
Radiation-Induced Dyspnea in Lung Cancer Patients Treated with Stereotactic Body Radiation Therapy

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Subsection
2.2. Dosimetric and Statistical Analysis
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cella, L.; Liuzzi, R.; D’Avino, V.; Conson, M.; Di Biase, A.; Picardi, M.; Pugliese, N.; Solla, R.; Salvatore, M.; Pacelli, R. Pulmonary damage in Hodgkin’s lymphoma patients treated with sequential chemo-radiotherapy: Predictors of radiation-induced lung injury. Acta Oncol. 2014, 53, 613–619. [Google Scholar] [CrossRef] [Green Version]
- Cella, L.; D’Avino, V.; Palma, G.; Conson, M.; Liuzzi, R.; Picardi, M.; Pressello, M.C.; Boboc, G.I.; Battistini, R.; Donato, V.; et al. Modeling the risk of radiation-induced lung fibrosis: Irradiated heart tissue is as important as irradiated lung. Radiother. Oncol. 2015, 117, 36–43. [Google Scholar] [CrossRef]
- Defraene, G.; Schuit, E.; De Ruysscher, D. Development and internal validation of a multinomial NTCP model for the severity of acute dyspnea after radiotherapy for lung cancer. Radiother. Oncol. 2019, 136, 176–184. [Google Scholar] [CrossRef]
- Pacelli, R.; Caroprese, M.; Palma, G.; Oliviero, C.; Clemente, S.; Cella, L.; Conson, M. Technological evolution of radiation treatment: Implications for clinical applications. Semin. Oncol. 2019, 46, 193–201. [Google Scholar] [CrossRef]
- Andruska, N.; Stowe, H.B.; Crockett, C.; Liu, W.; Palma, D.; Faivre-Finn, C.; Badiyan, S.N. Stereotactic radiation for lung cancer: A practical approach to challenging scenarios. J. Thorac. Oncol. 2021, 16, 1075–1085. [Google Scholar] [CrossRef]
- Chen, H.; Louie, A.V.; Boldt, R.G.; Rodrigues, G.B.; Palma, D.A.; Senan, S. Quality of life after stereotactic ablative radiotherapy for early-stage lung cancer: A systematic review. Clin. Lung Cancer 2016, 17, e141–e149. [Google Scholar] [CrossRef]
- D’Andrea, M.; Strolin, S.; Ungania, S.; Cacciatore, A.; Bruzzaniti, V.; Marconi, R.; Benassi, M.; Strigari, L. Radiobiological optimization in lung stereotactic body radiation therapy: Are we ready to apply radiobiological models? Front. Oncol. 2017, 7, 321. [Google Scholar] [CrossRef] [Green Version]
- Barriger, R.B.; Forquer, J.A.; Brabham, J.G.; Andolino, D.L.; Shapiro, R.H.; Henderson, M.A.; Johnstone, P.A.; Fakiris, A.J. A dose-volume analysis of radiation pneumonitis in non-small cell lung cancer patients treated with stereotactic body radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 457–462. [Google Scholar] [CrossRef]
- Guckenberger, M.; Klement, R.J.; Kestin, L.L.; Hope, A.J.; Belderbos, J.; Werner-Wasik, M.; Yan, D.; Sonke, J.J.; Bissonnette, J.P.; Xiao, Y.; et al. Lack of a dose-effect relationship for pulmonary function changes after stereotactic body radiation therapy for early-stage non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Li, Q.Q.; Xu, Q.Y.; Allen, P.K.; Rebueno, N.; Gomez, D.R.; Balter, P.; Komaki, R.; Mehran, R.; Swisher, S.G.; et al. Stereotactic ablative radiation therapy for centrally located early stage or isolated parenchymal recurrences of non-small cell lung cancer: How to fly in a “no fly zone”. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1120–1128. [Google Scholar] [CrossRef] [PubMed]
- Kanemoto, A.; Matsumoto, Y.; Sugita, T. Timing and characteristics of radiation pneumonitis after stereotactic body radiotherapy for peripherally located stage I lung cancer. Int. J. Clin. Oncol. 2015, 20, 680–685. [Google Scholar] [CrossRef]
- Zhao, J.; Yorke, E.D.; Li, L.; Kavanagh, B.D.; Li, X.A.; Das, S.; Miften, M.; Rimner, A.; Campbell, J.; Xue, J.; et al. Simple factors associated with radiation-induced lung toxicity after stereotactic body radiation therapy of the thorax: A pooled analysis of 88 studies. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1357–1366. [Google Scholar] [CrossRef] [Green Version]
- Berg, J.; Ramberg, C.; Haugstvedt, J.O.S.; Bengtson, M.B.; Gabrielsen, A.M.; Brustugun, O.T.; Halvorsen, A.R.; Helland, A. Lung function after stereotactic body radiation therapy for early-stage non-small cell lung cancer, changes and predictive markers. Front. Oncol. 2021, 11, 674731. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, W.; Shiue, K.; Yao, H.; Cerra-Franco, A.; Shapiro, R.H.; Huang, K.C.; Vile, D.; Langer, M.; Watson, G.; et al. Risk factors for symptomatic radiation pneumonitis after stereotactic body radiation therapy (SBRT) in patients with non-small cell lung cancer. Radiother. Oncol. 2021, 156, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.S.; Moiseenko, V.; Zhao, J.; Milano, M.T.; Li, L.; Rimner, A.; Das, S.; Li, X.A.; Miften, M.; Liao, Z.; et al. Organs at risk considerations for thoracic stereotactic body radiation therapy: What is safe for lung Parenchyma? Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 172–187. [Google Scholar] [CrossRef]
- Stokes, W.A.; Bronsert, M.R.; Meguid, R.A.; Blum, M.G.; Jones, B.L.; Koshy, M.; Sher, D.J.; Louie, A.V.; Palma, D.A.; Senan, S.; et al. Post-treatment mortality after surgery and stereotactic body radiotherapy for early-stage non-small-cell lung cancer. J. Clin. Oncol. 2018, 36, 642–651. [Google Scholar] [CrossRef]
- Adebahr, S.; Hechtner, M.; Schrader, N.; Schimek-Jasch, T.; Kaier, K.; Duncker-Rohr, V.; Gkika, E.; Momm, F.; Gaertner, J.; Becker, G.; et al. Early impact of pulmonary fractionated stereotactic body radiotherapy on quality of life: Benefit for patients with low initial scores (STRIPE trial). J. Thorac. Oncol. 2019, 14, 408–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nestle, U.; Adebahr, S.; Kaier, K.; Gkika, E.; Schimek-Jasch, T.; Hechtner, M.; Momm, F.; Gaertner, J.; Becker, G.; Grosu, A.L. Quality of life after pulmonary stereotactic fractionated radiotherapy (SBRT): Results of the phase II STRIPE trial. Radiother. Oncol. 2020, 148, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Shinde, A.; Li, R.; Kim, J.; Salgia, R.; Hurria, A.; Amini, A. Stereotactic body radiation therapy (SBRT) for early-stage lung cancer in the elderly. Semin. Oncol. 2018, 45, 210–219. [Google Scholar] [CrossRef]
- Leaman-Alcibar, O.; Cigarral, C.; Deniz, C.; Romero-Palomar, I.; Navarro-Martin, A. Quality of life after stereotactic body radiation therapy versus video-assisted thoracic surgery in early stage non-small cell lung cancer. Is there enough data to make a recommendation? J. Clin. Transl. Res. 2021, 7, 209–220. [Google Scholar] [PubMed]
- Von Reibnitz, D.; Shaikh, F.; Wu, A.J.; Treharne, G.C.; Dick-Godfrey, R.; Foster, A.; Woo, K.M.; Shi, W.; Zhang, Z.; Din, S.U.; et al. Stereotactic body radiation therapy (SBRT) improves local control and overall survival compared to conventionally fractionated radiation for stage I non-small cell lung cancer (NSCLC). Acta Oncol. 2018, 57, 1567–1573. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Thor, M.; Rimner, A.; Deasy, J.O.; Cella, L. Spatial signature of dose patterns associated with acute radiation-induced lung damage in lung cancer patients treated with stereotactic body radiation therapy. Phys. Med. Biol. 2019, 64, 155006. [Google Scholar] [CrossRef]
- Nalbantov, G.; Kietselaer, B.; Vandecasteele, K.; Oberije, C.; Berbee, M.; Troost, E.; Dingemans, A.M.; van Baardwijk, A.; Smits, K.; Dekker, A.; et al. Cardiac comorbidity is an independent risk factor for radiation-induced lung toxicity in lung cancer patients. Radiother. Oncol. 2013, 109, 100–106. [Google Scholar] [CrossRef]
- Conson, M.; Cella, L.; Pacelli, R.; Comerci, M.; Liuzzi, R.; Salvatore, M.; Quarantelli, M. Automated delineation of brain structures in patients undergoing radiotherapy for primary brain tumors: From atlas to dose-volume histograms. Radiother. Oncol. 2014, 112, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palma, G.; Monti, S.; Conson, M.; Xu, T.; Hahn, S.; Durante, M.; Mohan, R.; Liao, Z.; Cella, L. NTCP Models for severe radiation induced dermatitis after IMRT or proton therapy for thoracic cancer patients. Front. Oncol. 2020, 10, 344. [Google Scholar] [CrossRef] [PubMed]
- Alterio, D.; Gerardi, M.A.; Cella, L.; Spoto, R.; Zurlo, V.; Sabbatini, A.; Fodor, C.; D’Avino, V.; Conson, M.; Valoriani, F.; et al. Radiation-induced acute dysphagia: Prospective observational study on 42 head and neck cancer patients. Strahlenther. Onkol. 2017, 193, 971–981. [Google Scholar] [CrossRef]
- D’Avino, V.; Palma, G.; Liuzzi, R.; Conson, M.; Doria, F.; Salvatore, M.; Pacelli, R.; Cella, L. Prediction of gastrointestinal toxicity after external beam radiotherapy for localized prostate cancer. Radiat. Oncol. 2015, 10, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, L.; D’Avino, V.; Liuzzi, R.; Conson, M.; Doria, F.; Faiella, A.; Loffredo, F.; Salvatore, M.; Pacelli, R. Multivariate normal tissue complication probability modeling of gastrointestinal toxicity after external beam radiotherapy for localized prostate cancer. Radiat. Oncol. 2013, 8, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, L.; Oh, J.H.; Deasy, J.O.; Palma, G.; Liuzzi, R.; D’Avino, V.; Conson, M.; Picardi, M.; Salvatore, M.; Pacelli, R. Predicting radiation-induced valvular heart damage. Acta Oncol. 2015, 54, 1796–1804. [Google Scholar] [CrossRef]
- Palma, G.; Taffelli, A.; Fellin, F.; D’Avino, V.; Scartoni, D.; Tommasino, F.; Scifoni, E.; Durante, M.; Amichetti, M.; Schwarz, M.; et al. Modelling the risk of radiation induced alopecia in brain tumor patients treated with scanned proton beams. Radiother. Oncol. 2020, 144, 127–134. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Buonanno, A.; Pacelli, R.; Cella, L. PACE: A probabilistic atlas for normal tissue complication estimation in radiation oncology. Front. Oncol. 2019, 9, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temming, S.; Kocher, M.; Stoelben, E.; Hagmeyer, L.; Chang, D.H.; Frank, K.; Hekmat, K.; Wolf, J.; Baus, W.W.; Semrau, R.; et al. Risk-adapted robotic stereotactic body radiation therapy for inoperable early-stage non-small-cell lung cancer. Strahlenther. Onkol. 2018, 194, 91–97. [Google Scholar] [CrossRef]
- Ball, D.; Mai, G.T.; Vinod, S.; Babington, S.; Ruben, J.; Kron, T.; Chesson, B.; Herschtal, A.; Vanevski, M.; Rezo, A.; et al. Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): A phase 3, open-label, randomised controlled trial. Lancet Oncol. 2019, 20, 494–503. [Google Scholar] [CrossRef]
- Nyman, J.; Hallqvist, A.; Lund, J.A.; Brustugun, O.T.; Bergman, B.; Bergstrom, P.; Friesland, S.; Lewensohn, R.; Holmberg, E.; Lax, I. SPACE—A randomized study of SBRT vs conventional fractionated radiotherapy in medically inoperable stage I NSCLC. Radiother. Oncol. 2016, 121, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guckenberger, M.; Baier, K.; Polat, B.; Richter, A.; Krieger, T.; Wilbert, J.; Mueller, G.; Flentje, M. Dose-response relationship for radiation-induced pneumonitis after pulmonary stereotactic body radiotherapy. Radiother. Oncol. 2010, 97, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Baser, S.; Shannon, V.R.; Eapen, G.A.; Jimenez, C.A.; Onn, A.; Keus, L.; Lin, E.; Morice, R.C. Pulmonary dysfunction as a major cause of inoperability among patients with non-small-cell lung cancer. Clin. Lung Cancer 2006, 7, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Rancati, T.; Ceresoli, G.L.; Gagliardi, G.; Schipani, S.; Cattaneo, G.M. Factors predicting radiation pneumonitis in lung cancer patients: A retrospective study. Radiother. Oncol. 2003, 67, 275–283. [Google Scholar] [CrossRef]
- Paludan, M.; Traberg Hansen, A.; Petersen, J.; Grau, C.; Hoyer, M. Aggravation of dyspnea in stage I non-small cell lung cancer patients following stereotactic body radiotherapy: Is there a dose-volume dependency? Acta Oncol. 2006, 45, 818–822. [Google Scholar] [CrossRef]
- Inoue, T.; Shiomi, H.; Oh, R.J. Stereotactic body radiotherapy for stage I lung cancer with chronic obstructive pulmonary disease: Special reference to survival and radiation-induced pneumonitis. J. Radiat. Res. 2015, 56, 727–734. [Google Scholar] [CrossRef] [Green Version]
- Van Luijk, P.; Novakova-Jiresova, A.; Faber, H.; Schippers, J.M.; Kampinga, H.H.; Meertens, H.; Coppes, R.P. Radiation damage to the heart enhances early radiation-induced lung function loss. Cancer Res. 2005, 65, 6509–6511. [Google Scholar] [CrossRef] [Green Version]
- Ghobadi, G.; van der Veen, S.; Bartelds, B.; de Boer, R.A.; Dickinson, M.G.; de Jong, J.R.; Faber, H.; Niemantsverdriet, M.; Brandenburg, S.; Berger, R.M.; et al. Physiological interaction of heart and lung in thoracic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, e639–e646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, E.X.; Hope, A.J.; Lindsay, P.E.; Trovo, M.; El Naqa, I.; Deasy, J.O.; Bradley, J.D. Heart irradiation as a risk factor for radiation pneumonitis. Acta Oncol. 2011, 50, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, L.; Palma, G.; Deasy, J.O.; Oh, J.H.; Liuzzi, R.; D’Avino, V.; Conson, M.; Pugliese, N.; Picardi, M.; Salvatore, M.; et al. Complication probability models for radiation-induced heart valvular dysfunction: Do heart-lung interactions play a role? PLoS ONE 2014, 9, e111753. [Google Scholar] [CrossRef] [PubMed]
- Trott, K.R.; Doerr, W.; Facoetti, A.; Hopewell, J.; Langendijk, J.; van Luijk, P.; Ottolenghi, A.; Smyth, V. Biological mechanisms of normal tissue damage: Importance for the design of NTCP models. Radiother. Oncol. 2012, 105, 79–85. [Google Scholar] [CrossRef]
- Sardaro, A.; McDonald, F.; Bardoscia, L.; Lavrenkov, K.; Singh, S.; Ashley, S.; Traish, D.; Ferrari, C.; Meattini, I.; Asabella, A.N.; et al. Dyspnea in patients receiving radical radiotherapy for non-small cell lung cancer: A prospective study. Front. Oncol. 2020, 10, 594590. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Cella, L. Voxel-based analysis in radiation oncology: A methodological cookbook. Phys. Med. 2020, 69, 192–204. [Google Scholar] [CrossRef]
- Shortall, J.; Palma, G.; Mistry, H.; Vasquez Osorio, E.; McWilliam, A.; Choudhury, A.; Aznar, M.; van Herk, M.; Green, A. Flogging a dead salmon? Reduced dose posterior to prostate correlates with increased PSA progression in voxel-based analysis of 3 randomized phase 3 trials. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 696–699. [Google Scholar] [CrossRef]
- Monti, S.; Palma, G.; D’Avino, V.; Gerardi, M.; Marvaso, G.; Ciardo, D.; Pacelli, R.; Jereczek-Fossa, B.A.; Alterio, D.; Cella, L. Voxel-based analysis unveils regional dose differences associated with radiation-induced morbidity in head and neck cancer patients. Sci. Rep. 2017, 7, 7220. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; D’Avino, V.; Conson, M.; Liuzzi, R.; Pressello, M.C.; Donato, V.; Deasy, J.O.; Quarantelli, M.; Pacelli, R.; et al. A voxel-based approach to explore local dose differences associated with radiation-induced lung damage. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Beasley, W.; Thor, M.; McWilliam, A.; Green, A.; Mackay, R.; Slevin, N.; Olsson, C.; Pettersson, N.; Finizia, C.; Estilo, C.; et al. Image-based data mining to probe dosimetric correlates of radiation-induced trismus. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1330–1338. [Google Scholar] [CrossRef]
- Cella, L.; Monti, S.; Xu, T.; Liuzzi, R.; Stanzione, A.; Durante, M.; Mohan, R.; Liao, Z.; Palma, G. Probing thoracic dose patterns associated to pericardial effusion and mortality in patients treated with photons and protons for locally advanced non-small-cell lung cancer. Radiother. Oncol. 2021, 160, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Monti, S.; Pacelli, R.; Cella, L.; Palma, G. Inter-patient image registration algorithms to disentangle regional dose bioeffects. Sci. Rep. 2018, 8, 4915. [Google Scholar] [CrossRef] [PubMed]
- Palma, G.; Monti, S.; Xu, T.; Scifoni, E.; Yang, P.; Hahn, S.M.; Durante, M.; Mohan, R.; Liao, Z.; Cella, L. Spatial dose patterns associated with radiation pneumonitis in a randomized trial comparing intensity-modulated photon therapy with passive scattering proton therapy for locally advanced non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1124–1132. [Google Scholar] [CrossRef] [PubMed]
- Palma, G.; Monti, S.; Pacelli, R.; Liao, Z.; Deasy, J.O.; Mohan, R.; Cella, L. Radiation pneumonitis in thoracic cancer patients: Multi-center voxel-based analysis. Cancers 2021, 13, 3553. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n = 106 |
|---|---|
| Continuous variables | Median (Range) |
| Age at RT (yr.) | 75 (32–93) |
| Lung-GTV Volume (cm3) | 3013 (1537–7644) |
| GTV (cm3) | 6.4 (0.3–162.9) |
| Heart Volume (cm3) | 682 (340–1316) |
| KPS baseline (%) | 90 (60–100) |
| Categorical variables | n (%) |
| Gender | |
| Male | 45 (43) |
| Female | 61 (57) |
| Histology | |
| Adenocarcinoma | 82 (77) |
| Squamous Cell Carcinoma | 16 (15) |
| Unknown | 8 (8) |
| Tumor position | |
| Right lung | 66 (62) |
| Left lung | 40 (38) |
| Upper lobe | 61 (58) |
| Middle lobe | 4 (4) |
| Lower lobe | 41 (39) |
| COPD | |
| No | 61 (58) |
| Yes | 45 (42) |
| Smoking | |
| Never | 15 (14) |
| Former | 80 (76) |
| Current | 11 (10) |
| Fractionation schedule | |
| 18 Gy × 3 fx | 24 (23) |
| 12 Gy × 4 fx | 38 (36) |
| 10 Gy × 5 fx | 33 (31) |
| 9 Gy × 5 fx | 7 (7) |
| 8 Gy × 5 fx | 4 (4) |
| Dyspnea within 6 months | |
| Grade 0 | 50 (47) |
| Grade 1 | 31 (29) |
| Grade 2 | 17 (16) |
| Grade 3 | 8 (8) |
| Model Variables | Coefficient | SE | p |
|---|---|---|---|
| COPD | 1.02 | 0.43 | 0.02 |
| Lungs V15Gy|α/β=3 | 9.3 | 4.6 | 0.04 |
| Heart Volume (cc) | 0.0021 | 0.0011 | 0.06 |
| constant | −3.09 | 1.09 | 0.004 |
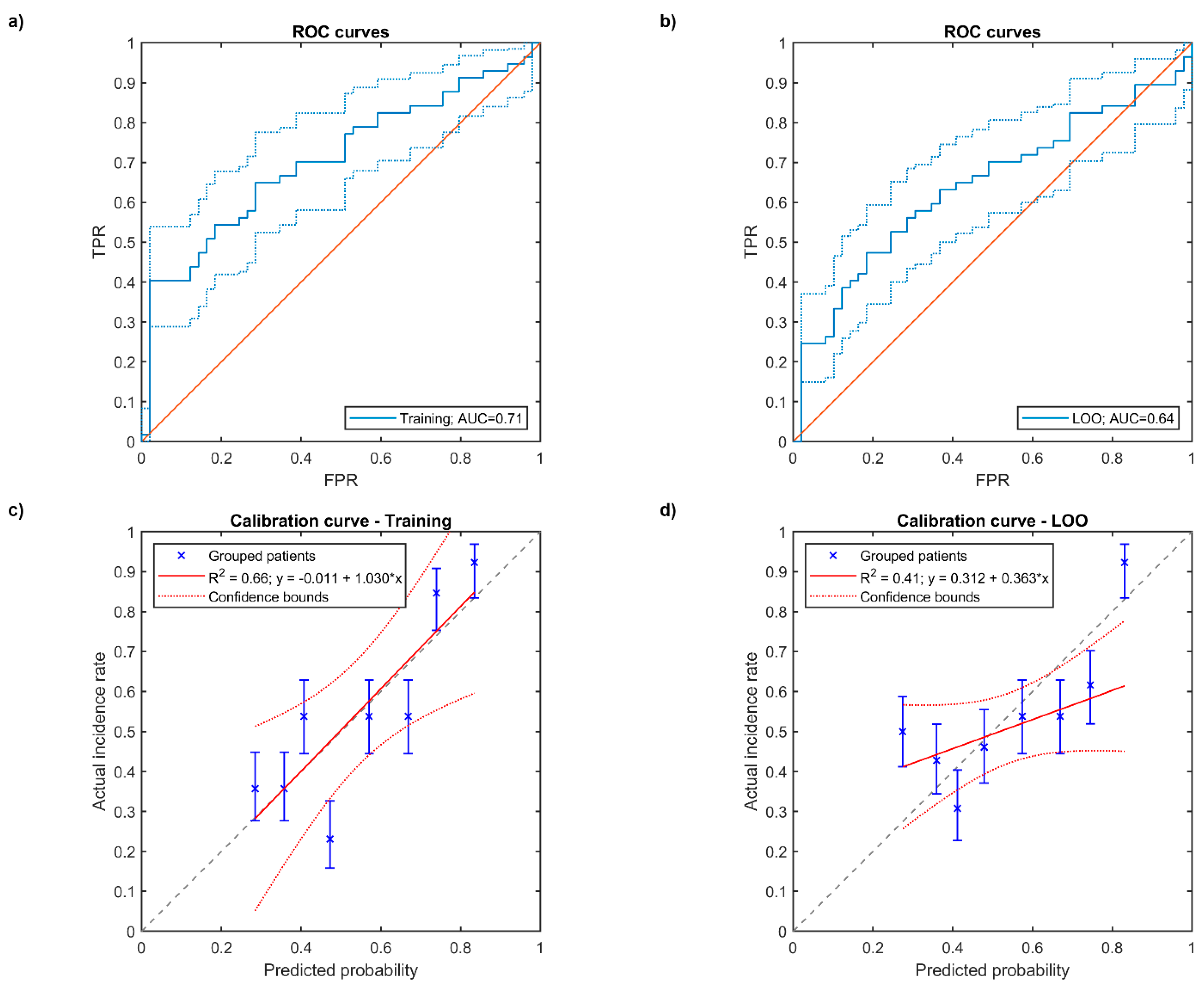
| AUC | 0.71 (0.61–0.80) | ||
| CV-AUC | 0.64 (0.53–0.74) | ||
| Brier score | 0.215 | ||
| CV-Brier score | 0.236 | ||
| Calibration intercept | −0.01 | 0.17 | |
| Calibration slope | 1.03 | 0.30 | |
| CV-Calibration intercept | 0.31 | 0.11 | |
| CV-Calibration slope | 0.36 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cella, L.; Monti, S.; Thor, M.; Rimner, A.; Deasy, J.O.; Palma, G. Radiation-Induced Dyspnea in Lung Cancer Patients Treated with Stereotactic Body Radiation Therapy. Cancers 2021, 13, 3734. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153734
Cella L, Monti S, Thor M, Rimner A, Deasy JO, Palma G. Radiation-Induced Dyspnea in Lung Cancer Patients Treated with Stereotactic Body Radiation Therapy. Cancers. 2021; 13(15):3734. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153734
Chicago/Turabian StyleCella, Laura, Serena Monti, Maria Thor, Andreas Rimner, Joseph O. Deasy, and Giuseppe Palma. 2021. "Radiation-Induced Dyspnea in Lung Cancer Patients Treated with Stereotactic Body Radiation Therapy" Cancers 13, no. 15: 3734. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153734