Early Tumor Shrinkage as a Predictive Factor for Outcomes in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Multicenter Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
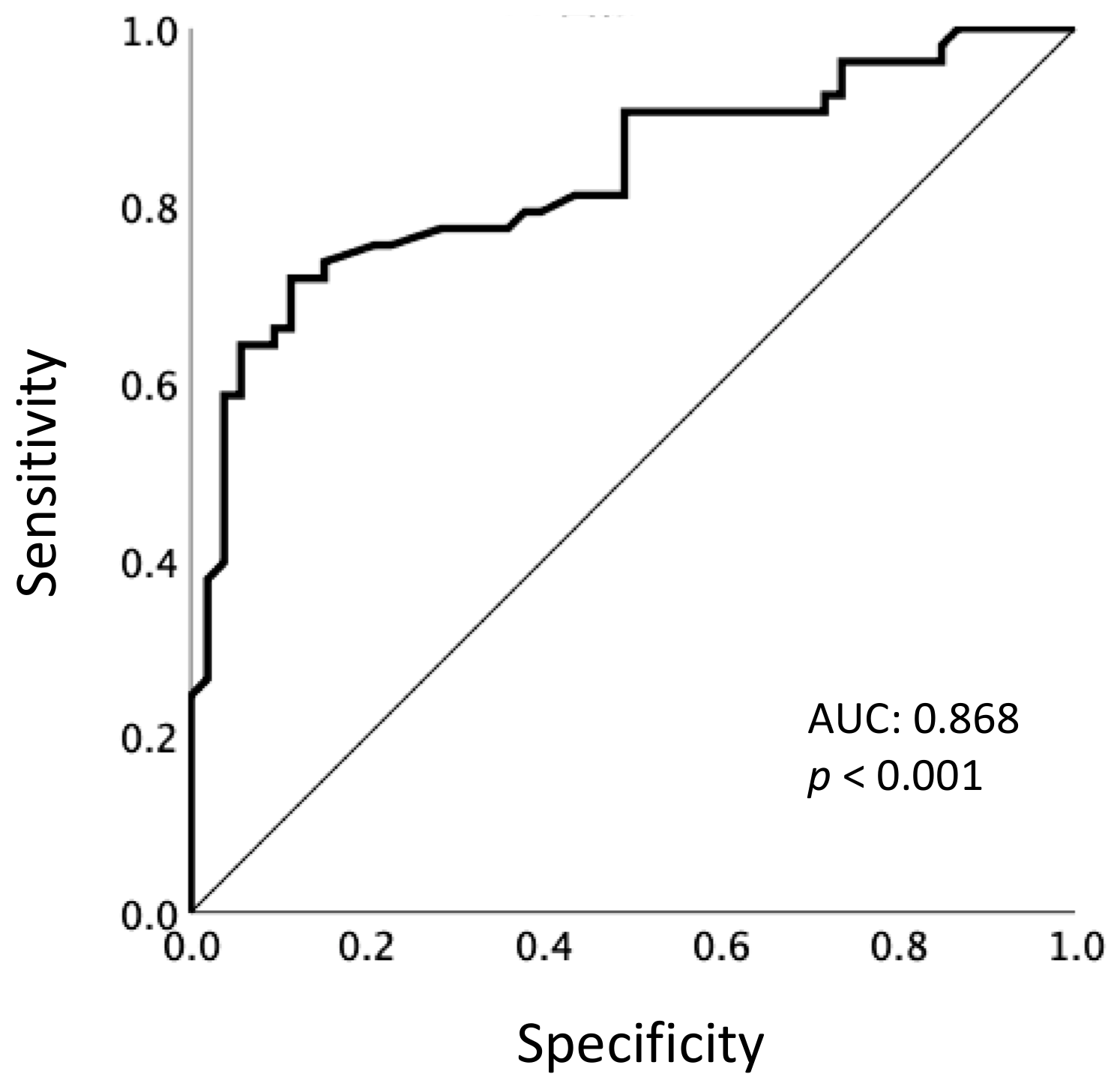
2.2. Definition of Early Tumor Shrinkage
2.3. Correlation of Early Tumor Shrinkage with AFP Response and Relative Dose Intensity
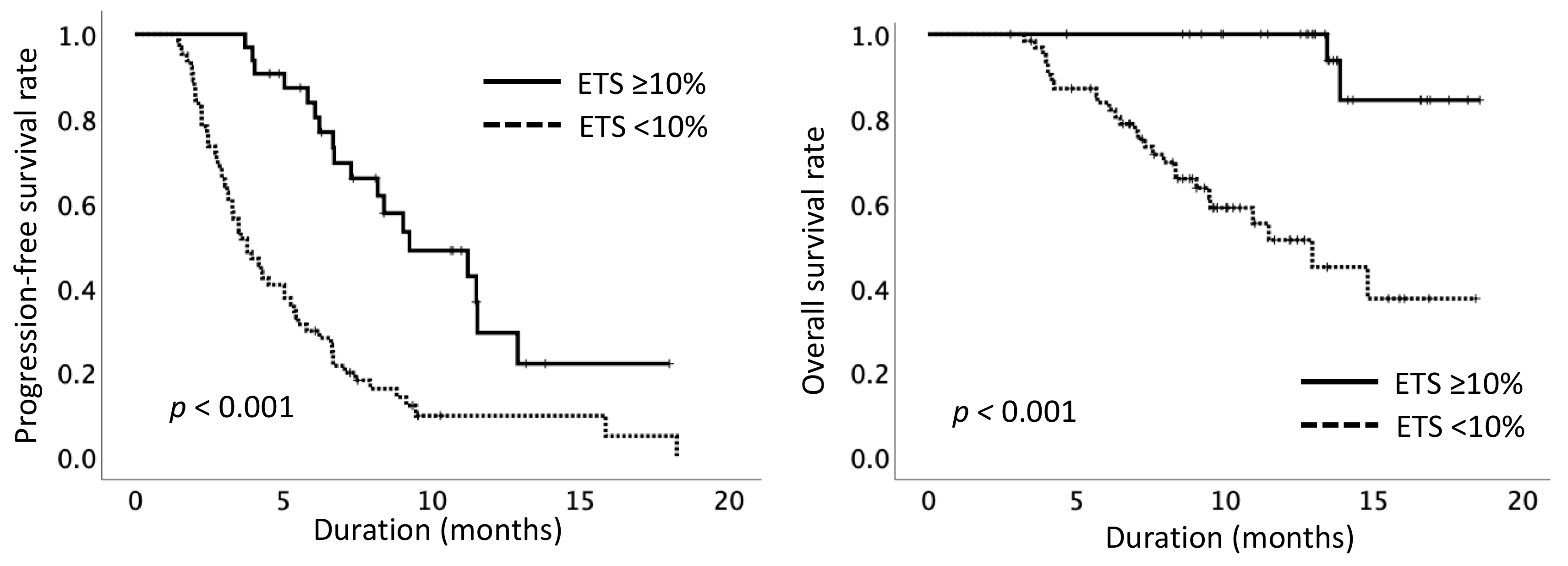
2.4. Treatment Outcome Based on Early Tumor Shrinkage
2.5. Comparison of Early Tumor Shrinkage with Modified RECIST/RECIST-Based Objective Response
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Diagnosis and Treatment
4.3. Assessments
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2016, 2, 16019. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Kang, Y.-K.; Yen, C.-J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lonardi, S.; Masi, G.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Spadi, R.; Zaniboni, A.; et al. Early tumor shrinkage and depth of response predict long-term outcome in metastatic colorectal cancer patients treated with first-line chemotherapy plus bevacizumab: Results from phase III TRIBE trial by the Gruppo Oncologico del Nord Ovest. Ann. Oncol. 2015, 26, 1188–1194. [Google Scholar] [CrossRef]
- Heinemann, V.; Modest, D.; Von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.-E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; et al. Independent Radiological Evaluation of Objective Response Early Tumor Shrinkage, and Depth of Response in FIRE-3 (AIO KRK-0306). Ann. Oncol. 2014, 25, ii117. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, V.; Stintzing, S.; Modest, D.P.; Gießen-Jung, C.; Michl, M.; Mansmann, U. Early tumour shrinkage (ETS) and depth of response (DpR) in the treatment of patients with metastatic colorectal cancer (mCRC). Eur. J. Cancer 2015, 51, 1927–1936. [Google Scholar] [CrossRef]
- Vivaldi, C.; Fornaro, L.; Cappelli, C.; Pecora, I.; Catanese, S.; Salani, F.; Insilla, A.C.; Kauffmann, E.F.; Donati, F.; Pasquini, G.; et al. Early Tumor Shrinkage and Depth of Response Evaluation in Metastatic Pancreatic Cancer Treated with First Line Chemotherapy: An Observational Retrospective Cohort Study. Cancers 2019, 11, 939. [Google Scholar] [CrossRef] [Green Version]
- Miyake, H.; Miyazaki, A.; Imai, S.; Harada, K.-I.; Fujisawa, M. Early Tumor Shrinkage Under Treatment with First-line Tyrosine Kinase Inhibitors as a Predictor of Overall Survival in Patients with Metastatic Renal Cell Carcinoma: A Retrospective Multi-Institutional Study in Japan. Target. Oncol. 2015, 11, 175–182. [Google Scholar] [CrossRef]
- Kawachi, H.; Fujimoto, D.; Morimoto, T.; Hosoya, K.; Sato, Y.; Kogo, M.; Nagata, K.; Nakagawa, A.; Tachikawa, R.; Tomii, K. Early depth of tumor shrinkage and treatment outcomes in non-small cell lung cancer treated using Nivolumab. Investig. New Drugs 2019, 37, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; Van Oosterom, A.T.; Christian, M.C.; et al. New Guidelines to Evaluate the Response to Treatment in Solid Tumors. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Cheng, A.-L.; Piscaglia, F.; Ueshima, K.; Aikata, H.; Vogel, A.; et al. Analysis of survival and objective response (OR) in patients with hepatocellular carcinoma in a phase III study of lenvatinib (REFLECT). J. Clin. Oncol. 2019, 37, 186. [Google Scholar] [CrossRef]
- Takahashi, A.; Moriguchi, M.; Seko, Y.; Ishikawa, H.; Yo, T.; Kimura, H.; Fujii, H.; Shima, T.; Mitsumoto, Y.; Ishiba, H.; et al. Impact of Relative Dose Intensity of Early-phase Lenvatinib Treatment on Therapeutic Response in Hepatocellular Carcinoma. Anticancer. Res. 2019, 39, 5149–5156. [Google Scholar] [CrossRef]
- Bruix, J.; Cheng, A.-L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J.M. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Pena, C.E.A.; Lathia, C.D.; Shan, M.; Meinhardt, G.; Bruix, J. Plasma Biomarkers as Predictors of Outcome in Patients with Advanced Hepatocellular Carcinoma. Clin. Cancer Res. 2012, 18, 2290–2300. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, T.; Kudo, M.; Ikeda, K.; Izumi, N.; Tateishi, R.; Ikeda, M.; Aikata, H.; Kawaguchi, Y.; Wada, Y.; Numata, K.; et al. REFLECT—A phase 3 trial comparing efficacy and safety of lenvatinib to sorafenib for the treatment of unresectable hepatocellular carcinoma: An analysis of Japanese subset. J. Gastroenterol. 2019, 55, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Eso, Y.; Nakano, S.; Mishima, M.; Arasawa, S.; Iguchi, E.; Nakamura, F.; Takeda, H.; Takai, A.; Takahashi, K.; Taura, K.; et al. Dose Intensity/Body Surface Area Ratio is a Novel Marker Useful for Predicting Response to Lenvatinib against Hepatocellular Carcinoma. Cancers 2019, 12, 49. [Google Scholar] [CrossRef] [Green Version]
- Hatanaka, T.; Kakizaki, S.; Nagashima, T.; Namikawa, M.; Tojima, H.; Shimada, Y.; Takizawa, D.; Naganuma, A.; Arai, H.; Sato, K.; et al. Analyses of objective response rate, progression-free survival, and adverse events in hepatocellular carcinoma patients treated with lenvatinib: A multicenter retrospective study. Hepatol. Res. 2019, 50, 382–395. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Prognostic factor of lenvatinib for unresectable hepatocellular carcinoma in real-world conditions-Multicenter analysis. Cancer Med. 2019, 8, 3719–3728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazard, T.; Boonsirikamchai, P.; Overman, M.; Asran, M.A.; Choi, H.; Herron, D.; Eng, C.; Maru, D.; Ychou, M.; Vauthey, J.-N.; et al. Comparison of early radiological predictors of outcome in patients with colorectal cancer with unresectable hepatic metastases treated with bevacizumab. Gut 2017, 67, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Terashima, T.; Yamashita, T.; Takata, N.; Nakagawa, H.; Toyama, T.; Arai, K.; Kitamura, K.; Yamashita, T.; Sakai, Y.; Mizukoshi, E.; et al. Post-progression survival and progression-free survival in patients with advanced hepatocellular carcinoma treated by sorafenib. Hepatol. Res. 2015, 46, 650–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogasawara, S.; Chiba, T.; Ooka, Y.; Suzuki, E.; Kanogawa, N.; Saito, T.; Motoyama, T.; Tawada, A.; Kanai, F.; Yokosuka, O. Post-progression survival in patients with advanced hepatocellular carcinoma resistant to sorafenib. Investig. New Drugs 2016, 34, 255–260. [Google Scholar] [CrossRef]
- Kuzuya, T.; Ishigami, M.; Ishizu, Y.; Honda, T.; Hayashi, K.; Ishikawa, T.; Nakano, I.; Hirooka, Y.; Goto, H. Prognostic Factors Associated with Postprogression Survival in Advanced Hepatocellular Carcinoma Patients Treated with Sorafenib Not Eligible for Second-Line Regorafenib Treatment. Oncology 2018, 95, 91–99. [Google Scholar] [CrossRef]
- Lencioni, R.; Montal, R.; Torres, F.; Park, J.-W.; Decaens, T.; Raoul, J.-L.; Kudo, M.; Chang, C.; Ríos, J.; Boige, V.; et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J. Hepatol. 2017, 66, 1166–1172. [Google Scholar] [CrossRef] [Green Version]
- Meyer, T.; Palmer, D.H.; Cheng, A.-L.; Hocke, J.; Loembé, A.; Yen, C. mRECIST to predict survival in advanced hepatocellular carcinoma: Analysis of two randomised phase II trials comparing nintedanib vs sorafenib. Liver Int. 2017, 37, 1047–1055. [Google Scholar] [CrossRef] [Green Version]
- Takeda, H.; Nishijima, N.; Nasu, A.; Komekado, H.; Kita, R.; Kimura, T.; Kudo, M.; Osaki, Y. Long-term antitumor effect of lenvatinib on unresectable hepatocellular carcinoma with portal vein invasion. Hepatol. Res. 2019, 49, 594–599. [Google Scholar] [CrossRef]
- Kuzuya, T.; Ishigami, M.; Ito, T.; Ishizu, Y.; Honda, T.; Ishikawa, T.; Fujishiro, M. Favorable radiological antitumor response at 2 weeks after starting lenvatinib for patients with advanced hepatocellular carcinoma. Hepatol. Res. 2019, 50, 374–381. [Google Scholar] [CrossRef]
- Ueshima, K.; Nishida, N.; Hagiwara, S.; Aoki, T.; Minami, T.; Chishina, H.; Takita, M.; Minami, Y.; Ida, H.; Takenaka, M.; et al. Impact of Baseline ALBI Grade on the Outcomes of Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Multicenter Study. Cancers 2019, 11, 952. [Google Scholar] [CrossRef] [Green Version]
- Kodama, K.; Kawaoka, T.; Namba, M.; Uchikawa, S.; Ohya, K.; Morio, K.; Nakahara, T.; Murakami, E.; Yamauchi, M.; Hiramatsu, A.; et al. Correlation between Early Tumor Marker Response and Imaging Response in Patients with Advanced Hepatocellular Carcinoma Treated with Lenvatinib. Oncology 2019, 97, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, R.; Fukushima, M.; Haraguchi, M.; Miuma, S.; Miyaaki, H.; Hidaka, M.; Eguchi, S.; Matsuo, S.; Tajima, K.; Matsuzaki, T.; et al. Response to Lenvatinib Is Associated with Optimal RelativeDose Intensity in Hepatocellular Carcinoma: Experience in Clinical Settings. Cancers 2019, 11, 1769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arizumi, T.; Ueshima, K.; Chishina, H.; Kono, M.; Takita, M.; Kitai, S.; Inoue, T.; Yada, N.; Hagiwara, S.; Minami, Y.; et al. Duration of Stable Disease Is Associated with Overall Survival in Patients with Advanced Hepatocellular Carcinoma Treated with Sorafenib. Dig. Dis. 2014, 32, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Tsuji, K.; Takaguchi, K.; Itobayashi, E.; Kariyama, K.; Ochi, H.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Validation of Modified ALBI Grade for More Detailed Assessment of Hepatic Function in Hepatocellular Carcinoma Patients: A Multicenter Analysis. Liver Cancer 2018, 8, 121–129. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Pencina, M.J.; D’Agostino, R.B. OverallC as a measure of discrimination in survival analysis: Model specific population value and confidence interval estimation. Stat. Med. 2004, 23, 2109–2123. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 104) | ETS ≥ 10% (n = 32) | ETS < 10% (n = 72) | p‡ |
|---|---|---|---|---|
| Age, years (range) | 74 (48–93) | 71 (53–91) | 75 (48–93) | 0.510 |
| Sex, male/female | 77/27 | 26/6 | 51/21 | 0.336 |
| ECOG PS, 0/1/2 | 80/20/4 | 26/5/1 | 54/15/3 | 0.831 |
| Body weight, kg (range) | 57.7 (38.0–103.0) | 58.8 (41.5–90.0) | 57.3 (38.0–103.0) | 0.938 |
| Etiology, HCV/HBV/alcohol/others | 40/17/20/27 | 14/5/5/8 | 26/12/15/19 | 0.294 |
| Child–Pugh score, 5/6/7 | 59/36/9 | 23/6/3 | 36/30/6 | 0.055 |
| Maximum diameter of lesions, mm | 34.5 (10–125) | 28.0 (10–124) | 37.3 (10–125) | 0.012 |
| Number of lesions, <5/≥5 | 54/50 | 21/11 | 33/39 | 0.062 |
| EHS, +/− | 42/62 | 13/19 | 29/43 | 1.000 |
| MVI, +/− | 18/86 | 4/28 | 14/58 | 0.575 |
| BCLC stage, A/B/C | 3/38/63 | 1/12/19 | 2/26/44 | 0.984 |
| AFP, ng/mL (range) | 94.3 (1.2–185772) | 113.2 (2.8–25881) | 92.5 (1.2–185772) | 0.404 |
| 1st/2nd/3rd line | 72/19/13 | 23/7/2 | 49/12/11 | 0.403 |
| Initial dose of LEN, full dose/reduced dose | 85/19 | 29/3 | 56/16 | 0.171 |
| Variable | ETS ≥ 10% (n = 32) | ETS < 10% (n = 72) | p‡ |
|---|---|---|---|
| AFP ratio at 8 weeks, <1.1/≥1.1 | 25/7 | 39/33 | 0.028 |
| RDI at 8 weeks, ≥70%/<70% | 23/9 | 31/42 | 0.010 |
| Factors | Univariate Analysis | Multivariate Analysis † | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p‡ | HR | 95% CI | p‡ | |
| Age, <75 years | 0.688 | 0.440–1.076 | 0.102 | |||
| Gender, male | 0.635 | 0.390–1.034 | 0.068 | |||
| ECOG-PS, 0 | 0.721 | 0.433–1.203 | 0.211 | |||
| Child-Pugh score, 5 | 0.617 | 0.398–0.958 | 0.031 | 0.885 | 0.556–1.410 | 0.608 |
| Maximum diameter of lesions, <35 mm | 0.780 | 0.506–1.201 | 0.259 | |||
| Number of lesions, <5 | 0.650 | 0.420–1.003 | 0.052 | |||
| EHS, absence | 0.841 | 0.541–1.307 | 0.441 | |||
| MVI, absence | 0.842 | 0.481–1.475 | 0.547 | |||
| AFP, <200 ng/mL | 0.552 | 0.357–0.855 | 0.008 | 0.476 | 0.299–0.759 | 0.004 |
| AFP ratio at 8 weeks, <1.1 | 0.641 | 0.412–0.997 | 0.049 | 0.912 | 0.569–1.462 | 0.702 |
| RDI at 8 weeks, ≥70% | 0.618 | 0.401–0.953 | 0.030 | 0.763 | 0.484–1.205 | 0.246 |
| ETS, ≥10% | 0.275 | 0.161–0.469 | <0.001 | 0.275 | 0.157–0.483 | <0.001 |
| Factors | Univariate Analysis | Multivariate Analysis † | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p‡ | HR | 95% CI | p‡ | |
| Age, <75 years | 0.598 | 0.305–1.169 | 0.133 | |||
| Gender, male | 0.575 | 0.286–1.158 | 0.122 | |||
| ECOG-PS, 0 | 0.623 | 0.304–1.274 | 0.195 | |||
| Child-Pugh score, 5 | 0.403 | 0.205–0.794 | 0.009 | 0.424 | 0.199–0.902 | 0.026 |
| Maximum diameter of lesions, <35 mm | 0.593 | 0.304–1.156 | 0.125 | |||
| Number of lesions, <5 | 0.443 | 0.220–0.891 | 0.022 | 0.474 | 0.222–1.014 | 0.054 |
| EHS, absence | 0.880 | 0.450–1.722 | 0.710 | |||
| MVI, absence | 0.455 | 0.211–0.981 | 0.044 | 0.454 | 0.222–0.926 | 0.030 |
| AFP, <200 ng/mL | 0.593 | 0.305–1.155 | 0.125 | |||
| AFP ratio at 8 weeks, <1.1 | 0.733 | 0.377–1.425 | 0.359 | |||
| RDI at 8 weeks, ≥70% | 0.429 | 0.252–0.957 | 0.037 | 0.787 | 0.379–1.634 | 0.521 |
| ETS, ≥10% | 0.090 | 0.020–0.394 | <0.001 | 0.091 | 0.021–0.392 | 0.001 |
| Variable | ETS ≥ 10% (n = 32) | ETS < 10% (n = 72) | p‡ |
|---|---|---|---|
| mRECIST, objective response/non-objective response | 22/10 | 13/59 | <0.001 |
| RECIST, objective response/non-objective response | 12/20 | 0/72 | <0.001 |
| Variable | C-Index (95% CI) |
|---|---|
| ETS, ≥ 10/< 10 % | 0.69 (0.64–0.74) |
| mRECIST, objective response/non-objective response † | 0.62 (0.56–0.69) |
| RECIST, objective response/non-objective response † | 0.58 (0.54–0.62) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, A.; Moriguchi, M.; Seko, Y.; Shima, T.; Mitsumoto, Y.; Takashima, H.; Kimura, H.; Fujii, H.; Ishikawa, H.; Yo, T.; et al. Early Tumor Shrinkage as a Predictive Factor for Outcomes in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Multicenter Analysis. Cancers 2020, 12, 754. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030754
Takahashi A, Moriguchi M, Seko Y, Shima T, Mitsumoto Y, Takashima H, Kimura H, Fujii H, Ishikawa H, Yo T, et al. Early Tumor Shrinkage as a Predictive Factor for Outcomes in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Multicenter Analysis. Cancers. 2020; 12(3):754. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030754
Chicago/Turabian StyleTakahashi, Aya, Michihisa Moriguchi, Yuya Seko, Toshihide Shima, Yasuhide Mitsumoto, Hidetaka Takashima, Hiroyuki Kimura, Hideki Fujii, Hiroki Ishikawa, Takaharu Yo, and et al. 2020. "Early Tumor Shrinkage as a Predictive Factor for Outcomes in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Multicenter Analysis" Cancers 12, no. 3: 754. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030754