Computer Extracted Features from Initial H&E Tissue Biopsies Predict Disease Progression for Prostate Cancer Patients on Active Surveillance


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset
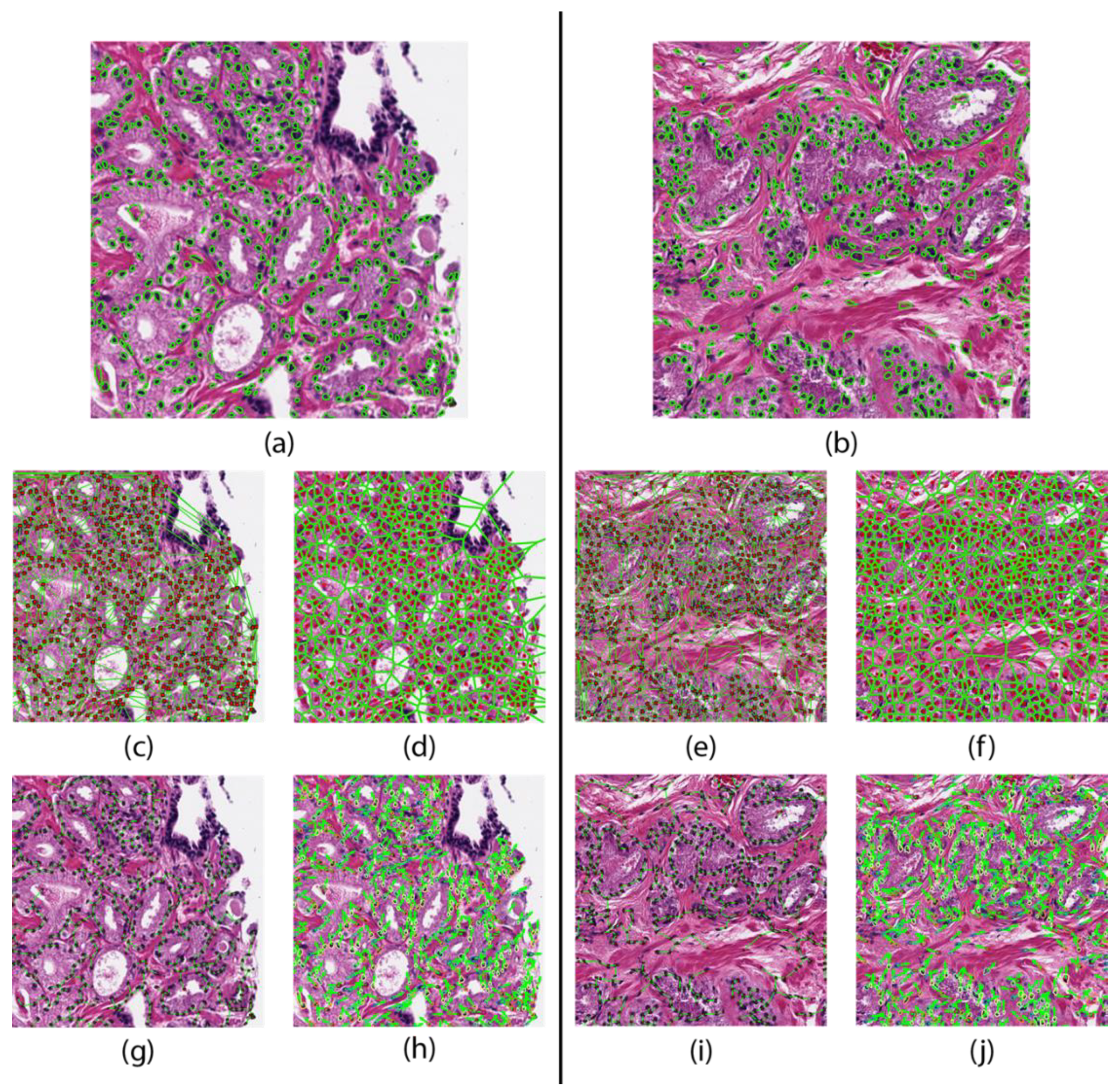
2.2. Nuclear Segmentation
2.3. Feature Extraction
2.4. Feature Identification
2.5. Classifier Construction
2.6. Deep Learning Model
3. Results
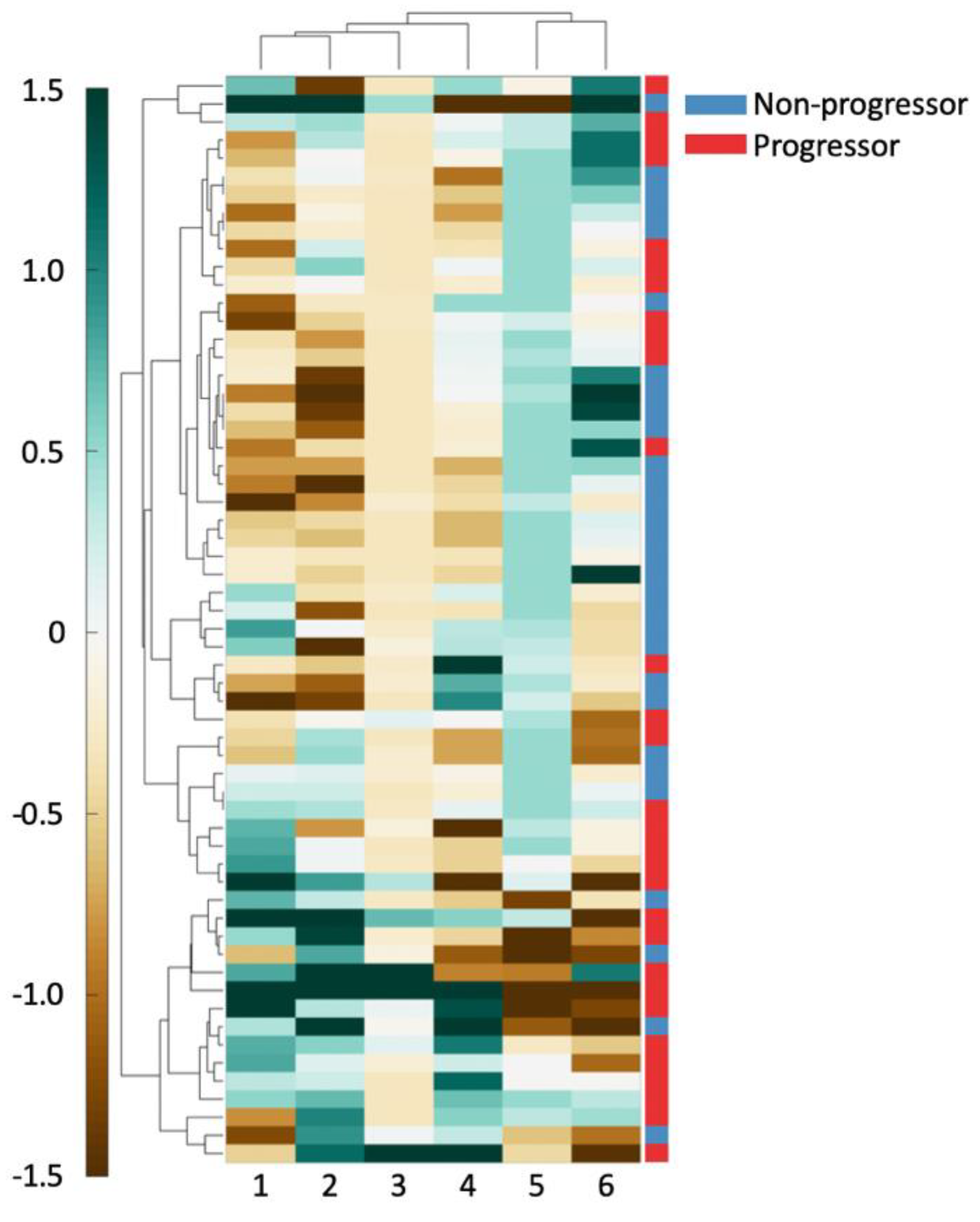
3.1. Experiment 1: Identifying Features Associated with Risk of Progression in AS Patients
3.2. Experiment 2: QH based Classifier Construction to Predict Progression in AS Patients
3.3. Experiment 3: Deep Learning Classifier for Prediction of Progression in AS Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Albertsen, P.C. Treatment of localized prostate cancer: When is active surveillance appropriate? Nat. Rev. Clin. Oncol. 2010, 7, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.; Loeb, A.; Kaye, K.S.; Cher, M.L.; Martin, E.T. Infection-Related Hospital Admissions After Prostate Biopsy in United States Men. Open Forum Infect. Dis. 2017, 4, ofw265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albertsen, P.C. Observational studies and the natural history of screen-detected prostate cancer. Curr. Opin. Urol. 2015, 25, 232. [Google Scholar] [CrossRef]
- Briganti, A.; Fossati, N.; Catto, J.W.F.; Cornford, P.; Montorsi, F.; Mottet, N.; Wirth, M.; Poppel, H.V. Active Surveillance for Low-risk Prostate Cancer: The European Association of Urology Position in 2018. Eur. Urol. 2018, 74, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Bul, M.; Zhu, X.; Valdagni, R.; Pickles, T.; Kakehi, Y.; Rannikko, A.; Bjartell, A.; van der Schoot, D.K.; Cornel, E.B.; Conti, G.N.; et al. Active Surveillance for Low-Risk Prostate Cancer Worldwide: The PRIAS Study. Eur. Urol. 2013, 63, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Soloway, M.S.; Soloway, C.T.; Eldefrawy, A.; Acosta, K.; Kava, B.; Manoharan, M. Careful Selection and Close Monitoring of Low-Risk Prostate Cancer Patients on Active Surveillance Minimizes the Need for Treatment. Eur. Urol. 2010, 58, 831–835. [Google Scholar] [CrossRef]
- Porten, S.P.; Whitson, J.M.; Cowan, J.E.; Cooperberg, M.R.; Shinohara, K.; Perez, N.; Greene, K.L.; Meng, M.V.; Carroll, P.R. Changes in prostate cancer grade on serial biopsy in men undergoing active surveillance. J. Clin. Oncol. 2011, 29, 2795–2800. [Google Scholar] [CrossRef]
- Welty, C.J.; Cooperberg, M.R.; Carroll, P.R. Meaningful End Points and Outcomes in Men on Active Surveillance for Early–Stage Prostate Cancer. Curr. Opin. Urol. 2014, 24, 288–292. [Google Scholar] [CrossRef]
- Bruinsma, S.M.; Bangma, C.H.; Carroll, P.R.; Leapman, M.S.; Rannikko, A.; Petrides, N.; Weerakoon, M.; Bokhorst, L.P.; Roobol, M.J. The Movember GAP3 Consortium. Active surveillance for prostate cancer: A narrative review of clinical guidelines. Nat. Rev. Urol. 2016, 13, 151–167. [Google Scholar] [CrossRef]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef]
- McLean, M.; Srigley, J.; Banerjee, D.; Warde, P.; Hao, Y. Interobserver variation in prostate cancer Gleason scoring: Are there implications for the design of clinical trials and treatment strategies? Clin. Oncol. 1997, 9, 222–225. [Google Scholar] [CrossRef]
- Loeb, S.; Tosoian, J.J. Biomarkers in active surveillance. Transl. Androl. Urol. 2018, 7, 155–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newcomb, L.F.; Brooks, J.D.; Carroll, P.R.; Feng, Z.; Gleave, M.E.; Nelson, P.S.; Thompson, I.M.; Lin, D.W. Canary Prostate Active Surveillance Study (PASS); Design of a Multi-institutional Active Surveillance Cohort and Biorepository. Urology 2010, 75, 407–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooperberg, M.R.; Carroll, P.R.; Klotz, L. Active Surveillance for Prostate Cancer: Progress and Promise. J. Clin. Oncol. 2011, 29, 3669–3676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, D.W.; Newcomb, L.F.; Brown, E.C.; Brooks, J.D.; Carroll, P.R.; Feng, Z.; Gleave, M.E.; Lance, R.S.; Sanda, M.G.; Thompson, I.M.; et al. Urinary TMPRSS2:ERG and PCA3 in an active surveillance cohort: Results from a baseline analysis in the Canary Prostate Active Surveillance Study. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2013, 19, 2442–2450. [Google Scholar] [CrossRef] [Green Version]
- Cooperberg, M.R.; Brooks, J.D.; Faino, A.V.; Newcomb, L.F.; Kearns, J.T.; Carroll, P.R.; Dash, A.; Etzioni, R.; Fabrizio, M.D.; Gleave, M.E.; et al. Refined Analysis of Prostate-specific Antigen Kinetics to Predict Prostate Cancer Active Surveillance Outcomes. Eur. Urol. 2018, 74, 211–217. [Google Scholar] [CrossRef]
- Gurcan, M.N.; Boucheron, L.E.; Can, A.; Madabhushi, A.; Rajpoot, N.M.; Yener, B. Histopathological Image Analysis: A Review. IEEE Rev. Biomed. Eng. 2009, 2, 147–171. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Sparks, R.; Ali, S.; Shih, N.N.C.; Feldman, M.D.; Spangler, E.; Rebbeck, T.; Tomaszewski, J.E.; Madabhushi, A. Co-occurring gland angularity in localized subgraphs: Predicting biochemical recurrence in intermediate-risk prostate cancer patients. PLoS ONE 2014, 9, e97954. [Google Scholar] [CrossRef] [Green Version]
- Veltri, R.W.; Isharwal, S.; Miller, M.C.; Epstein, J.I.; Partin, A.W. Nuclear roundness variance predicts prostate cancer progression, metastasis, and death: A prospective evaluation with up to 25 years of follow-up after radical prostatectomy. Prostate 2010, 70, 1333–1339. [Google Scholar] [CrossRef]
- Farjam, R.; Soltanian-Zadeh, H.; Jafari-Khouzani, K.; Zoroofi, R.A. An image analysis approach for automatic malignancy determination of prostate pathological images. Cytom. B Clin. Cytom. 2007, 72, 227–240. [Google Scholar] [CrossRef]
- Diamond, D.A.; Berry, S.J.; Umbricht, C.; Jewett, H.J.; Coffey, D.S. Computerized image analysis of nuclear shape as a prognostic factor for prostatic cancer. Prostate 1982, 3, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Tabesh, A.; Teverovskiy, M.; Pang, H.-Y.; Kumar, V.P.; Verbel, D.; Kotsianti, A.; Saidi, O. Multifeature prostate cancer diagnosis and Gleason grading of histological images. IEEE Trans. Med. Imaging 2007, 26, 1366–1378. [Google Scholar] [CrossRef] [PubMed]
- Ström, P.; Kartasalo, K.; Olsson, H.; Solorzano, L.; Delahunt, B.; Berney, D.M.; Bostwick, D.G.; Evans, A.J.; Grignon, D.J.; Humphrey, P.A.; et al. Artificial intelligence for diagnosis and grading of prostate cancer in biopsies: A population-based, diagnostic study. Lancet Oncol. 2020, 21, 222–232. [Google Scholar] [CrossRef]
- Bulten, W.; Pinckaers, H.; van Boven, H.; Vink, R.; de Bel, T.; van Ginneken, B.; van der Laak, J.; de Kaa, C.H.; Litjens, G. Automated deep-learning system for Gleason grading of prostate cancer using biopsies: A diagnostic study. Lancet Oncol. 2020, 21, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Macenko, M.; Niethammer, M.; Marron, J.S.; Borland, D.; Woosley, J.T.; Guan, X.; Schmitt, C.; Thomas, N.E. A method for normalizing histology slides for quantitative analysis. In Proceedings of the 2009 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Boston, MA, USA, 28 June–1 July 2009; pp. 1107–1110. [Google Scholar]
- Lee, G.; Ali, S.; Veltri, R.; Epstein, J.I.; Christudass, C.; Madabhushi, A. Cell orientation entropy (COrE): Predicting biochemical recurrence from prostate cancer tissue microarrays. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention—MICCAI 2013: Medical Image Computing and Computer-Assisted Intervention–MICCAI 2013, Nagoya, Japan, 22–26 September 2013; Volume 16, pp. 396–403. [Google Scholar]
- Ali, S.; Lewis, J.; Madabhushi, A. Spatially aware cell cluster(spACC1) graphs: Predicting outcome in oropharyngeal pl6+ tumors. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention—MICCAI 2013: Medical Image Computing and Computer-Assisted Intervention–MICCAI 2013, Nagoya, Japan, 22–26 September 2013; Volume 16, pp. 412–419. [Google Scholar]
- Lee, G.; Singanamalli, A.; Wang, H.; Feldman, M.D.; Master, S.R.; Shih, N.N.C.; Spangler, E.; Rebbeck, T.; Tomaszewski, J.E.; Madabhushi, A. Supervised multi-view canonical correlation analysis (sMVCCA): Integrating histologic and proteomic features for predicting recurrent prostate cancer. IEEE Trans. Med. Imaging 2015, 34, 284–297. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. arXiv 2018, arXiv:160806993 Cs. [Google Scholar]
- Wang, S.-Y.; Cowan, J.E.; Cary, K.C.; Chan, J.M.; Carroll, P.R.; Cooperberg, M.R. Limited ability of existing nomograms to predict outcomes in men undergoing active surveillance for prostate cancer. BJU Int. 2014, 114, E18–E24. [Google Scholar] [CrossRef]
- Isharwal, S.; Makarov, D.V.; Sokoll, L.J.; Landis, P.; Marlow, C.; Epstein, J.I.; Partin, A.W.; Carter, H.B.; Veltri, R.W. ProPSA and Diagnostic Biopsy Tissue DNA Content Combination Improves Accuracy to Predict Need for Prostate Cancer Treatment Among Men Enrolled in an Active Surveillance Program. Urology 2011, 77, 763.e1–763.e6. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; Veltri, R.; Epstein, J.A.; Christudass, C.; Madabhushi, A. Cell cluster graph for prediction of biochemical recurrence in prostate cancer patients from tissue microarrays. In Proceedings of the Medical Imaging 2013: Digital Pathology; International Society for Optics and Photonics, Lake Buena Vista (Orlando Area), FL, USA, 9–14 February 2013; Volume 8676, p. 86760H. [Google Scholar]
- Freedland, S.J.; Kane, C.J.; Amling, C.L.; Aronson, W.J.; Terris, M.K.; Presti, J.C. Upgrading and Downgrading of Prostate Needle Biopsies: Risk Factors and Clinical Implications. Urology 2007, 69, 495–499. [Google Scholar] [CrossRef] [Green Version]
- Veltri, R.W.; Miller, M.C.; Isharwal, S.; Marlow, C.; Makarov, D.V.; Partin, A.W. Prediction of Prostate-Specific Antigen Recurrence in Men with Long-term Follow-up Postprostatectomy Using Quantitative Nuclear Morphometry. Cancer Epidemiol. Prev. Biomark. 2008, 17, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.; Romo-Bucheli, D.; Wang, X.; Janowczyk, A.; Ganesan, S.; Gilmore, H.; Rimm, D.; Madabhushi, A. Nuclear shape and orientation features from H&E images predict survival in early-stage estrogen receptor-positive breast cancers. Lab. Investig. J. Tech. Methods Pathol. 2018, 98, 1438–1448. [Google Scholar]
- Christens-Barry, W.A.; Partin, A.W. Quantitative Grading of Tissue and Nuclei in Prostate Cancer for Prognosis Prediction. JOHNS HOPKINS APL Tech. Dig. 1997, 18, 8. [Google Scholar]
- Veltri, R.W. Serum marker %[-2]proPSA and the Prostate Health Index improve diagnostic accuracy for clinically relevant prostate cancer. BJU Int. 2016, 117, 12–13. [Google Scholar] [CrossRef] [PubMed]
- Tosoian, J.J.; Loeb, S.; Feng, Z.; Isharwal, S.; Landis, P.; Elliot, D.J.; Veltri, R.; Epstein, J.I.; Partin, A.W.; Carter, H.B.; et al. Association of [-2]proPSA with biopsy reclassification during active surveillance for prostate cancer. J. Urol. 2012, 188, 1131–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikolajczyk, S.D.; Rittenhouse, H.G. Pro PSA: A more cancer specific form of prostate specific antigen for the early detection of prostate cancer. Keio J. Med. 2003, 52, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Heidegger, I.; Klocker, H.; Pichler, R.; Pircher, A.; Prokop, W.; Steiner, E.; Ladurner, C.; Comploj, E.; Lunacek, A.; Djordjevic, D.; et al. ProPSA and the Prostate Health Index as predictive markers for aggressiveness in low-risk prostate cancer—Results from an international multicenter study. Prostate Cancer Prostatic Dis. 2017, 20, 271–275. [Google Scholar] [CrossRef]
- Caccomo, S. FDA Allows Marketing of First Whole Slide Imaging System for Digital Pathology. Available online: https://www.fda.gov/news-events/press-announcements/fda-allows-marketing-first-whole-slide-imaging-system-digital-pathology (accessed on 7 September 2020).



{kind=link}
{kind=link}
| Feature Family | Description | Features |
|---|---|---|
| Graph | Voronoi, Delaunay, minimum spanning trees, k-NN graphs | 51 |
| Shape | Area, perimeter ratio, smoothness, distance, etc. | 100 |
| Nuclear Disorder | Orientation entropy, energy, contrast | 39 |
| Cluster Graphs | Clustering coefficient, edge length, connected components | 26 |
| Feature |
|---|
| Voronoi: Min/max polygon perimeter |
| Shape: Min/max standard deviation of distance of contour point from centroid of nuclei |
| Shape: Min/max nuclei perimeter |
| Shape: Standard deviation of Fourier descriptor 6 |
| Orientation: Tensor contrast inverse moment range |
| Voronoi: Standard deviation of polygon area |
| Predicted | ||||
|---|---|---|---|---|
| Actual | Non-Progressor | Progressor | ||
| Non-Progressor | 22 | 14 | NPV: 44% | |
| Progressor | 28 | 67 | PPV: 83% | |
| Specificity: 61% | Sensitivity: 71% | |||
| Model Type | AUC | ACC | SENS | SPEC |
|---|---|---|---|---|
| LDA | 0.68 ± 0.12 | 0.63 ± 0.11 | 0.53 ± 0.16 | 0.26 ± 0.13 |
| QDA | 0.69 ± 0.11 | 0.62 ± 0.10 | 0.58 ± 0.17 | 0.67 ± 0.16 |
| RF | 0.73 ± 0.10 | 0.75 ± 0.09 | 0.70 ± 0.17 | 0.81 ± 0.16 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandramouli, S.; Leo, P.; Lee, G.; Elliott, R.; Davis, C.; Zhu, G.; Fu, P.; Epstein, J.I.; Veltri, R.; Madabhushi, A. Computer Extracted Features from Initial H&E Tissue Biopsies Predict Disease Progression for Prostate Cancer Patients on Active Surveillance. Cancers 2020, 12, 2708. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12092708
Chandramouli S, Leo P, Lee G, Elliott R, Davis C, Zhu G, Fu P, Epstein JI, Veltri R, Madabhushi A. Computer Extracted Features from Initial H&E Tissue Biopsies Predict Disease Progression for Prostate Cancer Patients on Active Surveillance. Cancers. 2020; 12(9):2708. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12092708
Chicago/Turabian StyleChandramouli, Sacheth, Patrick Leo, George Lee, Robin Elliott, Christine Davis, Guangjing Zhu, Pingfu Fu, Jonathan I. Epstein, Robert Veltri, and Anant Madabhushi. 2020. "Computer Extracted Features from Initial H&E Tissue Biopsies Predict Disease Progression for Prostate Cancer Patients on Active Surveillance" Cancers 12, no. 9: 2708. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12092708