Effect of Botulinum Toxin on Non-Motor Symptoms in Cervical Dystonia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. BoNT-A Treatment Parameters
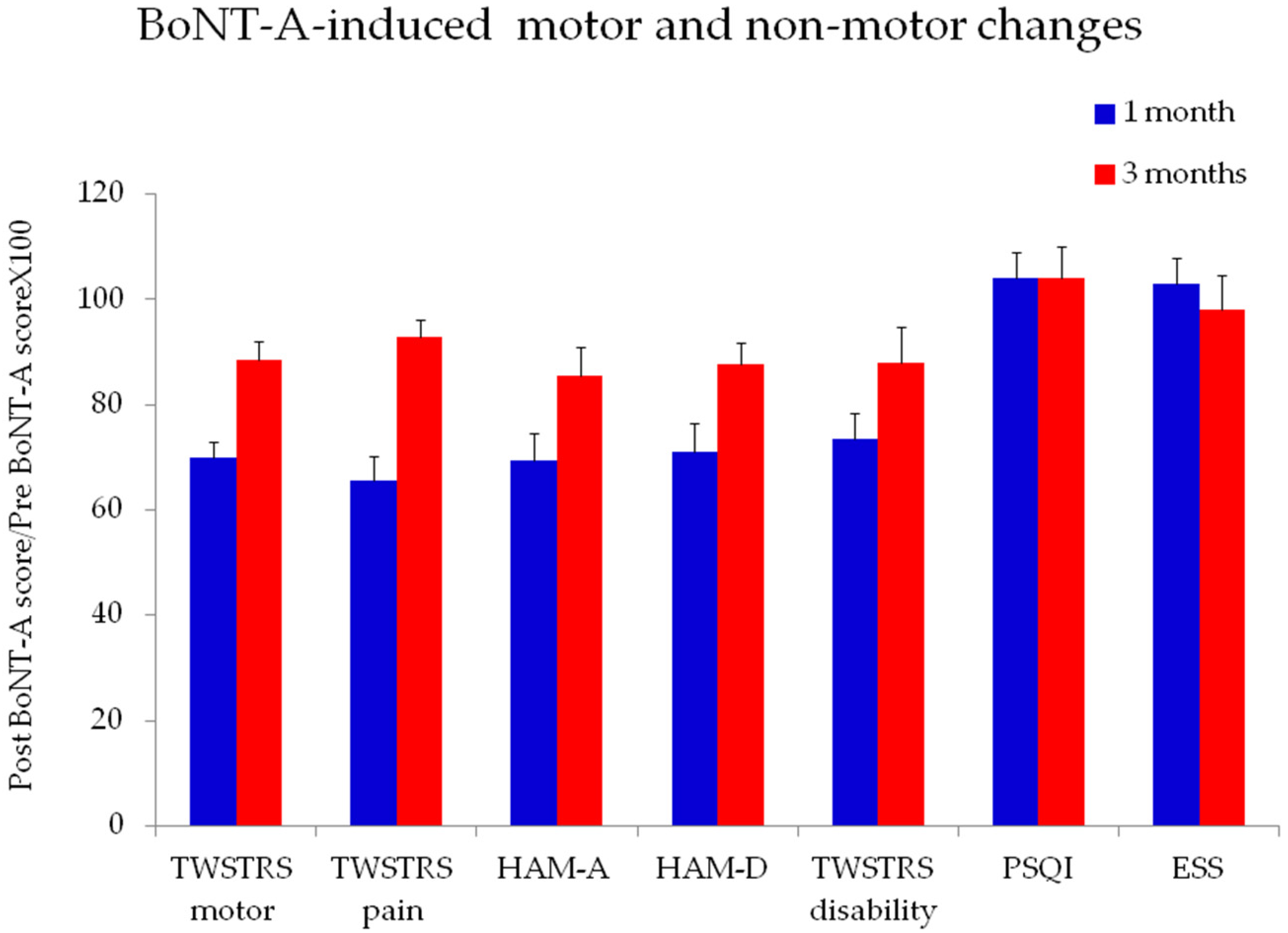
2.2. Effects of BoNT-A on Motor and Non-Motor Symptoms in Patients with CD
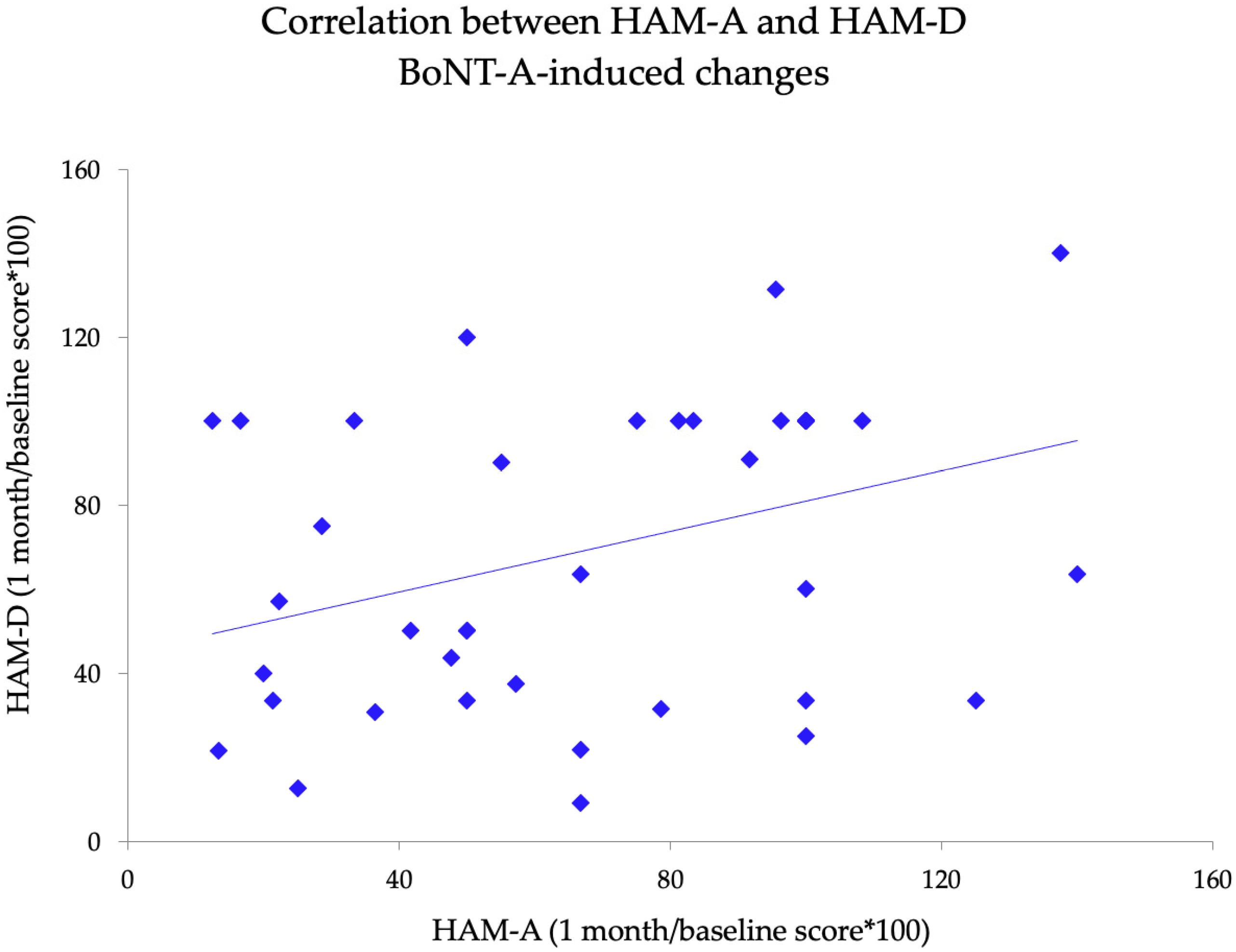
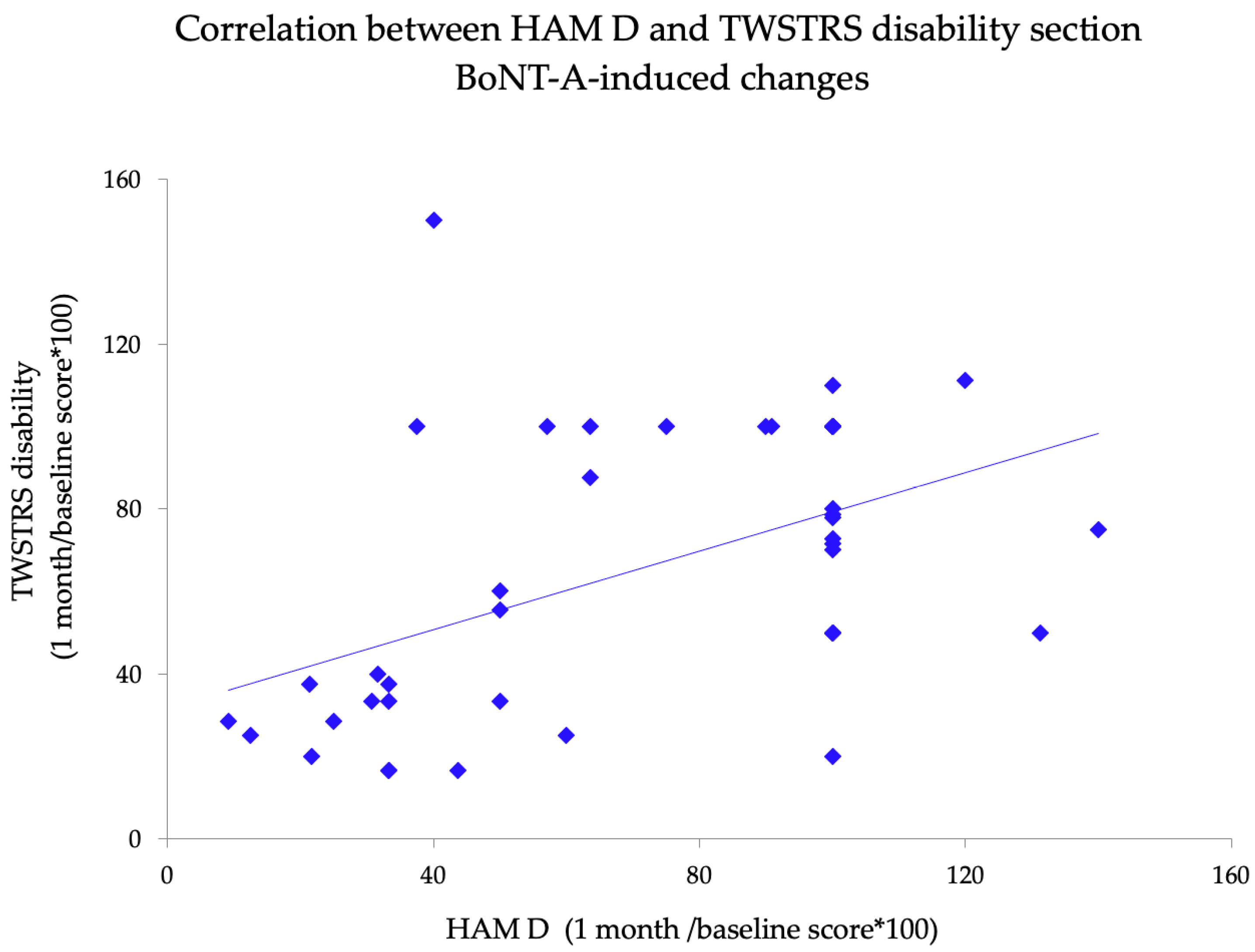
2.3. Relationship between Motor and Non-Motor BoNT-A-Induced Changes
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Participants and Ethics
5.2. Motor and Non-Motor Assessment
5.3. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jinnah, H.A.; Berardelli, A.; Comella, C.; Defazio, G.; Delong, M.R.; Factor, S.; Galpern, W.R.; Hallett, M.; Ludlow, C.L.; Perlmutter, J.S.; et al. The focal dystonias: Current views and challenges for future research. Mov. Disord. 2013, 28, 926–943. [Google Scholar] [CrossRef]
- Chan, J.; Brin, M.F.; Fahn, S. Idiopathic cervical dystonia: Clinical characteristics. Mov. Disord. 1991, 6, 119–126. [Google Scholar] [CrossRef]
- Dauer, W.T.; Burke, R.E.; Greene, P.; Fahn, S. Current concepts on the clinical features, aetiology and management of idiopathic cervical dystonia. Brain 1998, 121, 547–560. [Google Scholar] [CrossRef] [Green Version]
- Reichel, G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia 2011, 1, 5–12. [Google Scholar] [CrossRef]
- Jankovic, J.; Leder, S.; Warner, D.; Schwartz, K. Cervical dystonia: Clinical findings and associated movement disorders. Neurology 1991, 41, 1088. [Google Scholar] [CrossRef]
- Erro, R.; Rubio-Agusti, I.; Saifee, T.A.; Cordivari, C.; Ganos, C.; Batla, A.; Bhatia, K.P. Rest and other types of tremor in adult-onset primary dystonia. J. Neurol. Neurosurg. Psychiatry 2014, 85, 965–968. [Google Scholar] [CrossRef] [Green Version]
- Defazio, G.; Gigante, A.F.; Abbruzzese, G.; Bentivoglio, A.R.; Colosimo, C.; Esposito, M.; Fabbrini, G.; Guidubaldi, A.; Girlanda, P.; Liguori, R.; et al. Tremor in primary adult-onset dystonia: Prevalence and associated clinical features. J. Neurol. Neurosurg. Psychiatry 2013, 84, 404–408. [Google Scholar] [CrossRef]
- Defazio, G.; Conte, A.; Gigante, A.F.; Fabbrini, G.; Berardelli, A. Is tremor in dystonia a phenotypic feature of dystonia? Neurology 2015, 84, 1053–1059. [Google Scholar] [CrossRef]
- Berardelli, I.; Ferrazzano, G.; Pasquini, M.; Biondi, M.; Berardelli, A.; Fabbrini, G. Clinical course of psychiatric disorders in patients with cervical dystonia. Psychiatry Res. 2015, 229, 583–585. [Google Scholar] [CrossRef]
- Gündel, H.; Wolf, A.; Xidara, V.; Busch, R.; Ladwig, K.H.; Jacobi, F.; von Rad, M.; Ceballos-Baumann, A.O. High psychiatric comorbidity in spasmodic torticollis: A controlled study. J. Nerv. Ment. Dis. 2003, 191, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Moraru, E.; Schnider, P.; Wimmer, A.; Wenzel, T.; Birner, P.; Griengl, H.; Auff, E. Relation between depression and anxiety in dystonic patients: Implications for clinical management. Depress. Anxiety 2002, 16, 100–103. [Google Scholar] [CrossRef]
- Lencer, R.; Steinlechner, S.; Stahlberg, J.; Rehling, H.; Orth, M.; Baeumer, T.; Rumpf, H.J.; Meyer, C.; Klein, C.; Muenchau, A.; et al. Primary focal dystonia: Evidence for distinct neuropsychiatric and personality profiles. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1176–1179. [Google Scholar] [CrossRef] [Green Version]
- Fabbrini, G.; Berardelli, I.; Moretti, G.; Pasquini, M.; Bloise, M.; Colosimo, C.; Biondi, M.; Berardelli, A. Psychiatric disorders in adult-onset focal dystonia: A case-control study. Mov. Disord. 2010, 25, 459–465. [Google Scholar] [CrossRef]
- Trotti, L.M.; Esper, C.D.; Feustel, P.J.; Bliwise, D.L.; Factor, S.A. Excessive daytime sleepiness in cervical dystonia. Parkinsonism Relat. Disord. 2009, 15, 784–786. [Google Scholar] [CrossRef] [PubMed]
- Paus, S.; Gross, J.; Moll-Müller, M.; Hentschel, F.; Spottke, A.; Wabbels, B.; Klockgether, T.; Abele, M. Impaired sleep quality and restless legs syndrome in idiopathic focal dystonia: A controlled study. J. Neurol. 2011, 258, 1835–1840. [Google Scholar] [CrossRef]
- Avanzino, L.; Martino, D.; Marchese, R.; Aniello, M.S.; Minafra, B.; Superbo, M.; Defazio, G.; Abbruzzese, G. Quality of sleep in primary focal dystonia: A case-control study. Eur. J. Neurol. 2010, 17, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Tinazzi, M.; Fiorio, M.; Fiaschi, A.; Rothwell, J.C.; Bhatia, K.P. Sensory functions in dystonia: Insights from behavioral studies. Mov. Disord. 2009, 24, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Tinazzi, M.; Squintani, G.M.; Bhatia, K.P.; Segatti, A.; Donato, F.; Valeriani, M.; Erro, R. Pain in cervical dystonia: Evidence of abnormal inhibitory control. Parkinsonism Relat. Disord. 2019, 65, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Stamelou, M.; Edwards, M.J.; Hallett, M.; Bhatia, K.P. The non-motor syndrome of primary dystonia: Clinical and pathophysiological implications. Brain 2012, 135, 1668–1681. [Google Scholar] [CrossRef]
- Han, V.; Skorvanek, M.; Smit, M.; Turcanova Koprusakova, M.; Hoekstra, T.; van Dijk, J.P.; Tijssen, M.A.J.; Gdovinova, Z.; Reijneveld, S.A. Prevalence of non-motor symptoms and their association with quality of life in cervical dystonia. Acta Neurol. Scand. 2020, 142, 613–622. [Google Scholar] [CrossRef]
- Ortiz, R.M.; Scheperjans, F.; Mertsalmi, T.; Pekkonen, E. Comorbidity and retirement in cervical dystonia. J. Neurol. 2019, 266, 2216–2223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costanzo, M.; Belvisi, D.; Berardelli, I.; Maraone, A.; D’Antonio, F.; Baione, V.; Toscano, A.; Ferrazzano, G.; Pasquini, M.; Conte, A.; et al. Motor and non-motor subtypes of cervical dystonia. Parkinsonism Relat. Disord. 2021, 88, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Zurowski, M.; McDonald, W.M.; Fox, S.; Marsh, L. Psychiatric comorbidities in dystonia: Emerging concepts. Mov. Disord. 2013, 28, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, F.B.; Duarte, G.S.; Marques, R.E.; Castelão, M.; Ferreira, J.; Sampaio, C.; Moore, A.P.; Costa, J. Botulinum toxin type A therapy for cervical dystonia. Cochrane Database Syst. Rev. 2020, 11, CD003633. [Google Scholar] [CrossRef]
- Schiavo, G.; Matteoli, M.; Montecucco, C. Neurotoxins Affecting Neuroexocytosis. Physiol. Rev. 2000, 80, 717–766. [Google Scholar] [CrossRef]
- Caleo, M.; Restani, L. Direct central nervous system effects of botulinum neurotoxin. Toxicon 2018, 147, 68–72. [Google Scholar] [CrossRef]
- Hok, P.; Veverka, T.; Hluštík, P.; Nevrlý, M.; Kaňovský, P. The Central Effects of Botulinum Toxin in Dystonia and Spasticity. Toxins 2021, 13, 155. [Google Scholar] [CrossRef]
- Curra, A.; Berardelli, A. Do the unintended actions of botulinum toxin at distant sites have clinical implications? Neurology 2009, 72, 1095–1099. [Google Scholar] [CrossRef]
- Bozzi, Y.; Costantin, L.; Antonucci, F.; Caleo, M. Action of botulinum neurotoxins in the central nervous system: Antiepileptic effects. Neurotox Res. 2006, 9, 197–203. [Google Scholar] [CrossRef]
- Eichenseer, S.R.; Stebbins, G.T.; Comella, C.L. Beyond a motor disorder: A prospective evaluation of sleep quality in cervical dystonia. Parkinsonism Relat. Disord. 2014, 20, 405–408. [Google Scholar] [CrossRef]
- Comella, C.L.; Jankovic, J.; Truong, D.D.; Hanschmann, A.; Grafe, S.; U.S. XEOMIN Cervical Dystonia Study Group. Efficacy and safety of incobotulinumtoxinA (NT 201, XEOMIN®, botulinum neurotoxin type A, without accessory proteins) in patients with cervical dystonia. J. Neurol. Sci. 2011, 308, 103–109. [Google Scholar] [CrossRef]
- Defazio, G.; Albanese, A.; Pellicciari, R.; Scaglione, C.L.; Esposito, M.; Morgante, F.; Abbruzzese, G.; Bentivoglio, A.R.; Bono, F.; Coletti Moja, M.; et al. Expert recommendations for diagnosing cervical, oromandibular, and limb dystonia. Neurol. Sci. 2019, 40, 89–95. [Google Scholar] [CrossRef]
- Albanese, A.; Bhatia, K.; Bressman, S.B.; Delong, M.R.; Fahn, S.; Fung, V.S.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and classification of dystonia: A consensus update. Mov. Disord. 2013, 28, 863–873. [Google Scholar] [CrossRef] [Green Version]
- Dong, H.; Fan, S.; Luo, Y.; Peng, B. Botulinum toxin relieves anxiety and depression in patients with hemifacial spasm and blepharospasm. Neuropsychiatr Dis Treat. 2018, 15, 33–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahanshahi, M.; Marsden, C.D. Depression in torticollis: A controlled study. Psychol. Med. 1988, 18, 925–933. [Google Scholar] [CrossRef]
- Jahanshahi, M.; Marsden, C.D. A Longitudinal Follow-up Study of Depression, Disability, and Body Concept in Torticollis. Behav. Neurol. 1990, 3, 233–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahanshahi, M.; Marsden, C.D. Body Concept, Disability, and Depression in Patients with Spasmodic Torticollis. Behav. Neurol. 1990, 3, 117–131. [Google Scholar] [CrossRef] [Green Version]
- Egger, K.; Mueller, J.; Schocke, M.; Brenneis, C.; Rinnerthaler, M.; Seppi, K.; Trieb, T.; Wenning, G.K.; Hallett, M.; Poewe, W. Voxel based morphometry reveals specific gray matter changes in primary dystonia. Mov. Disord. 2007, 22, 1538–1542. [Google Scholar] [CrossRef]
- Ceballos-Baumann, A.O.; Passingham, R.E.; Warner, T.; Playford, E.D.; Marsden, C.D.; Brooks, D.J. Overactive prefrontal and underactive motor cortical areas in idiopathic dystonia. Ann. Neurol. 1995, 37, 363–372. [Google Scholar] [CrossRef]
- Delnooz, C.C.; Pasman, J.W.; Beckmann, C.F.; van de Warrenburg, B.P. Task-free functional MRI in cervical dystonia reveals multi-network changes that partially normalize with botulinum toxin. PLoS ONE 2013, 8, e62877. [Google Scholar] [CrossRef] [Green Version]
- Opavský, R.; Hluštík, P.; Otruba, P.; Kaňovský, P. Sensorimotor network in cervical dystonia and the effect of botulinum toxin treatment: A functional MRI study. J. Neurol. Sci. 2011, 306, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Nevrlý, M.; Hluštík, P.; Hok, P.; Otruba, P.; Tüdös, Z.; Kaňovský, P. Changes in sensorimotor network activation after botulinum toxin type A injections in patients with cervical dystonia: A functional MRI study. Exp. Brain. Res. 2018, 236, 2627–2637. [Google Scholar] [CrossRef] [Green Version]
- Jinnah, H.A.; Neychev, V.; Hess, E.J. The Anatomical Basis for Dystonia: The Motor Network Model. Tremor Other Hyperkinet. Mov. 2017, 7, 506. [Google Scholar] [CrossRef]
- Corp, D.T.; Joutsa, J.; Darby, R.R.; Delnooz, C.C.S.; van de Warrenburg, B.P.C.; Cooke, D.; Prudente, C.N.; Ren, J.; Reich, M.M.; Batla, A.; et al. Network localization of cervical dystonia based on causal brain lesions. Brain 2019, 142, 1660–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, A.G.; Zee, D.S.; Crawford, J.D.; Jinnah, H.A. Cervical dystonia: A neural integrator disorder. Brain 2016, 139, 2590–2599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camargo, C.; Cattai, L.; Teive, H.A. Pain Relief in Cervical Dystonia with Botulinum Toxin Treatment. Toxins 2015, 7, 2321–2335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marciniec, M.; Szczepańska-Szerej, A.; Kulczyński, M.; Sapko, K.; Popek-Marciniec, S.; Rejdak, K. Pain in cervical dystonia and the antinociceptive effects of botulinum toxin: What is currently known? Rev. Neurosci. 2019, 30, 771–779. [Google Scholar] [CrossRef]
- Velly, A.M.; Mohit, S. Epidemiology of pain and relation to psychiatric disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 87, 159–167. [Google Scholar] [CrossRef]
- Brans, J.W.; Lindeboom, R.; Snoek, J.W.; Zwarts, M.J.; van Weerden, T.W.; Brunt, E.R.; van Hilten, J.J.; van der Kamp, W.; Prins, M.H.; Speelman, J.D. Botulinurn Toxin Versus Trihexyphenidyl in Cervical Dystonia: A Prospective, Randomized, Double-Blind Controlled Trial. Neurology 1996, 46, 1066–1072. [Google Scholar] [CrossRef]
- Van Den Dool, J.; Tijssen, M.A.; Koelman, J.H.; Engelbert, R.H.; Visser, B. Determinants of disability in cervical dystonia. Parkinsonism Relat. Disord. 2016, 32, 48–53. [Google Scholar] [CrossRef]
- Comella, C.L.; Fox, S.H.; Bhatia, K.P.; Perlmutter, J.S.; Jinnah, H.A.; Zurowski, M.; McDonald, W.M.; Marsh, L.; Rosen, A.R.; Waliczek, T.; et al. Development of the Comprehensive Cervical Dystonia Rating Scale: Methodology. Mov. Disord. Clin. Pract. 2015, 2, 135–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comella, C.L.; Perlmutter, J.S.; Jinnah, H.A.; Waliczek, T.A.; Rosen, A.R.; Galpern, W.R.; Adler, C.A.; Barbano, R.L.; Factor, S.A.; Goetz, C.G.; et al. Clinimetric testing of the comprehensive cervical dystonia rating scale: Comprehensive Cervical Dystonia Rating Scale. Mov. Disord. 2016, 31, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Trajković, G.; Starčević, V.; Latas, M.; Leštarević, M.; Ille, T.; Bukumirić, Z.; Marinković, J. Reliability of the Hamilton Rating Scale for Depression: A meta-analysis over a period of 49years. Psychiatry Res. 2011, 189, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurosurg. Psychiat. 1960, 23, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsh, W.A.; Monroe, D.M.; Brin, M.F.; Gallagher, C.J. Systematic review and meta-analysis of the duration of clinical effect of onabotulinumtoxinA in cervical dystonia. BMC Neurol. 2014, 14, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dressler, D.; Tacik, P.; Saberi, F.A. Botulinum toxin therapy of cervical dystonia: Duration of therapeutic effects. J. Neural. Transm. 2015, 122, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Wissel, J.; Kanovsky, P.; Ruzicka, E.; Bares, M.; Hortova, H.; Streitova, H.; Jech, R.; Roth, J.; Brenneis, C.; Müller, J.; et al. Efficacy and safety of a standardised 500 unit dose of Dysport (clostridium botulinum toxin type A haemaglutinin complex) in a heterogeneous cervical dystonia population: Results of a prospective, multicentre, randomised, double-blind, placebo-controlled, parallel group study. J. Neurol. 2001, 248, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Ferrazzano, G.; Berardelli, I.; Belvisi, D.; De Bartolo, M.I.; Di Vita, A.; Conte, A.; Fabbrini, G. Awareness of Dystonic Posture in Patients With Cervical Dystonia. Front. Psychol. 2020, 11, 1434. [Google Scholar] [CrossRef]
- Ferrazzano, G.; Conte, A.; Fabbrini, G.; Bologna, M.; Macerollo, A.; Defazio, G.; Hallett, M.; Berardelli, A. Botulinum toxin and blink rate in patients with blepharospasm and increased blinking. J. Neurol. Neurosurg. Psychiatry 2015, 86, 336–340. [Google Scholar] [CrossRef]
- Ferrazzano, G.; Berardelli, I.; Conte, A.; Baione, V.; Concolato, C.; Belvisi, D.; Fabbrini, G.; Defazio, G.; Berardelli, A. Motor and non-motor symptoms in blepharospasm: Clinical and pathophysiological implications. J. Neurol. 2019, 266, 2780–2785. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innamorati, M.; Pompili, M.; De Filippis, S.; Gentili, F.; Erbuto, D.; Lester, D.; Tamburello, A.; Iacorossi, G.; Cuomo, I.; Dominici, G.; et al. The validation of the Italian Perceived Disability Scale (IPDS) in chronic daily headache sufferers. J. Headache Pain 2009, 10, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berardelli, I.; Belvisi, D.; Corigliano, V.; Costanzo, M.; Innamorati, M.; Fabbrini, G.; Berardelli, A.; Pompili, M. Suicidal ideation, perceived disability, hopelessness and affective temperaments in patients affected by Parkinson's disease. Int. J. Clin. Pract. 2018, 19, e13287. [Google Scholar] [CrossRef]
- Belvisi, D.; Berardelli, I.; Ferrazzano, G.; Costanzo, M.; Corigliano, V.; Fabbrini, G.; Berardelli, A.; Pompili, M. The clinical correlates of suicidal ideation in Parkinson’s disease. Parkinsonism Relat Disord. 2019, 63, 54–59. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Demographic and Clinical Data | CD Patients |
|---|---|
| Females (%) | 62% |
| Age in years (mean ± SD) | 58.5 ± 12.8 |
| Disease duration in years (mean ± SD) | 10 ± 9.2 |
| Schooling (years ± SD) | 12.3 ± 3.5 |
| Right-handed (%) | 97% |
| Motor domain | |
| Tremor (%) | 31% |
| TWSTRS severity Section 1 (mean ± SD) | 11.5 ± 3.4 |
| Psychiatric domain | |
| TWSTRS psychiatric Section 1 (mean ± SD) | 5 ± 4.2 |
| HAM-A 2 (mean ± SD) | 9 ± 7.8 |
| HAM-D 3 (mean ± SD) | 8.3 ± 7.2 |
| Sleep domain | |
| PSQI 4 (mean ± SD) | 5.1 ± 3.7 |
| ESS 5(mean ± SD) | 4.1 ± 4.1 |
| Pain domain | |
| TWSTRS pain Section 1 (mean ± SD) | 14.6 ± 10.2 |
| Disability domain | |
| TWSTRS disability Section 1 (mean ± SD) | 6.8 ± 5.5 |
| IPDS 6 (mean ± SD) | 31.5 ± 16.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costanzo, M.; Belvisi, D.; Berardelli, I.; Maraone, A.; Baione, V.; Ferrazzano, G.; Cutrona, C.; Leodori, G.; Pasquini, M.; Conte, A.; et al. Effect of Botulinum Toxin on Non-Motor Symptoms in Cervical Dystonia. Toxins 2021, 13, 647. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13090647
Costanzo M, Belvisi D, Berardelli I, Maraone A, Baione V, Ferrazzano G, Cutrona C, Leodori G, Pasquini M, Conte A, et al. Effect of Botulinum Toxin on Non-Motor Symptoms in Cervical Dystonia. Toxins. 2021; 13(9):647. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13090647
Chicago/Turabian StyleCostanzo, Matteo, Daniele Belvisi, Isabella Berardelli, Annalisa Maraone, Viola Baione, Gina Ferrazzano, Carolina Cutrona, Giorgio Leodori, Massimo Pasquini, Antonella Conte, and et al. 2021. "Effect of Botulinum Toxin on Non-Motor Symptoms in Cervical Dystonia" Toxins 13, no. 9: 647. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13090647