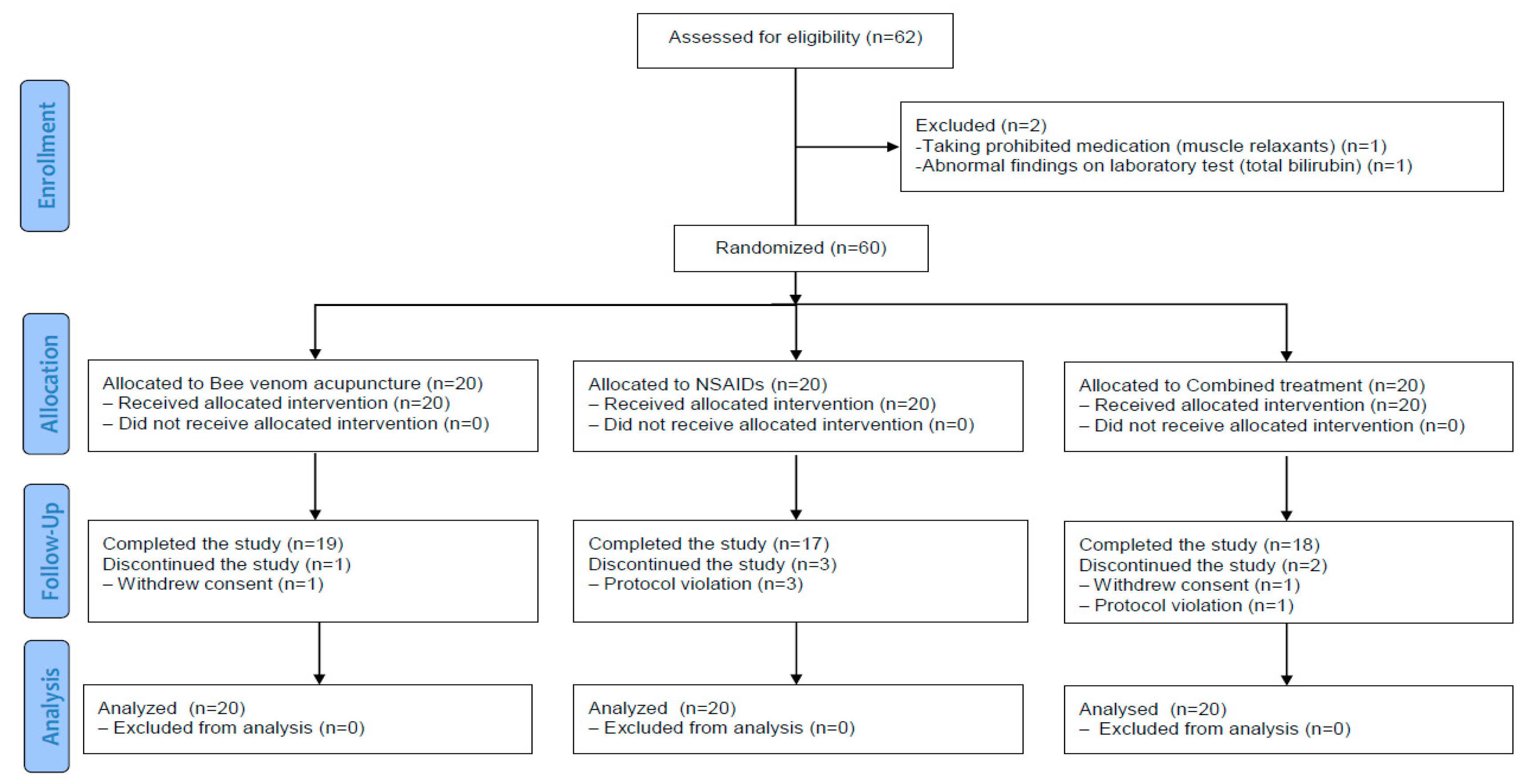
2.1. Study Participants and Feasibility Outcomes
2.2. Primary Outcome
2.3. Secondary Outcomes
2.4. Credibility Test
2.5. Safety
3. Discussion
4. Materials and Methods
4.1. Study Design and Ethics
4.2. Sample Size Calculation
4.3. Participants
4.4. Randomization and Blinding
4.5. Interventions
4.6. Outcomes
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Binder, A.I. Cervical spondylosis and neck pain. BMJ 2007, 334, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Monticone, M.; Iovine, R.; de Sena, G.; Rovere, G.; Uliano, D.; Arioli, G.; Bonaiuti, D.; Brugnoni, G.; Ceravolo, G.; Cerri, C.; et al. The Italian Society of Physical and Rehabilitation Medicine (SIMFER) recommendations for neck pain. G Ital. Med. Lav. Erg. 2013, 35, 36–50. [Google Scholar]
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine J. 2006, 15, 834–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef]
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Barendregt, J.; Blore, J.; Murray, C.; et al. The global burden of neck pain: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef]
- Borenstein, D.G. Chronic neck pain: How to approach treatment. Curr. Pain Headache Rep. 2007, 11, 436–439. [Google Scholar] [CrossRef]
- Marcum, Z.A.; Hanlon, J.T. Recognizing the risks of chronic nonsteroidal anti-inflammatory drug use in older adults. Ann. Long-Term Care Off. J. Am. Med. Dir. Assoc. 2010, 18, 24–27. [Google Scholar]
- Plastaras, C.T.; Schran, S.; Kim, N.; Sorosky, S.; Darr, D.; Chen, M.S.; Lansky, R. Complementary and alternative treatment for neck pain: Chiropractic, acupuncture, TENS, massage, yoga, Tai Chi, and Feldenkrais. Phys. Med. Rehabil. Clin. N. Am. 2011, 22, 521–537. [Google Scholar] [CrossRef] [PubMed]
- Linton, S.J.; Ryberg, M. Do epidemiological results replicate? The prevalence and health-economic consequences of neck and back pain in the general population. Eur. J. Pain 2000, 4, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Heneberg, P.; Riegerová, K.; Říhová, A.; Šimčíková, D.; Kučera, P. Updates on the surface antigens of basophils: CD16 on basophils of patients with respiratory or insect venom allergy and the rejection of CD203c and CD63 externalization decoupling by bisindolylmaleimides. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2019, 49, 54–67. [Google Scholar] [CrossRef] [Green Version]
- Son, D.J.; Lee, J.W.; Lee, Y.H.; Song, H.S.; Lee, C.K.; Hong, J.T. Therapeutic application of anti-arthritis, pain-releasing, and anti-cancer effects of bee venom and its constituent compounds. Pharmacol. Ther. 2007, 115, 246–270. [Google Scholar] [CrossRef]
- Bilò, B.M.; Bonifazi, F. Hymenoptera venom immunotherapy. Immunotherapy 2011, 3, 229–246. [Google Scholar] [CrossRef]
- Kim, S.H.; Jung, D.J.; Choi, Y.M.; Kim, J.U.; Yook, T.H. Trend of pharmacopuncture therapy for treating cervical disease in Korea. J. Pharmacopunct. 2014, 17, 7–14. [Google Scholar] [CrossRef]
- Byun, D.Y.; Kim, H.; Han, S.H.; Kim, K.W.; Lee, J.H.; Chung, W.S.; Song, M.Y.; Cho, J.H. Pharmacopuncture for lumbar herniated intervertebral disc: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2021, 43, 101369. [Google Scholar] [CrossRef] [PubMed]
- Sung, S.H.; Kim, J.W.; Han, J.E.; Shin, B.C.; Park, J.K.; Lee, G. Animal venom for medical usage in pharmacopuncture in Korean medicine: Current status and clinical implication. Toxins 2021, 13, 105. [Google Scholar] [CrossRef]
- Kwon, Y.B.; Kang, M.S.; Kim, H.W.; Ham, T.W.; Yim, Y.K.; Jeong, S.H.; Park, D.S.; Choi, D.Y.; Han, H.J.; Beitz, A.J.; et al. Antinociceptive effects of bee venom acupuncture (apipuncture) in rodent animal models: A comparative study of acupoint versus non-acupoint stimulation. Acupunct. Electro-Ther. Res. 2001, 26, 59–68. [Google Scholar] [CrossRef]
- Kwon, Y.B.; Lee, J.D.; Lee, H.J.; Han, H.J.; Mar, W.C.; Kang, S.K.; Beitz, A.J.; Lee, J.H. Bee venom injection into an acupuncture point reduces arthritis associated edema and nociceptive responses. Pain 2001, 90, 271–280. [Google Scholar] [CrossRef]
- Jeong, C.H.; Cheng, W.N.; Bae, H.; Lee, K.W.; Han, S.M.; Petriello, M.C.; Lee, H.G.; Seo, H.G.; Han, S.G. Bee venom decreases LPS-induced inflammatory responses in bovine mammary epithelial cells. J. Microbiol. Biotechnol. 2017, 27, 1827–1836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.T.; Song, H.S. A randomized controlled double blinding study of bee venom acupuncture therapy on sprain of c-spine. J. Acupunct. Res. 2005, 22, 189–195. [Google Scholar]
- Arnstein, P. Multimodal approaches to pain management. Nursing 2011, 41, 60–61. [Google Scholar] [CrossRef]
- López-de-Uralde-Villanueva, I.; Beltran-Alacreu, H.; Fernández-Carnero, J.; La Touche, R. Pain management using a multimodal physiotherapy program including a biobehavioral approach for chronic nonspecific neck pain: A randomized controlled trial. Physiother. Theory Pract. 2020, 36, 45–62. [Google Scholar] [CrossRef]
- Park, Y.C.; Koh, P.S.; Seo, B.K.; Lee, J.W.; Cho, N.S.; Park, H.S.; Park, D.S.; Baek, Y.H. Long-term effectiveness of bee venom acupuncture and physiotherapy in the treatment of adhesive capsulitis: A one-year follow-up analysis of a previous randomized controlled trial. J. Altern. Complement. Med. 2014, 20, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, T.; Fujiwara, Y.; Sollano, J.D.; Zhu, Q.; Kachintorn, U.; Rani, A.A.; Hahm, K.B.; Takahashi, S.; Joh, T.; Kinoshita, Y.; et al. A questionnaire-based survey on the prescription of non-steroidal anti-inflammatory drugs by physicians in East Asian countries in 2007. Digestion 2009, 79, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Kawatani, M.; Kinoshita, Y.; Satoh, K.; Miyagawa, I. Effectiveness of an anti-inflammatory drug, loxoprofen, for patients with nocturia. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2005, 12, 779–782. [Google Scholar] [CrossRef]
- Moore, N.; Pollack, C.; Butkerait, P. Adverse drug reactions and drug-drug interactions with over-the-counter NSAIDs. Ther. Clin. Risk Manag. 2015, 11, 1061–1075. [Google Scholar] [CrossRef] [Green Version]
- Greig, S.L.; Garnock-Jones, K.P. Loxoprofen: A review in pain and inflammation. Clin. Drug Investig. 2016, 36, 771–781. [Google Scholar] [CrossRef]
- Fine, M. Quantifying the impact of NSAID-associated adverse events. Am. J. Manag. Care 2013, 19, s267–s272. [Google Scholar] [PubMed]
- Yang, W.; Zhang, Y.; Yang, G.; Geng, Y.; Chen, D.; Wang, J.; Ye, Y.; Wang, H.; Xia, D.; Hu, F.; et al. Anti-PD-1 immunotherapy and bee venom for relapsed and refractory liposarcoma: A case report. Front. Oncol. 2021, 11, 668992. [Google Scholar] [CrossRef]
- Seo, B.K.; Han, K.; Kwon, O.; Jo, D.J.; Lee, J.H. Efficacy of bee venom acupuncture for chronic low back pain: A randomized, double-blinded, sham-controlled trial. Toxins 2017, 9, 361. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.; Kim, M.J.; Go, D.; Min, B.I.; Na, H.S.; Kim, S.K. Combined effects of bee venom acupuncture and morphine on oxaliplatin-induced neuropathic pain in mice. Toxins 2016, 8, 33. [Google Scholar] [CrossRef] [PubMed]
- Baek, Y.H.; Huh, J.E.; Lee, J.D.; Choi, D.Y.; Park, D.S. Antinociceptive effect and the mechanism of bee venom acupuncture (apipuncture) on inflammatory pain in the rat model of collagen-induced arthritis: Mediation by alpha2-adrenoceptors. Brain Res. 2006, 1073-1074, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Kwon, Y.B.; Han, H.J.; Yang, I.S.; Beitz, A.J.; Lee, J.H. Antinociceptive mechanisms associated with diluted bee venom acupuncture (apipuncture) in the rat formalin test: Involvement of descending adrenergic and serotonergic pathways. Pharmacol. Res. 2005, 51, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.S.; Moon, H.J.; Li, D.X.; Gil, M.; Min, J.K.; Lee, G.; Bae, H.; Kim, S.K.; Min, B.I. Effect of bee venom acupuncture on oxaliplatin-induced cold allodynia in rats. Evid. Based Complement. Altern. Med. eCAM 2013, 2013, 369324. [Google Scholar] [CrossRef]
- Kim, H.W.; Kwon, Y.B.; Ham, T.W.; Roh, D.H.; Yoon, S.Y.; Lee, H.J.; Han, H.J.; Yang, I.S.; Beitz, A.J.; Lee, J.H. Acupoint stimulation using bee venom attenuates formalin-induced pain behavior and spinal cord fos expression in rats. J. Vet. Med. Sci. 2003, 65, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Nam, K.W.; Je, K.H.; Lee, J.H.; Han, H.J.; Lee, H.J.; Kang, S.K.; Mar, W. Inhibition of COX-2 activity and proinflammatory cytokines (TNF-alpha and IL-1beta) production by water-soluble sub-fractionated parts from bee (Apis mellifera) venom. Arch. Pharmacal Res. 2003, 26, 383–388. [Google Scholar] [CrossRef]
- Jang, S.; Kim, K.H. Clinical effectiveness and adverse events of bee venom therapy: A systematic review of randomized controlled trials. Toxins 2020, 12, 558. [Google Scholar] [CrossRef]
- Seo, B.K.; Lee, J.H.; Kim, P.K.; Baek, Y.H.; Jo, D.J.; Lee, S. Bee venom acupuncture, NSAIDs or combined treatment for chronic neck pain: Study protocol for a randomized, assessor-blind trial. Trials 2014, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Jung, D.J.; Lee, H.G.; Choi, Y.M.; Song, B.Y.; Yook, T.H.; Kim, J.U. The clinical study on 130 cases with sweet bee venom treatment. J. Acupunct. Res. 2013, 30, 211–217. [Google Scholar] [CrossRef]
- Korean Society of Acupuncture and Moxibustion Medicine Textbook Compilation Committee. The Acupuncture and Moxibustion Medicine; Jipmoondang Publishing Co.: Seoul, Korea, 2014. [Google Scholar]
- Patrick, D.L.; Deyo, R.A.; Atlas, S.J.; Singer, D.E.; Chapin, A.; Keller, R.B. Assessing health-related quality of life in patients with sciatica. Spine 1995, 20, 1899–1909. [Google Scholar] [CrossRef]
- MacDowall, A.; Skeppholm, M.; Robinson, Y.; Olerud, C. Validation of the visual analog scale in the cervical spine. J. Neurosurg. Spine 2018, 28, 227–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- MacDermid, J.C.; Walton, D.M.; Avery, S.; Blanchard, A.; Etruw, E.; McAlpine, C.; Goldsmith, C.H. Measurement properties of the neck disability index: A systematic review. J. Orthop. Sports Phys. Ther. 2009, 39, 400–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, K.J.; Choi, B.W.; Choi, B.R.; Seo, G.B. Cross-cultural adaptation and validation of the Korean version of the neck disability index. Spine 2010, 35, E1045–E1049. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Cho, Y.S.; Uhm, W.S.; Kim, S.; Bae, S.C. Cross-cultural adaptation and validation of the Korean version of the EQ-5D in patients with rheumatic diseases. Qual. Life Res. Int. J. Qual. Life Aspects Treat. Care Rehabil. 2005, 14, 1401–1406. [Google Scholar] [CrossRef] [PubMed]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Han, C.W.; Lee, E.J.; Iwaya, T.; Kataoka, H.; Kohzuki, M. Development of the Korean version of Short-Form 36-Item Health Survey: Health related QOL of healthy elderly people and elderly patients in Korea. Tohoku J. Exp. Med. 2004, 203, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Vincent, C.; Lewith, G. Placebo controls for acupuncture studies. J. R. Soc. Med. 1995, 88, 199–202. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | BVA Group (n = 20) | NSAIDs Group (n = 20) | Combined Group (n = 20) | p-Value | F-Value |
|---|---|---|---|---|---|
| Sex (Male/Female) * | 7 (35.0%)/13 (65.0%) | 5 (25.0%)/15 (75.0%) | 3 (15.0%)/17 (85.0%) | 0.4023 | - |
| Age (years) + | 52.30 (48.10, 56.50) | 37.65 (33.45, 41.85) | 45.50 (40.18, 50.82) | <0.0001 | 11.11 |
| Height (cm) + | 164.15 (161.41, 166.89) | 164.72 (161.64, 167.80) | 161.99 (157.97, 166.01) | 0.4447 | 0.82 |
| Weight (kg) + | 63.75 (59.21, 68.28) | 62.13 (57.77, 66.49) | 59.03 (54.96, 63.09) | 0.2674 | 1.35 |
| BMI (kg/m2) + | 23.61 (22.18, 25.04) | 22.79 (21.76, 23.82) | 22.63 (21.44, 23.82) | 0.4526 | 0.80 |
| Smoke (Yes/No) * | 2 (10.0%)/18 (90.0%) | 2 (10.0%)/18 (90.0%) | 1 (5.0%)/19 (95.0%) | 0.9999 | - |
| Drink (Yes/No) * | 4 (20.0%)/16 (80.0%) | 6 (30.0%)/14 (70.0%) | 7 (35.0%)/13 (65.0%) | 0.6752 | - |
| SBP (mmHg) + | 119.8 (113.5, 126.0) | 120.1 (112.7, 127.4) | 119.6 (112.5, 126.6) | 0.9942 | 0.01 |
| DBP (mmHg) + | 78.40 (74.56, 82.24) | 79.95 (76.46, 83.44) | 74.90 (70.62, 79.18) | 0.7290 | 0.32 |
| Pulse (times/min) + | 73.05 (68.91, 77.19) | 74.95 (70.86, 79.04) | 72.65 (67.30, 78.00) | 0.1521 | 1.95 |
| Temperature (°C) + | 36.52 (36.48, 36.56) | 36.50 (36.45, 36.55) | 36.46 (36.41, 36.50) | 0.1147 | 2.25 |
| Outcome | BVA (n = 20) | NSAIDs (n = 20) | Combined (n = 20) | p-Value + (between the 3 Groups) | BVA Versus NSAIDs † | NSAIDs Versus Combined † | BVA Versus Combined † | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (95% CI) | p-Value * (within) | Mean (95% CI) | p-Value * (within) | Mean (95% CI) | p-Value * (within) | |||||
| VAS (Bothersomeness) | ||||||||||
| Baseline | 60.85 (52.68, 69.02) | 56.20 (47.60, 64.80) | 65.60 (59.65, 71.55) | |||||||
| Week 2 | 39.20 (29.95, 48.45) | <0.0001 | 37.15 (28.73, 45.57) | 0.0005 | 47.65 (38.96, 56.34) | <0.0001 | 0.3505 | −4.96 (−20.47, 10.55) | −3.07 (−17.19, 11.06) | −8.03 (−21.85, 5.79) |
| Week 3 | 32.00 (21.78, 42.22) | <0.0001 | 36.75 (27.52, 45.98) | 0.0003 | 45.30 (34.84, 55.76) | 0.0002 | 0.0442 | −15.10 (−32.21, 2.02) | 1.22 (−14.37, 16.81) | −13.88 (−29.13, 1.37) |
| Week 4 | 26.25 (17.70, 34.79) | <0.0001 | 31.65 (21.91, 41.39) | 0.0001 | 43.35 (33.62, 53.08) | <0.0001 | 0.0317 | −11.39 (−28.43, 5.66) | −4.91 (−20.44, 10.62) | −16.30 (−31.48, −1.11) |
| Week 8 | 26.95 (18.77, 35.13) | <0.0001 | 41.25 (31.37, 51.13) | 0.0012 | 40.00 (27.51, 52.49) | 0.0003 | 0.0214 | −20.93 (−39.37, −2.49) | 9.13 (−7.67, 25.92) | −11.80 (−28.23, 4.63) |
| VAS (Pain) | ||||||||||
| Baseline | 56.80 (46.94, 66.66) | 50.65 (40.38, 60.92) | 64.55 (56.88, 72.22) | |||||||
| Week 2 | 36.25 (27.35, 45.15) | <0.0001 | 36.15 (26.86, 45.44) | 0.0007 | 47.05 (39.67, 54.43) | 0.0004 | 0.3149 | −5.44 (−19.32, 8.44) | −2.02 (−14.82, 10.79) | −7.45 (−19.79, 4.88) |
| Week 3 | 29.65 (20.19, 39.11) | <0.0001 | 35.50 (26.09, 44.91) | 0.0016 | 43.00 (34.07, 51.93) | 0.0002 | 0.0314 | −15.44 (−30.30, −0.59) | 3.31 (−10.39, 17.01) | −12.13 (−25.33, 1.06) |
| Week 4 | 26.60 (17.62, 35.58) | <0.0001 | 31.45 (20.87, 42.03) | 0.0011 | 43.25 (34.36, 52.14) | <0.0001 | 0.0375 | −12.70 (−28.84, 3.43) | −1.71 (−16.61, 13.18) | −14.42 (−28.76, −0.08) |
| Week 8 | 25.75 (17.65, 33.85) | <0.0001 | 38.85 (27.28, 50.42) | 0.0304 | 38.70 (26.19, 51.21) | 0.0002 | 0.0864 | −17.83 (−37.71, 2.06) | 8.31 (−10.04, 26.66) | −9.52 (−27.19, 8.16) |
| NDI | ||||||||||
| Baseline | 30.1 (25.0, 35.1) | 27.1 (20.8, 33.3) | 31.1 (25.5, 36.6) | |||||||
| Week 2 | 22.1 (16.3, 27.9) | 0.0004 | 23.7 (17.5, 29.8) | 0.0628 | 22.5 (17.3, 27.7) | 0.0007 | 0.0479 | −6.8 (−14.2, 0.6) | 5.7 (−0.9, 12.3) | −1.1 (−7.7, 5.4) |
| Week 3 | 18.5 (12.6, 24.4) | <0.0001 | 21.7 (15.6, 27.7) | 0.0137 | 20.8 (15.9, 25.6) | 0.0003 | 0.0733 | −7.2 (−14.8, 0.4) | 4.7 (−2.1, 11.5) | −2.5 (−9.2, 4.2) |
| Week 4 | 17.9 (12.7, 23.0) | <0.0001 | 20.9 (12.8, 28.9) | 0.0196 | 22.6 (15.2, 29.9) | 0.0039 | 0.0756 | −8.6 (−17.9, 0.8) | 3.3 (−5.0, 11.7) | −5.2 (−13.5, 3.1) |
| Week 8 | 16.7 (10.6, 22.7) | <0.0001 | 24.1 (16.2, 31.9) | 0.1706 | 20.9 (14.4, 27.4) | 0.0008 | 0.0098 | −11.7 (−21.1, −2.3) | 7.5 (−0.9, 15.9) | −4.2 (−12.5, 4.2) |
| EQ-5D | ||||||||||
| Baseline | 0.782 (0.714, 0.850) | 0.827 (0.770, 0.884) | 0.801 (0.744, 0.858) | |||||||
| Week 2 | 0.818 (0.758, 0.879) | 0.1810 | 0.869 (0.824, 0.914) | 0.0084 | 0.859 (0.826, 0.892) | 0.0279 | 0.6737 | −0.006 (−0.078, 0.066) | −0.015 (−0.079, 0.049) | −0.021 (−0.084, 0.042) |
| Week 3 | 0.851 (0.790, 0.913) | 0.0036 | 0.850 (0.794, 0.906) | 0.3553 | 0.869 (0.838, 0.900) | 0.0079 | 0.1624 | 0.053 (−0.022, 0.128) | −0.048 (−0.114, 0.019) | 0.005 (−0.060, 0.071) |
| Week 4 | 0.844 (0.784, 0.905) | 0.0036 | 0.845 (0.781, 0.909) | 0.1000 | 0.850 (0.806, 0.894) | 0.0420 | 0.3985 | 0.037 (−0.034, 0.107) | −0.027 (−0.089, 0.036) | 0.010 (−0.052, 0.072) |
| Week 8 | 0.866 (0.817, 0.914) | 0.0011 | 0.847 (0.777, 0.916) | 0.2041 | 0.860 (0.817, 0.902) | 0.0169 | 0.0588 | 0.071 (−0.0034, 0.145) | −0.043 (−0.109, 0.023) | 0.029 (−0.036, 0.094) |
| SF-36 | ||||||||||
| Baseline | 63.41 (55.54, 71.27) | 66.90 (57.83, 75.97) | 62.00 (55.79, 68.21) | |||||||
| Week 4 | 68.77 (60.45, 77.09) | 0.0012 | 69.82 (59.75, 79.88) | 0.1269 | 65.35 (57.19, 73.50) | 0.2276 | 0.1164 | 6.86 (−1.41, 15.12) | −2.64 (−10.02, 4.74) | 4.22 (−3.11, 11.55) |
| Week 8 | 70.93 (62.66, 79.19) | 0.0002 | 67.52 (58.13, 76.91) | 0.7173 | 68.42 (60.91, 75.92) | 0.0245 | 0.0182 | 9.44 (1.00, 17.89) | −6.86 (−14.41, 0.68) | 2.58 (−4.91, 10.07) |
| BDI | ||||||||||
| Baseline | 10.65 (6.79, 14.51) | 9.50 (4.06, 14.94) | 10.55 (7.27, 13.83) | |||||||
| Week 4 | 5.90 (2.07, 9.73) | 0.0025 | 7.80 (2.05, 13.55) | 0.0417 | 6.70 (3.26, 10.14) | 0.0040 | 0.1496 | −3.67 (−8.42, 1.09) | 2.42 (−1.80, 6.64) | −1.24 (−5.42, 2.93) |
| Week 8 | 4.85 (1.47, 8.23) | 0.0001 | 8.20 (2.00, 14.40) | 0.1156 | 6.80 (3.25, 10.35) | 0.0041 | 0.0250 | −5.07 (−9.61, −0.53) | 0.075 (−0.009, 0.159) | −0.042 (−0.125, 0.042) |
| Outcome | BVA (n = 20) | NSAIDs (n = 20) | Combined (n = 20) | p-Value + (between the 3 Groups) | |||
|---|---|---|---|---|---|---|---|
| Mean (95% CI) | p-Value * (within) | Mean (95% CI) | p-Value * (within) | Mean (95% CI) | p-Value * (within) | ||
| Total score | |||||||
| Baseline | 20.20 (18.96, 21.44) | 18.80 (17.36, 20.24) | 18.30 (16.83, 19.77) | ||||
| Week 4 | 19.75 (18.48, 21.02) | 0.5473 | 17.75 (16.22, 19.28) | 0.0308 | 17.95 (16.65, 19.25) | 0.6032 | 0.3108 |
| Expectation of NCNP improvement | |||||||
| Baseline | 5.20 (4.87, 5.53) | 4.90 (4.56, 5.24) | 4.80 (4.44, 5.16) | ||||
| Week 4 | 5.00 (4.70, 5.30) | 0.2967 | 4.65 (4.21, 5.09) | 0.1713 | 4.60 (4.19, 5.01) | 0.3299 | 0.6682 |
| Willingness to recommend to others | |||||||
| Baseline | 5.15 (4.80, 5.50) | 4.65 (4.27, 5.03) | 4.65 (4.24, 5.06) | ||||
| Week 4 | 5.00 (4.66, 5.34) | 0.481 | 4.25 (3.73, 4.77) | 0.0421 | 4.55 (4.23, 4.87) | 0.5409 | 0.3162 |
| Rationality of treatment | |||||||
| Baseline | 4.95 (4.63, 5.27) | 4.70 (4.30, 5.10) | 4.50 (4.11, 4.89) | ||||
| Week 4 | 4.85 (4.54, 5.16) | 0.5770 | 4.35 (3.89, 4.81) | 0.0153 | 4.40 (3.99, 4.81) | 0.6493 | 0.4537 |
| Effectiveness for alleviating other complaints | |||||||
| Baseline | 4.90 (4.50, 5.30) | 4.55 (4.08, 5.02) | 4.35 (3.89, 4.81) | ||||
| Week 4 | 4.90 (4.40, 5.40) | 0.9999 | 4.50 (4.06, 4.94) | 0.8037 | 4.40 (4.05, 4.75) | 0.8336 | 0.3064 |
| Inclusion Criteria |
| (1) Age between 18 and 65 years old |
| (2) Non-specific, uncomplicated, and chronic neck pain for ≥3 months at screening visit |
| (3) Participants who voluntarily agree to participate and sign written informed consent |
| Exclusion Criteria |
| (1) Abnormalities on neurological examination |
| (2) Neck pain with radicular pain |
| (3) Serious spinal disorders including malignancy, vertebral fracture, spinal infection, and inflammatory spondylitis |
| (4) Other chronic diseases that were judged to affect the therapeutic outcomes, including cardiovascular disease, diabetic neuropathy, active hepatitis, fibromyalgia, rheumatoid arthritis, dementia, and epilepsy |
| (5) History of spinal surgery or scheduled spinal surgery during the trial period |
| (6) Pain induced by a traffic accident |
| (7) A substantial musculoskeletal problem other than neck pain |
| (8) Conditions for which the administration of bee venom treatment might not be safe, including clotting disorders, administration of an anticoagulant agent, pregnancy, and seizure disorders |
| (9) A hypersensitive reaction to previous bee venom treatment, bee stings, or insect bites |
| (10) A positive reaction observed during a skin hypersensitivity test at screening visit |
| (11) Diagnosis of severe psychiatric or psychological disorders |
| (12) Current use of corticosteroids, narcotics, muscle relaxants, or herbal medicines to treat neck pain or use of any medication judged inappropriate by the investigator |
| (13) Pending lawsuits or receipt of compensation due to neck pain |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, B.; Seo, B.-K.; Kwon, O.-J.; Jo, D.-J.; Lee, J.-H.; Lee, S. Effect of Combined Bee Venom Acupuncture and NSAID Treatment for Non-Specific Chronic Neck Pain: A Randomized, Assessor-Blinded, Pilot Clinical Trial. Toxins 2021, 13, 436. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070436
Lee B, Seo B-K, Kwon O-J, Jo D-J, Lee J-H, Lee S. Effect of Combined Bee Venom Acupuncture and NSAID Treatment for Non-Specific Chronic Neck Pain: A Randomized, Assessor-Blinded, Pilot Clinical Trial. Toxins. 2021; 13(7):436. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070436
Chicago/Turabian StyleLee, Boram, Byung-Kwan Seo, O-Jin Kwon, Dae-Jean Jo, Jun-Hwan Lee, and Sanghun Lee. 2021. "Effect of Combined Bee Venom Acupuncture and NSAID Treatment for Non-Specific Chronic Neck Pain: A Randomized, Assessor-Blinded, Pilot Clinical Trial" Toxins 13, no. 7: 436. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070436