Biomonitoring of Mycotoxins in Plasma of Patients with Alzheimer’s and Parkinson’s Disease

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Results and Discussion
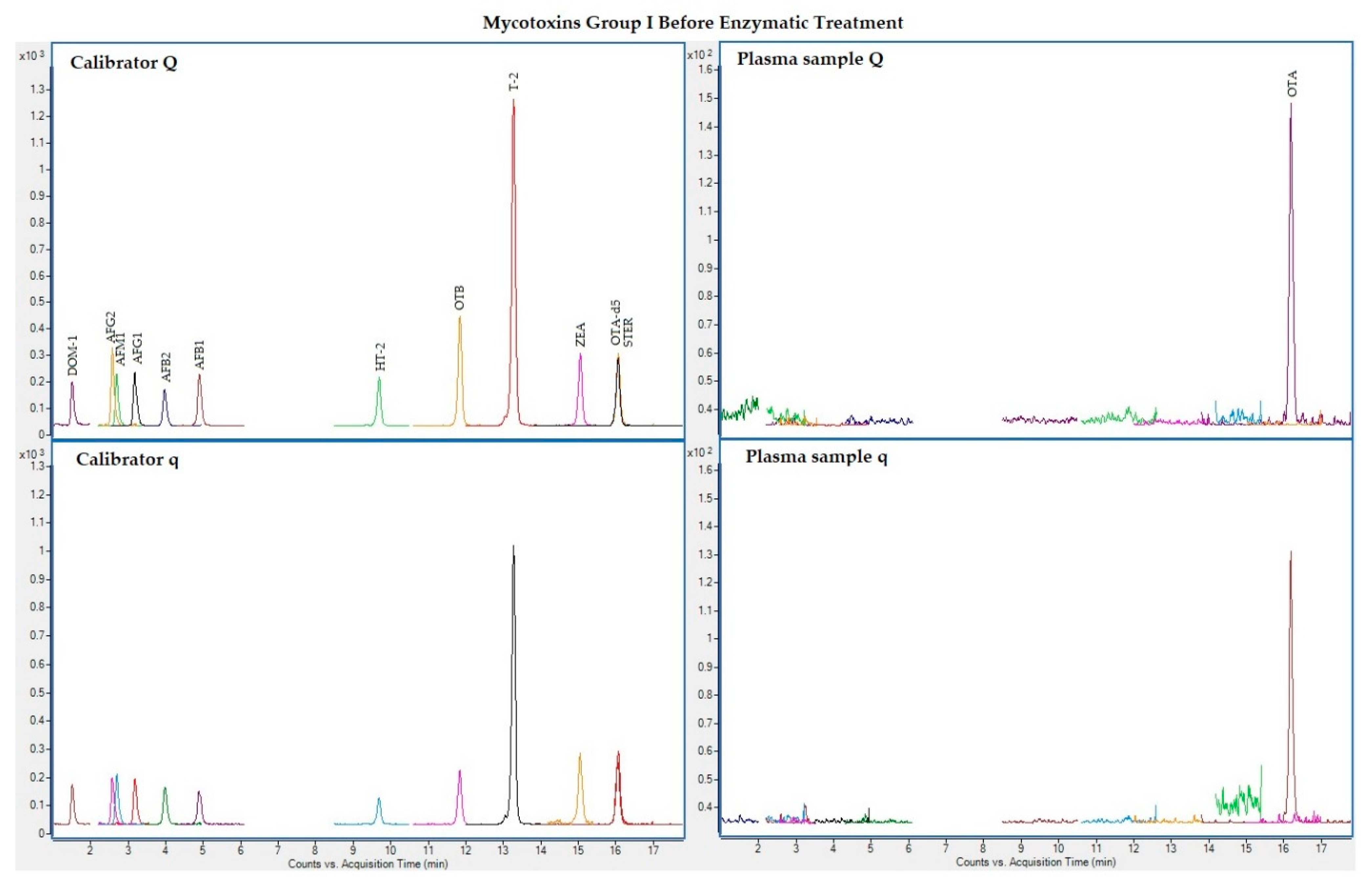
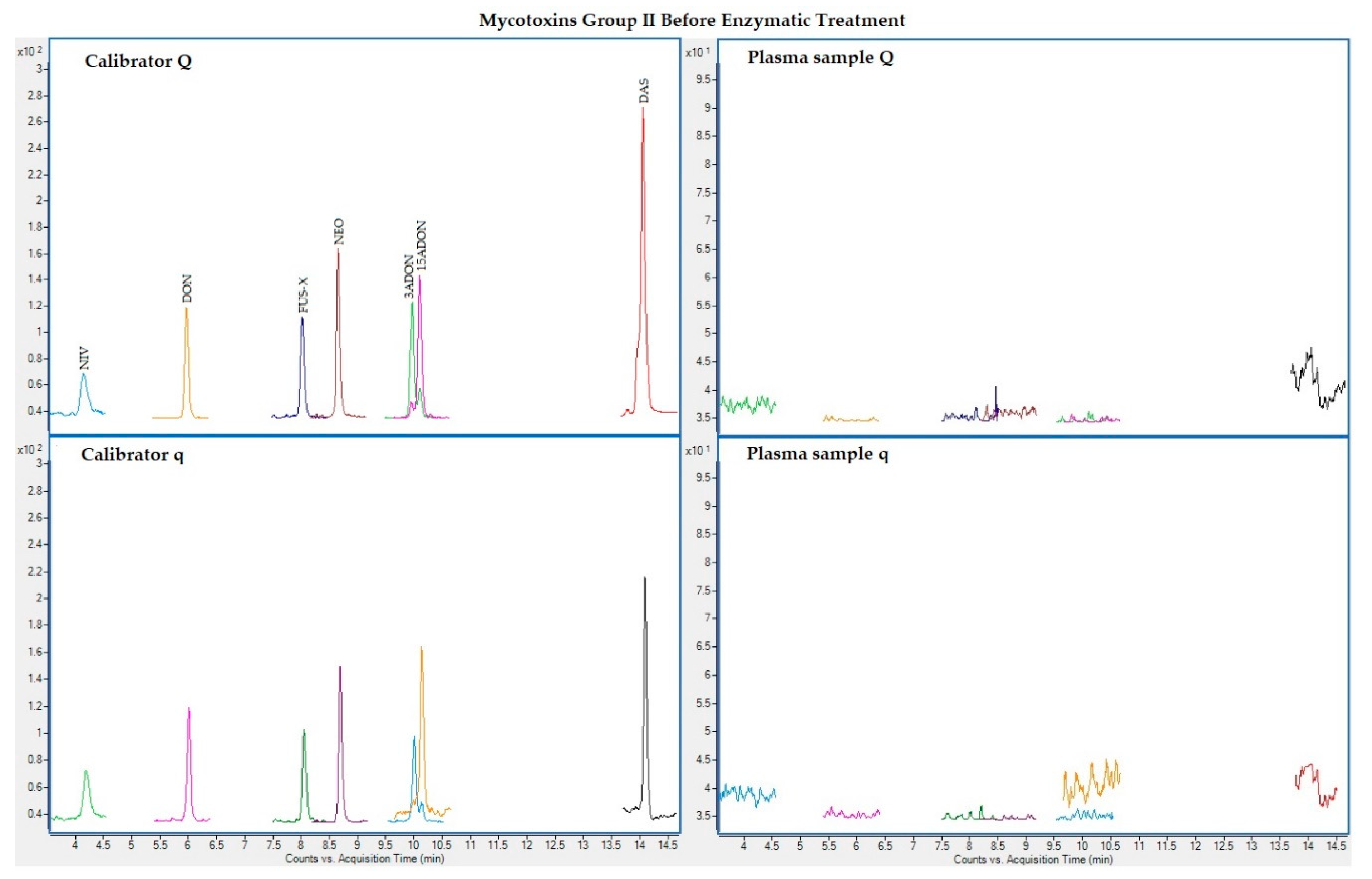
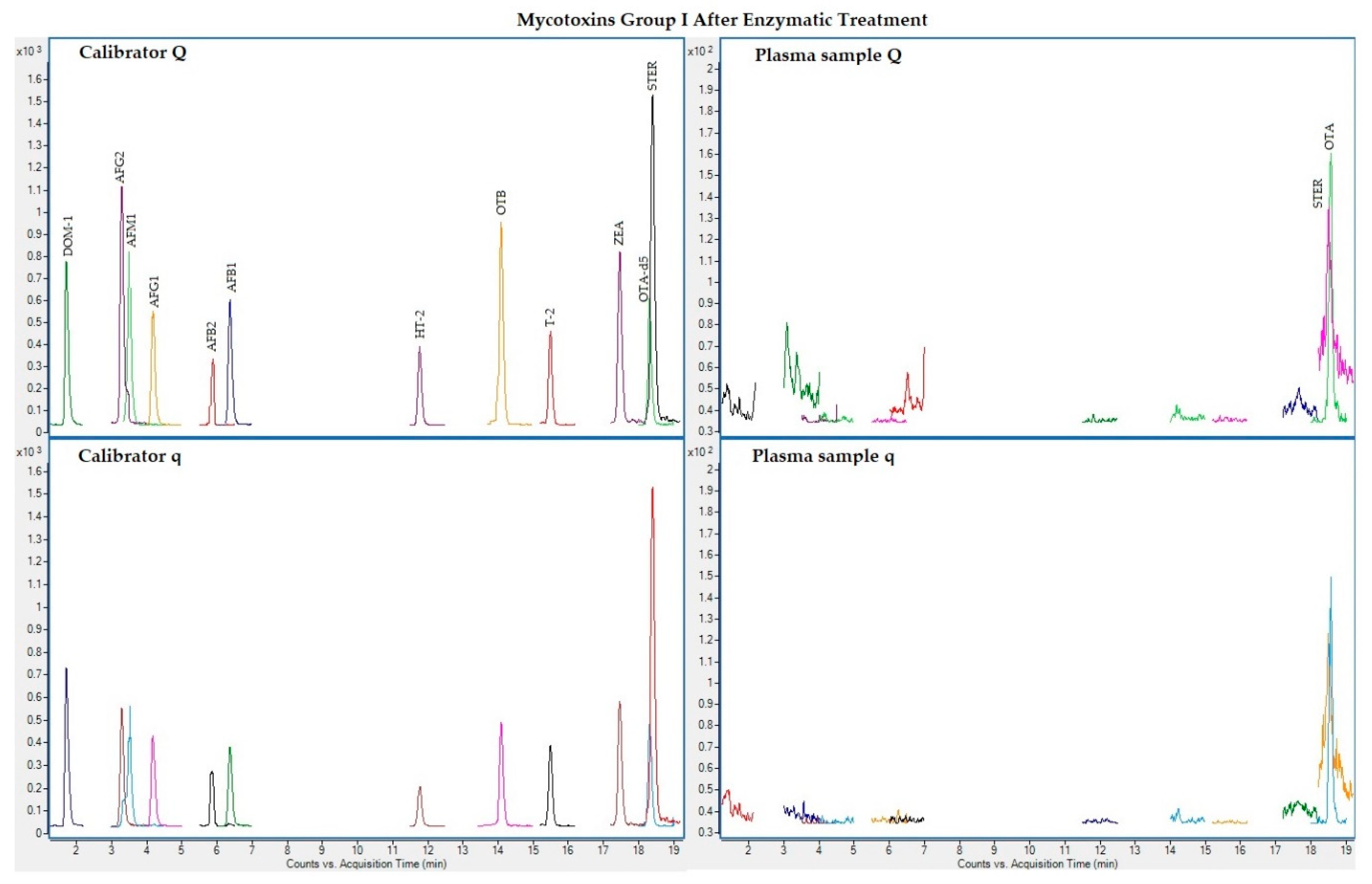
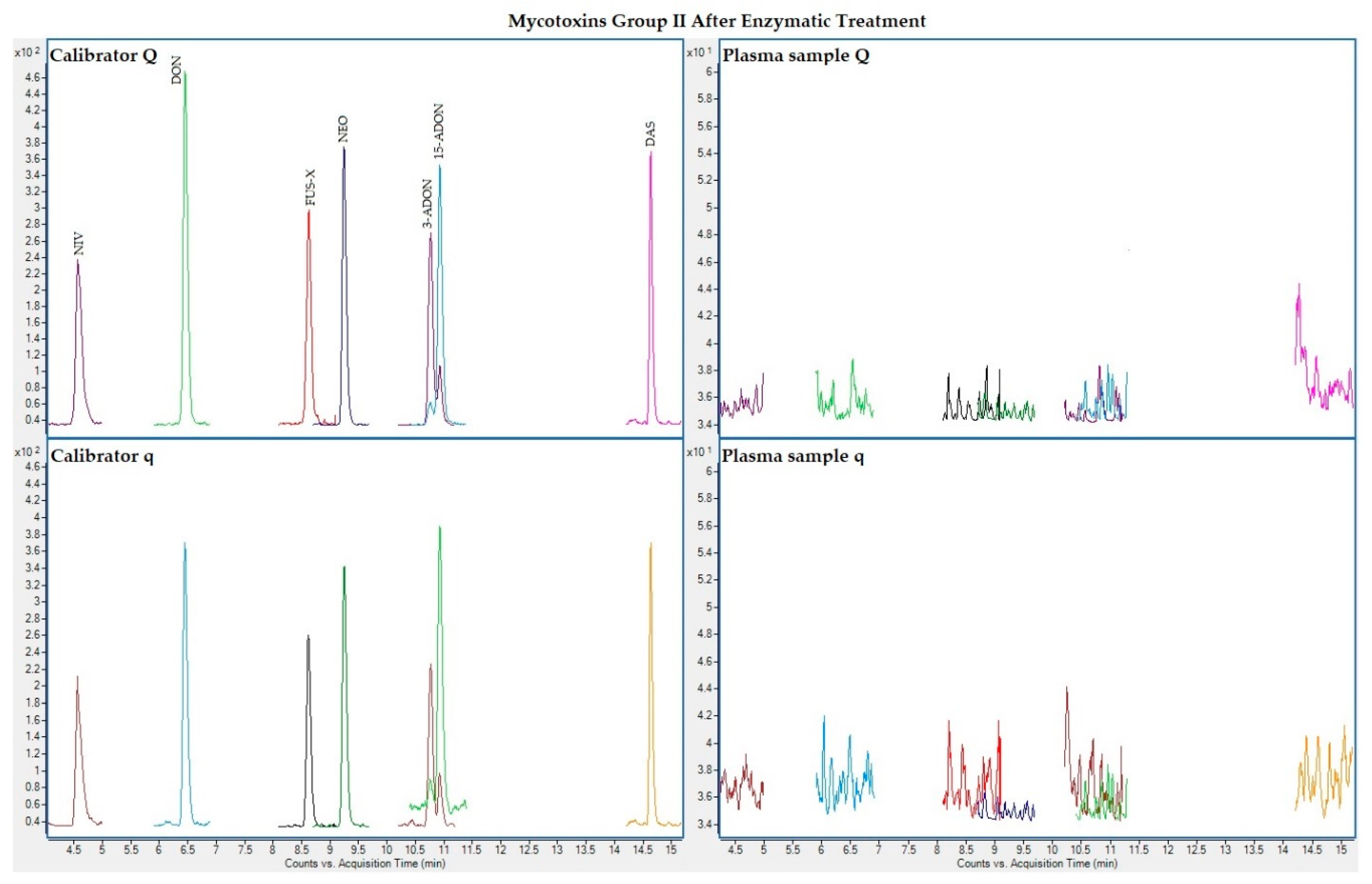
2.1. LC-MS/MS Analysis
2.2. Plasma Samples
2.3. Presence of Mycotoxins
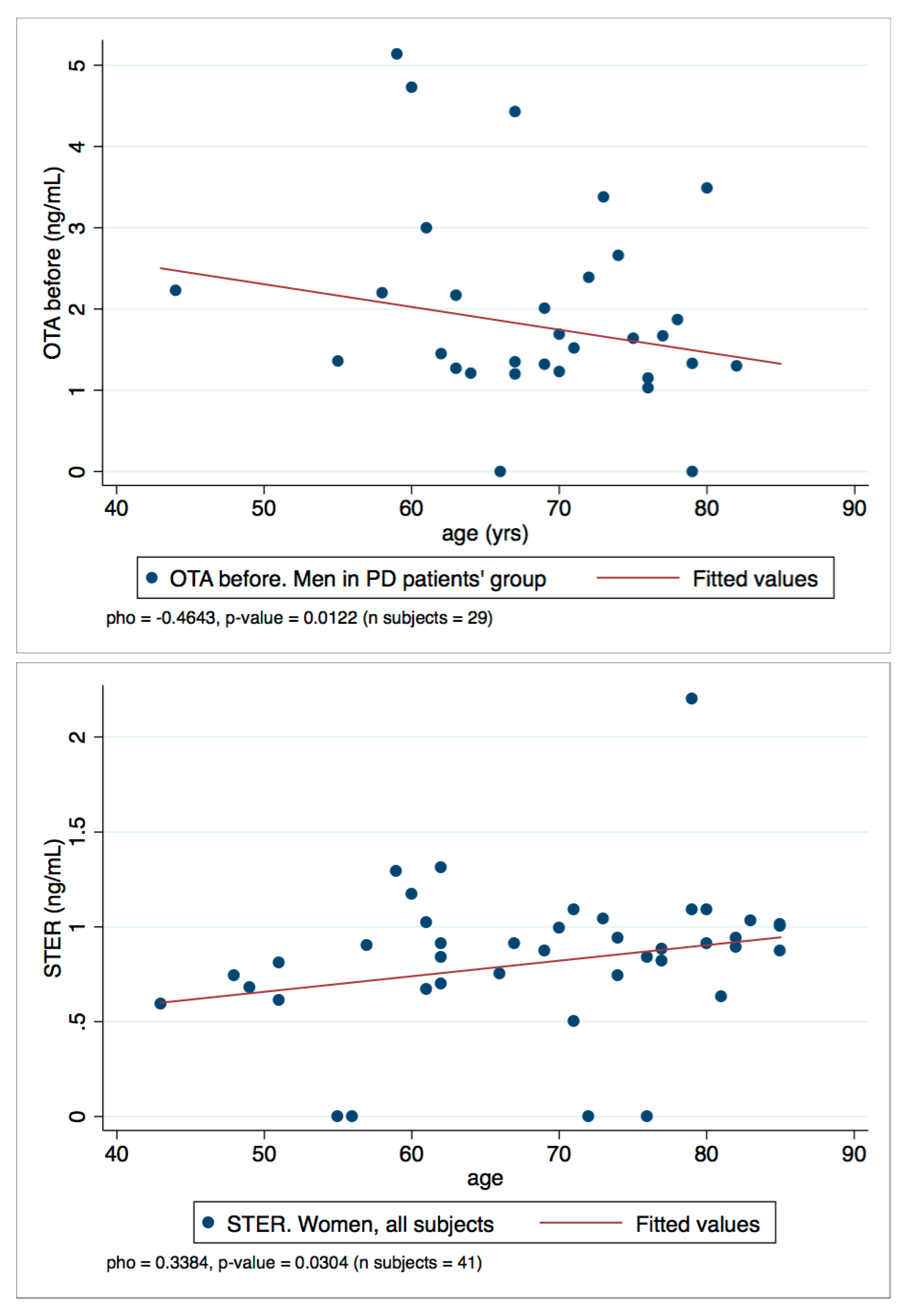
2.4. Statistical Analysis
3. Conclusions
4. Materials and Methods
4.1. Reagents
4.2. Subjects
4.3. Plasma Collection
4.4. Sample Preparation
4.5. LC/MS-MS Analysis
4.6. Analytical Method Validation
4.7. Statistical Analysis and Data Handling
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 15-ADON | 15-acetyldeoxynivalenol |
| 3-ADON | 3-acetyldeoxynivalenol |
| Aβ | amyloid beta |
| ACN | acetonitrile |
| AD | Alzheimer´s disease |
| AFB1 | aflatoxin B1 |
| AFB2 | aflatoxin B2 |
| AFG1 | aflatoxin G1 |
| AFG2 | aflatoxin G2 |
| AFM1 | aflatoxin M1 |
| CIRS | chronic inflammatory response syndrome |
| CNT | control |
| DAS | diacetoxyscirpenol |
| DOM-1 | deepoxy-deoxynivalenol |
| DON | deoxynivalenol |
| FUS-X | fusarenon-X |
| GDS | Global Deterioration Scale |
| HBM | human biomonitoring |
| HY | Hoehn and Yahr |
| LC | liquid chromatography |
| LC-MS/MS | liquid chromatography coupled to mass spectrometry in tandem |
| LOD | limit of detection |
| LOQ | limit of quantification |
| NEO | neosolaniol |
| NIV | nivalenol |
| OTA | ochratoxin A |
| OTA-d5 | ochratoxin A-(phenyl-d5) |
| OTB | ochratoxin B |
| PD | Parkinson´s disease |
| q | transition of qualification |
| Q | transition of quantification |
| QqQ | triple quadrupole |
| RE | relative error of the mean |
| SD | standard deviation |
| STER | sterigmatocystin |
| ZEA | zearalenone |
References
- Serrano-Pozo, A.; Frosch, M.P.; Masliah, E.; Hyman, B.T. Neuropathological alterations in Alzheimer disease. Cold Spring Harb. Perspect. Med. 2011, 1, a006189. [Google Scholar] [CrossRef]
- Fearnley, J.M.; Lees, A.J. Ageing and Parkinson’s disease: Substantia nigra regional selectivity. Brain 1991, 114, 2283–2301. [Google Scholar] [CrossRef]
- Barber, R.C. The genetics of Alzheimer’s disease. Scientifica (Cairo) 2012, 2012, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Izco, M.; Carlos, E.; Alvarez-Erviti, L. The two faces of Exosomes in Parkinson’s disease: From pathology to therapy. Neuroscientist 2021, 107385842199000. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Dan, X.; Babbar, M.; Wei, Y.; Hasselbalch, S.G.; Croteau, D.L.; Bohr, V.A. Ageing as a risk factor for neurodegenerative disease. Nat. Rev. Neurol. 2019, 15, 565–581. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.E.; Stecher, B.; Labrie, V.; Brundin, L.; Brundin, P. Triggers, Facilitators, and Aggravators: Redefining Parkinson’s Disease Pathogenesis. Trends Neurosci. 2019, 42, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Wainaina, M.N.; Chen, Z.; Zhong, C. Environmental factors in the development and progression of late-onset Alzheimer’s disease. Neurosci. Bull. 2014, 30, 253–270. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.A.; Rahman, M.S.; Uddin, M.J.; Mamum-Or-Rashid, A.N.M.; Pang, M.-G.; Rhim, H. Emerging risk of environmental factors: Insight mechanisms of Alzheimer’s diseases. Environ. Sci. Pollut. Res. 2020, 27, 44659–44672. [Google Scholar] [CrossRef] [PubMed]
- Bush, A.I. The Metal Theory of Alzheimer’s disease. J. Alzheimer’s Dis. 2012, 33, S277–S281. [Google Scholar] [CrossRef]
- Moulton, P.V.; Yang, W. Air pollution, oxidative stress, and Alzheimer’s disease. J. Environ. Public Health 2012, 2012, 472751. [Google Scholar] [CrossRef]
- Li, Y.; Fang, R.; Liu, Z.; Jiang, L.; Zhang, J.; Li, H.; Liu, C.; Li, F. The association between toxic pesticide environmental exposure and Alzheimer’s disease: A scientometric and visualization analysis. Chemosphere 2021, 263, 128238. [Google Scholar] [CrossRef]
- Fulop, T.; Witkowski, J.M.; Bourgade, K.; Khalil, A.; Zerif, E.; Larbi, A.; Hirokawa, K.; Pawelec, G.; Bocti, C.; Lacombe, G.; et al. Can an infection hypothesis explain the beta amyloid hypothesis of Alzheimer’s disease? Front. Aging Neurosci. 2018, 10, 224. [Google Scholar] [CrossRef] [Green Version]
- Vasefi, M.; Ghaboolian-Zare, E.; Abedelwahab, H.; Osu, A. Environmental toxins and Alzheimer’s disease progression. Neurochem. Int. 2020, 141, 104852. [Google Scholar] [CrossRef]
- Goldman, S.M. Environmental toxins and Parkinson’s disease. Annu. Rev. Pharmacol. Toxicol. 2014, 54, 141–164. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Canning, C.G.; Goldman, S.M. Environment, lifestyle, and Parkinson’s disease: Implications for prevention in the next decade. Mov. Disord. 2019, 34, 801–811. [Google Scholar] [CrossRef] [PubMed]
- van der Mark, M.; Brouwer, M.; Kromhout, H.; Nijssen, P.; Huss, A.; Vermeulen, R. Is pesticide use related to Parkinson disease? Some clues to heterogeneity in study results. Environ. Health Perspect. 2012, 120, 340–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorell, J.M.; Johnson, C.C.; Rybicki, B.A.; Peterson, E.L.; Richardson, R.J. The risk of Parkinson’s disease with exposure to pesticides, farming, well water, and rural living. Neurology 1998, 50, 1346–1350. [Google Scholar] [CrossRef]
- Priyadarshi, A.; Khuder, S.A.; Schaub, E.A.; Priyadarshi, S.S. Environmental risk factors and Parkinson’s disease: A metaanalysis. Environ. Res. 2001, 86, 122–127. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, N.J.; Bowers, E.; Hurburgh, C.; Wu, F. Potential economic losses to the US corn industry from aflatoxin contamination. Food Addit. Contam. Part A 2016, 33, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Marin, S.; Ramos, A.J.; Cano-Sancho, G.; Sanchis, V. Mycotoxins: Occurrence, toxicology, and exposure assessment. Food Chem. Toxicol. 2013, 60, 218–237. [Google Scholar] [CrossRef]
- Janik, E.; Niemcewicz, M.; Ceremuga, M.; Stela, M.; Saluk-Bijak, J.; Siadkowski, A.; Bijak, M. Molecular aspects of mycotoxins—A serious problem for human health. Int. J. Mol. Sci. 2020, 21, 8187. [Google Scholar] [CrossRef]
- Logrieco, A.; Miller, J.; Eskola, M.; Krska, R.; Ayalew, A.; Bandyopadhyay, R.; Battilani, P.; Bhatnagar, D.; Chulze, S.; De Saeger, S.; et al. The mycotox charter: Increasing awareness of, and concerted action for, minimizing mycotoxin exposure worldwide. Toxins (Basel) 2018, 10, 149. [Google Scholar] [CrossRef] [Green Version]
- European Commission. Commission regulation (EC) No 1881/2006 of 19 December 2006 setting maximun levels for certain contaminants in foodstuffs. Off. J. Eur. Union 2006, 364, 5–24. [Google Scholar]
- European Parliament. European Parliament and the Council of the EU Directive of The European Parliament and of the Council of 7 May 2002 on undesirable substances in animal feed 2002/32. Off. J. Eur. Communities 2002, L140, 10–22. [Google Scholar]
- European Commission. Commission Recommendation of 17 August 2006 on the presence of deoxynivalenol, zearalenone, ochratoxin A, T-2 and HT-2 and fumonisins in products intended for animal feeding. Off. J. Eur. Union 2006, L299, 7–9. [Google Scholar]
- Eskola, M.; Kos, G.; Elliott, C.T.; Hajšlová, J.; Mayar, S.; Krska, R. Worldwide contamination of food-crops with mycotoxins: Validity of the widely cited ‘FAO estimate’ of 25%. Crit. Rev. Food Sci. Nutr. 2020, 60, 2773–2789. [Google Scholar] [CrossRef] [PubMed]
- Escrivá, L.; Font, G.; Manyes, L.; Berrada, H. Studies on the presence of mycotoxins in biological samples: An overview. Toxins (Basel) 2017, 9, 251. [Google Scholar] [CrossRef] [Green Version]
- Gurusankar, R.; Yenugadhati, N.; Krishnan, K.; Hays, S.; Haines, D.; Zidek, A.; Kuchta, S.; Kinniburgh, D.; Gabos, S.; Mattison, D.; et al. The role of human biological monitoring in health risk assessment. Int. J. Risk Assess. Manag. 2017, 20, 136–197. [Google Scholar] [CrossRef]
- Bredesen, D.E. Inhalational Alzheimer’s disease: An unrecognized—And treatable—Epidemic. Aging (Albany NY) 2016, 8, 304–313. [Google Scholar] [CrossRef]
- Martins, I. Overnutrition determines LPS regulation of mycotoxin induced neurotoxicity in neurodegenerative diseases. Int. J. Mol. Sci. 2015, 16, 29554–29573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izco, M.; Vettorazzi, A.; Forcen, R.; Blesa, J.; de Toro, M.; Alvarez-Herrera, N.; Cooper, J.M.; Gonzalez-Peñas, E.; Lopez de Cerain, A.; Alvarez-Erviti, L. Oral subchronic exposure to the mycotoxin ochratoxin A induces key pathological features of Parkinson’s disease in mice six months after the end of the treatment. Food Chem. Toxicol. 2021, 152, 112164. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research (FDA). Bioanalytical Method Validation Guidance for Industry. 2018. Available online: https://www.fda.gov/files/drugs/published/Bioanalytical-Method-Validation-Guidance-for-Industry.pdf (accessed on 20 November 2019).
- European Commission. Commission Decision of 12 August 2002 implementing Council Directive 96/23/EC concerning the performance of analytical methods and the interpretation of results (2002/657/EC). Off. J. Eur. Communities 2002, 221, 8–36. [Google Scholar]
- EFSA. Management of left-censored data in dietary exposure assessment of chemical substances. EFSA J. 2010, 8, 1–96. [Google Scholar]
- Arce-López, B.; Lizarraga, E.; Irigoyen, Á.; González-Peñas, E. Presence of 19 mycotoxins in human plasma in a region of Northern Spain. Toxins (Basel) 2020, 12, 750. [Google Scholar] [CrossRef]
- Arce-López, B.; Lizarraga, E.; Flores-Flores, M.; Irigoyen, Á.; González-Peñas, E. Development and validation of a methodology based on Captiva EMR-lipid clean-up and LC-MS/MS analysis for the simultaneous determination of mycotoxins in human plasma. Talanta 2020, 206, 120193. [Google Scholar] [CrossRef]
- Remiro, R.; González-Peñas, E.; Lizarraga, E.; López de Cerain, A. Quantification of ochratoxin A and five analogs in Navarra red wines. Food Control 2012, 27, 139–145. [Google Scholar] [CrossRef]
- Yang, S.; Zhang, H.; De Saeger, S.; De Boevre, M.; Sun, F.; Zhang, S.; Cao, X.; Wang, Z. In vitro and in vivo metabolism of ochratoxin A: A comparative study using ultra-performance liquid chromatography-quadrupole/time-of-flight hybrid mass spectrometry. Anal. Bioanal. Chem. 2015, 407, 3579–3589. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, K.; Cramer, B.; Dopstadt, J.; Humpf, H.U.; Degen, G.H. Evidence of ochratoxin A conjugates in urine samples from infants and adults. Mycotoxin Res. 2017, 33, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Vidal, A.; Mengelers, M.; Yang, S.; De Saeger, S.; De Boevre, M. Mycotoxin Biomarkers of Exposure: A Comprehensive Review. Compr. Rev. Food Sci. Food Saf. 2018, 17, 1127–1155. [Google Scholar] [CrossRef] [Green Version]
- EFSA CONTAM Panel (EFSA Panel on Contaminants in the Food Chain); Schrenk, D.; Bodin, L.; Chipman, J.K.; del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Hoogenboom, L.; Leblanc, J.; Nebbia, C.S.; et al. Risk assessment of ochratoxin A in food. EFSA J. 2020, 18, 06113. [Google Scholar]
- Arce-López, B.; Lizarraga, E.; Vettorazzi, A.; González-Peñas, E. Human biomonitoring of mycotoxins in blood, plasma and serum in recent years: A review. Toxins (Basel) 2020, 12, 147. [Google Scholar] [CrossRef] [Green Version]
- De Santis, B.; Raggi, M.E.; Moretti, G.; Facchiano, F.; Mezzelani, A.; Villa, L.; Bonfanti, A.; Campioni, A.; Rossi, S.; Camposeo, S.; et al. Study on the association among mycotoxins and other variables in children with autism. Toxins (Basel) 2017, 9, 203. [Google Scholar] [CrossRef]
- De Santis, B.; Brera, C.; Mezzelani, A.; Soricelli, S.; Ciceri, F.; Moretti, G.; Debegnach, F.; Bonaglia, M.C.; Villa, L.; Molteni, M.; et al. Role of mycotoxins in the pathobiology of autism: A first evidence. Nutr. Neurosci. 2019, 22, 132–144. [Google Scholar] [CrossRef]
- Arce-López, B.; Lizarraga, E.; López de Mesa, R.; González-Peñas, E. Assessment of exposure to mycotoxins in Spanish children through the analysis of their levels in plasma samples. Toxins (Basel) 2021, 13, 150. [Google Scholar] [CrossRef] [PubMed]
- Soto, J.B.; Ruiz, M.-J.; Manyes, L.; Juan-García, A. Blood, breast milk and urine: Potential biomarkers of exposure and estimated daily intake of ochratoxin A: A review. Food Addit. Contam. Part A 2015, 33, 313–328. [Google Scholar] [CrossRef]
- Warensjö Lemming, E.; Montano Montes, A.; Schmidt, J.; Cramer, B.; Humpf, H.-U.; Moraeus, L.; Olsen, M. Mycotoxins in blood and urine of Swedish adolescents—Possible associations to food intake and other background characteristics. Mycotoxin Res. 2020, 36, 193–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coronel, M.B.; Sanchis, V.; Ramos, A.J.; Marin, S. Ochratoxin A in adult population of Lleida, Spain: Presence in blood plasma and consumption in different regions and seasons. Food Chem. Toxicol. 2011, 49, 2697–2705. [Google Scholar] [CrossRef] [PubMed]
- Wilcoxon, F. Individual Comparisons by Ranking Methods. Biometrics 1945, 1, 80–83. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of ranks in one-criterion variance analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups/ Sub Groups | Disease Stage | N° of Subjects (M/W *) | Age Range (Years) |
|---|---|---|---|
| Subjects | 93 (43/50) | 43–85 | |
| Control (CNT) | 25 (8/17) | 43–81 | |
| Patients | 68 (35/33) | 44–85 | |
| PD | 44 (29/15) | 44–85 | |
| PD sub-group 1. | HY scale: 1–2 | 35 (23/12) | 44–85 |
| PD sub-group 2 | HY scale: 2.5–3 | 9 (6/3) | 62–83 |
| AD | GDS scale 3–7 | 24 (6/18) | 60–85 |
| Before Enzymatic Treatment | After Enzymatic Treatment | |||
|---|---|---|---|---|
| OTA | OTB | OTA | STER | |
| Total population | ||||
| Positive samples (N/%) | 72 (77%) | 12 (13%) | 66 (89%) | 65 (88%) |
| Mean value (M/W); ng/mL | 1.77 (2.10/1.50) | 0.07 (0.10/0.04) | 2.00 (1.86/2.10) | 0.81 (0.78/0.84) |
| Median (M/W); ng/mL | 1.65 (1.92/1.47) | 0 (0/0) | 1.68 (1.52/1.93) | 0.87 (0.86/0.88) |
| Range (min-max); ng/mL | 0–8.81 | 0–0.75 | 0–6.45 | 0–2.20 |
| Control (CNT) | ||||
| Positive samples (N/%) | 23 (92%) | 6 (24%) | 19 (86%) | 16 (73%) |
| Mean value (M/W); ng/mL | 2.15 (2.47/1.99) | 0.12 (0.22/0.07) | 2.51 (2.11/2.69) | 0.51 (0.53/0.51) |
| Median (M/W); ng/mL | 1.56 (2.19/1.50) | 0 (0.22/0) | 2.35 (2.01/2.41) | 0.65 (0.69/0.63) |
| Range (min-max); ng/mL | 0–8.81 | 0–0.75 | 0–6.25 | 0–0.90 |
| Patients | ||||
| Positive samples (N/%) | 49 (72%) | 6 (9%) | 47 (90%) | 49 (94%) |
| Mean value (M/W); ng/mL | 1.64 (2.01/1.24) | 0.05 (0.07/0.02) | 1.78 (1.79/1.76) | 0.94 (0.84/1.02) |
| Median (M/W); ng/mL | 1.66 (1.92/1.45) | 0 (0/0) | 1.46 (1.46/1.43) | 0.94 (0.87/0.97) |
| Range (min-max); ng/mL | 0–6.44 | 0–0.71 | 0–6.45 | 0–2.22 |
| Patients with PD | ||||
| Positive samples (N/%) | 33 (75%) | 6 (14%) | 31 (91%) | 31 (91%) |
| Mean value (M/W); ng/mL | 1.93 (2.13/1.54) | 0.07 (0.09/0.05) | 1.88 (1.82/1.99) | 0.90 (0.82/1.04) |
| Median (M/W); ng/mL | 1.86 (1.98/1.50) | 0 (0/0) | 1.53 (1.41/1.61) | 0.95 (0.87/1.02) |
| Range (min-max); ng/mL | 0–6.44 | 0–0.71 | 0–6.45 | 0–1.31 |
| Patients with AD | ||||
| Positive samples (N/%) | 16 (67%) | 0 (0%) | 16 (89%) | 18 (100%) |
| Mean value (M/W); ng/mL | 1.11 (1.47/0.99) | 0 (0/0) | 1.59 (1.64/1.57) | 1.01 (0.98/1.02) |
| Median (M/W); ng/mL | 1.46 (1.75/1.45) | 0 (0/0) | 1.39 (1.96/1.37) | 0.91 (0.92/0.91) |
| Range (min-max); ng/mL | 0–2.11 | 0 | 0–3.94 | 0.74–2.20 |
| OTA | STER | |
|---|---|---|
| CNT/patient group (PD + AD) | - | <0.0001 |
| CNT/PD/AD | 0.0447 | 0.0001 |
| CNT/PD | - | <0.0001 |
| CNT/AD | - | <0.0001 |
| PD/AD | 0.0114 | - |
| M/W | 0.0014 | - |
| M/W in patient group (PD + AD) | 0.0013 | - |
| M/W in patient group PD | (0.0613) | 0.0304 |
| Sex = M in CNT/PD/AD | - | 0.0128 |
| Sex = M in CNT/patient group (PD + AD) | - | 0.0047 |
| Sex = M in CNT/PD | - | 0.0105 |
| Sex = M in CNT/AD | - | 0.0080 |
| Sex = W in CNT/PD/AD | - | 0.0001 |
| Sex = W in CNT/patient group (PD + AD) | - | 0.0001 |
| Sex = W in CNT/PD | - | <0.0001 |
| Sex = W in CNT/AD | - | <0.0001 |
| OTA | STER | |||||
|---|---|---|---|---|---|---|
| rho | p-Value | N° Observations | rho | p-Value | N° Observations | |
| Age | −0.2033 | 0.0507 | 93 | 0.2686 | 0.0207 | 74 |
| Age in PD | −0.3304 | 0.0285 | 44 | - | - | - |
| Age in men | −0.3775 | 0.0126 | 43 | - | - | - |
| Age in women | - | - | - | 0.3384 | 0.0305 | 41 |
| Age in PD men | −0.4643 | 0.0122 | 29 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arce-López, B.; Alvarez-Erviti, L.; De Santis, B.; Izco, M.; López-Calvo, S.; Marzo-Sola, M.E.; Debegnach, F.; Lizarraga, E.; López de Cerain, A.; González-Peñas, E.; et al. Biomonitoring of Mycotoxins in Plasma of Patients with Alzheimer’s and Parkinson’s Disease. Toxins 2021, 13, 477. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070477
Arce-López B, Alvarez-Erviti L, De Santis B, Izco M, López-Calvo S, Marzo-Sola ME, Debegnach F, Lizarraga E, López de Cerain A, González-Peñas E, et al. Biomonitoring of Mycotoxins in Plasma of Patients with Alzheimer’s and Parkinson’s Disease. Toxins. 2021; 13(7):477. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070477
Chicago/Turabian StyleArce-López, Beatriz, Lydia Alvarez-Erviti, Barbara De Santis, María Izco, Silvia López-Calvo, Maria Eugenia Marzo-Sola, Francesca Debegnach, Elena Lizarraga, Adela López de Cerain, Elena González-Peñas, and et al. 2021. "Biomonitoring of Mycotoxins in Plasma of Patients with Alzheimer’s and Parkinson’s Disease" Toxins 13, no. 7: 477. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070477