Hyperprogressive Disease during Anti-PD-1 (PDCD1) / PD-L1 (CD274) Therapy: A Systematic Review and Meta-Analysis

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
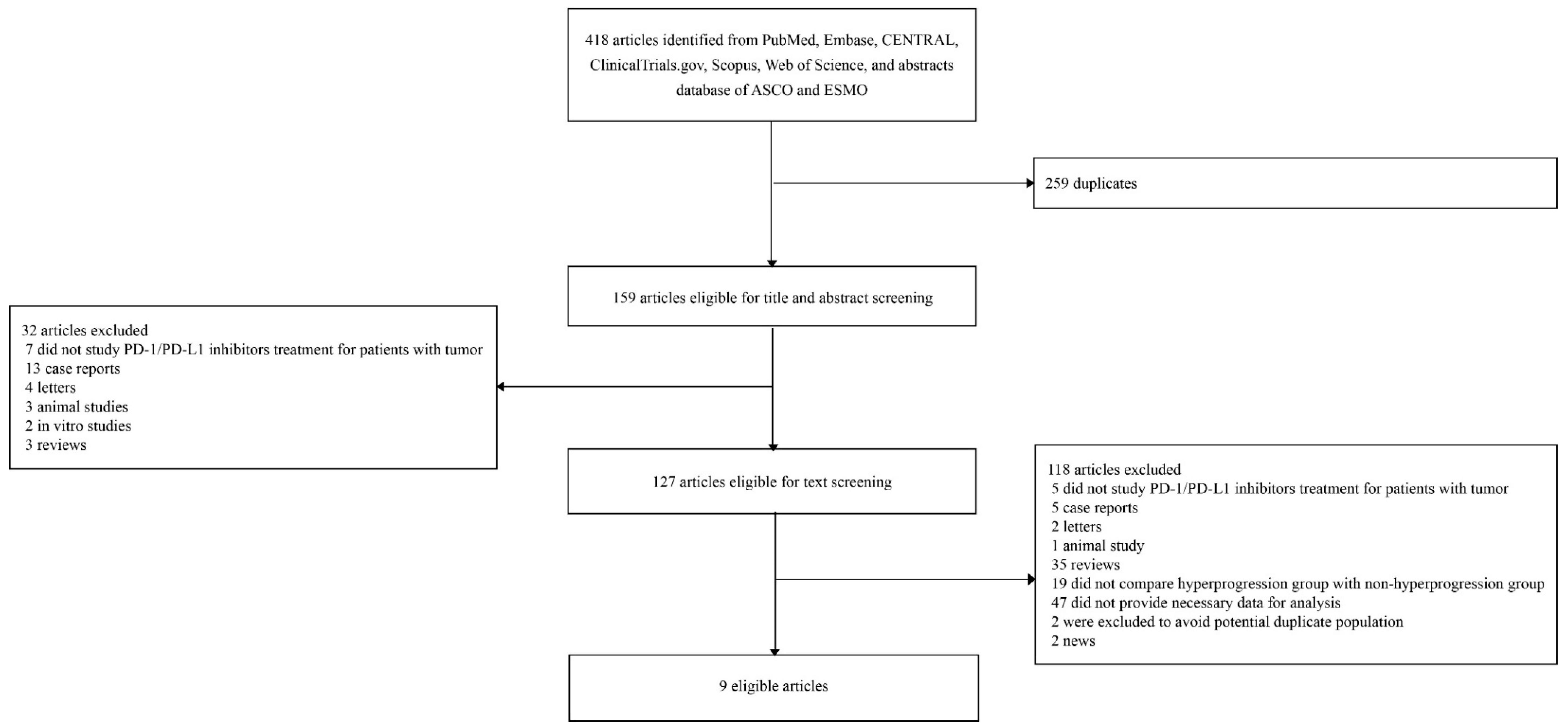
4.1. Literature Search Strategy and Eligibility Criteria
4.2. Data Extraction
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Miller, W.H., Jr.; Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; et al. Overall Survival in Patients with Advanced Melanoma Who Received Nivolumab Versus Investigator’s Choice Chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbe, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the evaluation of immune therapy activity in solid tumors: Immune-related response criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef]
- Guaitoli, G.; Baldessari, C.; Bertolini, F.; Tomasello, C.; Cascinu, S.; Barbieri, F. Are we ready to describe response or progression to immunotherapy in lung cancer? Crit. Rev. Oncol. Hematol. 2019, 138, 112–119. [Google Scholar] [CrossRef]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litiere, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef]
- Champiat, S.; Dercle, L.; Ammari, S.; Massard, C.; Hollebecque, A.; Postel-Vinay, S.; Chaput, N.; Eggermont, A.; Marabelle, A.; Soria, J.C.; et al. Hyperprogressive Disease Is a New Pattern of Progression in Cancer Patients Treated by Anti-PD-1/PD-L1. Clin. Cancer Res. 2017, 23, 1920–1928. [Google Scholar] [CrossRef]
- Saada-Bouzid, E.; Defaucheux, C.; Karabajakian, A.; Coloma, V.P.; Servois, V.; Paoletti, X.; Even, C.; Fayette, J.; Guigay, J.; Loirat, D.; et al. Hyperprogression during anti-PD-1/PD-L1 therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma. Ann. Oncol. 2017, 28, 1605–1611. [Google Scholar] [CrossRef]
- Kato, S.; Goodman, A.; Walavalkar, V.; Barkauskas, D.A.; Sharabi, A.; Kurzrock, R. Hyperprogressors after Immunotherapy: Analysis of Genomic Alterations Associated with Accelerated Growth Rate. Clin. Cancer Res. 2017, 23, 4242–4250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, R.; Mezquita, L.; Texier, M.; Lahmar, J.; Audigier-Valette, C.; Tessonnier, L.; Mazieres, J.; Zalcman, G.; Brosseau, S.; Le Moulec, S.; et al. Hyperprogressive Disease in Patients with Advanced Non-Small Cell Lung Cancer Treated with PD-1/PD-L1 Inhibitors or with Single-Agent Chemotherapy. JAMA Oncol. 2018, 4, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Aoki, M.; Shoji, H.; Nagashima, K.; Imazeki, H.; Miyamoto, T.; Hirano, H.; Honma, Y.; Iwasa, S.; Okita, N.; Takashima, A.; et al. Hyperprogressive disease during nivolumab or irinotecan treatment in patients with advanced gastric cancer. ESMO Open 2019, 4, e000488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo Russo, G.; Moro, M.; Sommariva, M.; Cancila, V.; Boeri, M.; Centonze, G.; Ferro, S.; Ganzinelli, M.; Gasparini, P.; Huber, V.; et al. Antibody-Fc/FcR Interaction on Macrophages as a Mechanism for Hyperprogressive Disease in Non-small Cell Lung Cancer Subsequent to PD-1/PD-L1 Blockade. Clin. Cancer Res. 2019, 25, 989–999. [Google Scholar] [CrossRef]
- Kanjanapan, Y.; Day, D.; Wang, L.; Al-Sawaihey, H.; Abbas, E.; Namini, A.; Siu, L.L.; Hansen, A.; Razak, A.A.; Spreafico, A.; et al. Hyperprogressive disease in early-phase immunotherapy trials: Clinical predictors and association with immune-related toxicities. Cancer 2019, 125, 1341–1349. [Google Scholar] [CrossRef]
- Tunali, I.; Gray, J.E.; Qi, J.; Abdalah, M.; Jeong, D.K.; Guvenis, A.; Gillies, R.J.; Schabath, M.B. Novel clinical and radiomic predictors of rapid disease progression phenotypes among lung cancer patients treated with immunotherapy: An early report. Lung Cancer 2019, 129, 75–79. [Google Scholar] [CrossRef]
- Kim, C.G.; Kim, K.H.; Pyo, K.H.; Xin, C.F.; Hong, M.H.; Ahn, B.C.; Kim, Y.; Choi, S.J.; Yoon, H.I.; Lee, J.G.; et al. Hyperprogressive disease during PD-1/PD-L1 blockade in patients with non-small-cell lung cancer. Ann. Oncol. 2019, 30, 1104–1113. [Google Scholar] [CrossRef]
- Sasaki, A.; Nakamura, Y.; Mishima, S.; Kawazoe, A.; Kuboki, Y.; Bando, H.; Kojima, T.; Doi, T.; Ohtsu, A.; Yoshino, T.; et al. Predictive factors for hyperprogressive disease during nivolumab as anti-PD1 treatment in patients with advanced gastric cancer. Gastric Cancer 2019, 22, 793–802. [Google Scholar] [CrossRef] [Green Version]
- Kamada, T.; Togashi, Y.; Tay, C.; Ha, D.; Sasaki, A.; Nakamura, Y.; Sato, E.; Fukuoka, S.; Tada, Y.; Tanaka, A.; et al. PD-1(+) regulatory T cells amplified by PD-1 blockade promote hyperprogression of cancer. Proc. Natl. Acad. Sci. USA 2019, 116, 9999–10008. [Google Scholar] [CrossRef]
- Garrido-Laguna, I.; Janku, F.; Vaklavas, C.; Falchook, G.S.; Fu, S.; Hong, D.S.; Naing, A.; Tsimberidou, A.M.; Wen, S.; Kurzrock, R. Validation of the Royal Marsden Hospital prognostic score in patients treated in the Phase I Clinical Trials Program at the MD Anderson Cancer Center. Cancer 2012, 118, 1422–1428. [Google Scholar] [CrossRef]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellmann, M.D.; Ciuleanu, T.-E.; Pluzanski, A.; Lee, J.S.; Otterson, G.A.; Audigier-Valette, C.; Minenza, E.; Linardou, H.; Burgers, S.; Salman, P.; et al. Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden. N. Engl. J. Med. 2018, 378, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Duran, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Champiat, S.; Ferrara, R.; Massard, C.; Besse, B.; Marabelle, A.; Soria, J.C.; Ferte, C. Hyperprogressive disease: Recognizing a novel pattern to improve patient management. Nat. Rev. Clin. Oncol. 2018, 15, 748–762. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Borghaei, H.; Langer, C.J.; Gadgeel, S.; Papadimitrakopoulou, V.A.; Patnaik, A.; Powell, S.F.; Gentzler, R.D.; Martins, R.G.; Stevenson, J.P.; Jalal, S.I.; et al. 24-Month Overall Survival from KEYNOTE-021 Cohort G: Pemetrexed and Carboplatin with or without Pembrolizumab as First-Line Therapy for Advanced Nonsquamous Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2019, 14, 124–129. [Google Scholar] [CrossRef]
- Champiat, S.; Besse, B.; Marabelle, A. Hyperprogression during immunotherapy: Do we really want to know? Ann. Oncol. 2019, 30, 1028–1031. [Google Scholar] [CrossRef]
- Refae, S.; Ebran, N.; Gal, J.; Otto, J.; Giacchero, D.; Borchiellini, D.; Guigay, J.; Peyrade, F.; Milano, G.; Saada, E. Host immunogenetics and hyperprogression under PD1/PD-L1 checkpoint inhibitors. Cancer Res. 2018, 78, Abstract nr 4548. [Google Scholar]
- Saada-Bouzid, E.; Refae, S.; Ebran, N.; Gal, J.; Peyrade, F.; Guigay, J.; Milano, G. Variations in PD1, PD-L1, IDO1 and VEGR2 genes and association with outcomes in advanced head and neck squamous cell carcinoma (HNSCC) patients treated with anti-PD1/PD-L1 based immunotherapy. Ann. Oncol. 2017, 28. [Google Scholar]
- Funazo, T.; Nomizo, T.; Kim, Y.H. Liver Metastasis Is Associated with Poor Progression-Free Survival in Patients with Non-Small Cell Lung Cancer Treated with Nivolumab. J. Thorac. Oncol. 2017, 12, e140–e141. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Hellmann, M.D.; Hamid, O.; Tsai, K.K.; Loo, K.L.; Gubens, M.A.; Rosenblum, M.; Harview, C.L.; Taube, J.M.; Handley, N.; et al. Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC. Cancer Immunol. Res. 2017, 5, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Mehdizadeh, S.; Tsai, K.; Algazi, A.; Rosenblum, M.; Daud, A.; Bluestone, J.A. Immunological Insights into Liver Metastasis Associated Resistance to Checkpoint Blockade Cancer Immunotherapy. J. Immunol. 2018, 200, 122.26. [Google Scholar]
- Tamiya, M.; Tamiya, A.; Inoue, T.; Kimura, M.; Kunimasa, K.; Nakahama, K.; Taniguchi, Y.; Shiroyama, T.; Isa, S.I.; Nishino, K.; et al. Metastatic site as a predictor of nivolumab efficacy in patients with advanced non-small cell lung cancer: A retrospective multicenter trial. PLoS ONE 2018, 13, e0192227. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, S.S.; Keilholz, U.; Gilles, E.; Bedikian, A.Y.; Wu, J.; Kay, R.; Stein, C.A.; Itri, L.M.; Suciu, S.; Eggermont, A.M. LDH correlation with survival in advanced melanoma from two large, randomised trials (Oblimersen GM301 and EORTC 18951). Eur. J. Cancer 2009, 45, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Koukourakis, M.I.; Giatromanolaki, A.; Sivridis, E.; Bougioukas, G.; Didilis, V.; Gatter, K.C.; Harris, A.L. Lactate dehydrogenase-5 (LDH-5) overexpression in non-small-cell lung cancer tissues is linked to tumour hypoxia, angiogenic factor production and poor prognosis. Br. J. Cancer 2003, 89, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Calcinotto, A.; Filipazzi, P.; Grioni, M.; Iero, M.; De Milito, A.; Ricupito, A.; Cova, A.; Canese, R.; Jachetti, E.; Rossetti, M.; et al. Modulation of microenvironment acidity reverses anergy in human and murine tumor-infiltrating T lymphocytes. Cancer Res. 2012, 72, 2746–2756. [Google Scholar] [CrossRef]
- Brand, A.; Singer, K.; Koehl, G.E.; Kolitzus, M.; Schoenhammer, G.; Thiel, A.; Matos, C.; Bruss, C.; Klobuch, S.; Peter, K.; et al. LDHA-Associated Lactic Acid Production Blunts Tumor Immunosurveillance by T and NK Cells. Cell Metab. 2016, 24, 657–671. [Google Scholar] [CrossRef] [Green Version]
- Feng, J.; Yang, H.; Zhang, Y.; Wei, H.; Zhu, Z.; Zhu, B.; Yang, M.; Cao, W.; Wang, L.; Wu, Z. Tumor cell-derived lactate induces TAZ-dependent upregulation of PD-L1 through GPR81 in human lung cancer cells. Oncogene 2017, 36, 5829–5839. [Google Scholar] [CrossRef]
- Wang, Q.; Gao, J.; Wu, X. Pseudoprogression and hyperprogression after checkpoint blockade. Int. Immunopharmacol. 2018, 58, 125–135. [Google Scholar] [CrossRef]
- Kurman, J.S.; Murgu, S.D. Hyperprogressive disease in patients with non-small cell lung cancer on immunotherapy. J. Thorac. Dis. 2018, 10, 1124–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, P.; Bera, K.; Vaidya, P.; Khorrami, M.; Jain, P.; Madabhushi, A.; Velcheti, V. Pre-Therapy Radiomic Features Can Distinguish Hyperprogression from Other Response Patterns to PD1/PD-L1 Inhibitors in NSCLC. J. Thorac. Oncol. 2018, 13, S737. [Google Scholar] [CrossRef]
- Matos Garcia, I.; García Ruiz, A.; Martin-Liberal, J.; Hierro, C.; Ochoa De Olza Amat, M.; Viaplana, C.; Mur, G.; Vieito Villar, M.; Brana, I.; Azaro, A.; et al. Refining criteria of hyperprogression (HPD) with immune checkpoint inhibitors (ICIs) to improve clinical applicability. Ann. Oncol. 2018, 29, viii649–viii669. [Google Scholar] [CrossRef]
- Weiss, G.J.; Beck, J.; Braun, D.P.; Bornemann-Kolatzki, K.; Barilla, H.; Cubello, R.; Quan, W.; Sangal, A.; Khemka, V.; Waypa, J.; et al. Tumor cell-free DNA copy number instability predicts therapeutic response to immunotherapy. Clin. Cancer Res. 2017, 23, 5074–5081. [Google Scholar] [CrossRef]
- Luchini, C.; Bibeau, F.; Ligtenberg MJ, L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.Y.; Andre, F.; et al. ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: A systematic review-based approach. Ann. Oncol. 2019. Epub ahead of print. Available online: https://0-academic-oup-com.brum.beds.ac.uk/annonc/article/30/8/1232/5485230 (accessed on 15 June 2019).
- Wells, G.A.; Shea, B.; Connell, D.O.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 June 2019).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Spiegelhalter, D.J. A re-evaluation of random-effects meta-analysis. J. R Stat. Soc. Ser. A Stat. Soc. 2009, 172, 137–159. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Smith, G.D. Sifting the evidence-what’s wrong with significance tests? BMJ 2001, 322, 226–231. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Type of Study | Country, Institution | Number of Patients | Underlying Malignancy | Treatment | Incidence of HPD |
|---|---|---|---|---|---|---|
| Champiat, et al. 2017 [9] | Retrospective analysis of clinical trials | France, single center | 131 | Melanoma (34%), lung (10%), renal (7%), colorectal (6%), urothelial (6%), others (37%) | PD-1/PD-L1 inhibitor monotherapy | 9% (12/131) |
| Kato, et al. 2017 [11] | Retrospective cohort | USA, single center | 102 | NSCLC (37%), head and neck (9%), cutaneous squamous cell carcinoma (9%), melanoma (6%), renal cell carcinoma (5%) | PD-1/PD-L1 inhibitor monotherapy | 6% (6/102) |
| Saada-Bouzid, et al. 2017 [10] | Retrospective cohort | France, 4 centers | 34 | Recurrent and/or metastatic head and neck squamous cell carcinoma | PD-1/PD-L1 inhibitors | 29% (10/34) |
| Ferrara, et al. 2018 [12] | Retrospective cohort | France, 8 centers | 406 | NSCLC | PD-1/PD-L1 inhibitors | 14% (56/406) |
| Lo Russo, et al. 2019 [14] | Retrospective cohort | Italy, single center | 152 | NSCLC | PD-1/PD-L1 inhibitors | 26% (39/152) |
| Sasaki, et al. 2019 [18] | Retrospective cohort | Japan, single center | 62 | Advanced gastric cancer | Nivolumab | 21% (13/62) |
| Kanjanapan, et al. 2019 [15] | Retrospective analysis of clinical trials | Canada, single center | 182 | Head and neck (18%), gynecological (16%), lung (15%), gastrointestinal (15%), genitourinary (12%), others (24%) | PD-1/PD-L1 inhibitors (89%), other checkpoint inhibitors (3%), or costimulatory molecules (8%) | 7% (12/182) |
| Tunali, et al. 2019 [16] | Retrospective analysis of clinical trials | USA, single center | 187 | NSCLC | PD-1/PD-L1 inhibitors | 8% (15/187) |
| Kim, et al. 2019 [17] | Retrospective cohort | Korea, single center | 263 | NSCLC | PD-1/PD-L1 inhibitors | 21% (54/263) |
| Study | Definition of HPD | Predictive Factors of HPD | Impact of HPD on Overall Survival | Impact of HPD on Progression-Free Survival |
|---|---|---|---|---|
| Champiat, et al. 2017 [9] | • RECIST-defined PD at first evaluation and TGRpost/TGRprea ≥ 2 | Advanced age of ≥ 65 years (p = 0.018) | HPD vs. complete response or partial response (HR 26, 95% CI 5.6–121, p < 0.0001) | NA |
| Kato, et al. 2017 [11] | • TGRpost/TGRprea ≥ 2 and > 50% increase in tumor burden and TTF < 2 months | EGFR mutation (p = 0.005), MDM2 mutation (p = 0.007) | NA | NA |
| Saada-Bouzid, et al. 2017 [10] | • TGKpost/TGKpreb ≥ 2 | Regional recurrence (p = 0.008) | HPD vs. non-HPD (6.1 vs. 8.1 months, p = 0.77) | HPD vs. non-HPD (2.5 vs. 3.4 months, p = 0.003) |
| Ferrara, et al. 2018 [12] | • RECIST-defined PD at first evaluation and TGRpost−TGRpre a > 50% | Number of metastatic sites > 2 (p = 0.006) | HPD vs. PD without HPD (HR 2.18, 95% CI 1.29–3.69, p = 0.03) | NA |
| Lo Russo, et al. 2019 [14] | • Fulfilling at least 3 of the following 5 criteria: 1) TTF < 2 months, 2) > 50% increase in the sum of target lesions major diameters between baseline and first radiologic evaluation, 3) appearance of at least two new lesions in an organ already involved between baseline and first radiologic evaluation, 4) spread of the disease to a new organ between baseline and first radiologic evaluation, 5) ECOG ≥ 2 during the first 2 months of treatment | NA | HPD vs. non-HPD (4.4 vs. 17.7 months) | NA |
| Sasaki, et al. 2019 [18] | • TGKpost/TGKpre b ≥ 2 and > 50% increase in tumor burden | ECOG performance status ≥ 1 (p = 0.003), liver metastases (p = 0.029), sum of the largest diameters of target lesions ≥ median (p = 0.003), absolute neutrophil count ≥ median (p = 0.002), neutrophil-to-lymphocyte ratio ≥ median (p = 0.008), C-reactive protein ≥ median (p = 0.006), serum LDH ≥ median (p = 0.006) | HPD vs. non-HPD (HR 9.16, 95% CI 3.72–22.6, p < 0.001) | HPD vs. non-HPD (HR 4.82, 95% CI 2.36–9.57, p < 0.001) |
| Kanjanapan, et al. 2019 [15] | • RECIST-defined PD at first evaluation and TGRpost/TGRpre a ≥ 2 | Female sex (p = 0.01) | HPD vs. non-HPD (HR 1.7, 95% CI 0.9–3.3, p = 0.11) | HPD vs. non-HPD (HR, 3.7, 95% CI 2.0–7.1, p < 0.001) |
| Tunali, et al. 2019 [16] | • RECIST-defined PD at first evaluation and TGRpost/TGRpre a ≥ 2 and TTF < 2 months | RMH prognostic score ≥ 2 (p = 0.003), higher serum LDH (p = 0.001) | HPD vs. PD without HPD (3.2 vs. 8.4 months, p < 0.001) | NA |
| Kim, et al. 2019 [17] | • RECIST-defined PD at first evaluation and TGRpost/TGRpre a ≥ 2 and TGKpost/TGKpre b ≥ 2 | Number of metastatic sites > 2 (p = 0.009), liver metastases (p < 0.001), serum LDH > upper normal limit (p = 0.013), RMH prognostic score ≥ 2 (p = 0.002) | HPD vs. PD without HPD (HR 5.71, 95% CI 3.14–8.23, p < 0.05) | HPD vs. PD without HPD (HR 4.62, 95% CI 2.87–7.44, p < 0.05) |
| Baseline Patient Characteristics | Number of Study Estimates | Number of HPD/Non-HPD Patients | Random-Effects Summary Estimate, Odds Ratio and 95% Confidence Interval a | p Value a | I2 | 95% Prediction Interval b | Egger p Value b | |
|---|---|---|---|---|---|---|---|---|
| Age ≥ 65 | 5 | 102/837 | 0.86 (0.56–1.32) | 0.49 | 0% | 0.43–1.73 | 0.25 | |
| Female sex | 7 | 155/856 | 1.34 (0.74–2.46) | 0.34 | 49% | 0.27–6.63 | 0.68 | |
| Smoking history | 5 | 174/859 | 0.78 (0.50–1.22) | 0.28 | 0% | 0.38–1.61 | 0.18 | |
| ECOG performance status ≥ 2 | 3 | 40/391 | 2.76 (0.83–9.13) | 0.096 | 52% | <0.01–690,014.13 | 0.70 | |
| ECOG performance status ≥ 1 | 3 | 149/672 | 1.14 (0.63–2.04) | 0.67 | 24% | 0.01–175.13 | 0.0075 | |
| Neutrophil-to-lymphocyte ratio ≤ 3 | 2 | 85/463 | 0.89 (0.55–1.43) | 0.62 | 0% | NA | NA | |
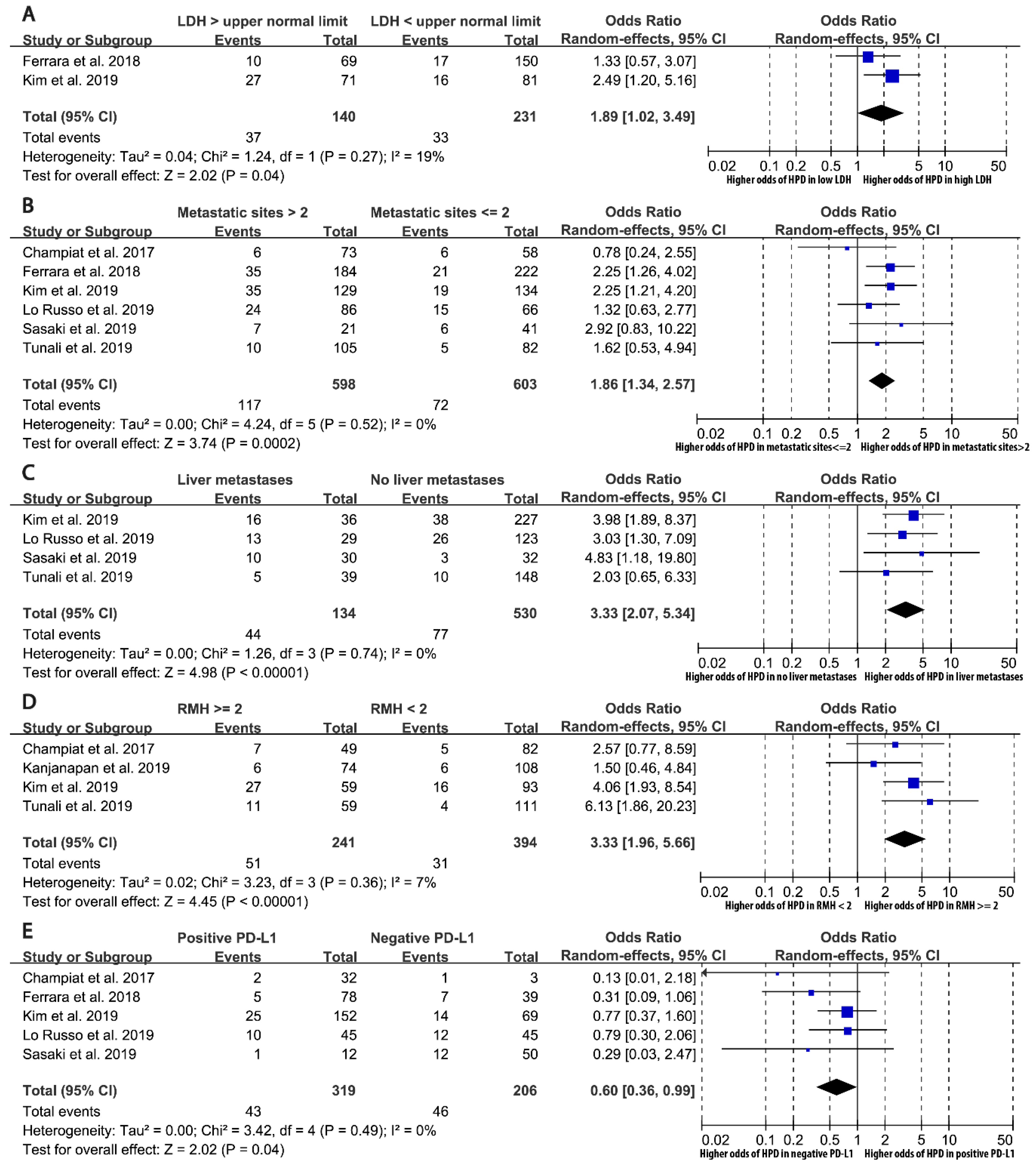
| Serum lactate dehydrogenase > upper normal limit | 2 | 70/301 | 1.89 (1.02–3.49) | 0.043 | 19% | NA | NA | |
| Number of metastatic sites > 2 | 6 | 189/1012 | 1.86 (1.34–2.57) | 0.00018 | 0% | 1.17–2.94 | 0.41 | |
| Liver metastases | 4 | 121/543 | 3.33 (2.07–5.34) | 0.00000064 | 0% | 1.18–9.40 | 0.86 | |
| RMH prognostic score ≥ 2 | 4 | 82/553 | 3.33 (1.96–5.66) | 0.0000086 | 7% | 0.88–12.58 | 0.64 | |
| PD-L1 positive | 5 | 89/436 | 0.60 (0.36–0.99) | 0.044 | 0% | 0.26–1.35 | 0.056 | |
| PD-1 inhibitor vs. PD-L1 inhibitor | 6 | 182/913 | 1.22 (0.76–1.94) | 0.41 | 0% | 0.63–2.36 | 0.33 | |
| Combination therapy vs. monotherapy | 3 | 107/632 | 1.98 (0.46–8.57) | 0.36 | 67% | <0.01-27,517,080.41 | 0.77 | |
| Previous treatment lines > 2 | 4 | 162/721 | 1.17 (0.81–1.68) | 0.40 | 7% | 0.47–2.91 | 0.49 | |
| Previous chemotherapy | 4 | 137/850 | 1.14 (0.72–1.81) | 0.58 | 3% | 0.38–3.40 | 0.18 | |
| Previous radiotherapy | 5 | 106/714 | 0.77 (0.33–1.83) | 0.56 | 0% | 0.19–3.14 | 0.44 | |
| Previous targeted therapy | 4 | 137/850 | 1.40 (0.84–2.32) | 0.20 | 1% | 0.45–4.34 | 0.90 | |
| Previous immunotherapy | 2 | 68/469 | 2.25 (0.67–7.56) | 0.19 | 0% | NA | NA | |
| Previous corticosteroid | 2 | 27/291 | 1.92 (0.67–5.49) | 0.23 | 0% | NA | NA | |
| NSCLC | EGFR mutation | 5 | 136/759 | 1.29 (0.48–3.52) | 0.61 | 37% | 0.09–19.35 | 0.57 |
| KRAS mutation | 2 | 46/197 | 0.59 (0.19–1.83) | 0.36 | 0% | NA | NA | |
| ALK rearrangement | 3 | 121/538 | 2.86 (0.65–12.52) | 0.16 | 0% | <0.01–41,535.21 | 0.15 | |
| Squamous histology | 4 | 164/844 | 0.87 (0.58–1.31) | 0.50 | 10% | 0.30–2.53 | 0.82 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.Y.; Lee, K.H.; Kang, J.; Borcoman, E.; Saada-Bouzid, E.; Kronbichler, A.; Hong, S.H.; de Rezende, L.F.M.; Ogino, S.; Keum, N.; et al. Hyperprogressive Disease during Anti-PD-1 (PDCD1) / PD-L1 (CD274) Therapy: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1699. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11111699
Kim JY, Lee KH, Kang J, Borcoman E, Saada-Bouzid E, Kronbichler A, Hong SH, de Rezende LFM, Ogino S, Keum N, et al. Hyperprogressive Disease during Anti-PD-1 (PDCD1) / PD-L1 (CD274) Therapy: A Systematic Review and Meta-Analysis. Cancers. 2019; 11(11):1699. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11111699
Chicago/Turabian StyleKim, Jong Yeob, Keum Hwa Lee, Jeonghyun Kang, Edith Borcoman, Esma Saada-Bouzid, Andreas Kronbichler, Sung Hwi Hong, Leandro Fórnias Machado de Rezende, Shuji Ogino, Nana Keum, and et al. 2019. "Hyperprogressive Disease during Anti-PD-1 (PDCD1) / PD-L1 (CD274) Therapy: A Systematic Review and Meta-Analysis" Cancers 11, no. 11: 1699. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11111699