
Trend Shifts in Age-Specific Incidence for In Situ and Invasive Cutaneous Melanoma in Sweden

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
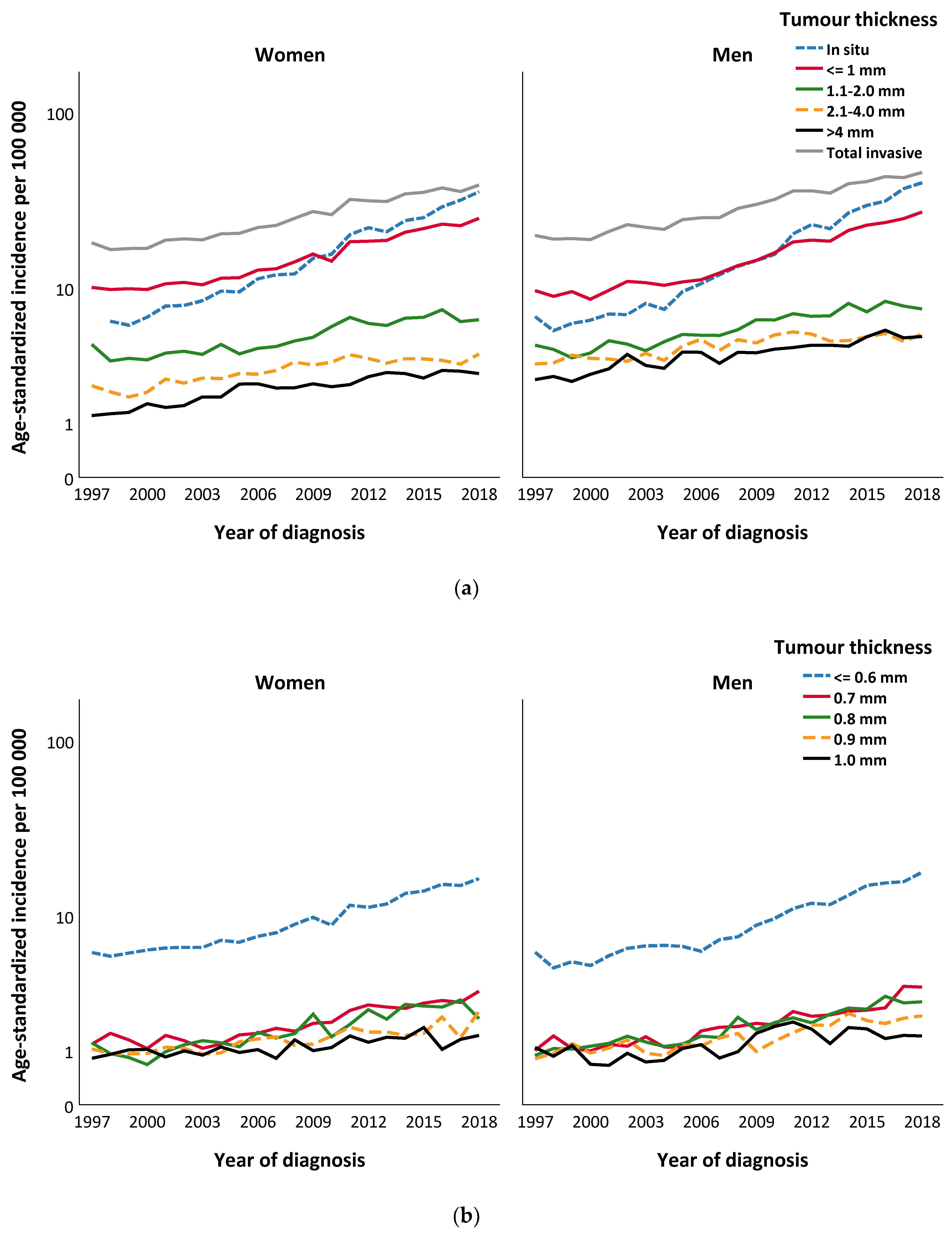
2.1. Annual Age-Standardised Incidence, 1997–2018
2.1.1. In Situ Cutaneous Melanomas
2.1.2. Invasive Cutaneous Melanomas
2.2. Incidence Trends of In Situ and Invasive Cutaneous Melanomas by Tumour Thickness
2.2.1. In Situ Cutaneous Melanomas
2.2.2. Invasive Cutaneous Melanomas
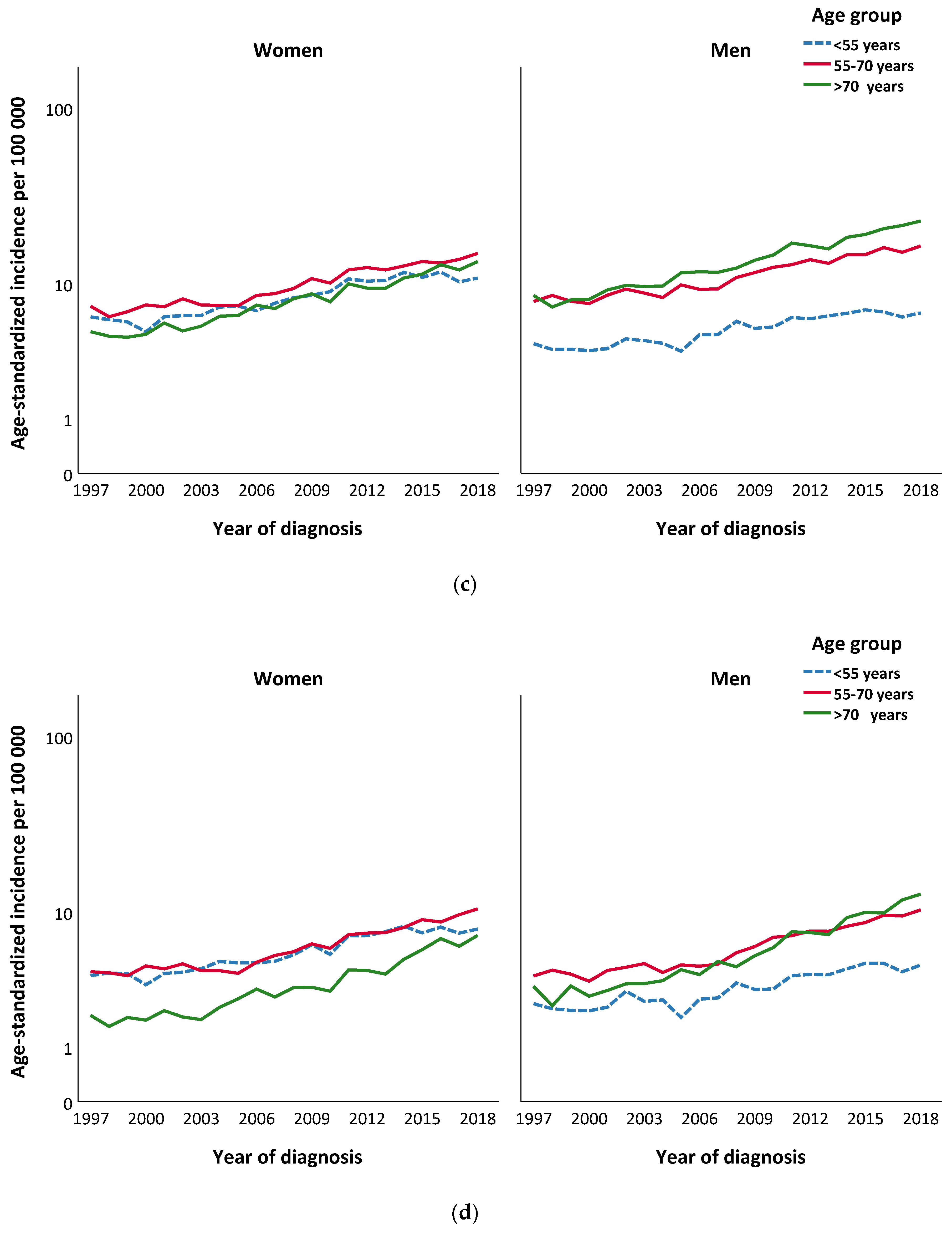
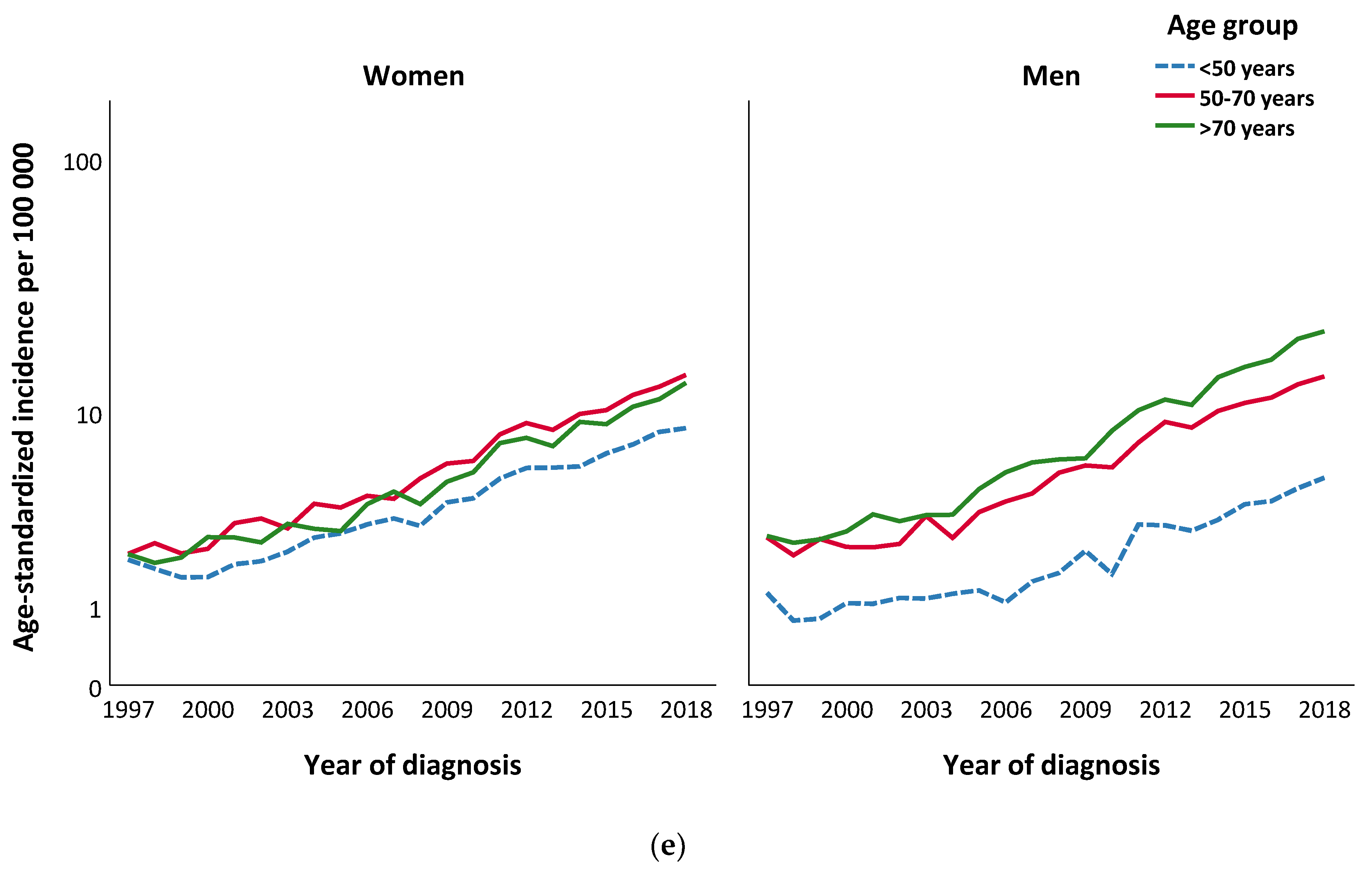
2.3. Incidence Trends of Invasive Cutaneous Melanomas by Age
3. Discussion
4. Patients and Methods
Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Aitken, J.F.; Youlden, D.R.; Baade, P.D.; Soyer, H.P.; Green, A.C.; Smithers, B.M. Generational shift in melanoma incidence and mortality in queensland, australia, 1995–2014. Int. J. Cancer 2018, 142, 1528–1535. [Google Scholar] [CrossRef]
- Whiteman, D.C.; Green, A.C.; Olsen, C.M. The growing burden of invasive melanoma: Projections of incidence rates and numbers of new cases in six susceptible populations through 2031. J. Investig. Dermatol. 2016, 136, 1161–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdmann, F.; Lortet-Tieulent, J.; Schuz, J.; Zeeb, H.; Greinert, R.; Breitbart, E.W.; Bray, F. International trends in the incidence of malignant melanoma 1953–2008—Are recent generations at higher or lower risk? Int. J. Cancer 2013, 132, 385–400. [Google Scholar] [CrossRef]
- Nikolaou, V.; Stratigos, A.J. Emerging trends in the epidemiology of melanoma. Br. J. Dermatol. 2014, 170, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; de Vries, E.; Whiteman, D.C.; Jemal, A.; Bray, F.; Parkin, D.M.; Soerjomataram, I. Global burden of cutaneous melanoma attributable to ultraviolet radiation in 2012. Int. J. Cancer 2018, 143, 1305–1314. [Google Scholar] [CrossRef]
- Lucas, R.M.; McMichael, A.J.; Armstrong, B.K.; Smith, W.T. Estimating the global disease burden due to ultraviolet radiation exposure. Int. J. Epidemiol. 2008, 37, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.K.; Kricker, A. How much melanoma is caused by sun exposure? Melanoma Res. 1993, 3, 395–401. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Ingested nitrate and nitrite, and cyanobacterial peptide toxins. IARC Monogr. Eval. Carcinog. Risks Hum. 2010, 94, 448. [Google Scholar]
- Stanton, W.R.; Janda, M.; Baade, P.D.; Anderson, P. Primary prevention of skin cancer: A review of sun protection in australia and internationally. Health Promot Int. 2004, 19, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Smith, T. The queensland melanoma project—An exercise in health education. Br. Med. J. 1979, 1, 253–254. [Google Scholar] [CrossRef] [Green Version]
- Iannacone, M.R.; Green, A.C. Towards skin cancer prevention and early detection: Evolution of skin cancer awareness campaigns in australia. Melanoma Manag. 2014, 1, 75–84. [Google Scholar] [CrossRef]
- Arnold, M.; Holterhues, C.; Hollestein, L.M.; Coebergh, J.W.; Nijsten, T.; Pukkala, E.; Holleczek, B.; Tryggvadottir, L.; Comber, H.; Bento, M.J.; et al. Trends in incidence and predictions of cutaneous melanoma across europe up to 2015. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1170–1178. [Google Scholar] [CrossRef]
- Sacchetto, L.; Zanetti, R.; Comber, H.; Bouchardy, C.; Brewster, D.H.; Broganelli, P.; Chirlaque, M.D.; Coza, D.; Galceran, J.; Gavin, A.; et al. Trends in incidence of thick, thin and in situ melanoma in europe. Eur. J. Cancer 2018, 92, 108–118. [Google Scholar] [CrossRef] [Green Version]
- Toender, A.; Kjaer, S.K.; Jensen, A. Increased incidence of melanoma in situ in denmark from 1997 to 2011: Results from a nationwide population-based study. Melanoma Res. 2014, 24, 488–495. [Google Scholar] [CrossRef]
- Podlipnik, S.; Carrera, C.; Boada, A.; Richarz, N.; Marcoval, J.; Ferreres, J.R.; Bodet, D.; Marti, R.M.; Segura, S.; Sabat, M.; et al. Incidence of melanoma in catalonia, spain, is rapidly increasing in the elderly population. A multicentric cohort study. J. Clin. Med. 2020, 9, 3396. [Google Scholar] [CrossRef] [PubMed]
- Guy, G.P., Jr.; Ekwueme, D.U.; Tangka, F.K.; Richardson, L.C. Melanoma treatment costs: A systematic review of the literature, 1990–2011. Am. J. Prev. Med. 2012, 43, 537–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyth, J.; Carstensen, J.; Synnerstad, I.; Lindholm, C. Stage-specific direct health care costs in patients with cutaneous malignant melanoma. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 789–793. [Google Scholar] [CrossRef]
- Buja, A.; Sartor, G.; Scioni, M.; Vecchiato, A.; Bolzan, M.; Rebba, V.; Sileni, V.C.; Palozzo, A.C.; Montesco, M.; Del Fiore, P.; et al. Estimation of direct melanoma-related costs by disease stage and by phase of diagnosis and treatment according to clinical guidelines. Acta Derm. Venereol. 2018, 98, 218–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbe, C.; Keim, U.; Eigentler, T.K.; Amaral, T.; Katalinic, A.; Holleczek, B.; Martus, P.; Leiter, U. Time trends in incidence and mortality of cutaneous melanoma in germany. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1272–1280. [Google Scholar] [CrossRef]
- Ghazawi, F.M.; Cyr, J.; Darwich, R.; Le, M.; Rahme, E.; Moreau, L.; Netchiporouk, E.; Zubarev, A.; Roshdy, O.; Glassman, S.J.; et al. Cutaneous malignant melanoma incidence and mortality trends in canada: A comprehensive population-based study. J. Am. Acad. Dermatol. 2019, 80, 448–459. [Google Scholar] [CrossRef]
- Lazovich, D.; Choi, K.; Vogel, R.I. Time to get serious about skin cancer prevention. Cancer Epidemiol. Biomarkers Prev. 2012, 21, 1893–1901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berge, L.A.M.; Andreassen, B.K.; Stenehjem, J.S.; Heir, T.; Furu, K.; Juzeniene, A.; Roscher, I.; Larsen, I.K.; Green, A.C.; Veierod, M.B.; et al. Use of antidepressants and risk of cutaneous melanoma: A prospective registry-based case-control study. Clin. Epidemiol. 2020, 12, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaune, E.; Rocchi, S. Metformin: Focus on melanoma. Front. Endocrinol. (Lausanne) 2018, 9, 472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, N.M.; Vincent, L.T.; Rodriguez, G.A.; Nouri, K. Antihypertensives and melanoma: An updated review. Pigment Cell Melanoma Res. 2020, 33, 806–813. [Google Scholar] [CrossRef]
- Sarrabayrouse, G.; Pich, C.; Teiti, I.; Tilkin-Mariame, A.F. Regulatory properties of statins and rho gtpases prenylation inhibitiors to stimulate melanoma immunogenicity and promote anti-melanoma immune response. Int. J. Cancer 2017, 140, 747–755. [Google Scholar] [CrossRef]
- Huber, V.; Camisaschi, C.; Berzi, A.; Ferro, S.; Lugini, L.; Triulzi, T.; Tuccitto, A.; Tagliabue, E.; Castelli, C.; Rivoltini, L. Cancer acidity: An ultimate frontier of tumor immune escape and a novel target of immunomodulation. Semin. Cancer Biol. 2017, 43, 74–89. [Google Scholar] [CrossRef]
- De Milito, A.; Canese, R.; Marino, M.L.; Borghi, M.; Iero, M.; Villa, A.; Venturi, G.; Lozupone, F.; Iessi, E.; Logozzi, M.; et al. Ph-dependent antitumor activity of proton pump inhibitors against human melanoma is mediated by inhibition of tumor acidity. Int. J. Cancer 2010, 127, 207–219. [Google Scholar] [CrossRef]
- Grygier, B.; Arteta, B.; Kubera, M.; Basta-Kaim, A.; Budziszewska, B.; Leskiewicz, M.; Curzytek, K.; Duda, W.; Lason, W.; Maes, M. Inhibitory effect of antidepressants on b16f10 melanoma tumor growth. Pharmacol. Rep. 2013, 65, 672–681. [Google Scholar] [CrossRef] [Green Version]
- Eggen, C.A.M.; Durgaram, V.V.L.; van Doorn, R.; Mooi, W.J.; Pardo, L.M.; Pasmans, S.; Hollestein, L.M. Incidence and relative survival of melanoma in children and adolescents in the netherlands, 1989–2013. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 956–961. [Google Scholar] [CrossRef]
- Paulson, K.G.; Gupta, D.; Kim, T.S.; Veatch, J.R.; Byrd, D.R.; Bhatia, S.; Wojcik, K.; Chapuis, A.G.; Thompson, J.A.; Madeleine, M.M.; et al. Age-specific incidence of melanoma in the united states. JAMA Dermatol. 2019, 156, 57–64. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Haines, J.; O’Brien, A.; McDonald, J.; Price, S.; Sherry, B.; Taveras, E.M. Systematic review of effective strategies for reducing screen time among young children. Obesity (Silver Spring) 2012, 20, 1338–1354. [Google Scholar] [CrossRef]
- McCurdy, L.E.; Winterbottom, K.E.; Mehta, S.S.; Roberts, J.R. Using nature and outdoor activity to improve children’s health. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 102–117. [Google Scholar] [CrossRef]
- Mocellin, S.; Nitti, D. Cutaneous melanoma in situ: Translational evidence from a large population-based study. Oncologist 2011, 16, 896–903. [Google Scholar] [CrossRef] [Green Version]
- Isaksson, K.; Mikiver, R.; Eriksson, H.; Lapins, J.; Nielsen, K.; Ingvar, C.; Lyth, J. Survival in 31,670 patients with thin melanomas: A swedish population-based study. Br. J. Dermatol. 2021, 184, 60–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, H.G.; Mazer, B.L.; Adamson, A.S. The rapid rise in cutaneous melanoma diagnoses. N. Engl. J. Med. 2021, 384, 72–79. [Google Scholar] [CrossRef]
- Forsea, A.M.; Tschandl, P.; Zalaudek, I.; Del Marmol, V.; Soyer, H.P.; Eurodermoscopy Working, G.; Argenziano, G.; Geller, A.C. The impact of dermoscopy on melanoma detection in the practice of dermatologists in europe: Results of a pan-european survey. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Kittler, H.; Pehamberger, H.; Wolff, K.; Binder, M. Diagnostic accuracy of dermoscopy. Lancet Oncol. 2002, 3, 159–165. [Google Scholar] [CrossRef]
- Vestergaard, M.E.; Macaskill, P.; Holt, P.E.; Menzies, S.W. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: A meta-analysis of studies performed in a clinical setting. Br. J. Dermatol. 2008, 159, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Elmore, J.G.; Barnhill, R.L.; Elder, D.E.; Longton, G.M.; Pepe, M.S.; Reisch, L.M.; Carney, P.A.; Titus, L.J.; Nelson, H.D.; Onega, T.; et al. Pathologists’ diagnosis of invasive melanoma and melanocytic proliferations: Observer accuracy and reproducibility study. BMJ 2017, 357, j2813. [Google Scholar] [CrossRef] [Green Version]
- Farmer, E.R.; Gonin, R.; Hanna, M.P. Discordance in the histopathologic diagnosis of melanoma and melanocytic nevi between expert pathologists. Hum. Pathol. 1996, 27, 528–531. [Google Scholar] [CrossRef]
- Swedish Melanoma Registry (SweMR–Svenska Melanomregistret). Available online: https://cancercentrum.se/globalassets/om-rcc/sydost/pdf/swemr-1990-2019.pdf (accessed on 27 May 2021).
- Lindholm, C.; Andersson, R.; Dufmats, M.; Hansson, J.; Ingvar, C.; Moller, T.; Sjodin, H.; Stierner, U.; Wagenius, G.; Swedish Melanoma Study Group. Invasive cutaneous malignant melanoma in sweden, 1990–1999. A prospective, population-based study of survival and prognostic factors. Cancer 2004, 101, 2067–2078. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the american joint committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- National Cancer Institute. Joinpoint Regression Program, Version 4.6.0.0; Statistical Methodology and Applications Branch, Surveillance Research Program; National Cancer Institute: Bethesda, MD, USA, April 2018. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 27 May 2021).
- National Cancer Institute. Permutation Test Details; National Cancer Institute: Bethesda, MD, USA. Available online: https://surveillance.Cancer.Gov/help/joinpoint/setting-parameters/method-and-parameters-tab/model-selection-method/permutation-tests/permutation-test-details (accessed on 27 May 2021).




{kind=link}
{kind=link}
{kind=link}
| Clinico-Pathological Characteristics | All CM N (%) | CM in Women N (%) | CM in Men N (%) |
|---|---|---|---|
| In situ CM | 35,350 | 18,110 (51.2) | 17,240 (48.8) |
| Age (median IQR) | 67.0 (55.0; 76.0) | 65.0 (52.0; 75.0) | 69.0 (59.0; 77.0) |
| Age group | |||
| <50 years | 6585 (18.6) | 4220 (23.3) | 2365 (13.7) |
| 50–70 years | 14,413 (40.8) | 7200 (39.8) | 7213 (41.8) |
| >70 years | 14,352 (40.6) | 6690 (36.9%) | 7662 (44.4) |
| Invasive CM | 59,932 | 29,503 (49.2) | 30,429 (50.8) |
| Age (median IQR) | 65.0 (51.0; 75.0) | 62.0 (48.0; 75.0) | 67.0 (55.0; 76.0) |
| Age group (years) | |||
| <50 | 14,100 (23.5) | 8607 (29.2) | 5493 (18.1) |
| 50–70 | 23,866 (39.8) | 11,104 (37.6) | 12,762 (41.9) |
| >70 | 21,965 (36.7) | 9792 (33.2) | 12,173 (40.0) |
| Breslow tumour thickness (mm; median IQR) | 0.90 (0.50; 2.00) | 0.8(0.5; 1.70) | 1.00 (0.5; 2.2) |
| Ulceration status | |||
| Absent | 42,895 (71.6) | 21,471 (72.8) | 21,424 (70.4) |
| Present | 10,702 (17.9) | 4749 (16.1) | 5953 (19.6) |
| Missing | 6335 (10.6) | 3283 (11.1) | 3052 (10.0) |
| Histopathologic subtype | |||
| SSM | 36,649 (61.2) | 18,445 (62.5) | 18,204 (59.8) |
| NM | 4100 (6.8) | 2024 (6.86) | 2076 (6.82) |
| LM | 9548 (15.9) | 4194 (14.2) | 5354 (17.6) |
| ALM | 667 (1.1) | 402 (1.4) | 265 (0.9) |
| Other | 7281 (12.1) | 3590 (12.2) | 3691 (12.1) |
| Missing | 1687 (2.8) | ||
| T-stage | |||
| TX | 2015 (3.4) | 1055 (3.6) | 960 (3.2) |
| T1 | 2032 (3.4) | 1117 (3.8) | 915 (3.0) |
| T1a | 21,352 (35.6) | 11,118 (37.7) | 10,234 (33.6) |
| T1b | 9450 (15.8) | 4755 (16.1) | 4695 (15.4) |
| T2 | 1046 (1.8) | 540 (1.8) | 506 (1.7) |
| T2a | 8298 (13.8) | 4017 (13.6) | 4281 (14.1) |
| T2b | 2046 (3.4) | 990 (3.4) | 1056 (3.5) |
| T3 | 622 (1.0) | 281 (1.0) | 341 (1.4) |
| T3a | 3674 (6.1) | 1699 (5.8) | 1975 (6.5) |
| T3b | 3260 (5.4) | 1365 (4.6) | 1895 (6.2) |
| T4 | 408 (0.68) | 167 (0.6) | 241 (0.8) |
| T4a | 1796 (3.0) | 743 (2.5) | 1053 (3.5) |
| T4b | 3933 (6.6) | 1656 (5.6) | 2277 (7.5) |
| (a) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All Ages | Women | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | APC2 | UCL | LCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 4.5 | 4.1 | 5.0 | <0.001 | - | - | - | - | - | - | - | - | |
| ≤0.6 | 5.4 | 4.5 | 6.3 | <0.001 | 2.9 | 0.8 | 5.1 | 0.009 | 2005 | 7.0 | 6.2 | 7.7 | <0.001 |
| 0.7 | 4.4 | 2.6 | 6.2 | <0.001 | −1.0 | −6.6 | 5.0 | 0.724 | 2003 | 6.6 | 5.4 | 7.8 | <0.001 |
| 0.8 | 5.7 | 4.3 | 7.0 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.9 | 3.8 | 2.7 | 4.8 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.0 | 2.5 | 1.5 | 3.5 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 3.6 | 2.8 | 4.4 | <0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 2.9 | 1.9 | 3.9 | <0.001 | 4.5 | 3.4 | 5.5 | <0.001 | 2011 | −0.1 | −2.4 | 2.2 | 0.904 |
| >4 | 4.6 | 3.5 | 5.6 | <0.001 | 7.7 | 5.1 | 10.4 | <0.001 | 2005 | 2.6 | 1.8 | 3.5 | <0.001 |
| Missing | 2.5 | −0.0 | 5.1 | 0.053 | 8.4 | 4.8 | 12.1 | <0.001 | 2009 | −4.9 | −8.9 | −0.6 | 0.027 |
| In situ | 10.0 | 9.4 | 10.5 | <0.001 | - | - | - | - | - | - | - | - | - |
| All Ages | Men | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | APC2 | LCL | UCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 4.2 | 3.0 | 5.4 | <0.001 | −0.4 | −8.4 | 8.3 | 0.920 | 2000 | 5.0 | 4.6 | 5.4 | <0.001 |
| ≤0.6 | 6.3 | 5.2 | 7.4 | <0.001 | 3.2 | 0.9 | 5.5 | 0.009 | 2006 | 8.7 | 7.7 | 9.8 | <0.001 |
| 0.7 | 6.4 | 4.2 | 8.7 | <0.001 | 5.0 | 3.7 | 6.4 | <0.001 | 2015 | 15.2 | 0.4 | 32.2 | 0.044 |
| 0.8 | 5.6 | 4.8 | 6.4 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.9 | 4.4 | 3.4 | 5.5 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.0 | 3.3 | 1.6 | 5.0 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 3.9 | 3.3 | 4.5 | <0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 2.1 | 1.1 | 3.2 | <0.001 | 3.4 | 2.3 | 4.5 | <0.001 | 2011 | −0.4 | −2.8 | 2.1 | 0.753 |
| >4 | 3.4 | 2.8 | 4.0 | <0.001 | - | - | - | - | - | - | - | - | |
| Missing | 2.3 | −0.6 | 5.3 | 0.119 | 6.7 | 2.7 | 11.0 | 0.003 | 2009 | −3.3 | −8.0 | 1.6 | 0.168 |
| In situ | 10.2 | 8.8 | 11.6 | <0.001 | 2.4 | −2.6 | 7.7 | 0.334 | 2002 | 12.8 | 11.9 | 13.7 | <0.001 |
| (b) | |||||||||||||
| Age Group: <50 | Women | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | AAPC | LCL | UCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 3.3 | 1.9 | 4.8 | <0.001 | 4.4 | 3.6 | 5.2 | <0.001 | 2015 | –2.9 | –11. | 6.7 | 0.513 |
| ≤0.6 | 4.8 | 4.1 | 5.4 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.7 | 3.7 | 2.3 | 5.2 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.8 | 1.5 | –5.6 | 9.2 | 0.680 | 5.5 | 3.0 | 8.1 | <0.001 | 2016 | –29.4 | –68.1 | 55. | 0.366 |
| 0.9 | 3.8 | 2.1 | 5.5 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.0 | 1.1 | –0.8 | 3.1 | 0.247 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 2.8 | 1.4 | 4.2 | <0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 3.7 | 2.5 | 4.9 | <0.001 | - | - | - | - | - | - | - | - | - |
| >4 | 2.2 | –0.1 | 4.7 | 0.061 | - | - | - | - | - | - | - | - | - |
| Missing | 1.4 | –3.2 | 6.4 | 0.552 | 7.6 | 3.1 | 12. | 0.002 | 2012 | –12.6 | –24.2 | 0.8 | 0.063 |
| Age Group: <50 | Men | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | AAPC | LCL | UCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 3.1 | 2.5 | 3.6 | <0.001 | - | - | - | - | - | - | - | - | - |
| ≤0.6 | 4.4 | 3.3 | 5.6 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.7 | 4.1 | 2.4 | 5.8 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.8 | 2.9 | 1.2 | 4.7 | 0.002 | - | - | - | - | - | - | - | - | - |
| 0.9 | 2.5 | 0.9 | 4.0 | 0.002 | - | - | - | - | - | - | - | - | - |
| 1.0 | 2.4 | 0.8 | 4.0 | 0.005 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 2.3 | 1.1 | 3.5 | 0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 0.8 | –0.4 | 2.1 | 0.200 | - | - | - | - | - | - | - | - | - |
| >4 | 0.1 | –1.6 | 1.9 | 0.886 | - | - | - | - | - | - | - | - | - |
| Missing | 0.9 | –4.73 | 6.9 | 0.749 | 10.6 | 1.9 | 20.2 | 0.019 | 2008 | –8.76 | –16.9 | 0.2 | 0.055 |
| (c) | |||||||||||||
| Age Group: 50–70 | Women | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | AAPC | LCL | UCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 4.8 | 3.6 | 6.0 | <0.001 | 1.3 | −1.5 | 4.1 | 0.344 | 2005 | 7.0 | 6.0 | 8.1 | <0.001 |
| ≤0.6 | 5.1 | 3.5 | 6.7 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.7 | 5.7 | 4.2 | 7.3 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.8 | 2.6 | 1.5 | 3.8 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.9 | 2.6 | 1.3 | 3.9 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.0 | 3.6 | 2.7 | 4.6 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 2.5 | 1.3 | 3.7 | <0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 2.7 | 1.4 | 4.1 | <0.001 | - | - | - | - | - | - | - | - | - |
| >4 | 1.8 | −2.9 | 6.9 | 0.449 | 8.2 | 2.2 | 14. | 0.010 | 2010 | −7.6 | −16.4 | 1.9 | 0.108 |
| Missing | 3.9 | 2.9 | 5.0 | <0.001 | 2.0 | −0.7 | 4.9 | 0.144 | 2004 | 4.9 | 4.1 | 5.7 | <0.001 |
| Age Group: 50–70 | Men | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | AAPC | LCL | UCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 5.8 | 4.7 | 6.9 | <0.001 | 3.7 | 1.4 | 6.1 | 0.003 | 2006 | 7.4 | 6.3 | 8.5 | <0.001 |
| ≤0.6 | 4.4 | 2.1 | 6.7 | <0.001 | −0.3 | −5.6 | 5.2 | 0.909 | 2005 | 7.4 | 5.3 | 9.4 | 0.000 |
| 0.7 | 4.8 | 3.6 | 6.0 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.8 | 3.4 | 2.0 | 4.8 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.9 | 2.2 | 0.3 | 4.1 | 0.023 | - | - | - | - | - | - | - | - | - |
| 1.0 | 3.6 | 2.9 | 4.3 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 1.8 | 0.9 | 2.7 | <0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 2.2 | 1.2 | 3.2 | <0.001 | - | - | - | - | - | - | - | - | - |
| >4 | 1.4 | −1.16 | 4.0 | 0.267 | - | - | - | - | - | - | - | - | - |
| Missing | 4.1 | 3.7 | 4.6 | <0.001 | - | - | - | - | - | - | - | - | - |
| (d) | |||||||||||||
| Age Group: >70 | Women | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | AAPC | LCL | UCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 5.5 | 5.0 | 6.0 | <0.001 | - | - | - | - | - | - | - | - | - |
| ≤0.6 | 8.2 | 7.1 | 9.3 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.7 | 7.8 | 6.0 | 9.7 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.8 | 6.3 | 1.4 | 11. | 0.010 | 9.2 | 7.0 | 11.5 | <0.001 | 2016 | −17.9 | −49.8 | 34. | 0.410 |
| 0.9 | 5.8 | 4.1 | 7.6 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.0 | 3.9 | 2.3 | 5.5 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 4.2 | 3.4 | 5.1 | <0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 3.0 | 2.1 | 4.0 | <0.001 | - | - | - | - | - | - | - | - | - |
| >4 | 5.2 | 3.8 | 6.6 | <0.001 | 7.6 | 4.6 | 10. | <0.001 | 2006 | 3.4 | 2.1 | 4.8 | <0.001 |
| Missing | 2.3 | 0.0 | 4.7 | 0.043 | - | - | - | - | - | - | - | - | - |
| Age Group: >70 | Men | ||||||||||||
| 1997–2018 | Period 1 | Y | Period 2 | ||||||||||
| AAPC | LCL | UCL | p-Value | APC1 | LCL | UCL | p-Value | AAPC | LCL | UCL | p-Value | ||
| Tumour Thickness | |||||||||||||
| All | 5.7 | 5.3 | 6.1 | <0.001 | - | - | - | - | - | - | - | - | - |
| ≤0.6 | 6.9 | 4.2 | 9.6 | <0.001 | −6.1 | −18.2 | 7.6 | 0.340 | 2001 | 10.2 | 9.1 | 11.4 | <0.001 |
| 0.7 | 8.3 | 6.1 | 10.6 | <0.001 | 6.0 | 4.5 | 7.6 | <0.001 | 2015 | 23.2 | 7.9 | 40.7 | 0.004 |
| 0.8 | 8.0 | 6.2 | 9.7 | <0.001 | - | - | - | - | - | - | - | - | - |
| 0.9 | 6.5 | 4.6 | 8.4 | <0.001 | - | - | - | - | - | - | - | - | - |
| 1.0 | 4.6 | 1.8 | 7.4 | 0.002 | - | - | - | - | - | - | - | - | - |
| 1.1–2.0 | 4.8 | 3.8 | 5.8 | <0.001 | - | - | - | - | - | - | - | - | - |
| 2.1–4.0 | 2.7 | 1.9 | 3.5 | <0.001 | - | - | - | - | - | - | - | - | - |
| >4 | 4.1 | 3.3 | 5.0 | <0.001 | - | - | - | - | - | - | - | - | - |
| Missing | 2.5 | 0.4 | 4.6 | 0.018 | - | - | - | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eriksson, H.; Nielsen, K.; Vassilaki, I.; Lapins, J.; Mikiver, R.; Lyth, J.; Isaksson, K. Trend Shifts in Age-Specific Incidence for In Situ and Invasive Cutaneous Melanoma in Sweden. Cancers 2021, 13, 2838. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13112838
Eriksson H, Nielsen K, Vassilaki I, Lapins J, Mikiver R, Lyth J, Isaksson K. Trend Shifts in Age-Specific Incidence for In Situ and Invasive Cutaneous Melanoma in Sweden. Cancers. 2021; 13(11):2838. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13112838
Chicago/Turabian StyleEriksson, Hanna, Kari Nielsen, Ismini Vassilaki, Jan Lapins, Rasmus Mikiver, Johan Lyth, and Karolin Isaksson. 2021. "Trend Shifts in Age-Specific Incidence for In Situ and Invasive Cutaneous Melanoma in Sweden" Cancers 13, no. 11: 2838. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13112838