Feasibility of Video Clip Analysis on Effect of Botulinum Toxin-A Injection for Post-Stroke Upper Limb Spasticity


Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Botox Injection
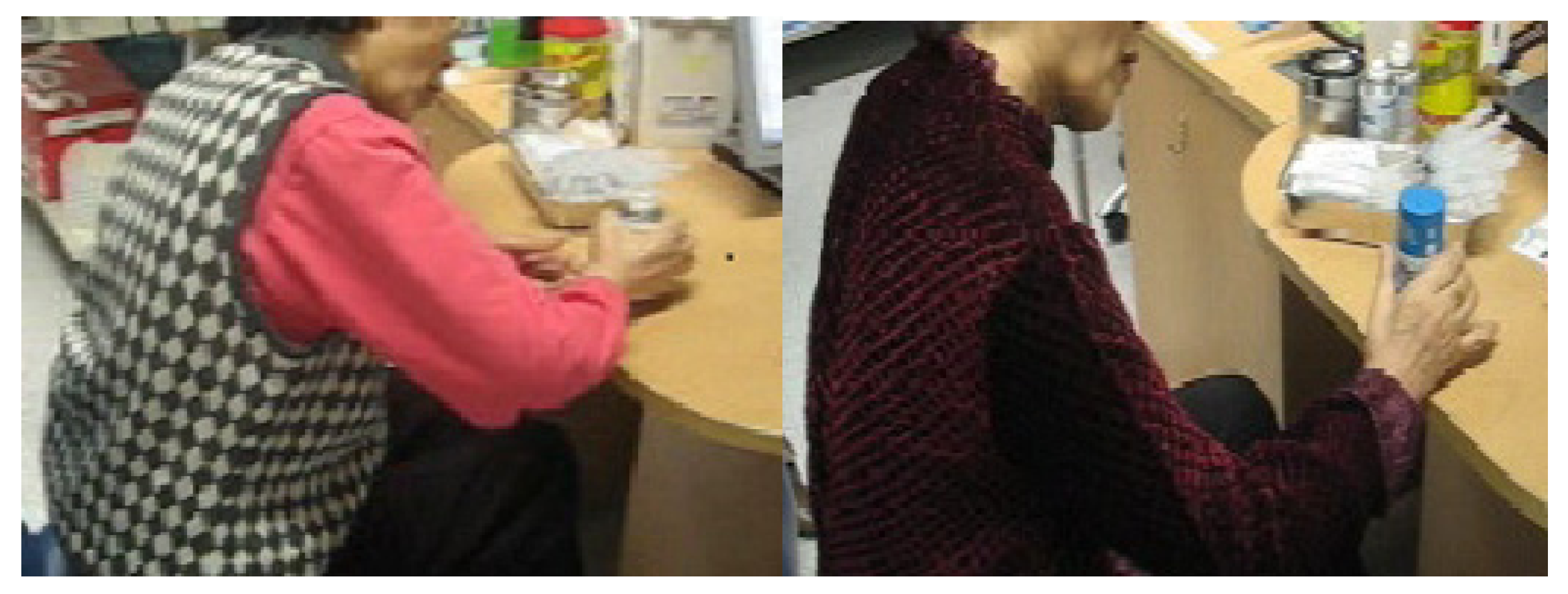
2.3. Functional Measures and Video Analysis

2.4. Statistics
3. Results

{kind=link}
| Pre | Post | p Value | |
|---|---|---|---|
| Age (years) | 60 ± 17 | ||
| M:F | 55:24 | ||
| Time from stroke onset to BTX-A injection (weeks) | 11 ± 9 | ||
| mRS | 4 | 3.5 | 0.335 |
| B stage (arm) | 2.83 | 3.39 | 0.144 |
| B stage (hand) | 2.43 | 3.08 | 0.036 |
| MAS | 2 | 1.58 | 0.011 |
| FMA (affected) | 17.3 | 23 | 0.161 |
| FMA (unaffected) | 52.6 | 61.6 | 0.116 |
| MBI | 26 | 57.1 | 0.335 |
Validity and Reliability Analysis
| Physician A | Physician B | Physician C | |
|---|---|---|---|
| Hand motion | 82.3% | 79.7% | 72.2% |
| Gait associated hand posture | 73.4% | 70.9% | 70.9% |
| kappa | ICC | Overall agreement (%) | |
|---|---|---|---|
| Hand motion | 0.86 | 0.79 | 78.1 |
| Gait associated hand posture | 0.92 | 0.92 | 71.7 |
4. Discussion
5. Conclusions
Acknowledgment
References
- Lundstrom, E.; Terent, A.; Borg, J. Prevalence of disabling spasticity 1 year after first-ever stroke. Eur. J. Neurol. 2008, 15, 533–539. [Google Scholar] [CrossRef]
- Elovic, E.P.; Brashear, A.; Kaelin, D.; Liu, J.; Millis, S.R.; Barron, R.; Turkel, C. Repeated treatments with botulinum toxin type a produce sustained decreases in the limitations associated with focal upper-limb poststroke spasticity for caregivers and patients. Arch. Phys. Med. Rehabil. 2008, 89, 799–806. [Google Scholar] [CrossRef]
- Ozcakir, S.; Sivrioglu, K. Botulinum toxin in poststroke spasticity. Clin. Med. Res. 2007, 5, 132–138. [Google Scholar] [CrossRef]
- Kamper, D.G.; Schmit, B.D.; Rymer, W.Z. Effect of muscle biomechanics on the quantification of spasticity. Ann. Biomed. Eng. 2001, 29, 1122–1134. [Google Scholar] [CrossRef]
- Lee, H.M.; Chen, J.J.; Wu, Y.N.; Wang, Y.L.; Huang, S.C.; Piotrkiewicz, M. Time course analysis of the effects of botulinum toxin type a on elbow spasticity based on biomechanic and electromyographic parameters. Arch. Phys. Med. Rehabil. 2008, 89, 692–699. [Google Scholar]
- Foran, J.R.; Steinman, S.; Barash, I.; Chambers, H.G.; Lieber, R.L. Structural and mechanical alterations in spastic skeletal muscle. Dev. Med. Child Neurol. 2005, 47, 713–717. [Google Scholar] [CrossRef]
- Lee, H.M.; Huang, Y.Z.; Chen, J.J.; Hwang, I.S. Quantitative analysis of the velocity related pathophysiology of spasticity and rigidity in the elbow flexors. J. Neurol. Neurosurg. Psychiatry 2002, 72, 621–629. [Google Scholar] [CrossRef]
- Ward, A.; Roberts, G.; Warner, J.; Gillard, S. Cost-effectiveness of botulinum toxin type a in the treatment of post-stroke spasticity. J. Rehabil. Med. 2005, 37, 252–257. [Google Scholar] [CrossRef]
- Platz, T.; Eickhof, C.; Nuyens, G.; Vuadens, P. Clinical scales for the assessment of spasticity, associated phenomena, and function: A systematic review of the literature. Disabil. Rehabil. 2005, 27, 7–18. [Google Scholar] [CrossRef]
- Johnson, G.R. Outcome measures of spasticity. Eur. J. Neurol. 2002, 9, 53–61. [Google Scholar] [CrossRef]
- Ashford, S.; Turner-Stokes, L. Goal attainment for spasticity management using botulinum toxin. Physiother. Res. Int. 2006, 11, 24–34. [Google Scholar] [CrossRef]
- Turner-Stokes, L.; Baguley, I.J.; de Graaff, S.; Katrak, P.; Davies, L.; McCrory, P.; Hughes, A. Goal attainment scaling in the evaluation of treatment of upper limb spasticity with botulinum toxin: A secondary analysis from a double-blind placebo-controlled randomized clinical trial. J. Rehabil. Med. 2010, 42, 81–89. [Google Scholar] [CrossRef]
- Turner-Stokes, L.; Williams, H.; Johnson, J. Goal attainment scaling: Does it provide added value as a person-centred measure for evaluation of outcome in neurorehabilitation following acquired brain injury? J. Rehabil. Med. 2009, 41, 528–535. [Google Scholar] [CrossRef]
- Van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef]
- Van Deusen, J.; Harlowe, D. Continued construct validation of the St. Marys CVA evaluation: Brunnstrom arm and hand stage ratings. Am. J. Occup. Ther. 1986, 40, 561–563. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- Witwer, A.N.; Lecavalier, L.; Norris, M. Reliability and validity of the Children’s interview for psychiatric syndromes-parent version in autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 1949–1958. [Google Scholar] [CrossRef]
- Rosales, R.L.; Chua-Yap, A.S. Evidence-based systematic review on the efficacy and safety of botulinum toxin-A therapy in post-stroke spasticity. J. Neural Transm. 2008, 115, 617–623. [Google Scholar] [CrossRef]
- Francis, H.; Wade, D.; Turner-Stokes, L.; Kingswell, R.; Dott, C.; Coxon, E. Does reducing spasticity translate into functional benefit? An exploratory meta-analysis. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1547–1551. [Google Scholar] [CrossRef]
- Hurn, J.; Kneebone, I.; Cropley, M. Goal setting as an outcome measure: A systematic review. Clin. Rehabil. 2006, 20, 756–772. [Google Scholar] [CrossRef]
- Mailloux, Z.; May-Benson, T.A.; Summers, C.A.; Miller, L.J.; Brett-Green, B.; Burke, J.P.; Cohn, E.S.; Koomar, J.A.; Parham, L.D.; Roley, S.S.; et al. Goal attainment scaling as a measure of meaningful outcomes for children with sensory integration disorders. Am. J. Occup. Ther. 2007, 61, 254–259. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kim, W.-J.; Kumthornthip, W.; Oh, B.M.; Yang, E.J.; Paik, N.-J. Feasibility of Video Clip Analysis on Effect of Botulinum Toxin-A Injection for Post-Stroke Upper Limb Spasticity. Toxins 2013, 5, 983-991. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins5050983
Kim W-J, Kumthornthip W, Oh BM, Yang EJ, Paik N-J. Feasibility of Video Clip Analysis on Effect of Botulinum Toxin-A Injection for Post-Stroke Upper Limb Spasticity. Toxins. 2013; 5(5):983-991. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins5050983
Chicago/Turabian StyleKim, Woo-Jin, Witsanu Kumthornthip, Byung Mo Oh, Eun Joo Yang, and Nam-Jong Paik. 2013. "Feasibility of Video Clip Analysis on Effect of Botulinum Toxin-A Injection for Post-Stroke Upper Limb Spasticity" Toxins 5, no. 5: 983-991. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins5050983