
Molecular Classification to Prognosticate Response in Medically Managed Endometrial Cancers and Endometrial Intraepithelial Neoplasia

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
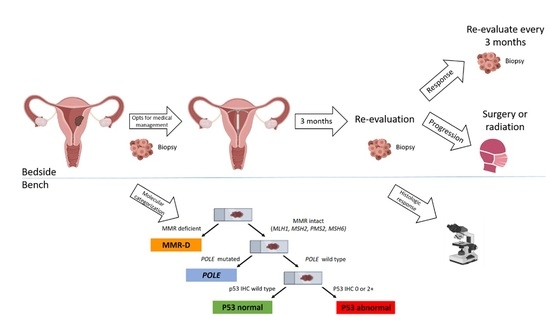
2.1. Application of ProMisE Algorithm
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
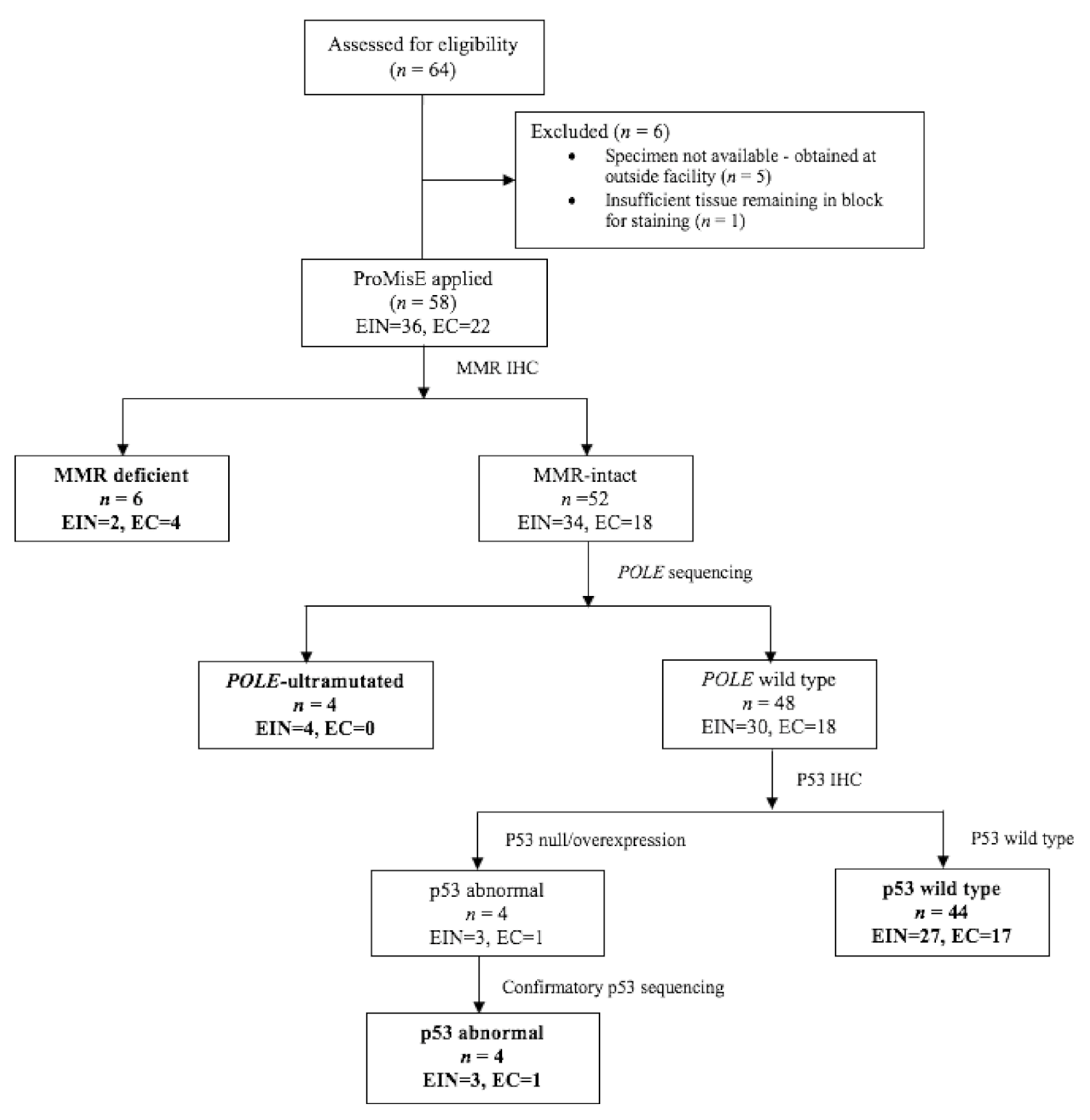
3.2. Molecular Classification
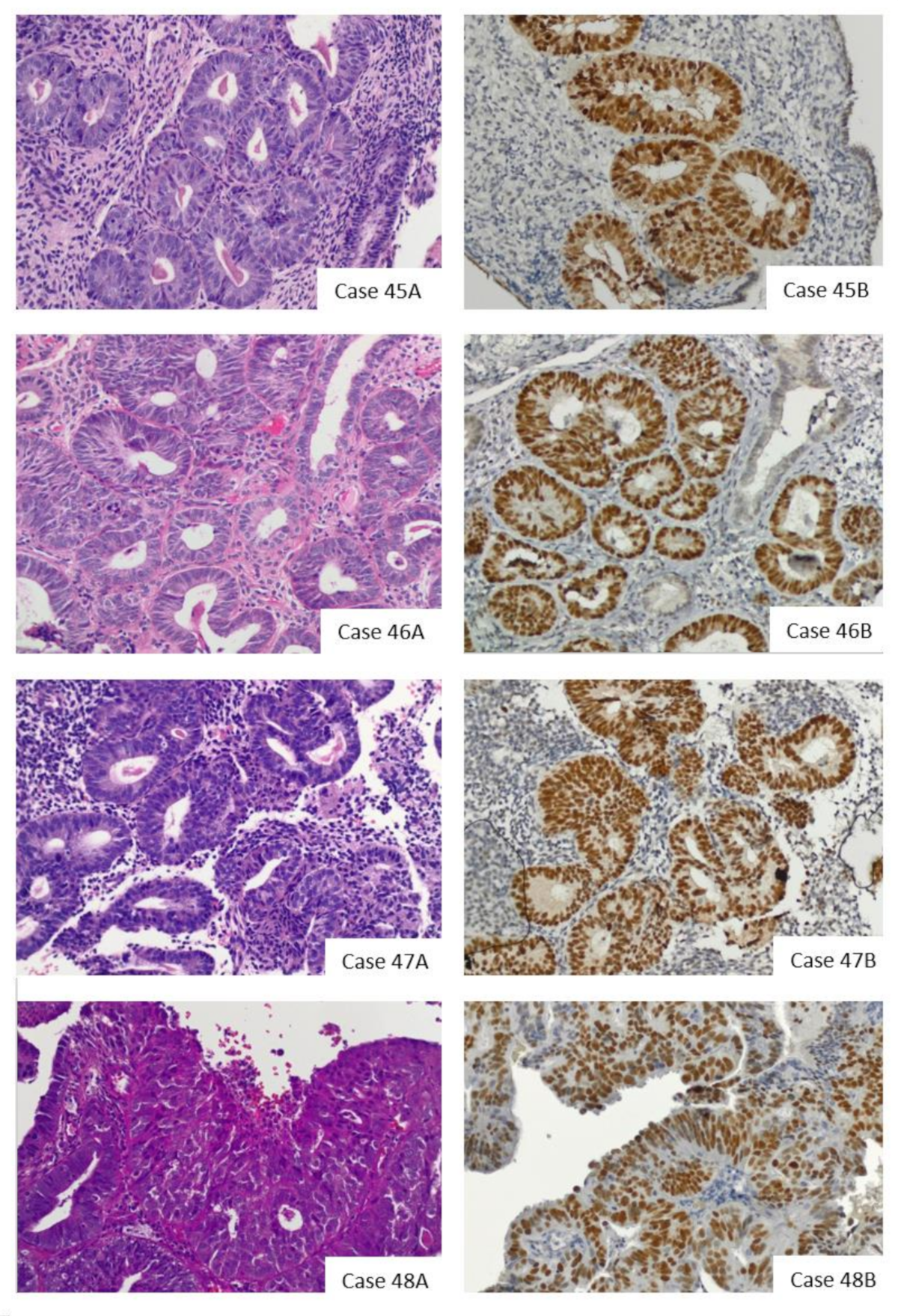
3.3. POLE Mutations
3.4. p53 Immunohistochemistry
3.5. Mismatch Repair Immunohistochemistry
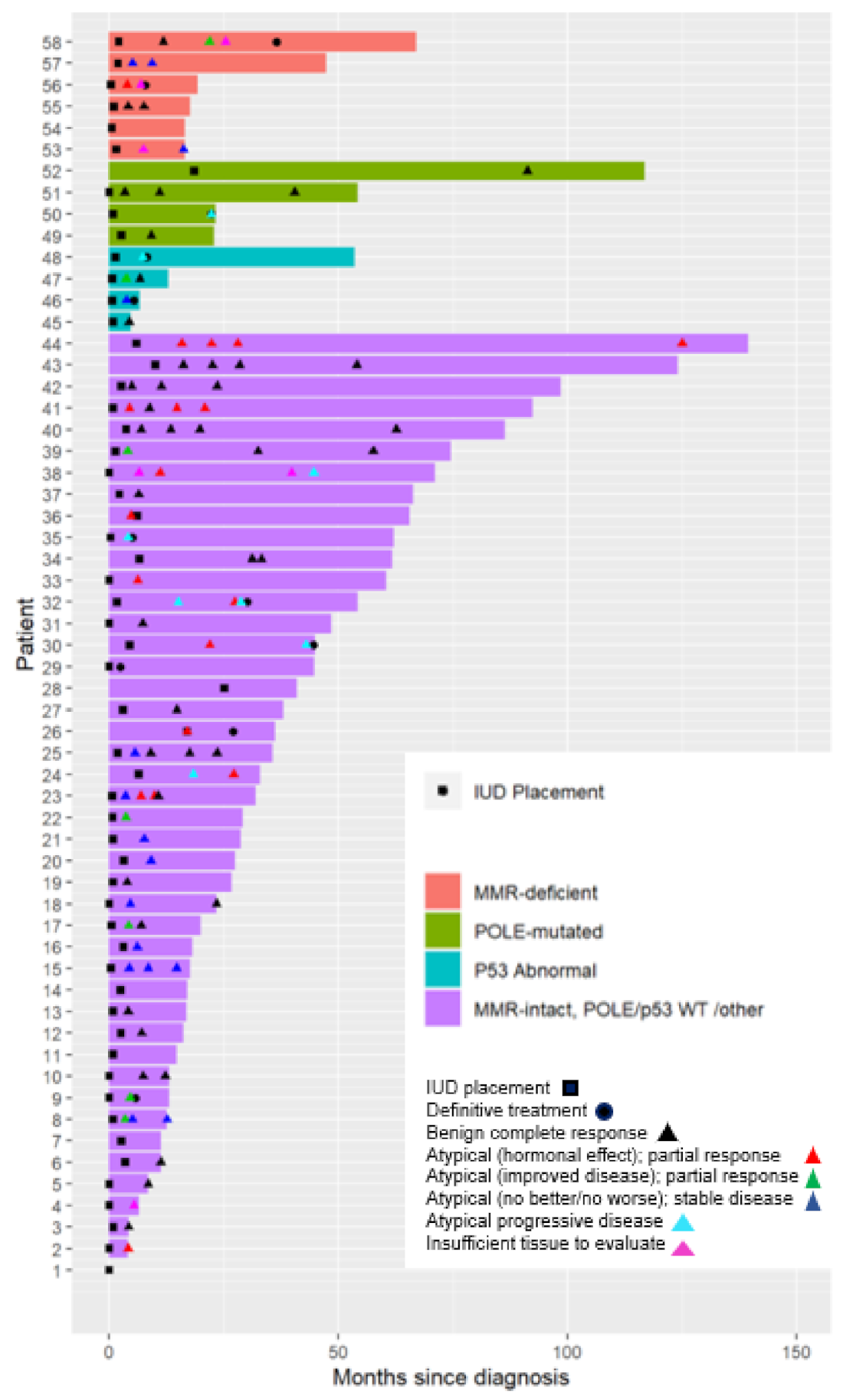
3.6. Treatment Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Comprehensive Cancer Network. Uterine Cancer (Version 1.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdg/uterine.prf (accessed on 26 March 2020).
- Gallos, I.D.; Krishan, P.; Shehmar, M.; Ganesan, R.; Gupta, J.K. LNG-IUS versus oral progestogen treatment for endometrial hyperplasia: A long-term comparative cohort study. Hum. Reprod. 2013, 28, 2966–2971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pronin, S.M.; Novikova, O.V.; Andreeva, J.Y.; Novikova, E.G. Fertility-Sparing Treatment of Early Endometrial Cancer and Complex Atypical Hyperplasia in Young Women of Childbearing Potential. Int. J. Gynecol. Cancer 2015, 25, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Montz, F.J.; Bristow, R.E.; Bovicelli, A.; Tomacruz, R.; Kurman, R.J. Intrauterine progesterone treatment of early endometrial cancer. Am. J. Obstet. Gynecol. 2002, 186, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Seong, S.J.; Kim, Y.S.; Song, T.; Yoon, B.S.; Jun, H.S.; Lee, Y.H. Combined medroxyprogesterone acetate/levonorgestrel-intrauterine system treatment in young women with early-stage endometrial cancer. Am. J. Obstet. Gynecol. 2013, 209, 358.e1–358.e4. [Google Scholar] [CrossRef]
- Hashim, H.A.; Ghayaty, E.; El Rakhawy, M. Levonorgestrel-releasing intrauterine system vs oral progestins for non-atypical endometrial hyperplasia: A systematic review and metaanalysis of randomized trials. Am. J. Obstet. Gynecol. 2015, 213, 469–478. [Google Scholar] [CrossRef]
- Ørbo, A.; Vereide, A.B.; Arnes, M.; Pettersen, I.; Straume, B. Levonorgestrel-impregnated intrauterine device as treatment for endometrial hyperplasia: A national multicentre randomised trial. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 477–486. [Google Scholar] [CrossRef] [Green Version]
- Wildemeersch, D.; Janssens, D.; Pylyser, K.; De Wever, N.; Verbeeck, G.; Dhont, M.; Tjalma, W. Management of patients with non-atypical and atypical endometrial hyperplasia with a levonorgestrel-releasing intrauterine system: Long-term follow-up. Maturitas 2007, 57, 210–213. [Google Scholar] [CrossRef]
- Varma, R.; Soneja, H.; Bhatia, K.; Ganesan, R.; Rollason, T.; Clark, T.J.; Gupta, J.K. The effectiveness of a levonorgestrel-releasing intrauterine system (LNG-IUS) in the treatment of endometrial hyperplasia—A long-term follow-up study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 139, 169–175. [Google Scholar] [CrossRef]
- Westin, S.N.; Fellman, B.; Sun, C.C.; Broaddus, R.R.; Woodall, M.L.; Pal, N.; Urbauer, D.L.; Ramondetta, L.M.; Schmeler, K.M.; Soliman, P.T.; et al. Prospective phase II trial of levonorgestrel intrauterine device: Nonsurgical approach for complex atypical hyperplasia and early-stage endometrial cancer. Am. J. Obstet. Gynecol. 2021, 224, 191.e1–191.e15. [Google Scholar] [CrossRef]
- Obermair, A. Complete Pathologic Response Following Levonorgestrel Intrauterine Device in Clinically Stage I Endometrial Adenocarcinoma: Results of a Randomized Control Trial. Society of Gynecologic Oncology Annual Meeting, Virtual Meeting. 19–21 March 2021. [Google Scholar]
- Park, J.Y.; Kim, D.Y.; Kim, J.H.; Kim, Y.M.; Kim, K.R.; Kim, Y.T.; Seong, S.J.; Kim, T.J.; Kim, J.W.; Kim, S.M.; et al. Long-term oncologic outcomes after fertility-sparing management using oral progestin for young women with endometrial cancer (KGOG 2002). Eur. J. Cancer 2013, 49, 868–874. [Google Scholar] [CrossRef]
- Ushijima, K.; Yahata, H.; Yoshikawa, H.; Konishi, I.; Yasugi, T.; Saito, T.; Nakanishi, T.; Sasaki, H.; Saji, F.; Iwasaka, T.; et al. Multicenter Phase II Study of Fertility-Sparing Treatment with Medroxyprogesterone Acetate for Endometrial Carcinoma and Atypical Hyperplasia in Young Women. J. Clin. Oncol. 2007, 25, 2798–2803. [Google Scholar] [CrossRef]
- Raffone, A.; Travaglino, A.; Flacco, M.E.; Iasevoli, M.; Mollo, A.; Guida, M.; Insabato, L.; Sardo, A.D.S.; Carugno, J.; Zullo, F. Clinical Predictive Factors of Response to Treatment in Patients Undergoing Conservative Management of Atypical Endometrial Hyperplasia and Early Endometrial Cancer. J. Adolesc. Young Adult Oncol. 2021, 10, 193–201. [Google Scholar] [CrossRef]
- Koskas, M.; Uzan, J.; Luton, D.; Rouzier, R.; Daraï, E. Prognostic factors of oncologic and reproductive outcomes in fertility-sparing management of endometrial atypical hyperplasia and adenocarcinoma: Systematic review and meta-analysis. Fertil. Steril. 2014, 101, 785–794.e3. [Google Scholar] [CrossRef]
- Raffone, A.; Travaglino, A.; Zullo, F.M.; Gencarelli, A.; Micheli, M.; Miranda, S.; De Franciscis, P.; Insabato, L.; Sardo, A.D.S.; Zullo, F.; et al. Predictive Accuracy of Progesterone Receptor B in Young Women with Atypical Endometrial Hyperplasia and Early Endometrial Cancer Treated with Hysteroscopic Resection plus LNG-IUD Insertion. J. Minim. Invasive Gynecol. 2020. [Google Scholar] [CrossRef]
- Zakhour, M.; Cohen, J.G.; Gibson, A.; Walts, A.E.; Karimian, B.; Baltayan, A.; Aoyama, C.; Garcia, L.; Dhaliwal, S.K.; Elashoff, D.; et al. Abnormal mismatch repair and other clinicopathologic predictors of poor response to progestin treatment in young women with endometrial complex atypical hyperplasia and well-differentiated endometrial adenocarcinoma: A consecutive case series. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1576–1583. [Google Scholar] [CrossRef] [Green Version]
- Travaglino, A.; Raffone, A.; Saccone, G.; Insabato, L.; Mollo, A.; De Placido, G.; Zullo, F. Immunohistochemical predictive markers of response to conservative treatment of endometrial hyperplasia and early endometrial cancer: A systematic review. Acta Obstet. Gynecol. Scand. 2019, 98, 1086–1099. [Google Scholar] [CrossRef]
- Raffone, A.; Catena, U.; Travaglino, A.; Masciullo, V.; Spadola, S.; Della Corte, L.; Piermattei, A.; Insabato, L.; Zannoni, G.F.; Scambia, G.; et al. Mismatch repair-deficiency specifically predicts recurrence of atypical endometrial hyperplasia and early endometrial carcinoma after conservative treatment: A multi-center study. Gynecol. Oncol. 2021, 161, 795–801. [Google Scholar] [CrossRef]
- Levine, D.A.; The Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.F.; Karnezis, A.N.; et al. A clinically applicable molecular-based classification for endometrial cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef] [Green Version]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef] [Green Version]
- Kommoss, S.; McConechy, M.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; Grevenkamp, F.; Karnezis, A.; Yang, W.; Lum, A.; et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef] [PubMed]
- Britton, H.; Huang, L.; Lum, A.; Leung, S.; Shum, K.; Kale, M.; Burleigh, A.; Senz, J.; Yang, W.; McConechy, M.; et al. Molecular classification defines outcomes and opportunities in young women with endometrial carcinoma. Gynecol. Oncol. 2019, 153, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Falcone, F.; Normanno, N.; Losito, N.S.; Scognamiglio, G.; Abate, R.E.; Chicchinelli, N.; Casella, G.; Laurelli, G.; Scaffa, C.; Greggi, S. Application of the Proactive Molecular Risk Classifier for Endometrial Cancer (ProMisE) to patients conservatively treated: Outcomes from an institutional series. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Parkash, V.; Fadare, O.; Tornos, C.; McCluggage, W.G. Committee Opinion No. 631: Endometrial Intraepithelial Neoplasia. Obstet. Gynecol. 2015, 126, 897. [Google Scholar]
- Singh, N.; Piskorz, A.M.; Bosse, T.; Jimenez-Linan, M.; Rous, B.; Brenton, J.D.; Gilks, C.B.; Köbel, M. p53 immunohistochemistry is an accurate surrogate forTP53mutational analysis in endometrial carcinoma biopsies. J. Pathol. 2020, 250, 336–345. [Google Scholar] [CrossRef]
- Wong, J.W.R.; Strickland, K.C.; Previs, R. Prognostic Significance of Histologic Squamous Metaplasia and Immunohistochemical Staining Patterns of B-Catenin and p53 in Biopsy-Proven Endometrial Intraepithelial Neoplasia. International Gynecologic Cancer Society Annual Global Meeting, Virtual Meeting. 10–13 September 2020. [Google Scholar]
- Raffone, A.; Travaglino, A.; Cerbone, M.; De Luca, C.; Russo, D.; Di Maio, A.; De Marco, M.; Turco, M.C.; Insabato, L.; Zullo, F. Diagnostic accuracy of p53 immunohistochemistry as surrogate of TP53 sequencing in endometrial cancer. Pathol. Res. Pr. 2020, 216, 153025. [Google Scholar] [CrossRef]
- Rakha, E.; Wong, S.C.; Soomro, I.; Chaudry, Z.; Sharma, A.; Deen, S.; Chan, S.; Abu, J.; Nunns, D.; Williamson, K.; et al. Clinical outcome of atypical endometrial hyperplasia diagnosed on an endometrial biopsy: Institutional experience and review of literature. Am. J. Surg. Pathol. 2012, 36, 1683–1690. [Google Scholar] [CrossRef]
- Lacey, J.V., Jr.; Sherman, M.E.; Rush, B.B.; Ronnett, B.M.; Ioffe, O.B.; Duggan, M.A.; Glass, A.G.; Richesson, D.A.; Chatterjee, N.; Langholz, B. Absolute Risk of Endometrial Carcinoma During 20-Year Follow-Up Among Women with Endometrial Hyperplasia. J. Clin. Oncol. 2010, 28, 788–792. [Google Scholar] [CrossRef]
- Cosgrove, C.M.; Tritchler, D.L.; Cohn, D.E.; Mutch, D.G.; Rush, C.M.; Lankes, H.A.; Creasman, W.T.; Miller, D.S.; Ramirez, N.C.; Geller, M.A.; et al. An NRG Oncology/GOG study of molecular classification for risk prediction in endometrioid endometrial cancer. Gynecol. Oncol. 2018, 148, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Stelloo, E.; Nout, R.A.; Osse, E.M.; Juergenliemk-Schulz, I.J.; Jobsen, J.J.; Lutgens, L.C.; Van Der Steen-Banasik, E.M.; Nijman, H.W.; Putter, H.; Bosse, T.; et al. Improved Risk Assessment by Integrating Molecular and Clinicopathological Factors in Early-stage Endometrial Cancer—Combined Analysis of the PORTEC Cohorts. Clin. Cancer Res. 2016, 22, 4215–4224. [Google Scholar] [CrossRef] [Green Version]
- Raffone, A.; Travaglino, A.; Mascolo, M.; Carbone, L.; Guida, M.; Insabato, L.; Zullo, F. TCGA molecular groups of endometrial cancer: Pooled data about prognosis. Gynecol. Oncol. 2019, 155, 374–383. [Google Scholar] [CrossRef]
- Raffone, A.; Travaglino, A.; Gabrielli, O.; Micheli, M.; Zuccalà, V.; Bitonti, G.; Camastra, C.; Gargiulo, V.; Insabato, L.; Zullo, F. Clinical features of ProMisE groups identify different phenotypes of patients with endometrial cancer. Arch. Gynecol. Obstet. 2021, 303, 1393–1400. [Google Scholar] [CrossRef]
- Raffone, A.; Travaglino, A.; Mascolo, M.; Carotenuto, C.; Guida, M.; Mollo, A.; Insabato, L.; Zullo, F. Histopathological characterization of ProMisE molecular groups of endometrial cancer. Gynecol. Oncol. 2020, 157, 252–259. [Google Scholar] [CrossRef]
- Lynch, H.T.; Snyder, C.L.; Shaw, T.G.; Heinen, C.D.; Hitchins, M.P. Milestones of Lynch syndrome: 1895–2015. Nat. Rev. Cancer 2015, 15, 181–194. [Google Scholar] [CrossRef]
- Lancaster, J.M.; Powell, C.B.; Kauff, N.; Cass, I.; Chen, L.-M.; Lu, K.H.; Mutch, D.G.; Berchuck, A.; Karlan, B.Y.; Herzog, T.J. Society of Gynecologic Oncologists Education Committee Statement on Risk Assessment for Inherited Gynecologic Cancer Predispositions. Gynecol. Oncol. 2007, 107, 159–162. [Google Scholar] [CrossRef]
- Watson, P.; Lynch, H.T. Extracolonic cancer in hereditary nonpolyposis colorectal cancer. Cancer 1993, 71, 677–685. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Genetic/Familial High-Risk Assessment: Colorectal (Version 1.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf (accessed on 26 March 2020).
- SGO Clinical Practice Statement: Screening for Lynch Syndrome in Endometrial Cancer. Available online: https://www.sgo.org/resources/screening-for-lynch-syndrome-in-endometrial-cancer/ (accessed on 26 March 2020).
- Chen, M.; Jin, Y.; Li, Y.; Bi, Y.; Shan, Y.; Pan, L. Oncologic and reproductive outcomes after fertility-sparing management with oral progestin for women with complex endometrial hyperplasia and endometrial cancer. Int. J. Gynecol. Obstet. 2016, 132, 34–38. [Google Scholar] [CrossRef]
- Yang, Y.-F.; Liao, Y.-Y.; Liu, X.-L.; Su, S.-G.; Li, L.-Z.; Peng, N.-F. Prognostic factors of regression and relapse of complex atypical hyperplasia and well-differentiated endometrioid carcinoma with conservative treatment. Gynecol. Oncol. 2015, 139, 419–423. [Google Scholar] [CrossRef]
- Zhou, R.; Yang, Y.; Lu, Q.; Wang, J.; Miao, Y.; Wang, S.; Wang, Z.; Zhao, C.; Wei, L. Prognostic factors of oncological and reproductive outcomes in fertility-sparing treatment of complex atypical hyperplasia and low-grade endometrial cancer using oral progestin in Chinese patients. Gynecol. Oncol. 2015, 139, 424–428. [Google Scholar] [CrossRef]
- Gonthier, C.; Walker, F.; Luton, D.; Yazbeck, C.; Madelenat, P.; Koskas, M. Impact of obesity on the results of fertility-sparing management for atypical hyperplasia and grade 1 endometrial cancer. Gynecol. Oncol. 2014, 133, 33–37. [Google Scholar] [CrossRef]
- Chung, Y.S.; Woo, H.Y.; Lee, J.-Y.; Park, E.; Nam, E.J.; Kim, S.; Kim, S.W.; Kim, Y.T. Mismatch repair status influences response to fertility-sparing treatment of endometrial cancer. Am. J. Obstet. Gynecol. 2021, 224, 370.e1–370.e13. [Google Scholar] [CrossRef] [PubMed]
- Talhouk, A.; Hoang, L.N.; McConechy, M.K.; Nakonechny, Q.; Leo, J.; Cheng, A.; Leung, S.; Yang, W.; Lum, A.; Köbel, M.; et al. Molecular classification of endometrial carcinoma on diagnostic specimens is highly concordant with final hysterectomy: Earlier prognostic information to guide treatment. Gynecol. Oncol. 2016, 143, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trimble, C.L.; Kauderer, J.; Zaino, R.; Silverberg, S.; Lim, P.C.; Burke, J.J., 2nd; Alberts, D.; Curtin, J. Concurrent endometrial carcinoma in women with a biopsy diagnosis of atypical endometrial hyperplasia: A Gynecologic Oncology Group study. Cancer 2006, 106, 812–819. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Molecular Classification | ||||
|---|---|---|---|---|---|
| MMRd (n = 6) | POLE Mutated (n = 4) | p53 Abnormal (n = 4) | p53 Wild Type (n = 44) | Total (n = 58) | |
| Age at Diagnosis (years) | |||||
| Median (range) | 71.7 (51.9–86.8) | 55.5 (52.1–68.3) | 67.0 (48.1–89.0) | 53.1 (24.3–91.1) | 56.4 (24.3–91.1) |
| Diagnosis | |||||
| Endometrioid cancer | 4 (66.7) | 0 (0) | 1 (25.0) | 17 (38.6) | 22 (37.9) |
| Endometrial intraepithelial neoplasia | 2 (33.3) | 4 (100.0) | 3 (75.0) | 27 (61.4) | 36 (62.1) |
| Race, n (%) | |||||
| White | 4 (66.7) | 1 (25.0) | 2 (50.0) | 25 (56.8) | 32 (55.2) |
| Black | 1 (16.7) | 3 (75.0) | 2 (50.0) | 17 (38.6) | 23 (39.7) |
| Asian | 1 (16.7) | 0 (0) | 0 (0) | 0 (0) | 1 (1.7) |
| Other | 0 (0) | 0 (0) | 0 (0) | 2 (4.6) | 2 (3.5) |
| Ethnicity, n (%) | |||||
| Hispanic or Latino | 0 (0) | 0 (0) | 0 (0) | 4 (9.1) | 4 (6.9) |
| Not Hispanic or Latino | 6 (100.0) | 4 (100.0) | 4 (100.0) | 40 (90.9) | 54 (93.1) |
| Parity | |||||
| Median | 1.5 | 0.5 | 2.5 | 0.0 | 1.0 |
| BMI, kilograms/meter2 | |||||
| Median (range) | 43.0 (21.6–50.3) | 46.7 (35.5–53.3) | 37.5 (22.1–54.1) | 47.2 (19.9–74.4) | 46.4 (19.9–74.4) |
| ECOG Performance Score, n (%) | |||||
| 0–1 | 6 (100.0) | 2 (50.0) | 4 (100.0) | 27 (61.4) | 39 (67.2) |
| 2 | 0 (0) | 0 (0) | 0 (0) | 4 (9.1) | 4 (6.9) |
| 3 | 0 (0) | 0 (0) | 0 (0) | 2 (4.6) | 2 (3.5) |
| Unknown | 0 (0) | 2 (50.0) | 0 (0) | 11 (25.0) | 13 (22.4) |
| History of Other Cancer, n (%) | |||||
| No | 5 (83.3) | 3 (75.0) | 3 (75.0) | 38 (86.4) | 49 (84.5) |
| Yes | 1 (16.7) | 1 (25.0) | 1 (25.0) | 6 (13.6) | 9 (15.5) |
| Initial specimen obtained through, n (%) | |||||
| EMB | 1 (16.7) | 3 (75.0) | 2 (50.0) | 23 (52.3) | 29 (50.0) |
| D&C | 5 (83.3) | 1 (25.0) | 2 (50.0) | 21 (47.7) | 29 (50.0) |
| Hormonal therapy prior to LNG-IUS insertion, n (%) | |||||
| No | 6 (100.0) | 3 (75.0) | 4 (100.0) | 32 (72.7) | 45 (77.6) |
| Yes | 0 (0) | 1 (25.0) | 0 (0) | 12 (27.3) | 13 (22.4) |
| Imaging prior to LNG-IUSinsertion, n (%) | |||||
| No | 0 (0) | 0 (0) | 0 (0) | 15 (34.1) | 15 (25.9) |
| Yes | 6 (100.0) | 4 (100.0) | 4 (100.0) | 29 (65.9) | 43 (74.1) |
| Medical co-morbidities precluding surgery | 4 (66.7) | 4 (100.0) | 3 (75.0) | 22 (50.0) | 33 (56.9) |
| Placed at time of D&C | 0 (0) | 0 (0) | 0 (0) | 3 (6.8) | 3 (5.2) |
| Patient preference | 1 (16.7) | 0 (0) | 1 (25.0) | 6 (13.6) | 8 (13.8) |
| Case | Initial Biopsy Histology | Codon Change | Amino Acid Change | Mutation Events | Total Events | Mutation Event Percent |
|---|---|---|---|---|---|---|
| 49 | EIN | 857C > G | Pro286Arg | 8 | 120 | 6.7 |
| 50 | EIN | 857C > G | Pro286Arg | 37 | 159 | 23.3 |
| 51 | EIN | 1231G > T | Val411Leu | 12 | 132 | 9.1 |
| 52 | EIN | 857C > G | Pro286Arg | 3 | 54 | 5.6 |
| Case | Initial Biopsy Histology | Nucleotide Mutation | Amino Acid Mutation | Mutation Type |
|---|---|---|---|---|
| 45 | EIN | c.877G > A | p.Gly293Arg | Amino acid substitution |
| 46 | EIN | c.517G > A p.210T > C c.693C > T | p.Val173Met p.Ala70= p.Thr231= | Amino acid substitution Silent mutation Silent mutation |
| 47 | EIN | c.651G > A | p.Val217= | Silent mutation |
| 48 | Grade 1 EC | c.548C > T c.817C > T | p.Ser183Leu p.Arg273Cys | Amino acid substitution Amino acid substitution |
| MMRd (n = 4) | POLE- Mutated (n = 0) | p53 Abnormal (n = 1) | p53 Wild Type (n = 17) | Total (n = 22) | |
|---|---|---|---|---|---|
| Progression or requireddefinitive treatment, n (%) | |||||
| No | 3 (75.0) | - | 0 (0) | 13 (76.5) | 16 (72.7) |
| Yes | 1 (25.0) | - | 1 (100.0) | 4 (23.5) | 6 (27.3) |
| Type of definitive therapy n (%) | n = 1 | n = 1 | n = 4 | n = 6 | |
| Surgery | 1 (100.0) | - | 1 (100.0) | 4 (100.0) | 6 (100.0) |
| Radiation | 0 (0) | - | 0 (0) | 0 (0) | 0 (0.0) |
| Final diagnosis on hysterectomy specimen n (%) | n = 1 | n = 1 | n = 4 | n = 6 | |
| No residual disease | 0 (0.0) | - | 0 (0.0) | 1 (25.0) | 1 (16.7) |
| EIN | 0 (0.0) | - | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Cancer | 1 (100.0) | - | 1 (100.0) | 3 (75.0) | 5 (83.33) |
| Title | MMRd (n = 2) | POLE- Mutated (n = 4) | p53- Abnormal (n = 3) | p53 Wild Type (n = 27) | Total (n = 36) |
|---|---|---|---|---|---|
| Progression or required definitive treatmentn (%) | |||||
| No | 1 (50.0) | 3 (75.0) | 2 (66.7) | 25 (92.6) | 31 (86.1) |
| Yes | 1 (50.0) | 1 (25.0) | 1 (33.3) | 2 (7.4) | 5 (13.9) |
| Type of definitive therapy, n (%) | n = 1 | n = 1 | n = 1 | n = 2 | n = 5 |
| Surgery | 1 (100.0) | 0 (0) | 1 (100.0) | 2 (100.0) | 4 (80.0) |
| Radiation | 0 (0.0) | 1 (25.0) | 0 (0.0) | 0 (0.0) | 1 (20.0) |
| Final diagnosis on hysterectomy specimen, n (%) | n = 1 | n = 0 | n = 1 | n = 2 | n = 4 |
| No residual disease | 0 (0.0) | - | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| EIN | 0 (0.0) | - | 1 (100.0) | 0 (0.0) | 1 (25.0) |
| Cancer | 1 (100.0) | - | 0 (0.0) | 2 (100.0) | 3 (75.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puechl, A.M.; Spinosa, D.; Berchuck, A.; Secord, A.A.; Drury, K.E.; Broadwater, G.; Wong, J.; Whitaker, R.; Devos, N.; Corcoran, D.L.; et al. Molecular Classification to Prognosticate Response in Medically Managed Endometrial Cancers and Endometrial Intraepithelial Neoplasia. Cancers 2021, 13, 2847. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13112847
Puechl AM, Spinosa D, Berchuck A, Secord AA, Drury KE, Broadwater G, Wong J, Whitaker R, Devos N, Corcoran DL, et al. Molecular Classification to Prognosticate Response in Medically Managed Endometrial Cancers and Endometrial Intraepithelial Neoplasia. Cancers. 2021; 13(11):2847. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13112847
Chicago/Turabian StylePuechl, Allison M., Daniel Spinosa, Andrew Berchuck, Angeles Alvarez Secord, Kerry E. Drury, Gloria Broadwater, Janice Wong, Regina Whitaker, Nicolas Devos, David L. Corcoran, and et al. 2021. "Molecular Classification to Prognosticate Response in Medically Managed Endometrial Cancers and Endometrial Intraepithelial Neoplasia" Cancers 13, no. 11: 2847. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13112847