
Acupoint Injection of Onabotulinumtoxin A for Migraines

Abstract
:1. Introduction
2. Results and Discussion
2.1. Subjects’ Characteristics

{kind=link}
{kind=link}
| Group | Case (n) | Gender M/F (n) | Age (y) | Weight (kg) | Stature (cm) | Duration of Migraine (y) | |
|---|---|---|---|---|---|---|---|
| Placebo | 19 | 4/15 | 41.7 ± 8.8 | 58.7 ± 5.8 | 159.1 ± 7.4 | 6.8 ± 2.6 | |
| BoNTA | Fixed-sites | 41 | 8/33 | 39.8 ± 9.2 | 57.4 ± 7.1 | 158.3 ± 7.5 | 5.0 ± 2.9 |
| Acupoint-sites | 42 | 9/33 | 41.0 ± 9.1 | 59.7 ± 6.6 | 160.9 ± 7.0 | 6.1 ± 3.6 | |
| Total | 102 | 21/81 | 40.7 ± 9.0 | 58.6 ± 6.7 | 159.5 ± 7.3 | 6.0 ± 3.6 | |
2.2. Effect of BoNTA Injection on the Attack Frequency, Intensity, Duration and Associated Symptoms of Migraines
| Group | Baseline | Post-Injection (Month) | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| Placebo | 7.5 ± 2.0 | 7.4 ± 3.2 | 7.1 ± 3.3 | 7.2 ± 3.0 | 7.4 ± 2.8 | |
| BoNTA | Fixed-sites | 7.2 ± 1.7 | 4.0 ± 1.4 * | 3.8 ± 1.6 * | 3.6 ± 1.4 * | 3.7 ± 1.3 * |
| Acupoint-sites | 7.6 ± 2.1 | 2.1 ± 1.0 *,† | 1.8 ± 0.9 *,† | 1.7 ± 0.8 *,† | 1.9 ± 1.0 *,† | |
| Group | Baseline | Post-Injection (Month) | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| Placebo | 6.9 ± 1.9 | 6.6 ± 2.1 | 6.1 ± 2.3 | 6.3 ± 2.2 | 6.4 ± 2.1 | |
| BoNTA | Fixed-sites | 6.8 ± 1.6 | 4.2 ± 1.4 * | 4.0 ± 1.3 * | 3.8 ± 1.5 * | 4.0 ± 1.4 * |
| Acupoint-sites | 7.0 ± 1.5 | 2.1 ± 1.0 *† | 1.9 ± 0.9 *,† | 1.8 ± 0.8 *,† | 2.0 ± 0.9 *,† | |
| Group | Baseline | Post-Injection (Month) | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| Placebo | 7.4 ± 2.1 | 7.3 ± 2.5 | 7.1 ± 2.6 | 7.2 ± 2.4 | 7.2 ± 2.2 | |
| BoNTA | Fixed-sites | 7.0 ± 2.4 | 3.8 ± 1.2 * | 3.1 ± 1.3 * | 3.0 ± 1.2 * | 3.5 ± 1.4 * |
| Acupoint-sites | 7.9 ± 2.6 | 2.0 ± 0.9 *,† | 1.5 ± 0.7 *,† | 1.4 ± 0.7 *,† | 1.6 ± 0.7 *,† | |
| Group | Baseline | Post-Injection (Month) | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| Placebo | 0.72 ± 0.20 | 0.71 ± 0.22 | 0.68 ± 0.21 | 0.69 ± 0.23 | 0.68 ± 0.21 | |
| BoNTA | Fixed-sites | 0.74 ± 0.21 | 0.36 ± 0.14 * | 0.33 ± 0.15 * | 0.31 ± 0.14 * | 0.34 ± 0.15 * |
| Acupoint-sites | 0.69 ± 0.23 | 0.18 ± 0.09 *,† | 0.16 ± 0.09 *,† | 0.15 ± 0.08 *,† | 0.18 ± 0.07 *,† | |
2.3. Efficiency of Fixed-Sites and Acupiont-Sites Injection of BoNTA
2.4. Side Effects
2.5. Discussion
3. Experimental Section
3.1. Study Design
3.2. Participant Characteristics
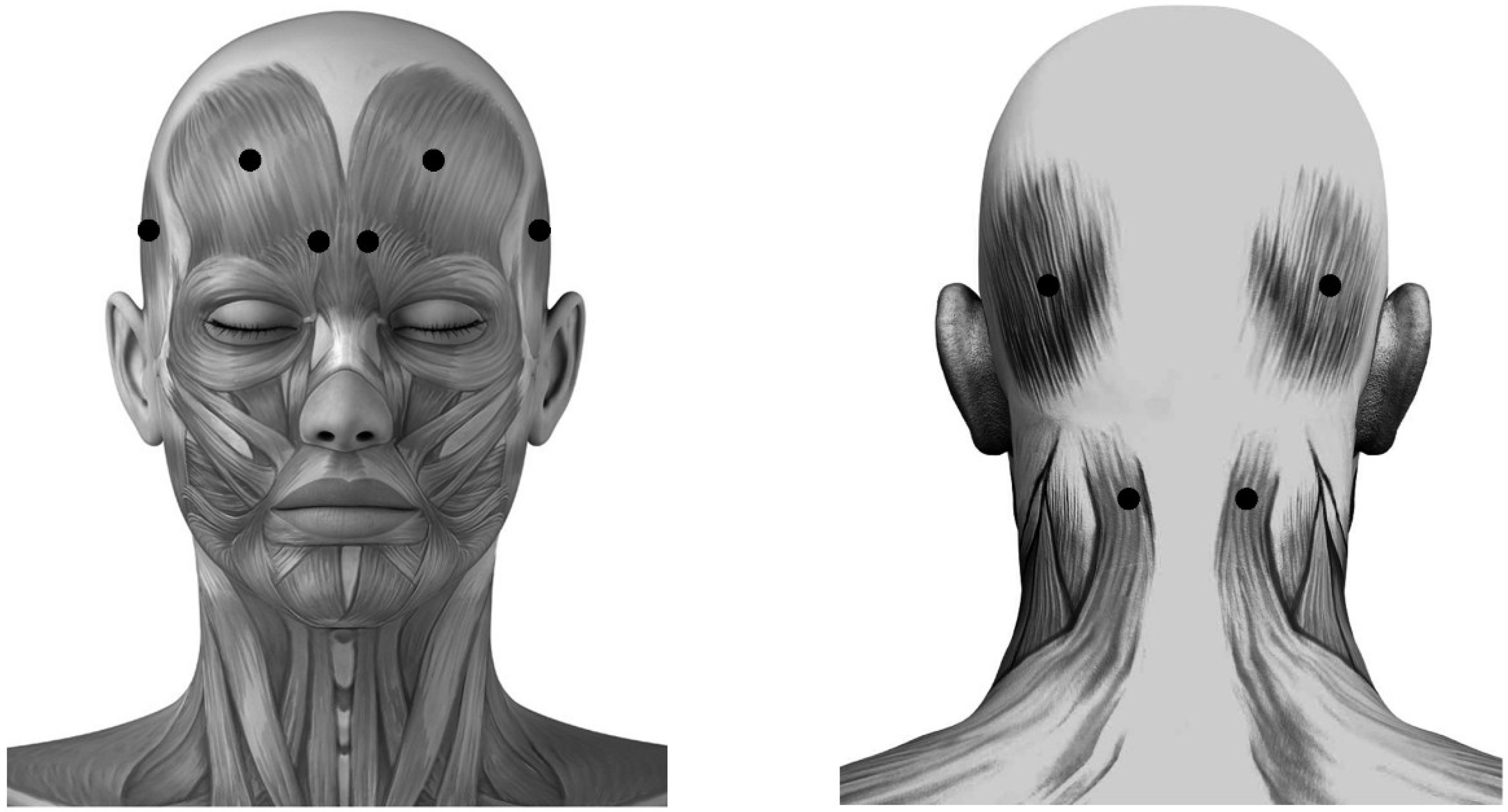
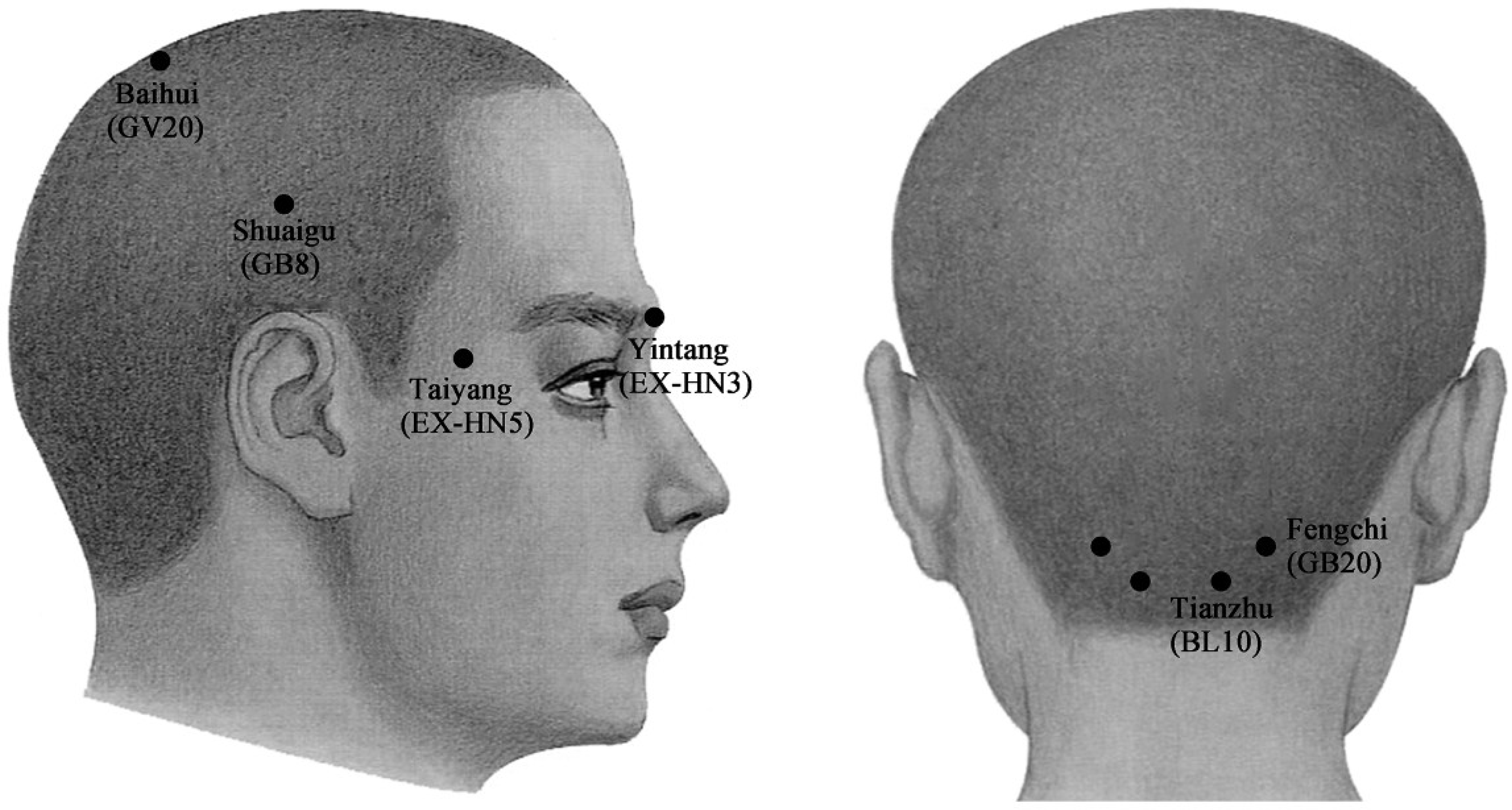
3.3. Treatment


3.4. Outcome Measure
3.5. Statistical Analyses
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jensen, R.; Stovner, L.J. Epidemiology and comorbidity of headache. Lancet Neurol. 2008, 7, 354–361. [Google Scholar] [CrossRef]
- Jensen, K. Extracranial blood flow, pain and tenderness in migraine. Clinical and experimental studies. Acta Neurol. Scand. Suppl. 1993, 147, 1–27. [Google Scholar] [PubMed]
- Olesen, J.; Bendtsen, L.; Dodick, D.; Ducros, A.; Evers, S.; First, M.; Goadsby, P.J.; Hershey, A.; Katsarava, Z.; Levin, M.; et al. The international classification of headache disorders, 3rd edition. Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Yarnitsky, D.; Goor-Aryeh, I.; Ransil, B.J.; Bajwa, Z.H. An association between migraine and cutaneous allodynia. Ann. Neurol. 2000, 47, 614–624. [Google Scholar] [CrossRef]
- Mathew, N.T.; Kailasam, J.; Seifert, T. Clinical recognition of allodynia in migraine. Neurology 2004, 63, 848–852. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. Clinical and pathophysiological observations in migraine and tension-type headache explained by integration of vascular, supraspinal and myofascial inputs. Pain 1991, 46, 125–132. [Google Scholar] [CrossRef]
- Farinelli, I.; De Filippis, S.; Coloprisco, G.; Missori, S.; Martelletti, P. Future drugs for migraine. Intern. Emerg. Med. 2009, 4, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.J.; Hargreaves, R.J. Neurogenic inflammation in the context of migraine. Microsc. Res. Tech. 2001, 53, 167–178. [Google Scholar] [CrossRef] [PubMed]
- May, A.; Goadsby, P.J. Substance p receptor antagonists in the therapy of migraine. Expert Opin. Investig. Drugs 2001, 10, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Fanciullacci, M.; Alessandri, M.; Figini, M.; Geppetti, P.; Michelacci, S. Increase in plasma calcitonin gene-related peptide from the extracerebral circulation during nitroglycerin-induced cluster headache attack. Pain 1995, 60, 119–123. [Google Scholar] [CrossRef]
- Dolly, O. Synaptic transmission: Inhibition of neurotransmitter release by botulinum toxins. Headache 2003, 43 (Suppl. 1), S16–S24. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.; Mathew, N.; Saper, J.; Jenkins, S. Botulinum toxin type A as a migraine preventive treatment. For the BOTOX migraine clinical research group. Headache 2000, 40, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Behmand, R.A.; Tucker, T.; Guyuron, B. Single-site botulinum toxin type A injection for elimination of migraine trigger points. Headache 2003, 43, 1085–1089. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Dodick, D.W.; Goadsby, P.J.; Lipton, R.B.; Olesen, J.; Silberstein, S.D. Chronic migraine—Classification, characteristics and treatment. Nat. Rev. Neurol. 2011, 8, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Farinelli, I.; Coloprisco, G.; De Filippis, S.; Martelletti, P. Long-term benefits of botulinum toxin type A (BOTOX) in chronic daily headache: A five-year long experience. J. Headache Pain 2006, 7, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Ashkenazi, A. Botulinum toxin type A for chronic migraine. Curr. Neurol. Neurosci. Rep. 2010, 10, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Schulte, L.H.; May, A. Headache research in 2014: Advancing migraine therapy. Lancet Neurol. 2015, 14, 6–7. [Google Scholar] [CrossRef]
- Semenov, I.A. Migraine headaches. Dis.-Month DM 2015, 61, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.R.; Childers, M.K. The Use of Botulinum Toxin Type a in Pain Management: A Clinecian’s Guide, 2nd ed.; Academic Information Systems Inc: Columbia, MO, USA, 2002. [Google Scholar]
- Blumenfeld, A.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; Binder, W.J. Method of injection of onabotulinumtoxina for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the preempt clinical program. Headache 2010, 50, 1406–1418. [Google Scholar] [CrossRef] [PubMed]
- Hollanda, L.; Monteiro, L.; Melo, A. Botulinum toxin type a for cephalic cutaneous allodynia in chronic migraine: A randomized, double-blinded, placebo-controlled trial. Neurol. Int. 2014, 6, 5133. [Google Scholar] [CrossRef] [PubMed]
- Poungvarin, N. The first world report of botulinum A toxin injection for status migrainosus. J. Med. Assoc. Thail. 2001, 84, 1199–1203. [Google Scholar]
- Tamura, B.M.; Chang, B. Botulinum toxin: Application into acupuncture points for migraine. Dermatol. Surg. 2003, 29, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.F.; Zhang, Y.; Zhao, P.; Yan, W.J.; Kong, X.P.; Fan, L.L.; Hou, Y.P. Botulinum toxin type A therapy in migraine: Preclinical and clinical trials. Iran. Red Crescent Med. J. 2013, 15, e7704. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Acupuncture: Review and Analysis of Repotrs on Controlled Clinical Trials; World Health Organization (WHO): Geneva, Switzerland, 2002. [Google Scholar]
- Witt, C.M.; Reinhold, T.; Jena, S.; Brinkhaus, B.; Willich, S.N. Cost-effectiveness of acupuncture treatment in patients with headache. Cephalalgia 2008, 28, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Linde, K.; Allais, G.; Brinkhaus, B.; Manheimer, E.; Vickers, A.; White, A.R. Acupuncture for migraine prophylaxis. Cochrane Database Syst. Rev. 2009, 1, CD001218. [Google Scholar] [PubMed]
- Karst, M.; Rollnik, J.D.; Fink, M.; Reinhard, M.; Piepenbrock, S. Pressure pain threshold and needle acupuncture in chronic tension-type headache—A double-blind placebo-controlled study. Pain 2000, 88, 199–203. [Google Scholar] [CrossRef]
- Strudwick, M.W.; Hinks, R.C.; Choy, S.T. Point injection as an alternative acupuncture technique—An exploratory study of responses in healthy subjects. Acupunct. Med. 2007, 25, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, W.; Li, L. Treating neurotic headache by point-injection with novocain. J. Tradit. Chin. Med. 1990, 10, 189–191. [Google Scholar] [PubMed]
- Ga, H.; Choi, J.H.; Park, C.H.; Yoon, H.J. Acupuncture needling versus lidocaine injection of trigger points in myofascial pain syndrome in elderly patients—A randomised trial. Acupunct. Med. 2007, 25, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.K.; Cheng, J. A case series of temporomandibular disorders treated with acupuncture, occlusal splint and point injection therapy. Acupunct. Med. 2003, 21, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Yeom, M.J.; Lee, H.C.; Kim, G.H.; Shim, I.; Lee, H.J.; Hahm, D.H. Therapeutic effects of hominis placenta injection into an acupuncture point on the inflammatory responses in subchondral bone region of adjuvant-induced polyarthritic rat. Biol. Pharm. Bull. 2003, 26, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Marx, C.; Silveira, M.D.; Selbach, I.; da Silva, A.S.; Braga, L.M.; Camassola, M.; Nardi, N.B. Acupoint injection of autologous stromal vascular fraction and allogeneic adipose-derived stem cells to treat hip dysplasia in dogs. Stem Cells Int. 2014, 2014, 391274. [Google Scholar] [CrossRef] [PubMed]
- Cady, R.; Schreiber, C. Botulinum toxin type A as migraine preventive treatment in patients previously failing oral prophylactic treatment due to compliance issues. Headache 2008, 48, 900–913. [Google Scholar] [CrossRef] [PubMed]
- Barrientos, N.; Chana, P. Botulinum toxin type A in prophylactic treatment of migraine headaches: A preliminary study. J. Headache Pain 2003, 4, 146–151. [Google Scholar] [CrossRef]
- Barbanti, P.; Egeo, G.; Fofi, L.; Aurilia, C.; Piroso, S. Rationale for use of onabotulinum toxin A (BOTOX) in chronic migraine. Neurol. Sci. 2015, 36, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Diener, H.C.; Degryse, R.E.; Lipton, R.B.; Turkel, C.C. Percent of patients with chronic migraine who responded per onabotulinumtoxin A treatment cycle: PREEMPT. J. Neurol. Neurosurg. Psychiatr. 2015, 86, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Wang, J.; Lawrence, G.; Dolly, J.O. Synaptobrevin i mediates exocytosis of cgrp from sensory neurons and inhibition by botulinum toxins reflects their anti-nociceptive potential. J. Cell Sci. 2007, 120, 2864–2874. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Zhang, X.; Levy, D.; Aoki, K.R.; Brin, M.F. Selective inhibition of meningeal nociceptors by botulinum neurotoxin type A: Therapeutic implications for migraine and other pains. Cephalalgia 2014, 34, 853–869. [Google Scholar] [CrossRef] [PubMed]
- Du, R.; Wang, Y.; Liu, X.; Liu, Z. Acupuncture for acute migraine attacks in adults: A systematic review protocol. BMJ Open 2015, 5, e006968. [Google Scholar] [CrossRef] [PubMed]
- de Vernejoul, P.; Albarede, P.; Darras, J.C. Nuclear medicine and acupuncture message transmission. J. Nuclear Med. 1992, 33, 409–412. [Google Scholar]
- Wang, L.; Cardini, F.; Zhao, W.; Regalia, A.L.; Wade, C.; Forcella, E.; Yu, J. Vitamin k acupuncture pint injection for severe primary dysmenorrhea: An international pilot study. MedGenMed 2004, 6, 45. [Google Scholar] [PubMed]
- Luo, L.; Chen, W.J. Development of acu-injedtion treatment. J. Clin. Acupunct. Moxibust. 2001, 17, 53–56. [Google Scholar]
- Mathew, N.T.; Kailasam, J.; Meadors, L. Predictors of response to botulinum toxin type A (BoNTA) in chronic daily headache. Headache 2008, 48, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Gobel, H. Botulinum toxin in migraine prophylaxis. J. Neurol. 2004, 251 (Suppl. 1), I8–I11. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.L.; Kuriyama, A.; Hayashino, Y. Botulinum toxin A for prophylactic treatment of migraine and tension headaches in adults: A meta-analysis. JAMA 2012, 307, 1736–1745. [Google Scholar] [PubMed]
- Lipton, R.B.; Silberstein, S.D. Episodic and chronic migraine headache: Breaking down barriers to optimal treatment and prevention. Headache 2015, 55, 103–122. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders: 2nd edition. Cephalalgia 2004, 24 (Suppl. 1), 9–160. [Google Scholar] [CrossRef] [PubMed]
- Sostak, P.; Krause, P.; Forderreuther, S.; Reinisch, V.; Straube, A. Botulinum toxin type-A therapy in cluster headache: An open study. J. Headache Pain 2007, 8, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, J. Illustration of Composed Acupoint in Acupuncture-Moxibustion Use, 2nd ed.; Shanghai Scientific and Technical Publishers: Shanghai, China, 2008. [Google Scholar]
- Shan, X.F.; Xu, H.; Cai, Z.G.; Wu, L.L.; Yu, G.Y. Botulinum toxin A inhibits salivary secretion of rabbit submandibular gland. Int. J. Oral Sci. 2013, 5, 217–223. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, M.; Xie, J.-F.; Kong, X.-P.; Zhang, Y.; Shao, Y.-F.; Wang, C.; Ren, W.-T.; Cui, G.-F.; Xin, L.; Hou, Y.-P. Acupoint Injection of Onabotulinumtoxin A for Migraines. Toxins 2015, 7, 4442-4454. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins7114442
Hou M, Xie J-F, Kong X-P, Zhang Y, Shao Y-F, Wang C, Ren W-T, Cui G-F, Xin L, Hou Y-P. Acupoint Injection of Onabotulinumtoxin A for Migraines. Toxins. 2015; 7(11):4442-4454. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins7114442
Chicago/Turabian StyleHou, Min, Jun-Fan Xie, Xiang-Pan Kong, Yi Zhang, Yu-Feng Shao, Can Wang, Wen-Ting Ren, Guang-Fu Cui, Le Xin, and Yi-Ping Hou. 2015. "Acupoint Injection of Onabotulinumtoxin A for Migraines" Toxins 7, no. 11: 4442-4454. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins7114442