
Feasibility Study and Experimental Evaluation of the Design of Nodule Prototype Developed for Palpation Display Apparatus: A Novel Device for Contactless Primary Tactile Diagnosis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Nodule Prototypes Design
2.2. Vacuum Controller
2.3. Experimental setup
2.4. Experimental Evaluation and Protocols
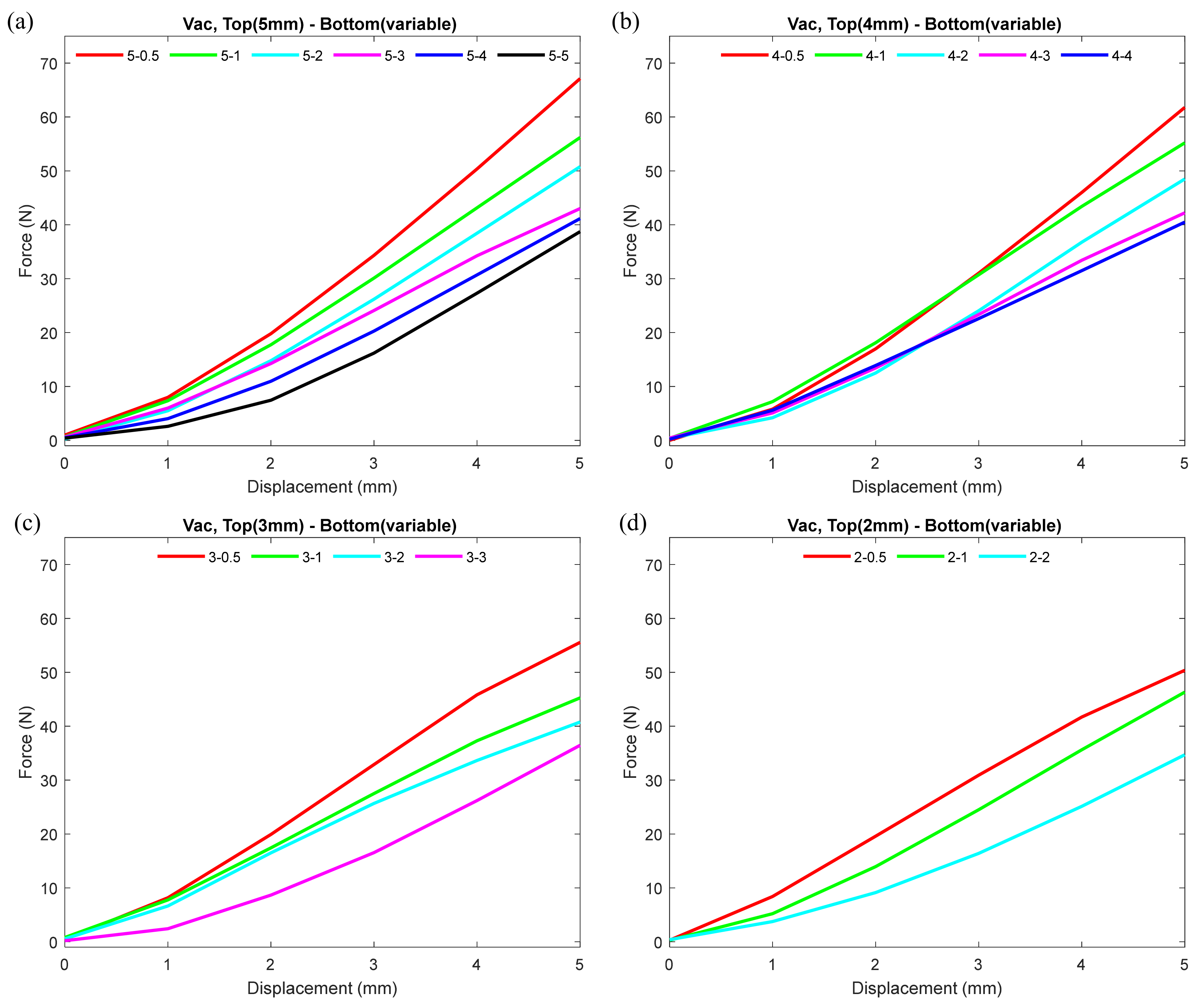
- Since one of the important features of our design included different thicknesses of two hemispheres of the nodule, we set a number of combinations by altering the wall thickness of the top and bottom hemispheres to study and evaluate the behavior of the nodule under uniform vacuum pressure. We 3D printed the top hemispheres of the nodule with thicknesses of 5, 4, 3, and 2 mm and bottom hemispheres with thicknesses of 5, 4, 3, 2, 1, and 0.5 mm.
- The thickness combinations we have chosen to assemble the nodules for this experiment are as follows (top hemisphere-bottom hemisphere):
- ▪
- 5 mm-5 mm, 5 mm-4 mm, 5 mm-3 mm, 5 mm-2 mm, 5 mm-1 mm, 5 mm-0.5 mm;
- ▪
- 4 mm-4 mm, 4 mm-3 mm, 4 mm-2 mm, 4 mm-1 mm, 4 mm-0.5 mm;
- ▪
- 3 mm-3 mm, 3 mm-2 mm, 3 mm-1 mm, 3 mm-0.5 mm;
- ▪
- 2 mm-2 mm, 2 mm-1 mm, 2 mm-0.5 mm.
- Each combination of the top and bottom hemisphere varied only by thickness but the internal hollow space (i.e., volume) remained the same. As mentioned earlier, the internal hollow space was filled with equal amount of coffee grains and sealed together to assemble each nodule.
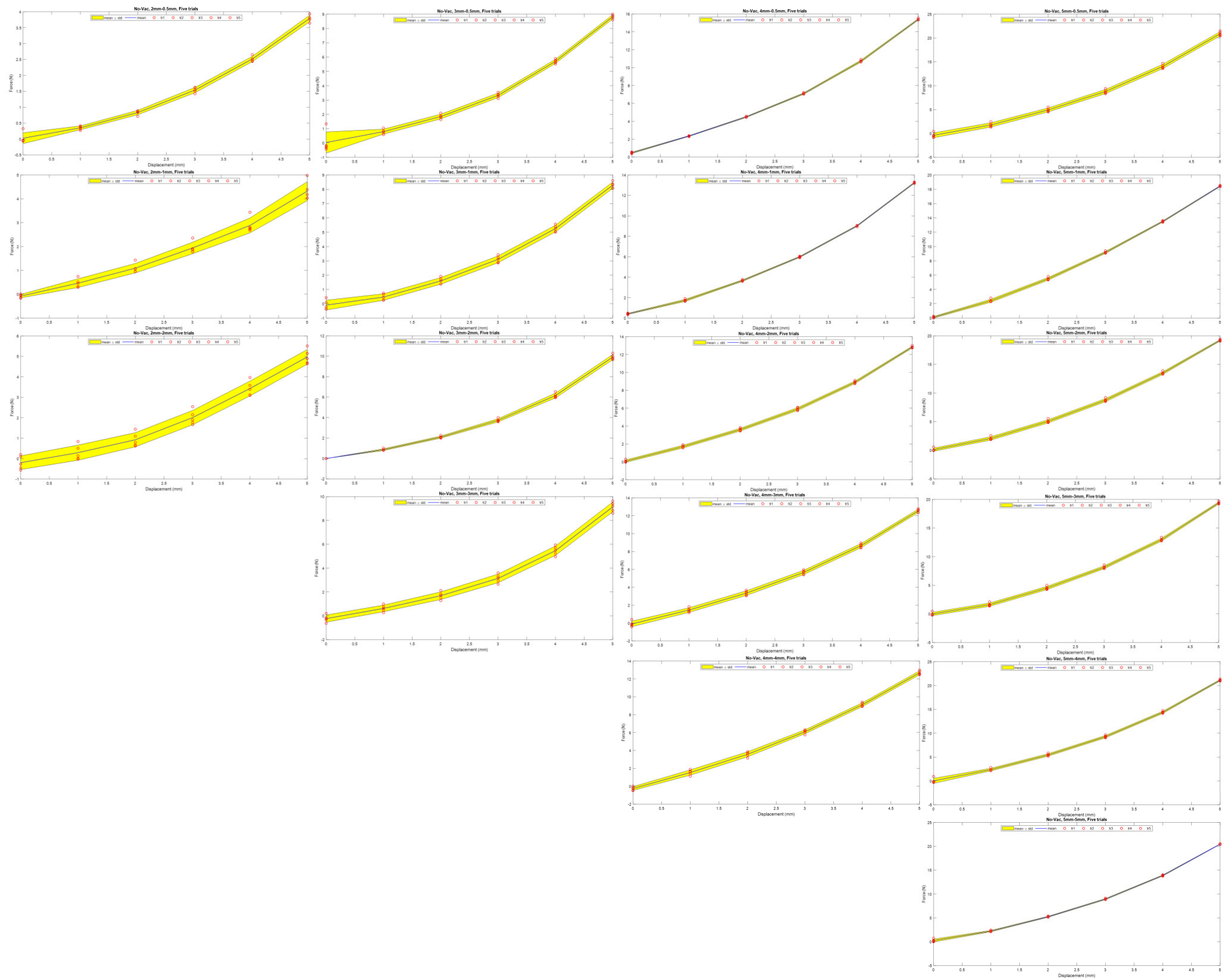
- First, we measured the stiffness of each nodules under no-vacuum (1 atmospheric pressure) condition.
- Later, we measured the stiffness under vacuum condition (2 ± 0.3 PSI).
2.5. Experimental Data Collection Method
3. Results
3.1. Nodule Stiffness Test Varying Thickness of Top and Bottom Hemispheres under No-Vacuum (No-Vac) Condition
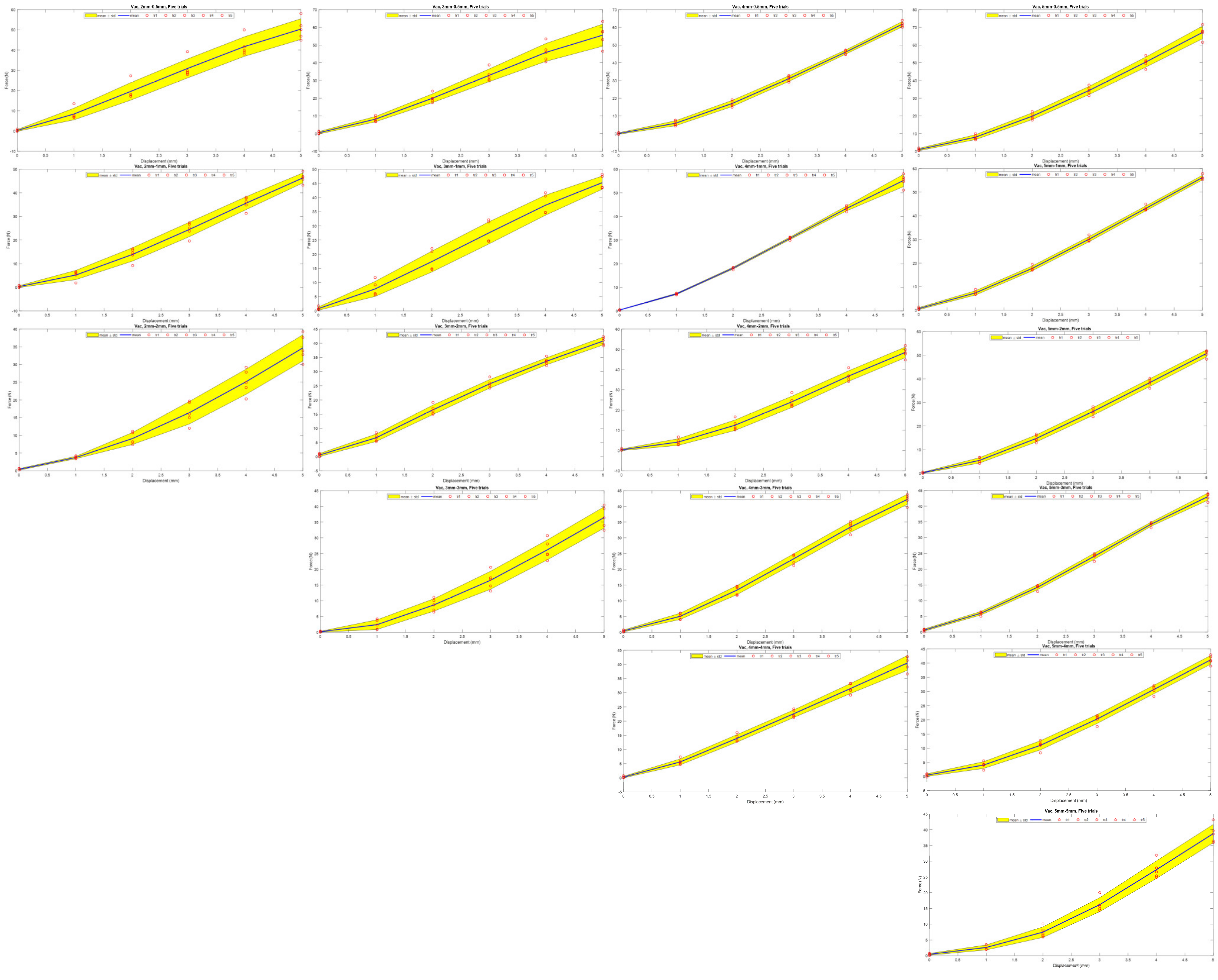
3.2. Stiffness Test Varying Top Hemisphere and Keeping Bottom Hemisphere Constant under Vacuum (Vac) Condition
3.3. Stiffness Test Keeping Thicknesses of Top Hemisphere Constant and Varying Bottom Hemisphere under Vacuum (Vac) Condition
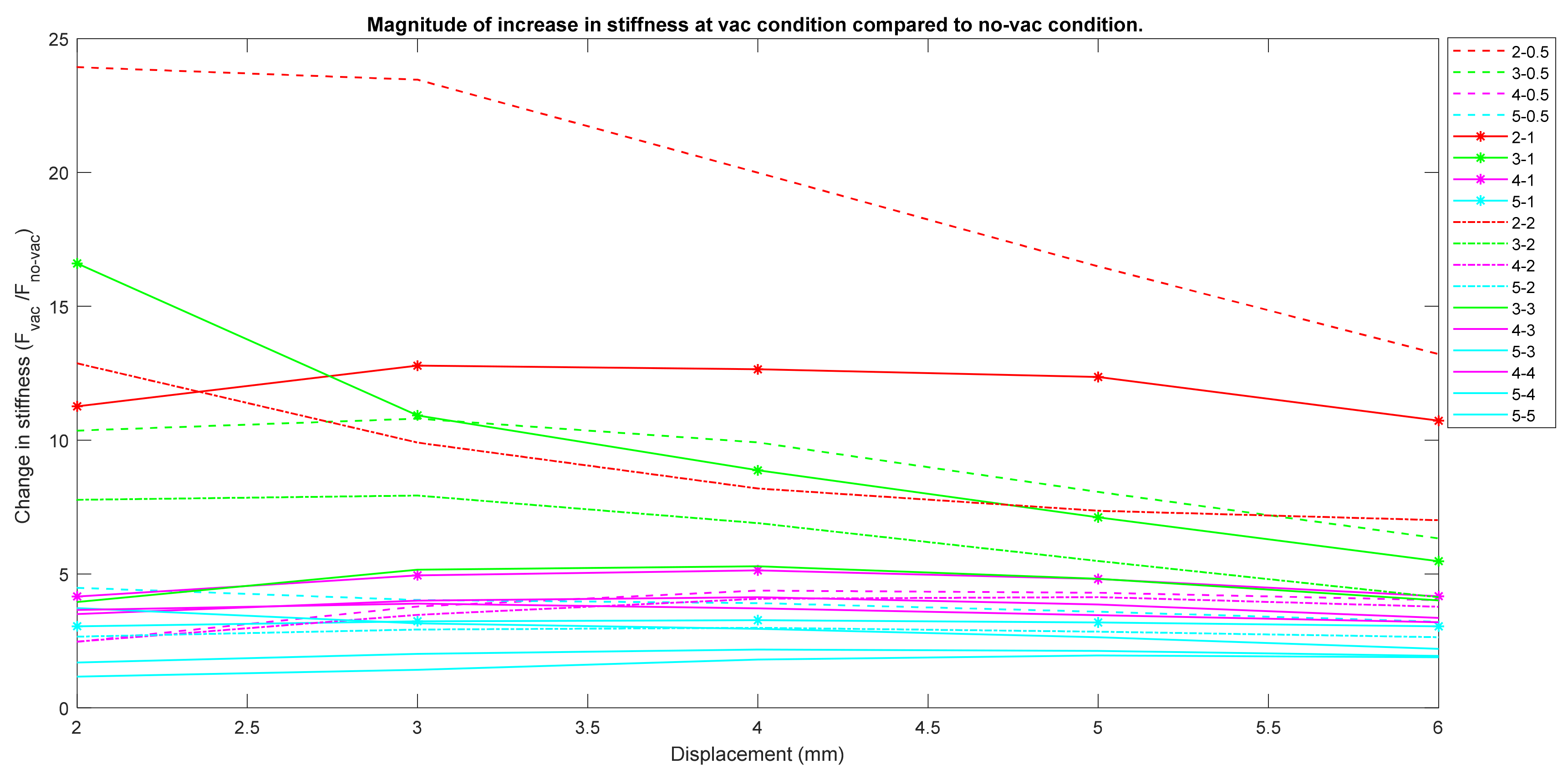
3.4. Change in Stiffness between No-Vac and Vac Conditions
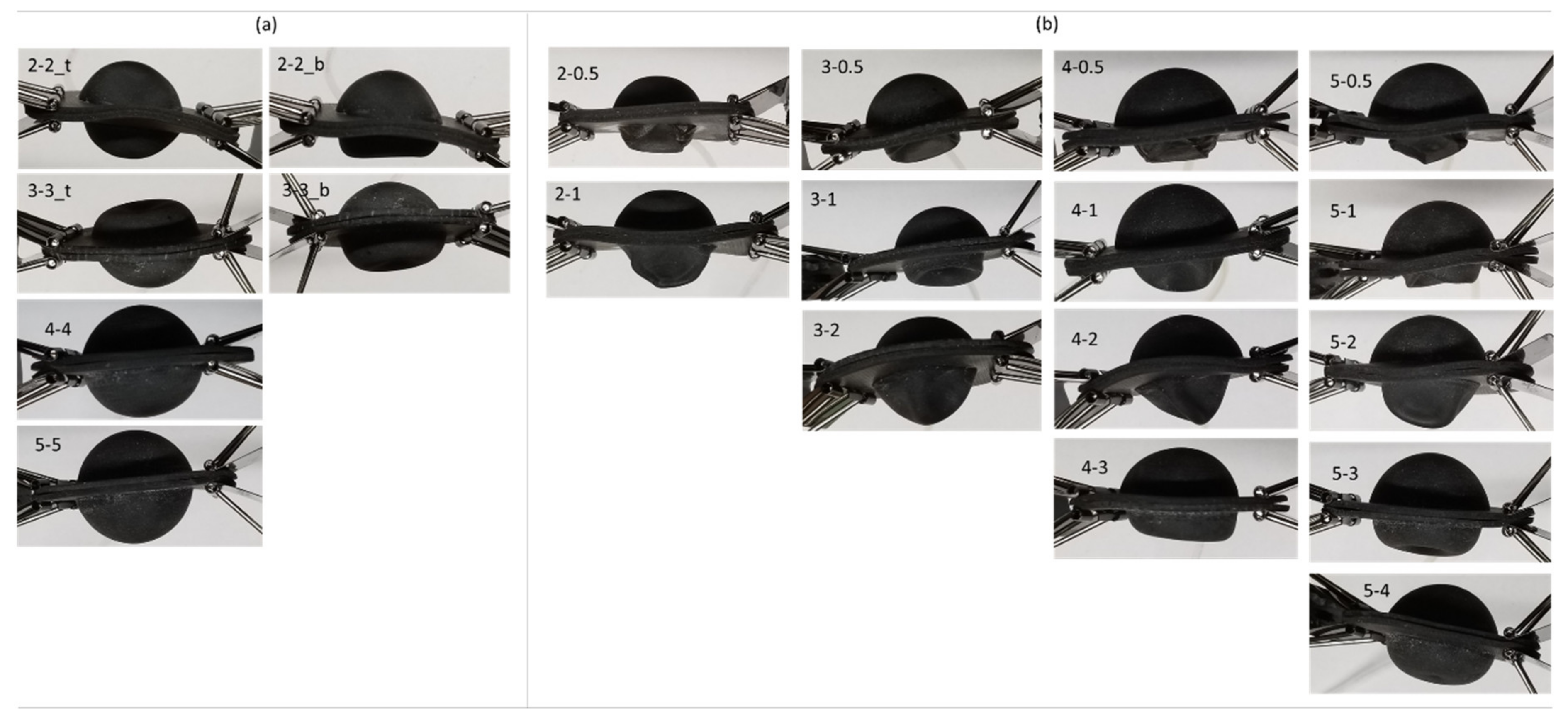
3.5. Deformation of the Nodule
Visual Record of Nodule Deformation Results
4. Discussion
5. Patents
Author Contributions
Funding
Conflicts of Interest
Appendix A


References
- Cancer Statistics; National Cancer Institut: Bethesda, MD, USA, 2019.
- Jain, R.K.; Martin, J.D.; Stylianopoulos, T. The role of mechanical forces in tumor growth and therapy. Annu. Rev. Biomed. Eng. 2014, 16, 321–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrance, S.E.; Voll, C.A.; Jochum, J.E. Enhancing Palpation Skills Through the Use of Stereognosis Drills. Athl. Train. Educ. J. 2016, 11, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Wiest, P.W.; Hartshorne, M.F.; Inskip, P.D.; Crooks, L.A.; Vela, B.S.; Telepak, R.J.; Williamson, M.R.; Blumhardt, R.; Bauman, J.M.; Tekkel, M. Thyroid palpation versus high-resolution thyroid ultrasonography in the detection of nodules. J. Ultrasound Med. 1998, 17, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Gwilliam, J.C.; Pezzementi, Z.; Jantho, E.; Okamura, A.M.; Hsiao, S. Human vs. robotic tactile sensing: Detecting lumps in soft tissue. In Proceedings of the 2010 IEEE Haptics Symposium, Waltham, MA, USA, 25–26 March 2010; 2010; pp. 21–28. [Google Scholar]
- Palpation. Med. Encycl., U.S. National Library of Medicine. Available online: https://medlineplus.gov/ency/article/002284.htm (accessed on 4 April 2020).
- Paszek, M.J.; Zahir, N.; Johnson, K.R.; Lakins, J.N.; Rozenberg, G.I.; Gefen, A.; Reinhart-King, C.A.; Margulies, S.S.; Dembo, M.; Boettiger, D.; et al. Tensional homeostasis and the malignant phenotype. Cancer Cell 2005, 8, 241–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phipps, S.; Yang, T.H.J.; Habib, F.K.; Reuben, R.L.; McNeill, S.A. Measurement of tissue mechanical characteristics to distinguish between benign and malignant prostatic disease. Urology 2005, 66, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Krouskop, T.A.; Wheeler, T.M.; Kallel, F.; Garra, B.S.; Hall, T. Elastic Moduli of Breast and Prostate Tissues under Compression. Ultrason. Imaging 1998, 20, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Brazier, Y. Tumors: Benign, premalignant and malignant. MedicalNewsToday 2019. Available online: https://www.medicalnewstoday.com/articles/249141 (accessed on 4 April 2020).
- Egorov, V.; Sarvazyan, A.P. Mechanical imaging of the breast. IEEE Trans. Med. Imaging 2008, 27, 1275–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Nguyen, C.; Saraf, R.F. Tactile Imaging of an Imbedded Palpable Structure for Breast Cancer Screening. ACS Appl. Mater. Interfaces 2014, 6, 16368–16374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lécuyer, A. Simulating Haptic Feedback Using Vision: A Survey of Research and Applications of Pseudo-Haptic Feedback. Presence Teleoperators Virtual Environ. 2009, 18, 39–53. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Ryu, J.-H.; Lee, W. Palpation simulator with stable haptic feedback. Minim. Invasive Ther. Allied Technol. 2015, 24, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Abdominal Assessment Training Simulator. Available online: https://www.gtsimulators.com/kyoto-kagaku-abdominal-assessment-model-p/kk-mw43.htm (accessed on 4 April 2020).
- Breast Examination Simulator. Available online: https://www.gtsimulators.com/Life-form-Breast-Examination-Simulator-p/lf00984u.htm (accessed on 4 April 2020).
- Limbs & Things-Abdominal Examination Trainer. Available online: https://limbsandthings.com/global/products/60000/60000-abdominal-examination-trainer (accessed on 4 April 2020).
- Breast palpation simulator, Breast examination simulator-All medical device manufacturers. Available online: https://www.medicalexpo.com/medical-manufacturer/breast-palpation-simulator-13310.html (accessed on 4 April 2020).
- Williams II, R.L.; Srivastava, M.; Howell, J.N.; Conatser, R.R.; Eland, D.C.; Janet Burns, D.M.; Anthony Chila, D.G. The Virtual Haptic Back for Palpatory Training. In Proceedings of the ICMI ’04, Proceedings of the 6th International Conference on Multimodal Interfaces, State College, PA, USA,, 14–15 October 2004; pp. 191–197. [Google Scholar]
- Jeon, S.; Knoerlein, B.; Harders, M.; Choi, S. Haptic simulation of breast cancer palpation: A case study of haptic augmented reality. In Proceedings of the 2010 IEEE International Symposium on Mixed and Augmented Reality, Seoul, Korea, 13–16 October 2010; pp. 237–238. [Google Scholar]
- Baillie, S.; Crossan, A.; Brewster, S.; Mellor, D.; Reid, S. Validation of a bovine rectal palpation simulator for training veterinary students. Stud. Health Technol. Inform. 2005, 111, 33–36. [Google Scholar] [PubMed]
- Ishizuka, H.; Lorenzoni, N.; Miki, N.; Leonardo Da Vinci, P. Tactile display for presenting stiffness distribution using magnetorheological fluid. Bull. JSME Mech. Eng. J. 2014, 1. [Google Scholar] [CrossRef]
- Takaiwa, M.; Noritsugu, T. Development of breast cancer palpation simulator using pneumatic parallel manipulator. In Proceedings of the SICE Annual Conference 2007, Takamatsu, Japan, 17–20 September 2007; pp. 823–827. [Google Scholar]
- Gwilliam, J.C.; Degirmenci, A.; Bianchi, M.; Okamura, A.M. Design and control of an air-jet lump display. In Proceedings of the 2012 IEEE Haptics Symposium (HAPTICS), Vancouver, BC, Canada, 4–7 March 2012; pp. 45–49. [Google Scholar]
- Li, M.; Luo, S.; Xu, G. A tactile sensing and feedback system for tumor localization. In Proceedings of the 2016 13th International Conference on Ubiquitous Robots and Ambient Intelligence (URAI), Xi’an, China, 19–22 August 2016; pp. 259–262. [Google Scholar]
- Talhan, A.; Jeon, S. Programmable prostate palpation simulator using property-changing pneumatic bladder. Comput. Biol. Med. 2018, 96, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Ranzani, T.; Sareh, S.; Seneviratne, L.D.; Dasgupta, P.; Wurdemann, H.A.; Althoefer, K. Multi-fingered haptic palpation utilizing granular jamming stiffness feedback actuators. Smart Mater. Struct. 2014, 23, 095007. [Google Scholar] [CrossRef]
- Kokes, R.; Lister, K.; Gullapalli, R.; Zhang, B.; MacMillan, A.; Richard, H.; Desai, J.P. Towards a teleoperated needle driver robot with haptic feedback for RFA of breast tumors under continuous MRI. Med. Image Anal. 2009, 13, 445–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamura, A.M. Methods for haptic feedback in teleoperated robot-assisted surgery. Ind. Rob. 2004, 31, 499–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sikander, S.; Biswas, P.; Kulkarni, P.; Harrington, C.; Chang, N.; Song, S.-E. Concept Development of Fixed Geometry Tactile Display using Granular Jamming. In Proceedings of the 2019 International Symposium on Medical Robotics (ISMR), Atlanta, GA, USA, 3–5 April 2019; pp. 1–4. [Google Scholar]
- Sikander, S.; Biswas, P.; Kulkarni, P.; Atwood, B.; Song, S.-E. Prototyping and Initial Feasibility Study of Palpation Display Apparatus Using Granular Jamming. In Proceedings of the 2019 IEEE Healthcare Innovations and Point of Care Technologies, (HI-POCT), Bethesda, MD, USA, 20–22 November 2019; pp. 71–74. [Google Scholar]
- Sikander, S.; Biswas, P.; Kulkarni, P.; Mansy, H.; Rahnavard, N.; Song, S.-E. A concept of medical expertise pooling by tele sensing and manipulation: Emergency medicine case. In Proceedings of the 2017 IEEE Healthcare Innovations and Point of Care Technologies (HI-POCT), Bethesda, MD, USA, 6–8 November 2017; pp. 233–236. [Google Scholar]
- Coronavirus Disease 2019 (COVID-19)|coronavirus.gov. Available online: https://www.coronavirus.gov/ (accessed on 2 February 2021).
- Cases in U.S. | CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html (accessed on 6 April 2020).
- Agilus 30: A Flexible Photopolymer 3D Printing Material | Stratasys. Available online: https://www.stratasys.com/materials/search/agilus30 (accessed on 25 February 2021).
- Cheng, N.G.; Lobovsky, M.B.; Keating, S.J.; Setapen, A.M.; Gero, K.I.; Hosoi, A.E.; Iagnemma, K.D. Design and analysis of a robust, low-cost, highly articulated manipulator enabled by jamming of granular media. In Proceedings of the IEEE International Conference on Robotics and Automation, Saint Paul, MN, USA, 14–18 May 2012; pp. 4328–4333. [Google Scholar]
- Fibrianto, K.; Febryana, Y.R.; Wulandari, E.S. Effect of brewing technique and particle size of the ground coffee on sensory profiling of brewed Dampit robusta coffee. IOP Conf. Ser. Earth Environ. Sci. 2018, 131, 12009. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nodule Wall Thickness (Top_Bottom) | 2_0.5 | 2_1 | 2_2 | 3_0.5 | 3_1 | 3_2 | 3_3 | 4_0.5 | 4_1 | 4_2 | 4_3 | 4_4 | 5_0.5 | 5_1 | 5_2 | 5_3 | 5_4 | 5_5 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trial 1 | 2.15 | 4.04 | 3.77 | 1.34 | 1.15 | 3.86 | 7.00 | 1.32 | 1.75 | 2.14 | 5.29 | 7.30 | 1.25 | 1.22 | 1.54 | 2.36 | 2.71 | 2.92 |
| Trial 2 | 2.24 | 3.34 | 7.13 | 1.66 | 1.38 | 4.20 | 7.29 | 1.24 | 1.70 | 2.48 | 5.49 | 7.24 | 1.19 | 1.24 | 1.46 | 2.21 | 2.84 | 2.62 |
| Trial 3 | 2.42 | 3.26 | 7.23 | 1.77 | 1.37 | 5.02 | 7.28 | 1.28 | 1.79 | 2.44 | 5.44 | 7.09 | 1.16 | 1.22 | 1.54 | 2.38 | 2.80 | 2.82 |
| Mean | 2.27 | 3.54 | 6.04 | 1.59 | 1.23 | 4.36 | 7.19 | 1.28 | 1.74 | 2.35 | 5.41 | 7.21 | 1.20 | 1.22 | 1.51 | 2.31 | 2.78 | 2.78 |
| Standard Deviation | 0.14 | 0.43 | 1.97 | 0.22 | 0.13 | 0.60 | 0.17 | 0.04 | 0.05 | 0.19 | 0.10 | 0.11 | 0.05 | 0.01 | 0.05 | 0.09 | 0.07 | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikander, S.; Biswas, P.; Song, S.-E. Feasibility Study and Experimental Evaluation of the Design of Nodule Prototype Developed for Palpation Display Apparatus: A Novel Device for Contactless Primary Tactile Diagnosis. Micromachines 2021, 12, 576. https://0-doi-org.brum.beds.ac.uk/10.3390/mi12050576
Sikander S, Biswas P, Song S-E. Feasibility Study and Experimental Evaluation of the Design of Nodule Prototype Developed for Palpation Display Apparatus: A Novel Device for Contactless Primary Tactile Diagnosis. Micromachines. 2021; 12(5):576. https://0-doi-org.brum.beds.ac.uk/10.3390/mi12050576
Chicago/Turabian StyleSikander, Sakura, Pradipta Biswas, and Sang-Eun Song. 2021. "Feasibility Study and Experimental Evaluation of the Design of Nodule Prototype Developed for Palpation Display Apparatus: A Novel Device for Contactless Primary Tactile Diagnosis" Micromachines 12, no. 5: 576. https://0-doi-org.brum.beds.ac.uk/10.3390/mi12050576