
Pre-Therapeutic Measurements of Iodine Avidity in Papillary and Poorly Differentiated Thyroid Cancer Reveal Associations with Thyroglobulin Expression, Histological Variants and Ki-67 Index

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Conduct and Patient Inclusion
2.2. Patient Specimen Collection and Measurements
2.3. Histopathology Work-Up
2.4. Data Processing
2.5. Statistical Analysis
3. Results
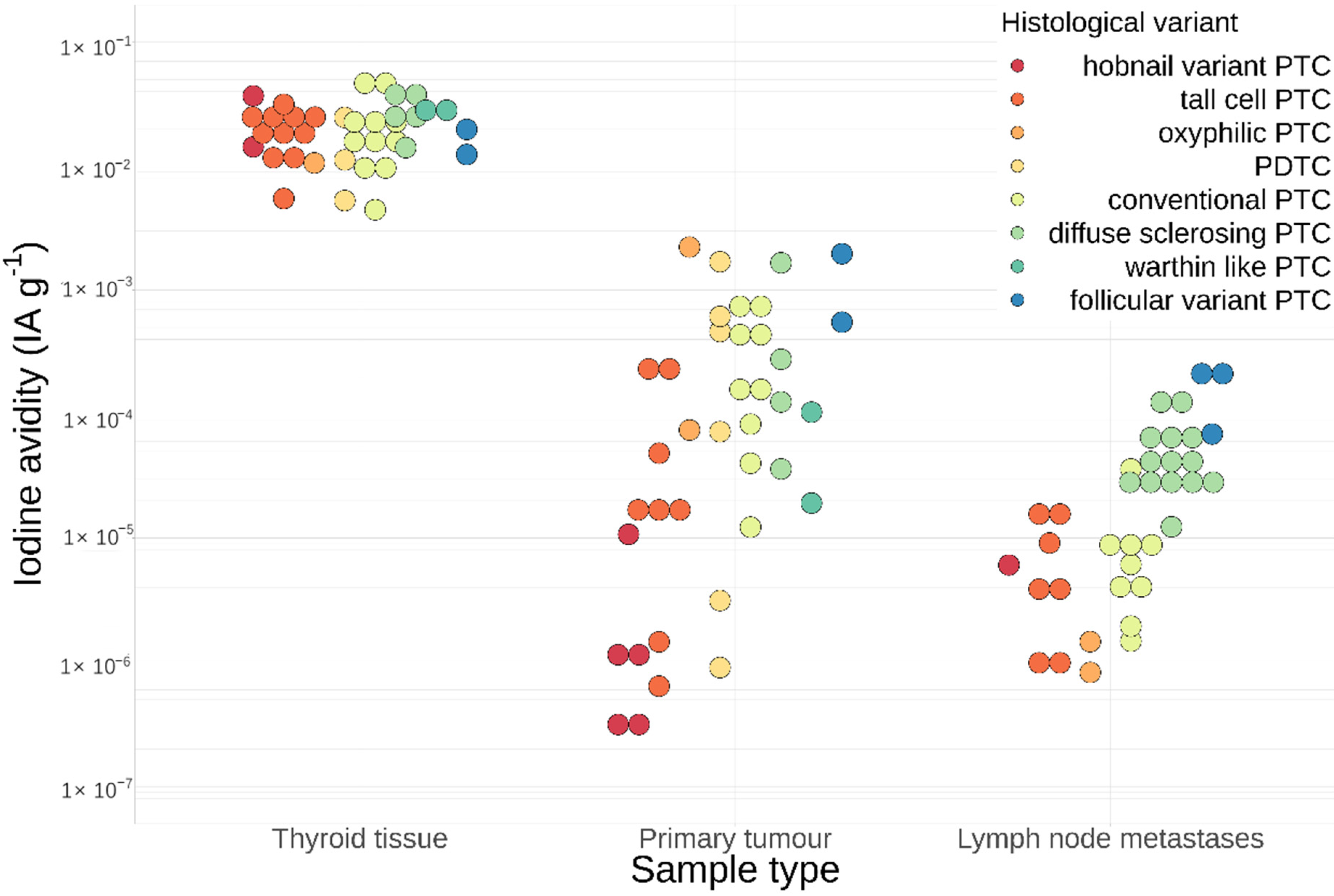
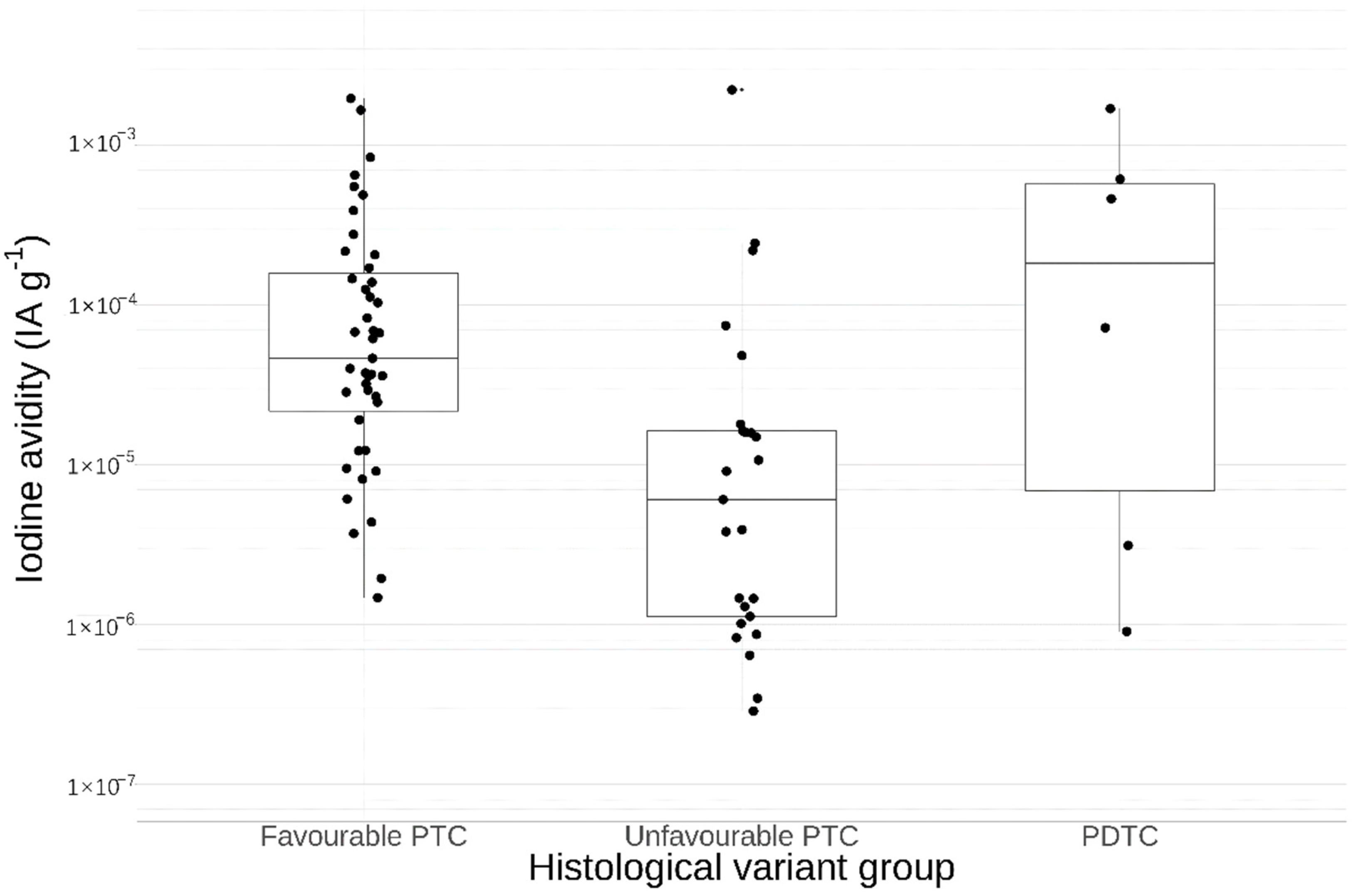
3.1. Histological Variants
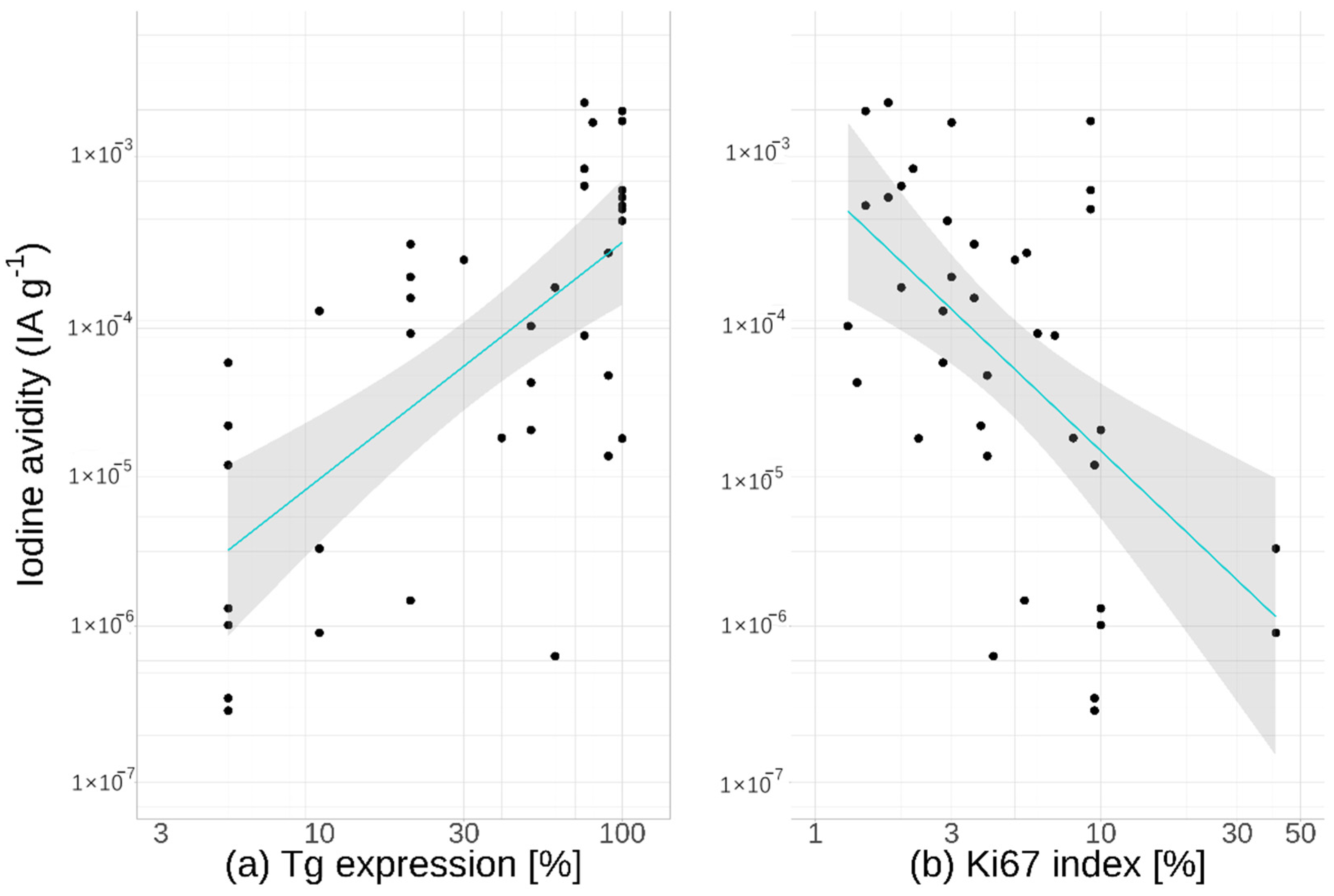
3.2. Thyroglobulin Expression
3.3. Ki-67 Index
3.4. Age
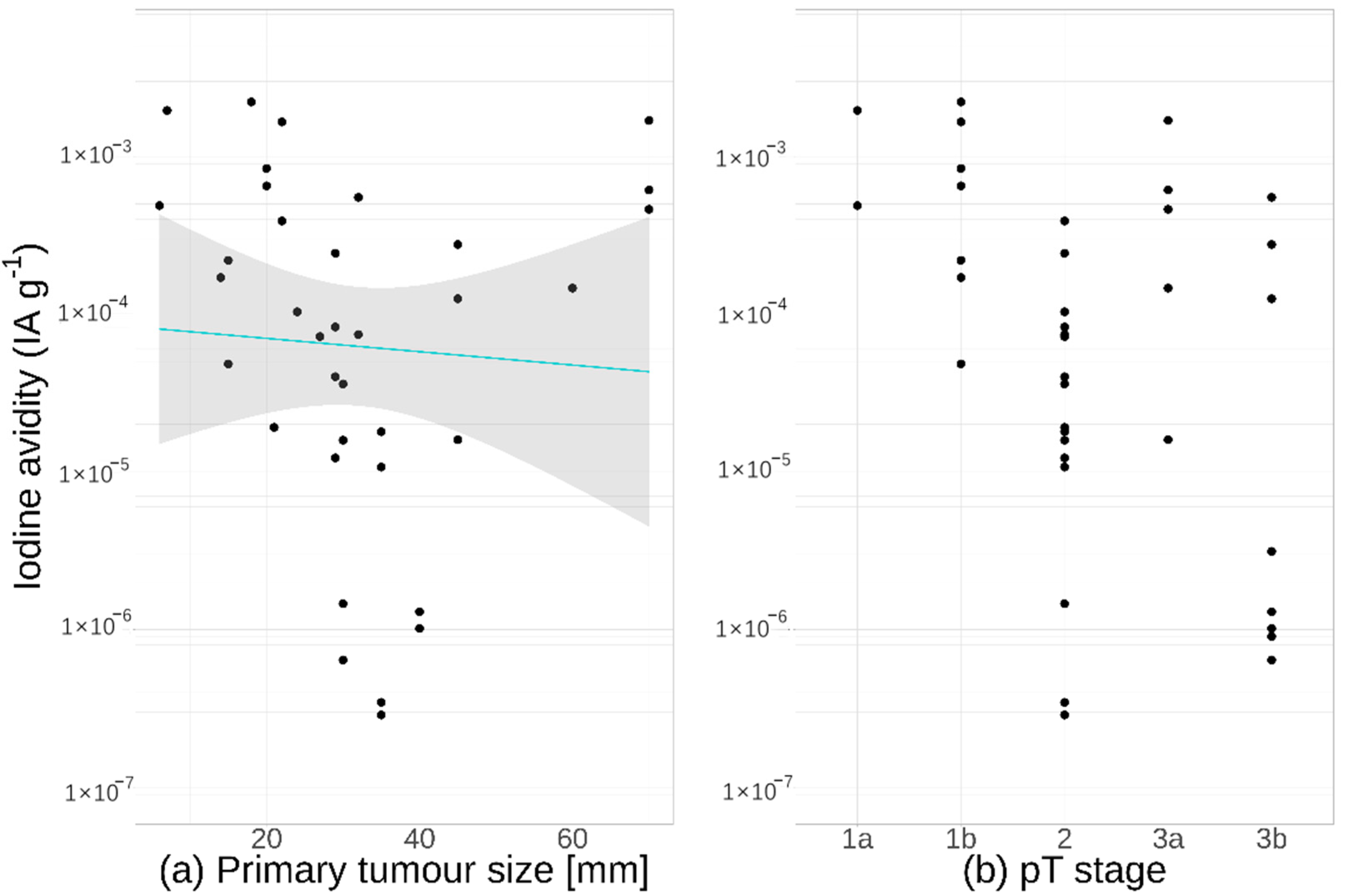
3.5. Tumour Size
3.6. Blood Iodine Kinetics
3.7. Thyroid Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mayson, S.E.; Yoo, D.C.; Gopalakrishnan, G. The Evolving Use of Radioiodine Therapy in Differentiated Thyroid Cancer. Oncology 2015, 88, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Zhong, L.; Yi, H. A Review on the Mechanism of Iodide Metabolic Dysfunction in Differentiated Thyroid Cancer. Mol. Cell. Endocrinol. 2019, 479, 71–77. [Google Scholar] [CrossRef]
- Lin, J.-D. Thyroglobulin and Human Thyroid Cancer. Clin. Chim. Acta 2008, 388, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.R.; Bergert, E.R.; Goellner, J.R.; Hay, I.D.; Morris, J.C. Immunohistochemical Analysis of Sodium Iodide Symporter Expression in Metastatic Differentiated Thyroid Cancer: Correlation with Radioiodine Uptake. J. Clin. Endocrinol. Metab. 2001, 86, 5627–5632. [Google Scholar] [CrossRef]
- Fragu, P.; Nataf, B.M. Human Thyroid Peroxidase Activity in Benign and Malign Thyroid Disorders. J. Clin. Endocrinol. Metab. 1977, 45, 1089–1096. [Google Scholar] [CrossRef]
- Sabra, M.M.; Dominguez, J.M.; Grewal, R.K.; Larson, S.M.; Ghossein, R.A.; Tuttle, R.M.; Fagin, J.A. Clinical Outcomes and Molecular Profile of Differentiated Thyroid Cancers With Radioiodine-Avid Distant Metastases. J. Clin. Endocrinol. Metab. 2013, 98, E829–E836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; De Vathaire, F.; et al. Long-Term Outcome of 444 Patients with Distant Metastases from Papillary and Follicular Thyroid Carcinoma: Benefits and Limits of Radioiodine Therapy. J. Clin. Endocrinol. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Challeton, C.; De Vathaire, F.; Travagli, J.P.; Gardet, P.; Lumbroso, J.D.; Francese, C.; Fontaine, F.; Ricard, M.; Parmentier, C. Radioactive Iodine Treatment and External Radiotherapy for Lung and Bone Metastases from Thyroid Carcinoma. J. Nucl. Med. 1996, 37, 598–605. [Google Scholar] [PubMed]
- Bernier, M.O.; Leenhardt, L.; Hoang, C.; Aurengo, A.; Mary, J.Y.; Menegaux, F.; Enkaoua, E.; Turpin, G.; Chiras, J.; Saillant, G.; et al. Survival and Therapeutic Modalities in Patients with Bone Metastases of Differentiated Thyroid Carcinomas. J. Clin. Endocrinol. Metab. 2001, 86, 1568–1573. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, J.I.; Kim, N.K.; Min, Y.-K.; Kim, S.W.; Chung, J.H. Prognostic Implications of Radioiodine Avidity and Serum Thyroglobulin in Differentiated Thyroid Carcinoma with Distant Metastasis. World J. Surg. 2013, 37, 2845–2852. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-H.; Jung, J.; Son, S.H.; Kim, C.-Y.; Hong, C.M.; Jeong, S.Y.; Lee, S.-W.; Lee, J.; Ahn, B.-C. Difference of Clinical and Radiological Characteristics According to Radioiodine Avidity in Pulmonary Metastases of Differentiated Thyroid Cancer. Nucl. Med. Mol Imaging 2014, 48, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marotta, V.; Sciammarella, C.; Colao, A.; Faggiano, A. Application of Molecular Biology of Differentiated Thyroid Cancer for Clinical Prognostication. Endocr. Relat. Cancer 2016, 23, R499–R515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perros, P.; Boelaert, K.; Colley, S.; Evans, C.; Evans, R.M.; Gerrard BA, G.; Gilbert, J.; Harrison, B.; Johnson, S.J.; Giles, T.E.; et al. Guidelines for the Management of Thyroid Cancer. Clin. Endocrinol. 2014, 81, 1–122. [Google Scholar] [CrossRef] [PubMed]
- Hennings, J.; Asp, P.; Dahlberg, J.; Grimm, O. Sköldkörtelcancer, Nationellt Vårdprogram 2019. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/skoldkortelcancer/ (accessed on 19 July 2021).
- Blue, P.W.; Brownt, P.H.; Manier, S.M.; Ghaed, N. Calculation of Minimal Detectable Activity for Scintillation Detection Systems. J. Nucl. Med. Technol. 1987, 15, 4. [Google Scholar]
- Lloyd, R.; Osamura, R.; Klöppel, G.; Rosai, J. WHO Classification of Tumours of Endocrine Organs, World Health Organization Classification of Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017; ISBN 978-92-832-4493-6. [Google Scholar]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge from a Population-Based to a More “Personalized” Approach to Cancer Staging: The Eighth Edition AJCC Cancer Staging Manual. CA A Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Ho, A.S.; Luu, M.; Barrios, L.; Chen, I.; Melany, M.; Ali, N.; Patio, C.; Chen, Y.; Bose, S.; Fan, X.; et al. Incidence and Mortality Risk Spectrum Across Aggressive Variants of Papillary Thyroid Carcinoma. JAMA Oncol. 2020, 6, 706. [Google Scholar] [CrossRef]
- Nakanishi, K.; Kikumori, T.; Miyajima, N.; Takano, Y.; Noda, S.; Takeuchi, D.; Iwano, S.; Kodera, Y. Impact of Patient Age and Histological Type on Radioactive Iodine Avidity of Recurrent Lesions of Differentiated Thyroid Carcinoma. Clin. Nucl. Med. 2018, 43, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.; Ghossein, R.A.; Schoder, H.; Gomez, D.; Larson, S.M.; Tuttle, R.M. Histopathologic Characterization of Radioactive Iodine-refractory Fluorodeoxyglucose-positron Emission Tomography-positive Thyroid Carcinoma. Cancer 2008, 113, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Ambrosi, F.; Righi, A.; Ricci, C.; Erickson, L.A.; Lloyd, R.V.; Asioli, S. Hobnail Variant of Papillary Thyroid Carcinoma: A Literature Review. Endocr. Pathol. 2017, 28, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Nath, M.C.; Erickson, L.A. Aggressive Variants of Papillary Thyroid Carcinoma: Hobnail, Tall Cell, Columnar, and Solid. Adv. Anat. Pathol. 2018, 25, 8. [Google Scholar] [CrossRef]
- Mihailovic, J.; Stefanovic, L.; Malesevic, M.; Markoski, B. The Importance of Age over Radioiodine Avidity as a Prognostic Factor in Differentiated Thyroid Carcinoma with Distant Metastases. Thyroid 2009, 19, 227–232. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, C.J.; Bullock, M.; Chou, A.; Sidhu, S.B.; Delbridge, L.W.; Robinson, B.G.; Gill, A.J.; Learoyd, D.L.; Clifton-Bligh, R.; Sywak, M.S. BRAF(V600E) Mutation Is Associated with an Increased Risk of Nodal Recurrence Requiring Reoperative Surgery in Patients with Papillary Thyroid Cancer. Surgery 2010, 148, 1139–1145; discussion 1145–1146. [Google Scholar] [CrossRef]
- Ho, A.L.; Grewal, R.K.; Leboeuf, R.; Sherman, E.J.; Pfister, D.G.; Deandreis, D.; Pentlow, K.S.; Zanzonico, P.B.; Haque, S.; Gavane, S.; et al. Selumetinib-Enhanced Radioiodine Uptake in Advanced Thyroid Cancer. N. Engl. J. Med. 2013, 368, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, L.A.; Sherman, E.J.; Baxi, S.S.; Tchekmedyian, V.; Grewal, R.K.; Larson, S.M.; Pentlow, K.S.; Haque, S.; Tuttle, R.M.; Sabra, M.M.; et al. Vemurafenib Redifferentiation of BRAF Mutant, RAI-Refractory Thyroid Cancers. J. Clin. Endocrinol. Metab. 2019, 104, 1417–1428. [Google Scholar] [CrossRef] [PubMed]
- Iravani, A.; Solomon, B.; Pattison, D.A.; Jackson, P.; Ravi Kumar, A.; Kong, G.; Hofman, M.S.; Akhurst, T.; Hicks, R.J. Mitogen-Activated Protein Kinase Pathway Inhibition for Redifferentiation of Radioiodine Refractory Differentiated Thyroid Cancer: An Evolving Protocol. Thyroid 2019, 29, 1634–1645. [Google Scholar] [CrossRef]
- Burt, A.; Goudie, R.B. Diagnosis of Primary Thyroid Carcinoma by Immunohistological Demonstration of Thyroglobulin. Histopathology 1979, 3, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Ryff-de Lèche, A.; Staub, J.J.; Kohler-Faden, R.; Müller-Brand, J.; Heitz, P.U. Thyroglobulin Production by Malignant Thyroid Tumors. An Immunocytochemical and Radioimmunoassay Study. Cancer 1986, 57, 1145–1153. [Google Scholar] [CrossRef]
- Dralle, H.; Schwarzrock, R.; Lang, W.; Böcker, W.; Ziegler, H.; Schröder, S.; Geerlings, H. Comparison of Histology and Immunohistochemistry with Thyroglobulin Serum Levels and Radioiodine Uptake in Recurrences and Metastases of Differentiated Thyroid Carcinomas. Acta Endocrinol. 1985, 108, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Ringel, M.D.; Anderson, J.; Souza, S.L.; Burch, H.B.; Tambascia, M.; Shriver, C.D.; Tuttle, R.M. Expression of the Sodium Iodide Symporter and Thyroglobulin Genes Are Reduced in Papillary Thyroid Cancer. Mod. Pathol. 2001, 14, 289–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walczyk, A.; Kopczyński, J.; Gąsior-Perczak, D.; Pałyga, I.; Kowalik, A.; Chrapek, M.; Hejnold, M.; Góźdź, S.; Kowalska, A. Histopathology and Immunohistochemistry as Prognostic Factors for Poorly Differentiated Thyroid Cancer in a Series of Polish Patients. PLoS ONE 2020, 15, e0229264. [Google Scholar] [CrossRef]
- Kakudo, K.; Liu, Z.; Bai, Y.; Li, Y.; Kitayama, N.; Satoh, S.; Nakashima, M.; Jung, C.K. How to Identify Indolent Thyroid Tumors Unlikely to Recur and Cause Cancer Death Immediately after Surgery-Risk Stratification of Papillary Thyroid Carcinoma in Young Patients. Endocr. J. 2021. [Google Scholar] [CrossRef]
- Van Nostrand, D. Prescribed Activity of 131I Therapy in Differentiated Thyroid Cancer. J. Nucl. Med. 2017, 58, 697–699. [Google Scholar] [CrossRef] [Green Version]
- Deandreis, D.; Rubino, C.; Tala, H.; Leboulleux, S.; Terroir, M.; Baudin, E.; Larson, S.; Fagin, J.A.; Schlumberger, M.; Tuttle, R.M. Comparison of Empiric Versus Whole-Body/-Blood Clearance Dosimetry–Based Approach to Radioactive Iodine Treatment in Patients with Metastases from Differentiated Thyroid Cancer. J. Nucl. Med. 2017, 58, 717–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjögreen Gleisner, K.; Spezi, E.; Solny, P.; Gabina, P.M.; Cicone, F.; Stokke, C.; Chiesa, C.; Paphiti, M.; Brans, B.; Sandström, M.; et al. Variations in the Practice of Molecular Radiotherapy and Implementation of Dosimetry: Results from a European Survey. EJNMMI Phys. 2017, 4, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clement, S.C.; Peeters, R.P.; Ronckers, C.M.; Links, T.P.; van den Heuvel-Eibrink, M.M.; Nieveen van Dijkum, E.J.M.; van Rijn, R.R.; van der Pal, H.J.H.; Neggers, S.J.; Kremer, L.C.M.; et al. Intermediate and Long-Term Adverse Effects of Radioiodine Therapy for Differentiated Thyroid Carcinoma—A Systematic Review. Cancer Treat. Rev. 2015, 41, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Hayes, S.; Kermode, J.C.; Thompson, B.D. Measurement of Serum TSH and Thyroid Hormones in the Management of Treatment of Thyroid Carcinoma with Radioiodine. Br. J. Radiol. 1977, 50, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Masoodi, T.; Siraj, A.K.; Siraj, S.; Azam, S.; Qadri, Z.; Albalawy, W.N.; Parvathareddy, S.K.; Al-Sobhi, S.S.; Al-Dayel, F.; Alkuraya, F.S.; et al. Whole-Exome Sequencing of Matched Primary and Metastatic Papillary Thyroid Cancer. Thyroid 2020, 30, 42–56. [Google Scholar] [CrossRef] [PubMed]
- Siraj, A.K.; Masoodi, T.; Bu, R.; Beg, S.; Al-Sobhi, S.S.; Al-Dayel, F.; Al-Dawish, M.; Alkuraya, F.S.; Al-Kuraya, K.S. Genomic Profiling of Thyroid Cancer Reveals a Role for Thyroglobulin in Metastasis. Am. J. Hum. Genet. 2016, 98, 1170–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, K.; Wang, H.; Liang, Z.; Lin, Y. BRAFV600E Mutation Associated with Non-Radioiodine-Avid Status in Distant Metastatic Papillary Thyroid Carcinoma. Clin. Nucl. Med. 2014, 39, 5. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, R.; Shen, X.; Zhu, G.; Li, B.; Xing, M. The Genetic Duet of BRAF V600E and TERT Promoter Mutations Robustly Predicts Loss of Radioiodine Avidity in Recurrent Papillary Thyroid Cancer. J. Nucl. Med. 2020, 61, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Li, J.; Li, X.; Liang, Z.; Gao, W.; Liang, J.; Cheng, S.; Lin, Y. TERT Promoter Mutation Predicts Radioiodine-Refractory Character in Distant Metastatic Differentiated Thyroid Cancer. J. Nucl. Med. 2017, 58, 258–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Gong, Y.; Yan, S.; Chen, H.; Qin, S.; Gong, R. Association between TERT Promoter Mutations and Clinical Behaviors in Differentiated Thyroid Carcinoma: A Systematic Review and Meta-Analysis. Endocrine 2020, 67, 44–57. [Google Scholar] [CrossRef] [Green Version]
- Hysek, M.; Paulsson, J.O.; Jatta, K.; Shabo, I.; Stenman, A.; Höög, A.; Larsson, C.; Zedenius, J.; Juhlin, C.C. Clinical Routine TERT Promoter Mutational Screening of Follicular Thyroid Tumors of Uncertain Malignant Potential (FT-UMPs): A Useful Predictor of Metastatic Disease. Cancers 2019, 11, 1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 35) |
|---|---|
| Age | |
| Median (range) | 53 (19, 81) |
| Sex | |
| Male | 14 (40%) |
| Female | 21 (60%) |
| Time from injection to surgery (h) | |
| Median (range) | 48 (44, 54) |
| BMI (kg/m2) | |
| Median (range) | 26 (19, 34) |
| eGFR (ml/min/m2) | |
| Median (range) | 80 (57, 90) |
| Serum TSH level (mU/l) | |
| High (>4.0) | 1 (3%) |
| Normal (0.4–4.0) | 32 (91%) |
| Low (<0.4) | 2 (6%) |
| Parameter | Primary Tumour (n = 38) | Lymph Node Metastasis (n = 36) | Total (n = 74) |
|---|---|---|---|
| Histological type | |||
| Conventional PTC | 9 (24%) | 9 (25%) | 18 (24%) |
| Diffuse sclerosing PTC | 4 (11%) | 14 (39%) | 18 (24%) |
| Warthin-like PTC | 2 (5%) | 0 (0%) | 2 (3%) |
| Follicular variant PTC | 2 (5%) | 3 (8%) | 5 (7%) |
| Oxyphilic PTC | 2 (5%) | 2 (6%) | 4 (5%) |
| Hobnail variant PTC | 5 (13%) | 1 (3%) | 6 (8%) |
| Tall cell variant PTC | 8 (21%) | 7 (19%) | 15 (20%) |
| PDTC | 6 (16%) | 0 (0%) | 6 (8%) |
| Thyroglobulin expression (%) * | |||
| Median (range) | 50 (5, 100) | 60 (5, 100) | 50 (5, 100) |
| Ki-67 index (%) * | |||
| Median (range) | 4.0 (1.3, 41) | 3.5 (1.0, 14) | 4.0 (1.0, 41) |
| Extrathyroidal/nodal extension | |||
| Yes/No | 10/28 (26%/74%) | 10/26 (28%/76%) | 20/54 (27%/73%) |
| Negative surgical margins ** | |||
| Yes/No | 29/9 (76/24%) | 36/0 (100/0%) | 65/9 (88/12%) |
| Iodine avidity (log10 of IA g−1) | |||
| Median (range) | −4.1 (−6.5 −2.7) | −4.8 (−6.1 −3.7) | −4.5 (−6.5 −2.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nilsson, J.N.; Siikanen, J.; Hedman, C.; Juhlin, C.C.; Ihre Lundgren, C. Pre-Therapeutic Measurements of Iodine Avidity in Papillary and Poorly Differentiated Thyroid Cancer Reveal Associations with Thyroglobulin Expression, Histological Variants and Ki-67 Index. Cancers 2021, 13, 3627. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143627
Nilsson JN, Siikanen J, Hedman C, Juhlin CC, Ihre Lundgren C. Pre-Therapeutic Measurements of Iodine Avidity in Papillary and Poorly Differentiated Thyroid Cancer Reveal Associations with Thyroglobulin Expression, Histological Variants and Ki-67 Index. Cancers. 2021; 13(14):3627. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143627
Chicago/Turabian StyleNilsson, Joachim N., Jonathan Siikanen, Christel Hedman, C. Christofer Juhlin, and Catharina Ihre Lundgren. 2021. "Pre-Therapeutic Measurements of Iodine Avidity in Papillary and Poorly Differentiated Thyroid Cancer Reveal Associations with Thyroglobulin Expression, Histological Variants and Ki-67 Index" Cancers 13, no. 14: 3627. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143627