The Value of Laboratory Parameters for Anemia, Renal Function, Systemic Inflammation and Nutritional Status as Predictors for Outcome in Elderly Patients with Head-and-Neck Cancers

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
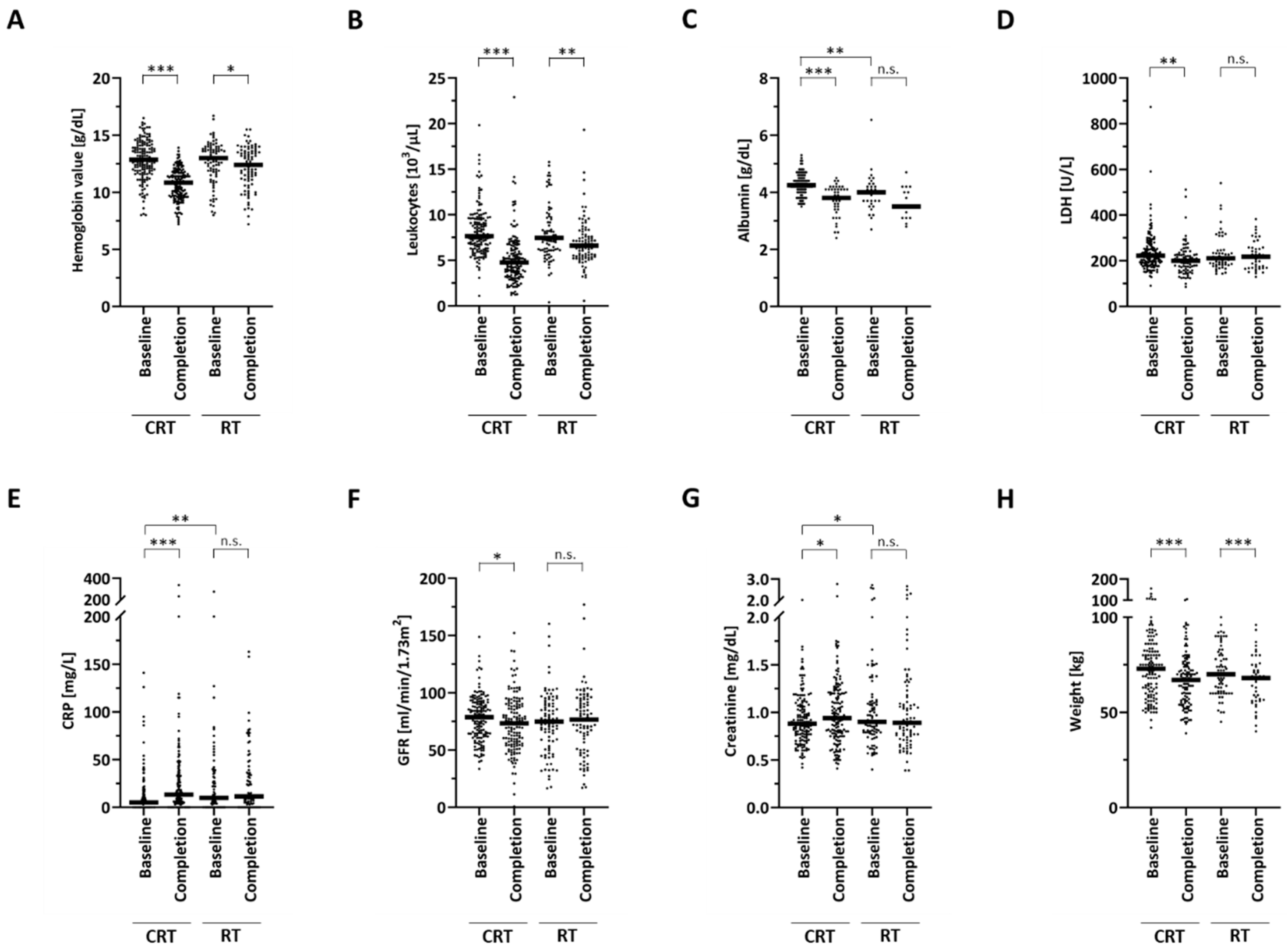
2.2. Dynamics of Routine Biomarkers during Therapy
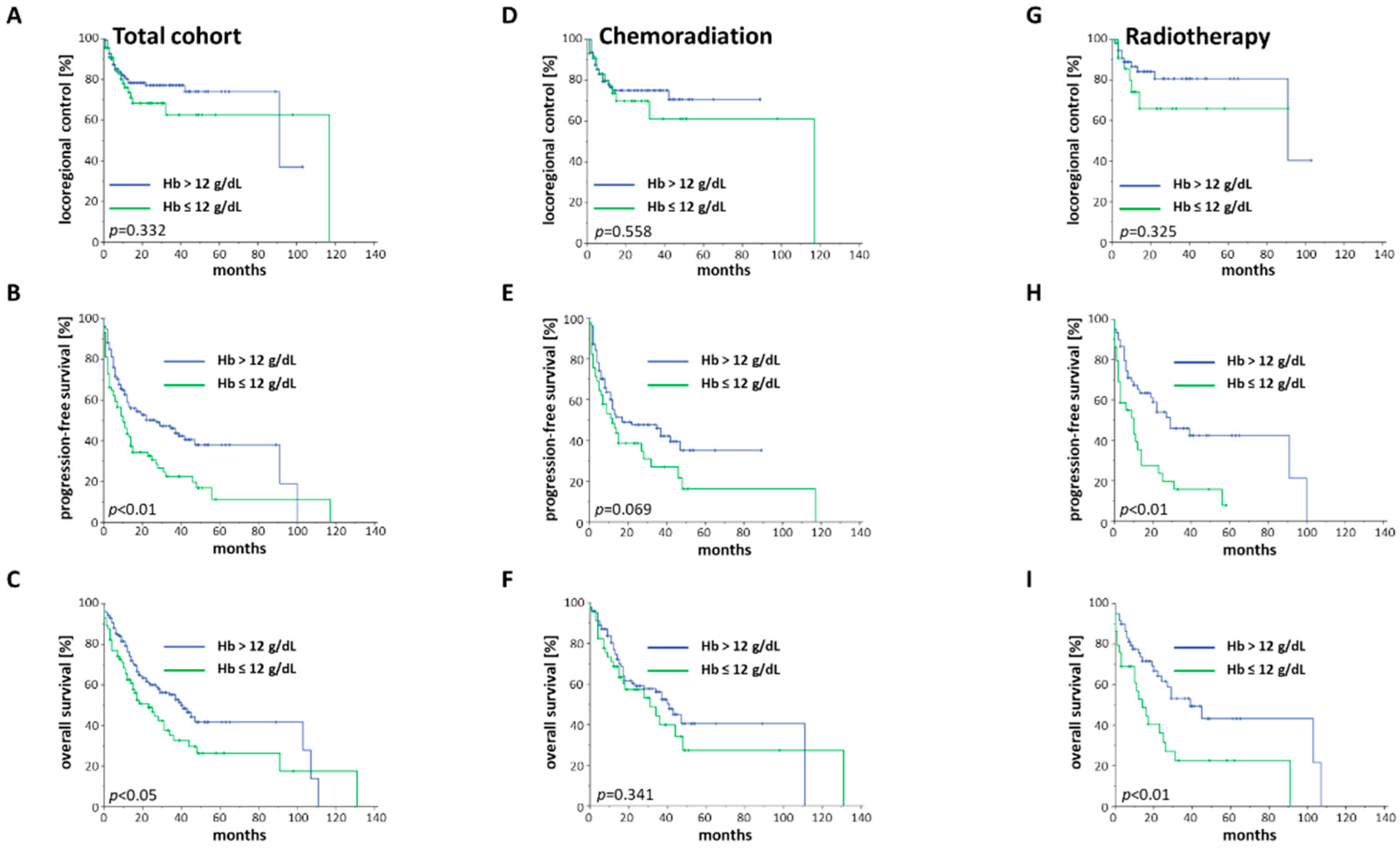
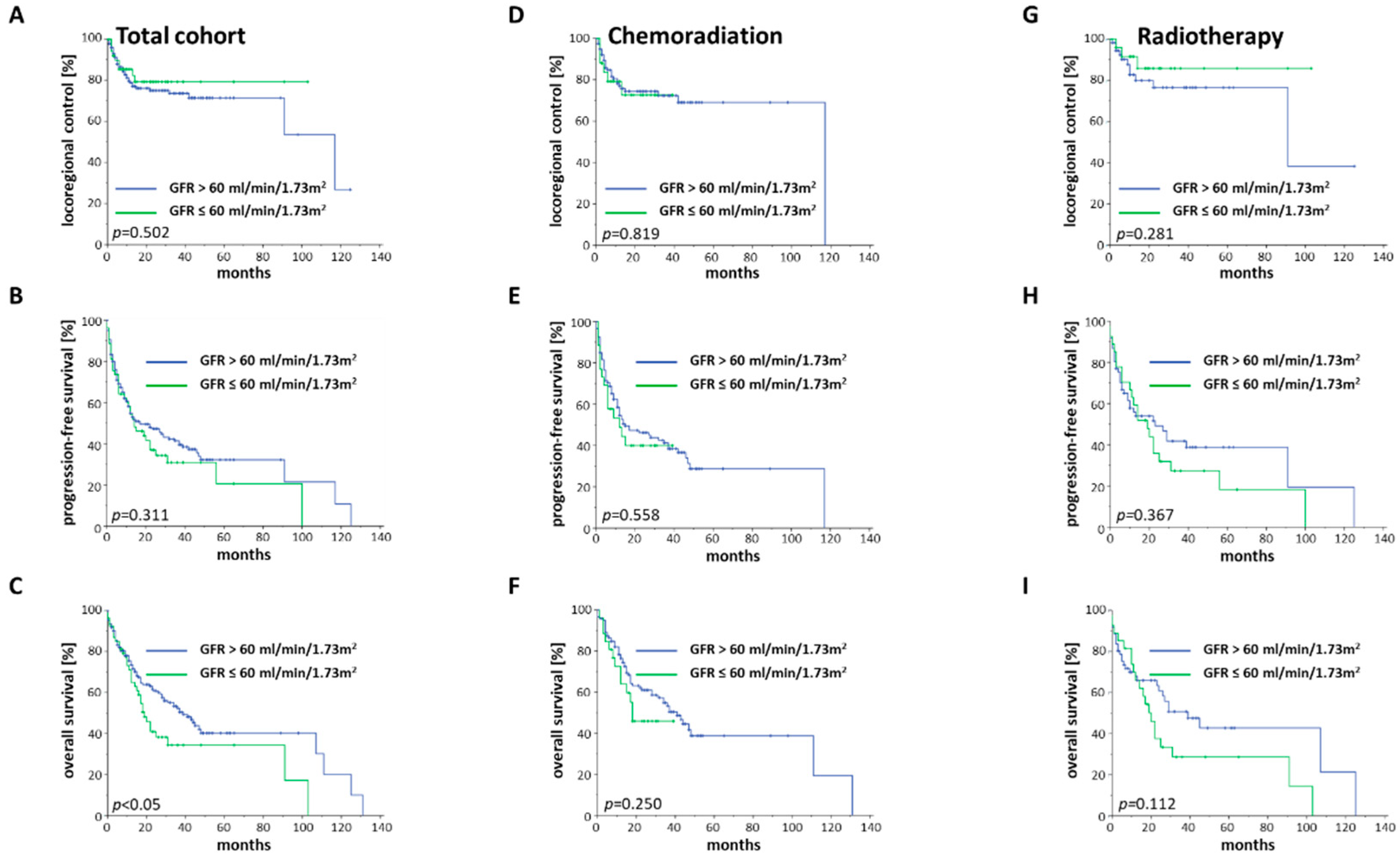
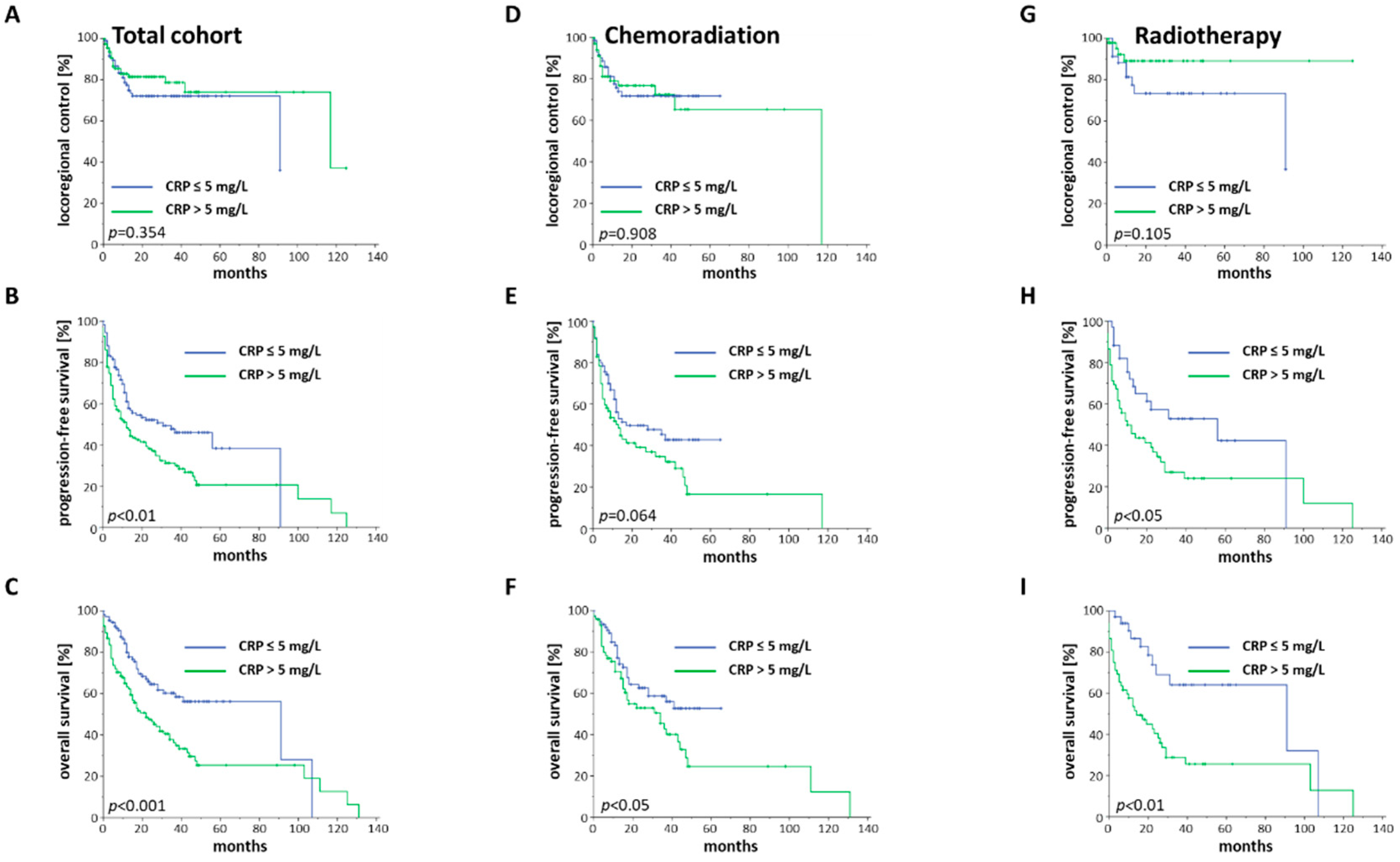
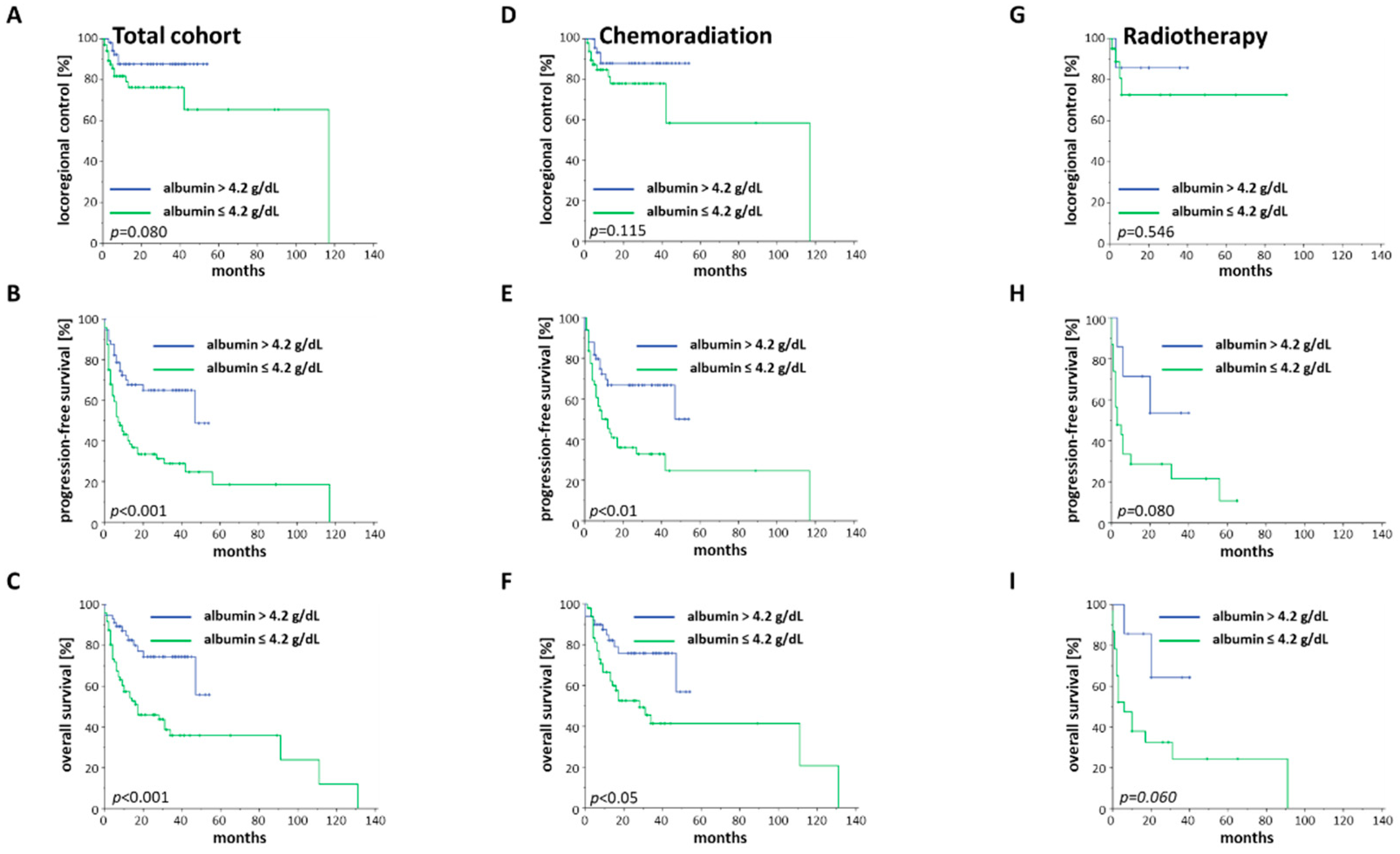
2.3. Treatment Outcome in Dependence of Baseline Blood Parameters
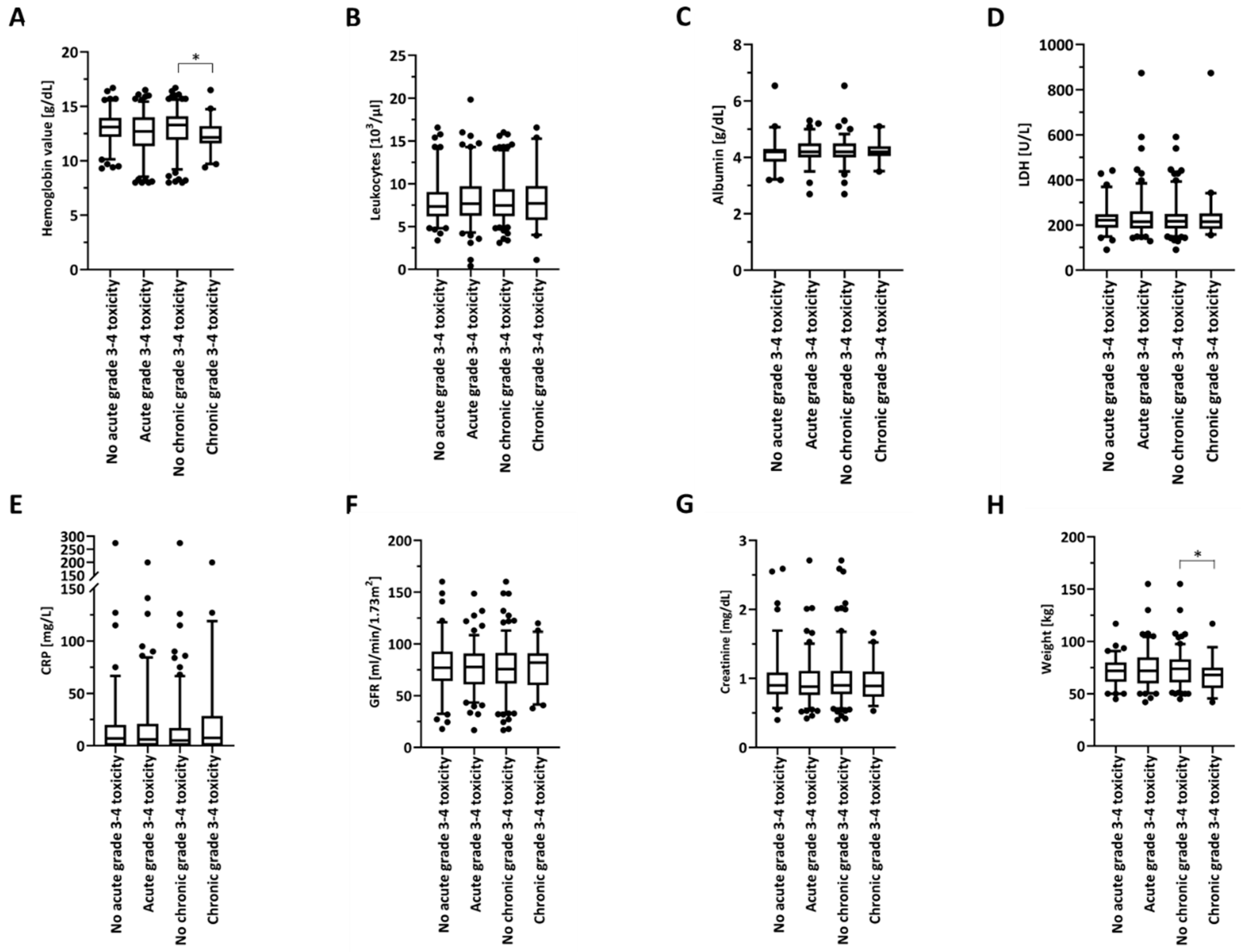
2.4. Routine Biomarkers as Potential Prognosticators for Treatment-Associated Toxicities
3. Discussion
4. Materials and Methods
4.1. Patients and Treatment
4.2. Survival and Toxicity
4.3. Blood Value and Body Weight Analyses
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grenman, R.; Chevalier, D.; Gregoire, V.; Myers, E.; Rogers, S. Treatment of head and neck cancer in the elderly: European Consensus (panel 6) at the EUFOS Congress in Vienna 2007. Eur. Arch. Otorhinolaryngol. 2010, 267, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, N.; Williams, M.D. Epidemiologic trends in head and neck cancer and aids in diagnosis. Oral Maxillofac. Surg. Clin. N. Am 2014, 26, 123–141. [Google Scholar] [CrossRef]
- Smith, B.D.; Smith, G.L.; Hurria, A.; Hortobagyi, G.N.; Buchholz, T.A. Future of cancer incidence in the United States: Burdens upon an aging, changing nation. J. Clin. Oncol. 2009, 27, 2758–2765. [Google Scholar] [CrossRef] [PubMed]
- Adelstein, D.J.; Li, Y.; Adams, G.L.; Wagner, H., Jr.; Kish, J.A.; Ensley, J.F.; Schuller, D.E.; Forastiere, A.A. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J. Clin. Oncol. 2003, 21, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.-L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [Green Version]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus Cetuximab for Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef] [Green Version]
- Gugić, J.; Strojan, P. Squamous cell carcinoma of the head and neck in the elderly. Rep. Pract. Oncol. Radiother. 2012, 18, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Giacalone, N.J.; Qureshi, M.M.; Mak, K.S.; Kirke, D.; Patel, S.A.; Shah, B.A.; Salama, A.R.; Jalisi, S.; Truong, M.T. Adjuvant chemoradiation does not improve survival in elderly patients with high-risk resected head and neck cancer. Laryngoscope 2018, 128, 831–840. [Google Scholar] [CrossRef]
- Pignon, J.P.; le Maitre, A.; Maillard, E.; Bourhis, J.; Group, M.-N.C. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Cohen, R.B.; Jones, C.U.; Sur, R.K.; Raben, D.; Baselga, J.; Spencer, S.A.; Zhu, J.; et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol. 2010, 11, 21–28. [Google Scholar] [CrossRef]
- Bourhis, J.; Overgaard, J.; Audry, H.; Ang, K.K.; Saunders, M.; Bernier, J.; Horiot, J.C.; Le Maitre, A.; Pajak, T.F.; Poulsen, M.G.; et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: A meta-analysis. Lancet 2006, 368, 843–854. [Google Scholar] [CrossRef]
- Summerer, I.; Unger, K.; Braselmann, H.; Schuettrumpf, L.; Maihoefer, C.; Baumeister, P.; Kirchner, T.; Niyazi, M.; Sage, E.; Specht, H.M.; et al. Circulating microRNAs as prognostic therapy biomarkers in head and neck cancer patients. Br. J. Cancer 2015, 113, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Nowicka, Z.; Stawiski, K.; Tomasik, B.; Fendler, W. Extracellular miRNAs as Biomarkers of Head and Neck Cancer Progression and Metastasis. Int. J. Mol. Sci. 2019, 20, 4799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rühle, A.; Sprave, T.; Kalckreuth, T.; Stoian, R.; Haehl, E.; Zamboglou, C.; Laszig, R.; Knopf, A.; Grosu, A.-L.; Nicolay, N.H. The value of moderate dose escalation for re-irradiation of recurrent or second primary head-and-neck cancer. Radiat. Oncol. 2020, 15, 81. [Google Scholar] [CrossRef] [PubMed]
- Knittelfelder, O.; Delago, D.; Jakse, G.; Lukasiak, K.; Thurner, E.M.; Thurnher, D.; Pichler, M.; Renner, W.; Stranzl-Lawatsch, H.; Langsenlehner, T. The Pre-Treatment C-Reactive Protein Represents a Prognostic Factor in Patients with Oral and Oropharyngeal Cancer Treated with Radiotherapy. Cancers 2020, 12, 626. [Google Scholar] [CrossRef] [Green Version]
- Haehl, E.; Ruhle, A.; David, H.; Kalckreuth, T.; Sprave, T.; Stoian, R.; Becker, C.; Knopf, A.; Grosu, A.L.; Nicolay, N.H. Radiotherapy for geriatric head-and-neck cancer patients: What is the value of standard treatment in the elderly? Radiat. Oncol. 2020, 15, 31. [Google Scholar] [CrossRef] [Green Version]
- International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma. N. Engl. J. Med. 1993, 329, 987–994. [Google Scholar] [CrossRef]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef] [Green Version]
- Van Wilpe, S.; Koornstra, R.; Den Brok, M.; De Groot, J.W.; Blank, C.; De Vries, J.; Gerritsen, W.; Mehra, N. Lactate dehydrogenase: A marker of diminished antitumor immunity. OncoImmunology 2020, 9, 1731942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danan, D.; Shonka, D.C., Jr.; Selman, Y.; Chow, Z.; Smolkin, M.E.; Jameson, M.J. Prognostic value of albumin in patients with head and neck cancer. Laryngoscope 2016, 126, 1567–1571. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.S.; Roh, J.-L.; Kim, S.-B.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Pretreatment albumin level predicts survival in head and neck squamous cell carcinoma. Laryngoscope 2017, 127, E437–E442. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.; Liu, F.; Lin, J.; Chen, Q.; Chen, L.; Chen, F.; Wang, J.; Qiu, Y.; Shi, B.; Pan, L.; et al. Nutritional assessment and prognosis of oral cancer patients: A large-scale prospective study. BMC Cancer 2020, 20, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chargi, N.; Bril, S.I.; Emmelot-Vonk, M.H.; de Bree, R. Sarcopenia is a prognostic factor for overall survival in elderly patients with head-and-neck cancer. Eur. Arch. Otorhinolaryngol. 2019, 276, 1475–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- Unsal, D.; Mentes, B.; Akmansu, M.; Uner, A.; Oguz, M.; Pak, Y. Evaluation of nutritional status in cancer patients receiving radiotherapy: A prospective study. Am. J. Clin. Oncol. 2006, 29, 183–188. [Google Scholar] [CrossRef]
- Gorenc, M.; Kozjek, N.R.; Strojan, P. Malnutrition and cachexia in patients with head and neck cancer treated with (chemo)radiotherapy. Rep. Pract. Oncol. Radiother. 2015, 20, 249–258. [Google Scholar] [CrossRef] [Green Version]
- McMillan, D.C.; Watson, W.S.; O’Gorman, P.; Preston, T.; Scott, H.R.; McArdle, C.S. Albumin Concentrations Are Primarily Determined by the Body Cell Mass and the Systemic Inflammatory Response in Cancer Patients With Weight Loss. Nutr. Cancer 2001, 39, 210–213. [Google Scholar] [CrossRef] [Green Version]
- Spiro, A.; Baldwin, C.; Patterson, A.; Thomas, J.; Andreyev, H.J.N. The views and practice of oncologists towards nutritional support in patients receiving chemotherapy. Br. J. Cancer 2006, 95, 431–434. [Google Scholar] [CrossRef] [Green Version]
- Talwar, B.; Donnelly, R.; Skelly, R.; Donaldson, M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S32–S40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunst, J.; Kuhnt, T.; Strauss, H.G.; Krause, U.; Pelz, T.; Koelbl, H.; Haensgen, G. Anemia in cervical cancers: Impact on survival, patterns of relapse, and association with hypoxia and angiogenesis. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 778–787. [Google Scholar] [CrossRef]
- Dubray, B.; Mosseri, V.; Brunin, F.; Jaulerry, C.; Poncet, P.; Rodriguez, J.; Brugère, J.; Point, D.; Giraud, P.; Cosset, J.M. Anemia is associated with lower local-regional control and survival after radiation therapy for head and neck cancer: A prospective study. Radiology 1996, 201, 553–558. [Google Scholar] [CrossRef]
- Becker, A.; Stadler, P.; Lavey, R.S.; Hänsgen, G.; Kuhnt, T.; Lautenschläger, C.; Feldmann, H.J.; Molls, M.; Dunst, J. Severe anemia is associated with poor tumor oxygenation in head and neck squamous cell carcinomas11Accepted for publication 30 August 1999. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 459–466. [Google Scholar] [CrossRef]
- Nicolay, N.H.; Wiedenmann, N.; Mix, M.; Weber, W.A.; Werner, M.; Grosu, A.L.; Kayser, G. Correlative analyses between tissue-based hypoxia biomarkers and hypoxia PET imaging in head and neck cancer patients during radiochemotherapy-results from a prospective trial. Eur. J. Nucl. Med. Mol. Imaging 2019. [Google Scholar] [CrossRef]
- Wiedenmann, N.E.; Bucher, S.; Hentschel, M.; Mix, M.; Vach, W.; Bittner, M.I.; Nestle, U.; Pfeiffer, J.; Weber, W.A.; Grosu, A.L. Serial [18F]-fluoromisonidazole PET during radiochemotherapy for locally advanced head and neck cancer and its correlation with outcome. Radiother. Oncol. 2015, 117, 113–117. [Google Scholar] [CrossRef]
- Henke, M.; Laszig, R.; Rübe, C.; Schäfer, U.; Haase, K.-D.; Schilcher, B.; Mose, S.; Beer, K.T.; Burger, U.; Dougherty, C.; et al. Erythropoietin to treat head and neck cancer patients with anaemia undergoing radiotherapy: Randomised, double-blind, placebo-controlled trial. Lancet 2003, 362, 1255–1260. [Google Scholar] [CrossRef]
- Machtay, M.; Pajak, T.F.; Suntharalingam, M.; Shenouda, G.; Hershock, D.; Stripp, D.C.; Cmelak, A.J.; Schulsinger, A.; Fu, K.K. Radiotherapy With or Without Erythropoietin for Anemic Patients With Head and Neck Cancer: A Randomized Trial of the Radiation Therapy Oncology Group (RTOG 99-03). Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1008–1017. [Google Scholar] [CrossRef]
- Hoff, C.M.; Lassen, P.; Eriksen, J.G.; Hansen, H.S.; Specht, L.; Overgaard, M.; Grau, C.; Johansen, J.; Bentzen, J.; Andersen, L.; et al. Does transfusion improve the outcome for HNSCC patients treated with radiotherapy?—Results from the randomized DAHANCA 5 and 7 trials. Acta Oncol. 2011, 50, 1006–1014. [Google Scholar] [CrossRef]
- Goodnough, L.T.; Schrier, S.L. Evaluation and management of anemia in the elderly. Am. J. Hematol. 2014, 89, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.V. Epidemiology of anemia in older adults. Semin. Hematol. 2008, 45, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakai, N.A.; Katz, R.; Hirsch, C.; Shlipak, M.G.; Chaves, P.H.; Newman, A.B.; Cushman, M. A prospective study of anemia status, hemoglobin concentration, and mortality in an elderly cohort: The Cardiovascular Health Study. Arch. Intern. Med. 2005, 165, 2214–2220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tracy, R.P.; Lemaitre, R.N.; Psaty, B.M.; Ives, D.G.; Evans, R.W.; Cushman, M.; Meilahn, E.N.; Kuller, L.H. Relationship of C-reactive protein to risk of cardiovascular disease in the elderly. Results from the Cardiovascular Health Study and the Rural Health Promotion Project. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Wang, J.; Tan, D.; Cheng, P.; Wu, A. Relationship between circulating inflammatory factors and glioma risk and prognosis: A meta-analysis. Cancer Med. 2019, 8, 7454–7468. [Google Scholar] [CrossRef] [PubMed]
- Allin, K.H.; Nordestgaard, B.G. Elevated C-reactive protein in the diagnosis, prognosis, and cause of cancer. Crit. Rev. Clin. Lab. Sci. 2011, 48, 155–170. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, S.; Zheng, C.; Ding, M.; Zhang, L.; Wang, L.; Xie, M.; Zhou, J. The prognostic value of the preoperative c-reactive protein/albumin ratio in ovarian cancer. BMC Cancer 2017, 17, 285. [Google Scholar] [CrossRef]
- Katano, A.; Takahashi, W.; Yamashita, H.; Yamamoto, K.; Ando, M.; Yoshida, M.; Saito, Y.; Abe, O.; Nakagawa, K. The impact of elevated C-reactive protein level on the prognosis for oro-hypopharynx cancer patients treated with radiotherapy. Sci. Rep. 2017, 7, 17805. [Google Scholar] [CrossRef] [Green Version]
- Fu, J.; Yang, X. The Prognostic Value of the C-reactive Protein/Prognostic Nutritional Index Ratio in Stage III and IV Laryngeal Cancer Patients Treated with Radiotherapy. Cureus 2019, 11, e4648. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-H.; Wang, H.-M.; Fan, K.-H.; Lin, C.-Y.; Yen, T.-C.; Liao, C.-T.; Chen, I.H.; Kang, C.-J.; Huang, S.-F. Pre-Treatment Levels of C-Reactive Protein and Squamous Cell Carcinoma Antigen for Predicting the Aggressiveness of Pharyngolaryngeal Carcinoma. PLoS ONE 2013, 8, e55327. [Google Scholar] [CrossRef]
- Yadav, A.; Kumar, B.; Datta, J.; Teknos, T.N.; Kumar, P. IL-6 promotes head and neck tumor metastasis by inducing epithelial-mesenchymal transition via the JAK-STAT3-SNAIL signaling pathway. Mol. Cancer Res. 2011, 9, 1658–1667. [Google Scholar] [CrossRef] [Green Version]
- Buckley, D.I.; Fu, R.; Freeman, M.; Rogers, K.; Helfand, M. C-reactive protein as a risk factor for coronary heart disease: A systematic review and meta-analyses for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2009, 151, 483–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yellen, S.B.; Cella, D.F.; Leslie, W.T. Age and clinical decision making in oncology patients. J. Natl. Cancer Inst. 1994, 86, 1766–1770. [Google Scholar] [CrossRef] [PubMed]
- Sarini, J.; Fournier, C.; Lefebvre, J.-L.; Bonafos, G.; Van, J.T.; Coche-Dequéant, B. Head and Neck Squamous Cell Carcinoma in Elderly Patients: A Long-term Retrospective Review of 273 Cases. Arch. Otolaryngol.–Head Neck Surg. 2001, 127, 1089–1092. [Google Scholar] [CrossRef] [Green Version]
- van Bokhorst-de van der Schueren, M.A.E.; Lonterman-Monasch, S.; de Vries, O.J.; Danner, S.A.; Kramer, M.H.H.; Muller, M. Prevalence and determinants for malnutrition in geriatric outpatients. Clin. Nutr. 2013, 32, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Schilp, J.; Wijnhoven, H.A.; Deeg, D.J.; Visser, M. Early determinants for the development of undernutrition in an older general population: Longitudinal Aging Study Amsterdam. Br. J. Nutr. 2011, 106, 708–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total Cohort (n = 246) | RT (n = 99) | CRT (n = 147) | p | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Sex | male | 170 | 69.1 | 67 | 67.7 | 103 | 70.1 | 0.779 |
| female | 76 | 30.9 | 32 | 32.3 | 44 | 29.9 | ||
| Age | 65–74 years | 153 | 62.2 | 45 | 45.5 | 108 | 73.5 | <0.001 |
| ≥75 years | 93 | 37.8 | 54 | 54.5 | 39 | 26.5 | ||
| Smoking | non-smoker | 54 | 22.0 | 18 | 18.2 | 36 | 24.5 | 1.000 |
| smoker | 142 | 57.7 | 48 | 48.5 | 94 | 63.9 | ||
| missing | 50 | 20.3 | 33 | 33.3 | 17 | 11.6 | ||
| Karnofsky | 100% | 28 | 11.4 | 9 | 9.1 | 19 | 12.9 | 0.109 |
| 90% | 108 | 43.9 | 38 | 38.4 | 70 | 47.6 | ||
| 80% | 51 | 20.7 | 20 | 20.2 | 31 | 21.1 | ||
| 70% | 23 | 9.3 | 9 | 9.1 | 14 | 9.5 | ||
| 60% | 14 | 5.7 | 10 | 10.1 | 4 | 2.7 | ||
| 50% | 3 | 1.2 | 2 | 2.0 | 1 | 0.7 | ||
| 40% | 1 | 0.4 | 1 | 1.0 | 0 | 0.0 | ||
| missing | 18 | 7.3 | 10 | 10.1 | 8 | 5.4 | ||
| T stage | T1 | 35 | 14.2 | 23 | 23.2 | 12 | 8.2 | <0.001 |
| T2 | 53 | 21.5 | 28 | 28.3 | 25 | 17.0 | ||
| T3 | 64 | 26.0 | 20 | 20.2 | 44 | 29.9 | ||
| T4 | 86 | 35.0 | 24 | 24.2 | 62 | 42.2 | ||
| missing | 8 | 3.3 | 4 | 4.0 | 4 | 2.7 | ||
| N stage | N0 | 82 | 33.3 | 49 | 49.5 | 33 | 22.4 | <0.001 |
| N1 | 33 | 13.4 | 16 | 16.1 | 17 | 11.6 | ||
| N2 | 120 | 48.8 | 32 | 32.3 | 88 | 59.9 | ||
| N3 | 11 | 4.5 | 2 | 2.0 | 9 | 6.1 | ||
| M stage | M0 | 232 | 94.3 | 93 | 93.9 | 139 | 94.6 | 1.000 |
| M1 | 10 | 4.1 | 4 | 4.0 | 6 | 4.1 | ||
| missing | 4 | 1.6 | 2 | 2.0 | 2 | 1.4 | ||
| Grading | G1 | 6 | 2.4 | 5 | 5.1 | 1 | 0.7 | 0.207 |
| G2 | 157 | 63.8 | 62 | 62.6 | 95 | 64.6 | ||
| G3 | 74 | 30.1 | 29 | 29.3 | 45 | 30.6 | ||
| G4 | 1 | 0.4 | 0 | 0.0 | 1 | 0.7 | ||
| missing | 8 | 3.3 | 4 | 4.0 | 4 | 2.7 | ||
| HPV status | HPV-negative | 49 | 19.9 | 17 | 17.2 | 32 | 21.8 | 0.643 |
| HPV-positive | 34 | 13.8 | 10 | 10.1 | 24 | 16.3 | ||
| missing | 163 | 66.3 | 72 | 72.7 | 91 | 61.9 | ||
| Parameter | HR | CI 95% | p-Value |
|---|---|---|---|
| Univariate | |||
| Karnofsky < 80/≥ 80% | 2.803 | 1.817–4.324 | <0.001 |
| Age ≥ 75/65-74 years | 1.584 | 1.101–2.280 | 0.013 |
| Smoker/non-smoker | 1.731 | 1.045–2.868 | 0.033 |
| T3-T4/T1-T2 | 1.267 | 0.863–1.861 | 0.227 |
| N1-N3/N0 | 1.099 | 0.746–1.617 | 0.633 |
| Baseline GFR ≤ 60/> 60 mL/min/1.73 m2 | 1.537 | 1.024–2.308 | 0.038 |
| Baseline Hb ≤ 12/> 12 g/dL | 1.536 | 1.058–2.231 | 0.024 |
| Baseline CRP > 5/≤ 5 mg/L | 1.991 | 1.356–2.923 | <0.001 |
| Baseline albumin ≤ 4.2/> 4.2 g/dL | 2.916 | 1.561–5.445 | <0.001 |
| Baseline LDH > 250/≤ 250 U/L | 1.106 | 0.713–1.715 | 0.654 |
| Baseline leukocytes < 4/4-0 × 103/µL | 0.703 | 0.173–2.858 | 0.623 |
| Baseline leukocytes > 10/4-10 × 103/µL | 1.158 | 0.737–1.818 | 0.525 |
| Baseline body weight ≤ 72/> 72 kg | 1.079 | 0.712–1.637 | 0.719 |
| Multivariate | |||
| Karnofsky < 80/≥ 80% | 2.460 | 1.227–4.930 | 0.011 |
| Age ≥ 75/65-74 years | 1.918 | 0.992–3.708 | 0.053 |
| Smoker/non-smoker | 1.670 | 0.710–3.931 | 0.240 |
| Baseline GFR ≤ 60/> 60 mL/min | 0.582 | 0.247–1.373 | 0.216 |
| Baseline Hb ≤ 12/> 12 g/dL | 1.433 | 0.686–2.995 | 0.339 |
| Baseline CRP > 5/≤ 5 mg/L | 1.136 | 0.548–2.353 | 0.732 |
| Baseline albumin ≤ 4.2/> 4.2 g/dL | 2.305 | 1.060–5.011 | 0.035 |
| Univariate | Age 65–74 Years | Age ≥ 75 Years | ||||
|---|---|---|---|---|---|---|
| HR | CI 95% | p | HR | CI 95% | p | |
| Karnofsky < 80/≥ 80% | 2.108 | 1.090–4.075 | 0.027 | 3.218 | 1.748–5.926 | <0.001 |
| Smoker/non-smoker | 2.733 | 1.168–6.393 | 0.020 | 1.435 | 0.736–2.797 | 0.289 |
| T3-T4/T1-T2 | 1.112 | 0.673–1.838 | 0.679 | 1.607 | 0.872–2.960 | 0.128 |
| N1-N3/N0 | 1.616 | 0.911–2.866 | 0.101 | 0.815 | 0.468–1.420 | 0.470 |
| Baseline GFR ≤ 60/> 60 mL/min | 1.636 | 0.866–3.091 | 0.129 | 1.086 | 0.620–1.902 | 0.773 |
| Baseline Hb ≤ 12/> 12 g/dL | 1.215 | 0.734–2.011 | 0.449 | 2.153 | 1.220–3.797 | 0.008 |
| Baseline CRP > 5/≤ 5 mg/L | 1.782 | 1.073–2.960 | 0.026 | 2.317 | 1.255–4.280 | 0.007 |
| Baseline albumin ≤ 4.2/> 4.2 g/dL | 2.274 | 0.972–5.320 | 0.058 | 3.224 | 1.227–8.477 | 0.018 |
| Baseline LDH > 250/≤ 250 U/L | 1.470 | 0.853–2.535 | 0.166 | 0.765 | 0.351–1.666 | 0.500 |
| Baseline body weight ≤ 72/> 72 kg | 1.080 | 0.620–1.882 | 0.785 | 1.010 | 0.533–1.915 | 0.976 |
| Parameter | No Chronic Grade 3–4 Toxicities | Chronic Grade 3–4 Toxicities |
|---|---|---|
| Hb > 12 g/dL | 128 | 22 |
| Hb ≤ 12 g/dL | 45 | 21 |
| p < 0.01 (χ2-test) | ||
| Body weight > 72 kg | 79 | 13 |
| Body weight ≤ 72 kg | 69 | 24 |
| p < 0.05 (χ2-test) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rühle, A.; Haehl, E.; David, H.; Kalckreuth, T.; Sprave, T.; Stoian, R.; Zamboglou, C.; Gkika, E.; Knopf, A.; Grosu, A.-L.; et al. The Value of Laboratory Parameters for Anemia, Renal Function, Systemic Inflammation and Nutritional Status as Predictors for Outcome in Elderly Patients with Head-and-Neck Cancers. Cancers 2020, 12, 1698. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061698
Rühle A, Haehl E, David H, Kalckreuth T, Sprave T, Stoian R, Zamboglou C, Gkika E, Knopf A, Grosu A-L, et al. The Value of Laboratory Parameters for Anemia, Renal Function, Systemic Inflammation and Nutritional Status as Predictors for Outcome in Elderly Patients with Head-and-Neck Cancers. Cancers. 2020; 12(6):1698. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061698
Chicago/Turabian StyleRühle, Alexander, Erik Haehl, Hélène David, Tobias Kalckreuth, Tanja Sprave, Raluca Stoian, Constantinos Zamboglou, Eleni Gkika, Andreas Knopf, Anca-Ligia Grosu, and et al. 2020. "The Value of Laboratory Parameters for Anemia, Renal Function, Systemic Inflammation and Nutritional Status as Predictors for Outcome in Elderly Patients with Head-and-Neck Cancers" Cancers 12, no. 6: 1698. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061698