Switching to Immune Checkpoint Inhibitors upon Response to Targeted Therapy; The Road to Long-Term Survival in Advanced Melanoma Patients with Highly Elevated Serum LDH?


 ,
,
Abstract
:1. Introduction
2. Results
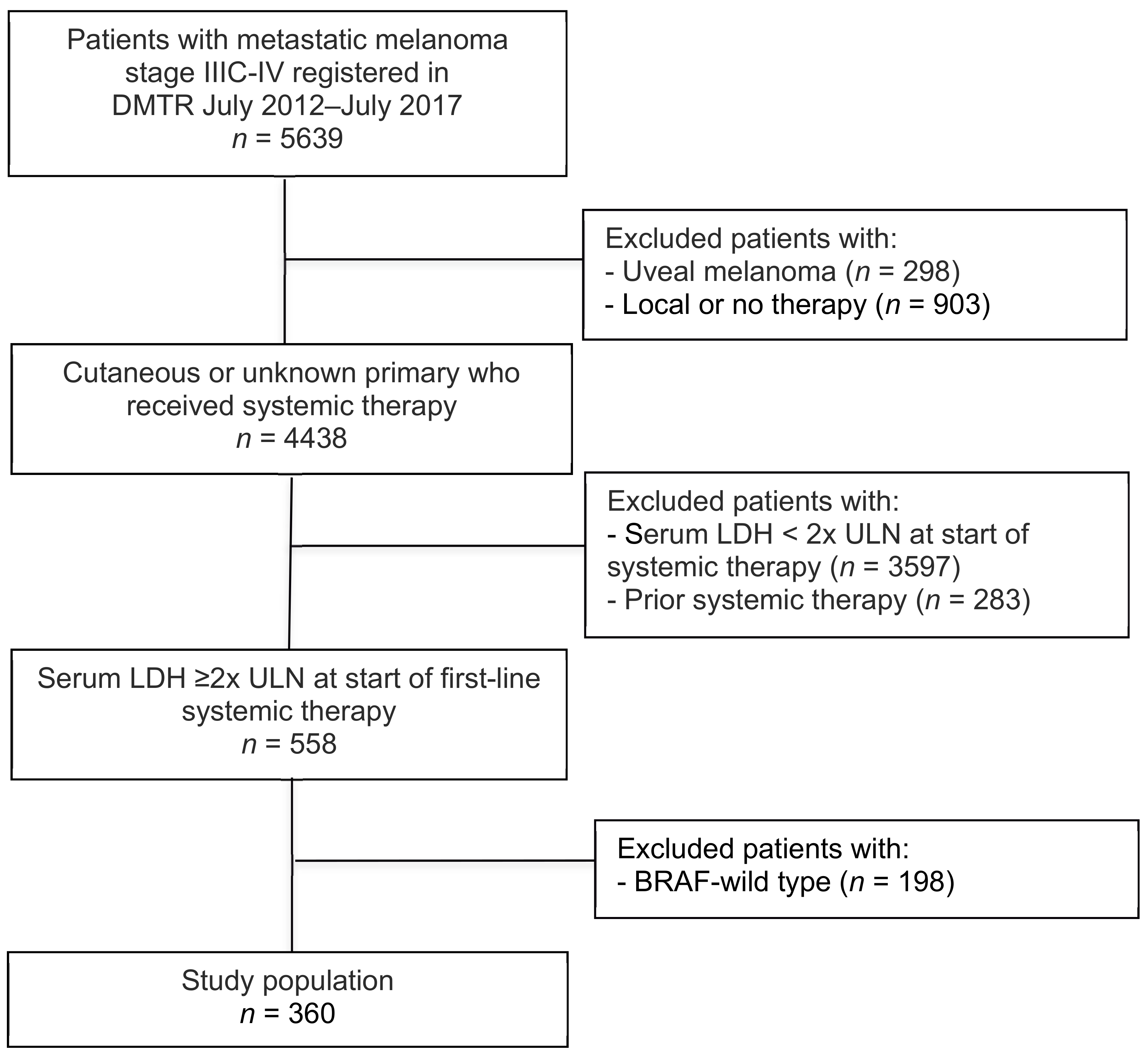
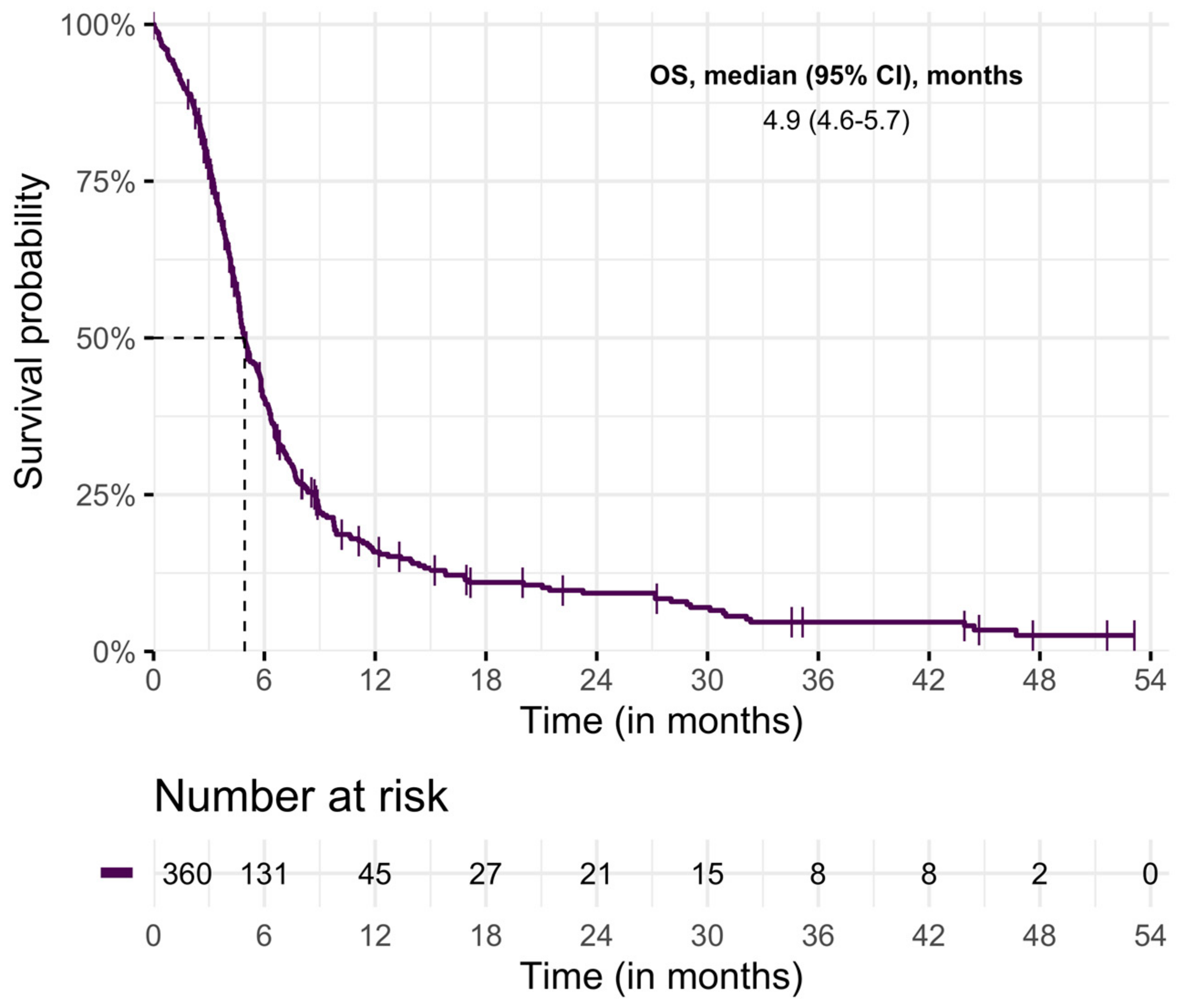
2.1. Overall Study Population
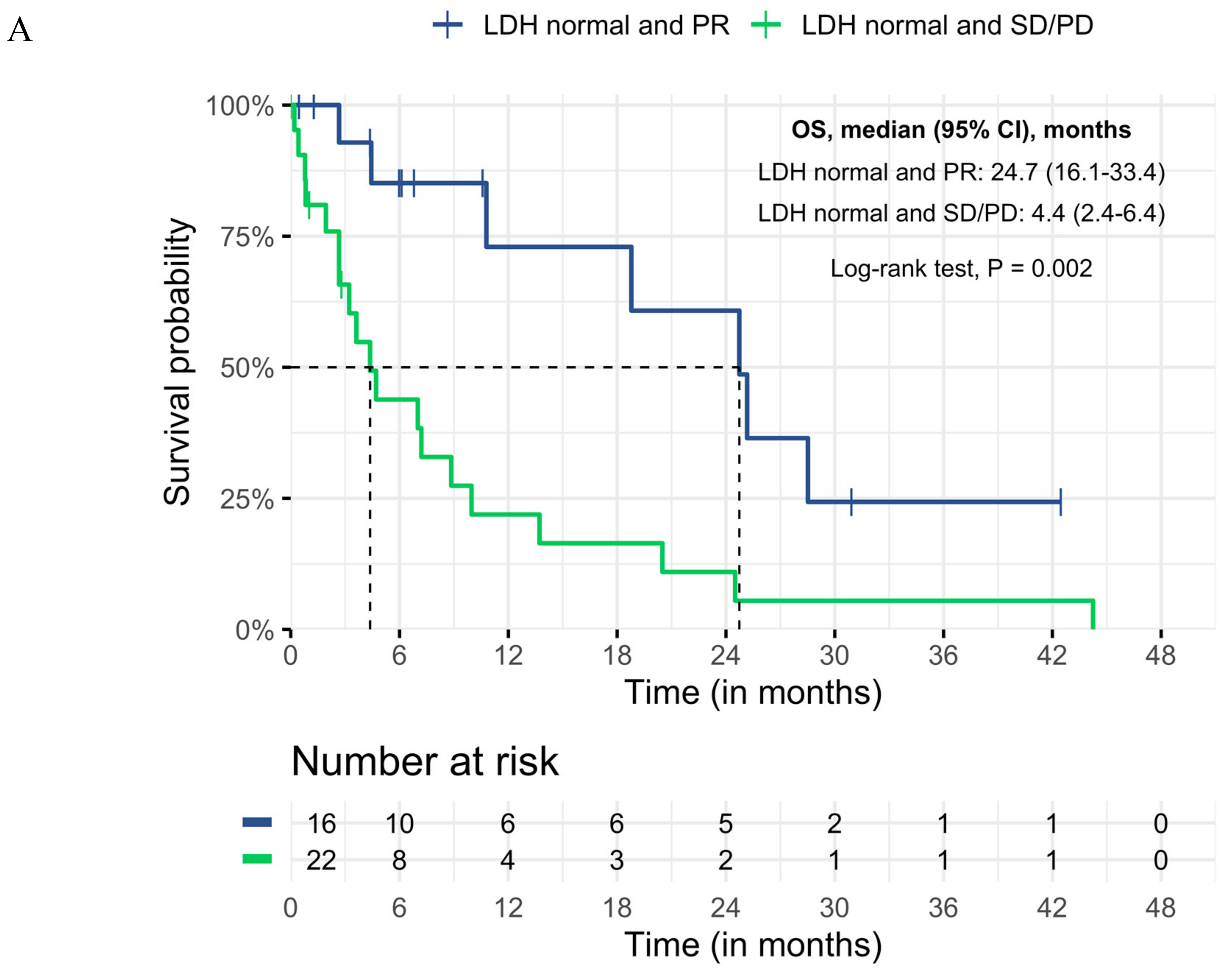
2.2. Patients with Subsequent Treatment with ICI
3. Discussion
4. Materials and Methods
4.1. Data: The Dutch Melanoma Treatment Registry (DMTR)
4.2. Patients
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chapman, P.B.; Hauschild, A.; Robert, C.; Haanen, J.B.; Ascierto, P.; Larkin, J.; Dummer, R.; Garbe, C.; Testori, A.; Maio, M.; et al. Improved Survival with Vemurafenib in Melanoma with BRAF V600E Mutation for the BRIM-3 Study Group. N. Engl. J. Med. 2011, 364, 2507–2516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved Overall Survival in Melanoma with Combined Dabrafenib and Trametinib. N. Engl. J. Med. 2014, 372, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in Previously Untreated Melanoma without BRAF Mutation. N. Engl. J. Med. 2015. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2017. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.J.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Factors predictive of response, disease progression, and overall survival after dabrafenib and trametinib combination treatment: A pooled analysis of individual patient data from randomised trials. Lancet Oncol. 2016, 1743–1754. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.J.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Durable Complete Response After Discontinuation of Pembrolizumab in Patients With Metastatic Melanoma. J. Clin. Oncol. 2018. [Google Scholar] [CrossRef]
- Kelderman, S.; Heemskerk, B.; van Tinteren, H.; van den Brom, R.R.; Hospers, G.A.; van den Eertwegh, A.J.; Kapiteijn, E.W.; de Groot, J.W.; Soetekouw, P.; Jansen, R.L.; et al. Lactate dehydrogenase as a selection criterion for ipilimumab treatment in metastatic melanoma. Cancer Immunol. Immunother. 2014, 449–458. [Google Scholar] [CrossRef]
- Weide, B.; Martens, A.; Hassel, J.C.; Berking, C.; Postow, M.A.; Bisschop, K.; Simeone, E.; Mangana, J.; Schilling, B.; Di Giacomo, A.M.; et al. Baseline Biomarkers for Outcome of Melanoma Patients Treated with Pembrolizumab. Clin. Cancer Res. 2016, 5487–5496. [Google Scholar] [CrossRef] [Green Version]
- Long, G.V.; Eroglu, Z.; Infante, J.; Patel, S.; Daud, A.; Johnson, D.B.; Gonzalez, R.; Kefford, R.; Hamid, O.; Schuchter, L.; et al. Long-Term Outcomes in Patients With BRAF V600—Mutant Metastatic Melanoma Who Received Dabrafenib Combined with Trametinib. J. Clin. Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Y.; Menzies, A.M.; Rizos, H. Mechanisms and Strategies to Overcome Resistance to Molecularly Targeted Therapy for Melanoma. Cancer 2017, 123, 2118–2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, S.D.; Chen, Z.; Melendez, B.; Talukder, A.; Khalili, J.S.; Rodriguez-Cruz, T.; Liu, S.; Whittington, M.; Deng, W.; Li, F.; et al. BRAF V600E Co-opts a Conserved MHC Class I Internalization Pathway to Diminish Antigen Presentation and CD8 þ T-cell Recognition of Melanoma. Cancer Immunol. Res. 2015, 3, 602–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diem, S.; Kasenda, B.R.; Gore, M.J. Serum lactate dehydrogenase as an early marker for outcome in patients treated with anti-PD-1 therapy in metastatic melanoma. Br. J. Cancer 2016, 114, 256–261. [Google Scholar] [CrossRef]
- Schadendorf, D.; Long, G.V.; Stroiakovski, D.; Karaszewska, B.; Hauschild, A.; Levchenko, E.; Chiarion-Sileni, V.; Schachter, J.; Garbe, C.; Dutriaux, C.; et al. Inhibitory effect of tumor cell—Derived lactic acid on human T cells. Blood 2018, 109, 3812–3820. [Google Scholar] [CrossRef]
- Blank, C.U.; Angeles, L.; Khersonsky, O.; Fleishman, S.J. The cancer immunogram. Science 2016, 352, 658–660. [Google Scholar] [CrossRef]
- Schadendorf, D.; Long, G.V.; Stroiakovski, D.; Karaszewska, B.; Hauschild, A.; Levchenko, E.; Chiarion-Sileni, V.; Schachter, J.; Garbe, C.; Dutriaux, C.; et al. Three-year pooled analysis of factors associated with clinical outcomes across dabrafenib and trametinib combination therapy phase 3 randomised trials. Eur. J. Cancer 2017, 82, 45–55. [Google Scholar] [CrossRef]
- Seifert, H.; Fisher, R.; Martin-Liberal, J.; Edmonds, K.; Hughes, P.; Khabra, K.; Gore, M.; Larkin, J. Prognostic markers and tumour growth kinetics in melanoma patients progressing on vemurafenib. Melanoma Res. 2016, 26, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Ascierto, P.A.; Simeone, E.; Giannarelli, D.; Grimaldi, A.M.; Romano, A.; Mozzillo, N. Sequencing of BRAF inhibitors and ipilimumab in patients with metastatic melanoma: A possible algorithm for clinical use. J. Transl. Med. 2012, 10, 107. [Google Scholar] [CrossRef] [Green Version]
- Ascierto, P.A.; Simeone, E.; Sileni, V.C.; Del Vecchio, M.; Marchetti, P.; Cappellini, G.C.; Ridolfi, R.; de Rosa, F.; Cognetti, F.; Ferraresi, V.; et al. Sequential Treatment with Ipilimumab and BRAF Inhibitors in Patients With Metastatic Melanoma: Data From the Italian Cohort of the Ipilimumab Expanded Access Program. Cancer Investig. 2017, 32, 144–149. [Google Scholar] [CrossRef]
- Jochems, A.; Schouwenburg, M.G.; Leeneman, B.; Franken, M.G.; van den Eertwegh, A.J.; Haanen, J.B.; Gelderblom, H.; Uyl-de Groot, C.A.; Aarts, M.J.; van den Berkmortel, F.W.; et al. ScienceDirect Dutch Melanoma Treatment Registry: Quality assurance in the care of patients with metastatic melanoma in the Netherlands. Eur. J. Cancer 2017, 72, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n = 360 |
|---|---|
| n (%) | |
| Median age, years (IQR) | 60 (50–68) |
| Age in categories | |
| <50 | 90 (25) |
| 50–59 | 85 (23) |
| 60–69 | 110 (31) |
| ≥70 | 75 (21) |
| Gender | |
| Male | 214 (60) |
| Female | 146 (40) |
| ECOG PS | |
| 0 | 75 (21) |
| 1 | 110 (31) |
| ≥2 | 136 (38) |
| Unknown | 39 (10) |
| Median baseline LDH (IQR) | 823 (625–1419) |
| No. of organ sites involved | |
| <3 | 60 (17) |
| ≥3 | 261 (72) |
| Unknown | 39 (11) |
| M stage | |
| M1a | 6 (2) |
| M1b | 3 (1) |
| M1c | 349 (96) |
| Unknown | 2 (1) |
| Brain metastases | |
| No | 231 (64) |
| Asymptomatic | 42 (12) |
| Symptomatic | 63 (17) |
| Unknown | 24 (7) |
| Type of targeted therapy | |
| BRAFi monotherapy | 206 (76) |
| BRAFi + MEKi | 154 (24) |
| Variable | n = 113 |
|---|---|
| n (%) | |
| Median age, years (min–max) | 56 (47–67) |
| Age in categories | |
| <50 | 35 (31) |
| 50–59 | 28 (25) |
| 60–69 | 30 (26) |
| ≥70 | 20 (18) |
| Gender | |
| Male | 69 (61) |
| Female | 44 (39) |
| Serum LDH | |
| <ULN | 38 (34) |
| ≥1 to <2× ULN | 42 (37) |
| ≥2× ULN | 33 (29) |
| ECOG PS | |
| 0 | 24 (21) |
| 1 | 61 (54) |
| ≥2 | 15 (13) |
| Unknown | 13 (12) |
| No. of organ sites involved | |
| <3 | 17 (15) |
| ≥3 | 84 (74) |
| Unknown | 12 (11) |
| M stage | |
| M1a | 0 (0) |
| M1b | 0 (0) |
| M1c | 113 (100) |
| Unknown | 0 (0) |
| Brain metastases | |
| No | 68 (60) |
| Asymptomatic | 18 (16) |
| Symptomatic | 19 (17) |
| Unknown | 8 (7) |
| Type of prior targeted therapy | |
| BRAFi monotherapy | 41 (36) |
| BRAFi + MEKi | 72 (64) |
| Response on targeted therapy | |
| Partial response | 27 (24) |
| Stable disease | 7 (6) |
| Progressive disease | 79 (70) |
| Type of subsequent ICI | |
| Ipilimumab | 22 (19) |
| Nivolumab | 16 (14) |
| Pembrolizumab | 20 (18) |
| Ipilimumab and nivolumab | 55 (49) |
| Serum LDH at Start ICI | Response on Targeted Therapy | Deaths/No. of Patients | Median OS | 6 m Survival Rate | 1 y Survival Rate |
|---|---|---|---|---|---|
| (95% CI), m | (95% CI), % | (95% CI), % | |||
| <ULN | |||||
| PR | 7/16 | 24.7 (16.1–33.4) | 85 (66–100) | 73 (46–100) | |
| SD | 5/6 | 7.0 (0–14.9) | 63 (21–100) | 21 (0–57) | |
| PD | 14/16 | 4.4 (1.3–7.4) | 36 (11–61) | 22 (0–44) | |
| ≥1 to <2× ULN a | |||||
| PR | 5/9 | 10.4 (0–22.5) | 60 (24–96) | 40 (0–80) | |
| PD | 25/32 | 2.7 (1.9–3.5) | 24 (8–40) | 20 (5–35) | |
| ≥2× ULN b | |||||
| PD | 29/31 | 1.1 (0.7–1.6) | 17 (3–30) | 8 (0–19) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schouwenburg, M.G.; Suijkerbuijk, K.P.M.; Koornstra, R.H.T.; Jochems, A.; van Zeijl, M.C.T.; van den Eertwegh, A.J.M.; Haanen, J.B.A.G.; Aarts, M.J.B.; van Akkooi, A.C.J.; van den Berkmortel, F.W.P.J.; et al. Switching to Immune Checkpoint Inhibitors upon Response to Targeted Therapy; The Road to Long-Term Survival in Advanced Melanoma Patients with Highly Elevated Serum LDH? Cancers 2019, 11, 1940. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11121940
Schouwenburg MG, Suijkerbuijk KPM, Koornstra RHT, Jochems A, van Zeijl MCT, van den Eertwegh AJM, Haanen JBAG, Aarts MJB, van Akkooi ACJ, van den Berkmortel FWPJ, et al. Switching to Immune Checkpoint Inhibitors upon Response to Targeted Therapy; The Road to Long-Term Survival in Advanced Melanoma Patients with Highly Elevated Serum LDH? Cancers. 2019; 11(12):1940. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11121940
Chicago/Turabian StyleSchouwenburg, Maartje G., Karijn P.M. Suijkerbuijk, Rutger H.T. Koornstra, Anouk Jochems, Michiel C.T. van Zeijl, Alfons J.M. van den Eertwegh, John B.A.G. Haanen, Maureen J.B. Aarts, Alexander C.J. van Akkooi, Franchette W.P.J. van den Berkmortel, and et al. 2019. "Switching to Immune Checkpoint Inhibitors upon Response to Targeted Therapy; The Road to Long-Term Survival in Advanced Melanoma Patients with Highly Elevated Serum LDH?" Cancers 11, no. 12: 1940. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11121940