Prognostic Impacts of D816V KIT Mutation and Peri-Transplant RUNX1–RUNX1T1 MRD Monitoring on Acute Myeloid Leukemia with RUNX1–RUNX1T1

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics and KIT Mutations
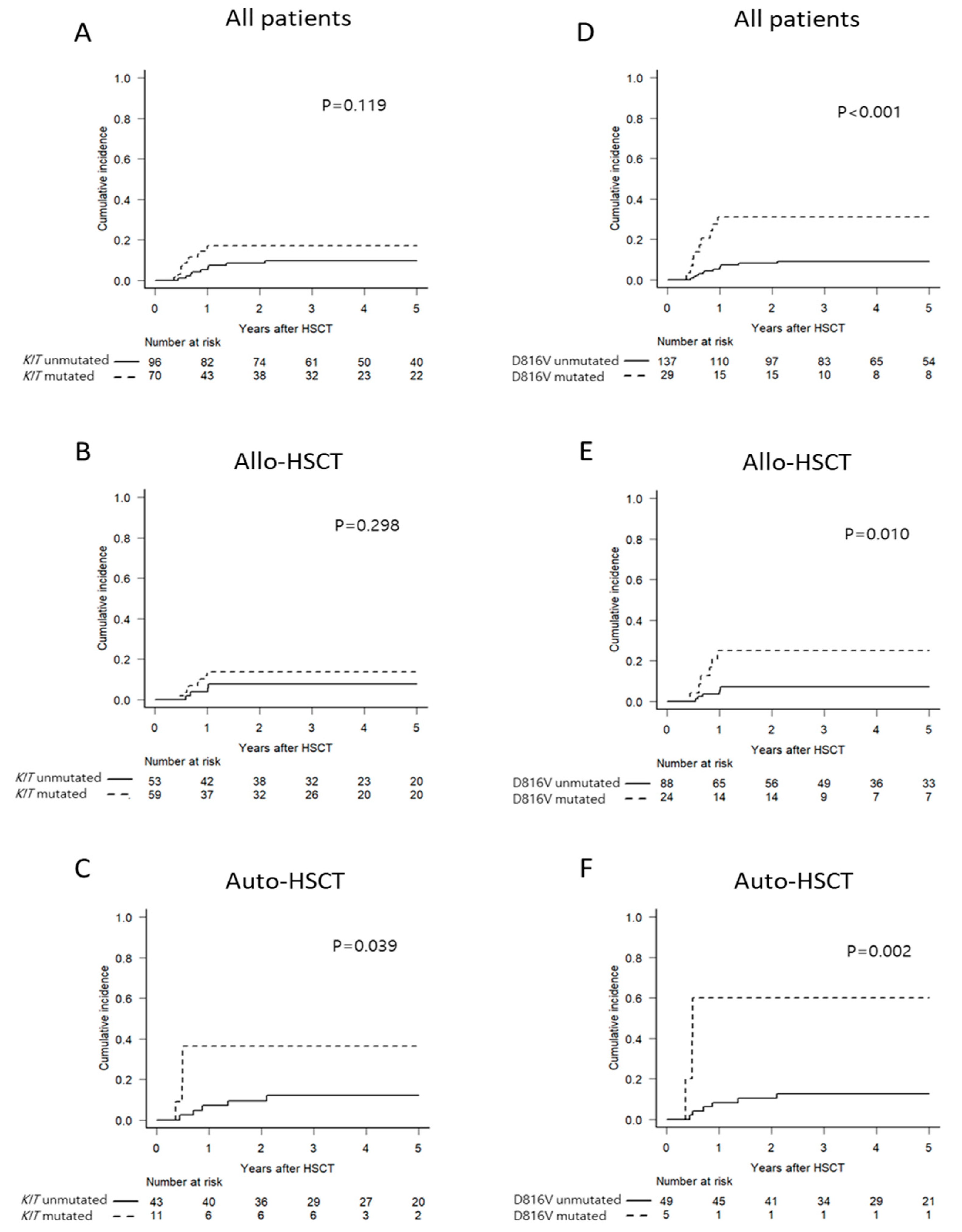
2.2. Impact of KIT Mutations Status on RUNX1–RUNX1T1 MRD Kinetics and Survival Outcomes
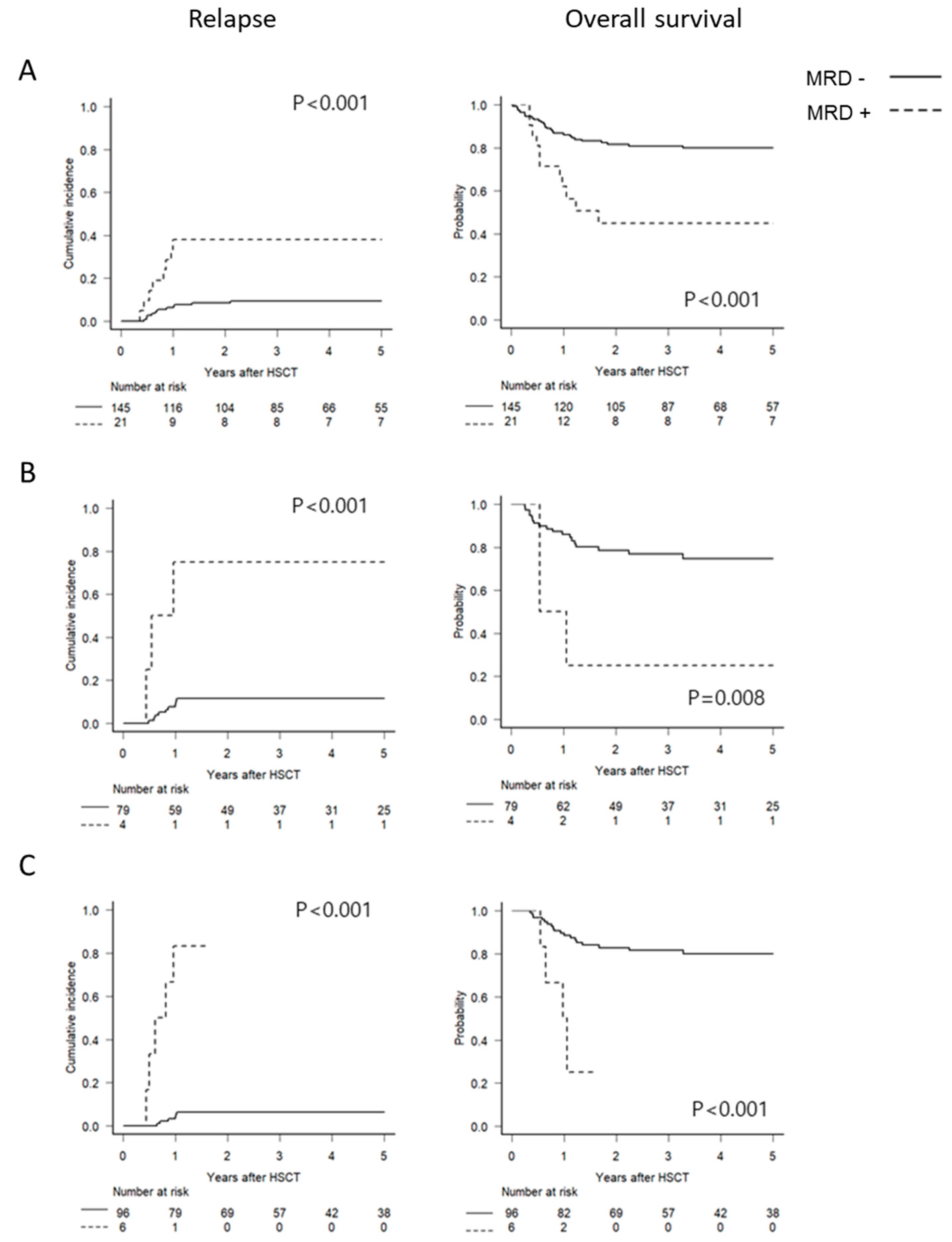
2.3. Optimal Time Points and Thresholds for RUNX1–RUNX1T1 MRD Monitoring
2.4. Prognostic Independency of D816V KIT Mutation and RUNX1–RUNX1T1 MRD Status
2.5. Outcomes of Transplant Type in Each Group Stratified by D816V KIT Mutation and RUNX1–RUNX1T1 MRD Status at Pre-HSCT
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Chemotherapy and Transplant Procedures
4.3. Cytogenetic and Molecular Analyses
4.4. RUNX1–RUNX1T1 MRD Assessment and Definitions
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jourdan, E.; Boissel, N.; Chevret, S.; Delabesse, E.; Renneville, A.; Cornillet, P.; Blanchet, O.; Cayuela, J.M.; Recher, C.; Raffoux, E.; et al. Prospective evaluation of gene mutations and minimal residual disease in patients with core binding factor acute myeloid leukemia. Blood 2013, 121, 2213–2223. [Google Scholar] [CrossRef] [PubMed]
- Marcucci, G.; Mrozek, K.; Ruppert, A.S.; Maharry, K.; Kolitz, J.E.; Moore, J.O.; Mayer, R.J.; Pettenati, M.J.; Powell, B.L.; Edwards, C.G.; et al. Prognostic factors and outcome of core binding factor acute myeloid leukemia patients with t(8;21) differ from those of patients with inv(16): A Cancer and Leukemia Group B study. J. Clin. Oncol. 2005, 23, 5705–5717. [Google Scholar] [CrossRef] [PubMed]
- Schlenk, R.F.; Benner, A.; Krauter, J.; Buchner, T.; Sauerland, C.; Ehninger, G.; Schaich, M.; Mohr, B.; Niederwieser, D.; Krahl, R.; et al. Individual patient data-based meta-analysis of patients aged 16 to 60 years with core binding factor acute myeloid leukemia: A survey of the German Acute Myeloid Leukemia Intergroup. J. Clin. Oncol. 2004, 22, 3741–3750. [Google Scholar] [CrossRef] [PubMed]
- Cher, C.Y.; Leung, G.M.; Au, C.H.; Chan, T.L.; Ma, E.S.; Sim, J.P.; Gill, H.; Lie, A.K.; Liang, R.; Wong, K.F.; et al. Next-generation sequencing with a myeloid gene panel in core-binding factor AML showed KIT activation loop and TET2 mutations predictive of outcome. Blood Cancer J. 2016, 6, e442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duployez, N.; Marceau-Renaut, A.; Boissel, N.; Petit, A.; Bucci, M.; Geffroy, S.; Lapillonne, H.; Renneville, A.; Ragu, C.; Figeac, M.; et al. Comprehensive mutational profiling of core binding factor acute myeloid leukemia. Blood 2016, 127, 2451–2459. [Google Scholar] [CrossRef]
- Faber, Z.J.; Chen, X.; Gedman, A.L.; Boggs, K.; Cheng, J.; Ma, J.; Radtke, I.; Chao, J.R.; Walsh, M.P.; Song, G.; et al. The genomic landscape of core-binding factor acute myeloid leukemias. Nat. Genet. 2016, 48, 1551–1556. [Google Scholar] [CrossRef]
- Kawashima, N.; Akashi, A.; Nagata, Y.; Kihara, R.; Ishikawa, Y.; Asou, N.; Ohtake, S.; Miyawaki, S.; Sakura, T.; Ozawa, Y.; et al. Clinical significance of ASXL2 and ZBTB7A mutations and C-terminally truncated RUNX1-RUNX1T1 expression in AML patients with t(8;21) enrolled in the JALSG AML201 study. Ann. Hematol. 2019, 98, 83–91. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Kawashima, N.; Atsuta, Y.; Sugiura, I.; Sawa, M.; Dobashi, N.; Yokoyama, H.; Doki, N.; Tomita, A.; Kiguchi, T.; et al. Prospective evaluation of prognostic impact of KIT mutations on acute myeloid leukemia with RUNX1-RUNX1T1 and CBFB-MYH11. Blood Adv. 2020, 4, 66–75. [Google Scholar] [CrossRef]
- Kim, H.J.; Ahn, H.K.; Jung, C.W.; Moon, J.H.; Park, C.H.; Lee, K.O.; Kim, S.H.; Kim, Y.K.; Kim, H.J.; Sohn, S.K.; et al. KIT D816 mutation associates with adverse outcomes in core binding factor acute myeloid leukemia, especially in the subgroup with RUNX1/RUNX1T1 rearrangement. Ann. Hematol. 2013, 92, 163–171. [Google Scholar] [CrossRef]
- Rucker, F.G.; Agrawal, M.; Corbacioglu, A.; Weber, D.; Kapp-Schwoerer, S.; Gaidzik, V.I.; Jahn, N.; Schroeder, T.; Wattad, M.; Lubbert, M.; et al. Measurable residual disease monitoring in acute myeloid leukemia with t(8;21)(q22;q22.1): Results from the AML Study Group. Blood 2019, 134, 1608–1618. [Google Scholar] [CrossRef]
- Krauth, M.T.; Eder, C.; Alpermann, T.; Bacher, U.; Nadarajah, N.; Kern, W.; Haferlach, C.; Haferlach, T.; Schnittger, S. High number of additional genetic lesions in acute myeloid leukemia with t(8;21)/RUNX1-RUNX1T1: Frequency and impact on clinical outcome. Leukemia 2014, 28, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Xie, H.; Wang, H.; Chen, L.; Sun, Y.; Chen, Z.; Li, Q. Prognostic Significance of KIT Mutations in Core-Binding Factor Acute Myeloid Leukemia: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0146614. [Google Scholar] [CrossRef] [PubMed]
- Dohner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Buchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, G.; Yin, C.; Wu, F.; Jiang, L.; Zheng, Z.; Xu, D.; Zhou, J.; Jiang, X.; Liu, Q.; Meng, F. Gene mutation profile and risk stratification in AML1ETOpositive acute myeloid leukemia based on nextgeneration sequencing. Oncol. Rep. 2019, 42, 2333–2344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuurhuis, G.J.; Heuser, M.; Freeman, S.; Bene, M.C.; Buccisano, F.; Cloos, J.; Grimwade, D.; Haferlach, T.; Hills, R.K.; Hourigan, C.S.; et al. Minimal/measurable residual disease in AML: A consensus document from the European LeukemiaNet MRD Working Party. Blood 2018, 131, 1275–1291. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wu, D.P.; Liu, Q.F.; Qin, Y.Z.; Wang, J.B.; Xu, L.P.; Liu, Y.R.; Zhu, H.H.; Chen, J.; Dai, M.; et al. In adults with t(8;21)AML, posttransplant RUNX1/RUNX1T1-based MRD monitoring, rather than c-KIT mutations, allows further risk stratification. Blood 2014, 124, 1880–1886. [Google Scholar] [CrossRef]
- Yin, J.A.; O’Brien, M.A.; Hills, R.K.; Daly, S.B.; Wheatley, K.; Burnett, A.K. Minimal residual disease monitoring by quantitative RT-PCR in core binding factor AML allows risk stratification and predicts relapse: Results of the United Kingdom MRC AML-15 trial. Blood 2012, 120, 2826–2835. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.H.; Zhang, X.H.; Qin, Y.Z.; Liu, D.H.; Jiang, H.; Chen, H.; Jiang, Q.; Xu, L.P.; Lu, J.; Han, W.; et al. MRD-directed risk stratification treatment may improve outcomes of t(8;21) AML in the first complete remission: Results from the AML05 multicenter trial. Blood 2013, 121, 4056–4062. [Google Scholar] [CrossRef]
- Gorin, N.C.; Labopin, M.; Frassoni, F.; Milpied, N.; Attal, M.; Blaise, D.; Meloni, G.; Iori, A.P.; Michallet, M.; Willemze, R.; et al. Identical outcome after autologous or allogeneic genoidentical hematopoietic stem-cell transplantation in first remission of acute myelocytic leukemia carrying inversion 16 or t(8;21): A retrospective study from the European Cooperative Group for Blood and Marrow Transplantation. J. Clin. Oncol. 2008, 26, 3183–3188. [Google Scholar] [CrossRef]
- Nakasone, H.; Izutsu, K.; Wakita, S.; Yamaguchi, H.; Muramatsu-Kida, M.; Usuki, K. Autologous stem cell transplantation with PCR-negative graft would be associated with a favorable outcome in core-binding factor acute myeloid leukemia. Biol. Blood Marrow Transplant. 2008, 14, 1262–1269. [Google Scholar] [CrossRef] [Green Version]
- Kuwatsuka, Y.; Miyamura, K.; Suzuki, R.; Kasai, M.; Maruta, A.; Ogawa, H.; Tanosaki, R.; Takahashi, S.; Koda, K.; Yago, K.; et al. Hematopoietic stem cell transplantation for core binding factor acute myeloid leukemia: T(8;21) and inv(16) represent different clinical outcomes. Blood 2009, 113, 2096–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eom, K.S.; Kim, H.J.; Cho, B.S.; Lee, S.E.; Yahng, S.A.; Yoon, J.H.; Shin, S.H.; Jeon, Y.W.; Kim, J.H.; Kim, Y.J.; et al. Equivalent outcome of autologous stem cell transplantation and reduced intensity conditioning stem cell transplantation in acute myeloid leukemia patients with t(8;21). Acta Haematol. 2015, 133, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.J.; Min, W.S.; Min, Y.H.; Cheong, J.W.; Lee, J.H.; Kim, I.H.; Hong, D.S.; Ahn, J.S.; Kim, H.J.; Lee, W.S.; et al. Different prognostic effects of core-binding factor positive AML with Korean AML registry data. Ann. Hematol. 2019, 98, 1135–1147. [Google Scholar] [CrossRef] [PubMed]
- Al-Harbi, S.; Aljurf, M.; Mohty, M.; Almohareb, F.; Ahmed, S.O.A. An update on the molecular pathogenesis and potential therapeutic targeting of AML with t(8;21)(q22;q22.1);RUNX1-RUNX1T1. Blood Adv. 2020, 4, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansrivijit, P.; Gale, R.P.; Barrett, J.; Ciurea, S.O. Cellular therapy for acute myeloid Leukemia—Current status and future prospects. Blood Rev. 2019, 37, 100578. [Google Scholar] [CrossRef]
- Greiner, J.; Gotz, M.; Bunjes, D.; Hofmann, S.; Wais, V. Immunological and Clinical Impact of Manipulated and Unmanipulated DLI after Allogeneic Stem Cell Transplantation of AML Patients. J. Clin. Med. 2019, 9, 39. [Google Scholar] [CrossRef] [Green Version]
- Tarlock, K.; Alonzo, T.A.; Wang, Y.C.; Gerbing, R.B.; Ries, R.; Loken, M.R.; Pardo, L.; Hylkema, T.; Joaquin, J.; Sarukkai, L.; et al. Functional Properties of KIT Mutations Are Associated with Differential Clinical Outcomes and Response to Targeted Therapeutics in CBF Acute Myeloid Leukemia. Clin. Cancer Res. 2019, 25, 5038–5048. [Google Scholar] [CrossRef]
- Willekens, C.; Blanchet, O.; Renneville, A.; Cornillet-Lefebvre, P.; Pautas, C.; Guieze, R.; Ifrah, N.; Dombret, H.; Jourdan, E.; Preudhomme, C.; et al. Prospective long-term minimal residual disease monitoring using RQ-PCR in RUNX1-RUNX1T1-positive acute myeloid leukemia: Results of the French CBF-2006 trial. Haematologica 2016, 101, 328–335. [Google Scholar] [CrossRef] [Green Version]
- Opatz, S.; Bamopoulos, S.A.; Metzeler, K.H.; Herold, T.; Ksienzyk, B.; Braundl, K.; Tschuri, S.; Vosberg, S.; Konstandin, N.P.; Wang, C.; et al. The clinical mutatome of core binding factor leukemia. Leukemia 2020, 34, 1553–1562. [Google Scholar] [CrossRef] [Green Version]
- Derman, B.A.; Larson, R.A. Post-remission therapy in acute myeloid leukemia: Are we ready for an individualized approach? Best Pract. Res. Clin. Haematol. 2019, 32, 101102. [Google Scholar] [CrossRef]
- Appelbaum, F.R.; Kopecky, K.J.; Tallman, M.S.; Slovak, M.L.; Gundacker, H.M.; Kim, H.T.; Dewald, G.W.; Kantarjian, H.M.; Pierce, S.R.; Estey, E.H. The clinical spectrum of adult acute myeloid leukaemia associated with core binding factor translocations. Br. J. Haematol. 2006, 135, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Byrd, J.C.; Weiss, R.B.; Arthur, D.C.; Lawrence, D.; Baer, M.R.; Davey, F.; Trikha, E.S.; Carroll, A.J.; Tantravahi, R.; Qumsiyeh, M.; et al. Extramedullary leukemia adversely affects hematologic complete remission rate and overall survival in patients with t(8;21)(q22;q22): Results from Cancer and Leukemia Group B 8461. J. Clin. Oncol. 1997, 15, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Kim, H.J.; Kim, J.W.; Jeon, Y.W.; Shin, S.H.; Lee, S.E.; Cho, B.S.; Eom, K.S.; Kim, Y.J.; Lee, S.; et al. Identification of molecular and cytogenetic risk factors for unfavorable core-binding factor-positive adult AML with post-remission treatment outcome analysis including transplantation. Bone Marrow Transplant. 2014, 49, 1466–1474. [Google Scholar] [CrossRef]
- Yoon, J.H.; Kim, H.J.; Park, S.S.; Jeon, Y.W.; Lee, S.E.; Cho, B.S.; Eom, K.S.; Kim, Y.J.; Lee, S.; Min, C.K.; et al. Long-term clinical outcomes of hematopoietic cell transplantation for intermediate-to-poor-risk acute myeloid leukemia during first remission according to available donor types. Oncotarget 2017, 8, 41590–41604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyurkocza, B.; Sandmaier, B.M. Conditioning regimens for hematopoietic cell transplantation: One size does not fit all. Blood 2014, 124, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Lee, G.D.; Park, J.; Yoon, J.H.; Kim, H.J.; Min, W.S.; Kim, M. Quantitative fragment analysis of FLT3-ITD efficiently identifying poor prognostic group with high mutant allele burden or long ITD length. Blood Cancer J. 2015, 5, e336. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (n = 166) | KIT Unmutated (n = 96) | KIT Mutated (n = 70) | p |
|---|---|---|---|---|
| Age at transplantation, years | ||||
| Median (range) | 40 (18–69) | 38 (18–64) | 42 (18–69) | 0.529 |
| Sex, n (%) | 0.814 | |||
| Male | 105 (63) | 60 (64) | 45 (64) | |
| Female | 61 (37) | 36 (36) | 25 (36) | |
| AML type, n (%) | 0.074 | |||
| De novo | 161 (97) | 91 (95) | 70 (100) | |
| Therapy-related | 5 (3) | 5 (5) | 0 | |
| WBC count per liter at diagnosis | ||||
| Median (range) | 8.65 (0.53–100.91) | 7.19 (1.33–100.91) | 10.80 (0.53–68.6) | 0.206 |
| Additional cytogenetic abnormalities, n (%) | ||||
| Del(9q) | 12 (7) | 5 (5) | 7 (10) | 0.239 |
| Trisomy 8 | 2 (1) | 1 (1) | 1 (1) | 1.000 |
| Loss of sex chromosome | 104 (63) | 64 (67) | 40 (57) | 0.210 |
| Del(7q) | 3 (2) | 1 (1) | 2 (3) | 0.574 |
| Complex karyotype | 9 (5) | 4 (4) | 5 (7) | 0.495 |
| KIT mutations n (%) | ||||
| Exon 17-D816V | 29 (18) | 0 | 29 (41) | - |
| Exon 17-D816Y | 14 (8) | 0 | 14 (20) | - |
| Exon 17-D816H | 19 (11) | 0 | 19 (27) | - |
| Exon 17-N822K | 25 (15) | 0 | 25 (36) | - |
| Exon 8 | 5 (3) | 0 | 5 (7) | - |
| FLT3 mutations, n (%) | ||||
| FLT3-ITD | 9 (5) | 6 (6) | 3 (4) | 0.379 |
| FLT3-TKD | 3 (2) | 1 (1) | 2 (3) | 0.327 |
| Missing data | 9 (5) | 7 (7) | 2 (3) | |
| Disease status at HSCT, n (%) | 0.194 | |||
| CR1 | 156 (94) | 88 (92) | 68 (97) | |
| CR2 | 10 (6) | 8 (8) | 2 (3) | |
| Donor type, n (%) | 0.001 | |||
| Matched sibling | 64 (39) | 34 (35) | 30 (43) | |
| Matched unrelated | 25 (15) | 10 (10) | 15 (21) | |
| Haploidentical | 23 (14) | 9 (9) | 14 (20) | |
| Autologous | 54 (32) | 43 (45) | 11 (16) | |
| Stem cell source, n (%) | 0.003 | |||
| Peripheral blood | 111 (67) | 55 (57) | 56 (80) | |
| Bone marrow | 28 (17) | 18 (19) | 10 (14) | |
| Peripheral blood and bone marrow | 27 (16) | 23 (24) | 4 (6) | |
| Conditioning intensity, n (%) | 0.256 | |||
| Myeloablative | 105 (63) | 57 (59) | 48 (69) | |
| Reduced intensity | 61 (37) | 39 (41) | 22 (31) | |
| Interval from diagnosis to transplant, days | ||||
| Median (range) | 194 (96–260) | 195 (96–260) | 184 (102–243) | 0.174 |
| CD34+ cells × 106/kg in graft | ||||
| Median (range) | 3.88 (0.73–16.73) | 3.52 (1.01–16.10) | 4.88 (0.73–16.73) | 0.059 |
| Variables | n Unmutated vs. Mutated | Log10 Transformed Transcript Levels | Log Reduction | ||||
|---|---|---|---|---|---|---|---|
| Unmutated | Mutated | p | Unmutated | Mutated | p | ||
| KIT mutations | |||||||
| Diagnosis | 96 vs. 70 | 0.68 ± 0.02 | 0.64 ± 0.03 | 0.295 | - | - | - |
| Post-induction | 87 vs. 62 | −2.39 ± 0.11 | −2.02 ± 0.11 | 0.021 | −3.07 ± 0.10 | −2.65 ± 0.12 | 0.009 |
| Pre-HSCT | 96 vs. 70 | −4.02 ± 0.14 | −3.32 ± 0.17 | 0.002 | −4.70 ± 0.14 | −3.95 ± 0.17 | 0.001 |
| 1 month after HSCT | 43 vs. 40 | −4.69 ± 0.21 | −4.05 ± 0.24 | 0.044 | −5.38 ± 0.21 | −4.65 ± 0.24 | 0.024 |
| 3 months after HSCT | 57 vs. 45 | −5.07 ± 0.15 | −4.63 ± 0.26 | 0.140 | −5.78 ± 0.15 | −5.24 ± 0.26 | 0.076 |
| D816V KIT mutation | |||||||
| Diagnosis | 137 vs. 29 | 0.67 ± 0.02 | 0.61 ± 0.04 | 0.160 | - | - | - |
| Post-induction | 122 vs. 27 | −2.30 ± 0.09 | −1.92 ± 0.17 | 0.068 | −2.97 ± 0.09 | −2.52 ± 0.17 | 0.026 |
| Pre-HSCT | 137 vs. 29 | −3.82 ± 0.12 | −3.26 ± 0.25 | 0.055 | −4.50 ± 0.12 | −3.86 ± 0.25 | 0.031 |
| 1 month after HSCT | 67 vs. 16 | −4.55 ± 0.17 | −3.68 ± 0.38 | 0.032 | −5.21 ± 0.17 | −4.25 ± 0.41 | 0.019 |
| 3 months after HSCT | 85 vs. 17 | −5.00 ± 0.14 | −4.25 ± 0.44 | 0.049 | −5.68 ± 0.14 | −4.85 ± 0.46 | 0.029 |
| Model #1 | Pre-HSCT | 1 Month after HSCT | 3 Months after HSCT | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| RUNX1–RUNX1T1 levels | ||||||
| ≥3 log reduction | 1 | 1 | 1 | |||
| <3 log reduction | 5.31 (2.06–13.65) | 0.001 | 7.15 (1.59–32.11) | 0.010 | 22.23 (5.03–98.23) | <0.001 |
| KIT mutations | ||||||
| Unmutated | 1 | 1 | 1 | |||
| Mutated | 2.14 (0.81–5.62) | 0.123 | 4.07 (0.73–22.72) | 0.110 | 2.69 (0.42–17.46) | 0.299 |
| Disease state | ||||||
| CR1 | 1 | 1 | 1 | |||
| CR2 | 7.55 (2.0–28.47) | 0.003 | 13.3 (2.18–81.41) | 0.005 | 9.37 (1.31–66.87) | 0.026 |
| Model #2 | Relapse | 1 Month after HSCT | 3 Months after HSCT | |||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| RUNX1–RUNX1T1 levels | ||||||
| ≥3 log reduction | 1 | 1 | 1 | |||
| <3 log reduction | 4.89 (1.91–12.49) | 0.001 | 4.76 (0.95–23.86) | 0.058 | 20.50 (4.68–89.81) | <0.001 |
| D816V KIT mutation | ||||||
| Unmutated | 1 | 1 | 1 | |||
| Mutated | 4.10 (1.63–10.30) | 0.003 | 4.56 (1.02–20.33) | 0.047 | 4.33 (1.01–18.56) | 0.049 |
| Disease state | ||||||
| CR1 | 1 | 1 | 1 | |||
| CR2 | 6.75 (1.86–24.5) | 0.004 | 9.22 (2.04–41.66) | 0.004 | 7.59 (1.31–44.20) | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, B.-S.; Min, G.-J.; Park, S.-S.; Park, S.; Jeon, Y.-W.; Shin, S.-H.; Yahng, S.-A.; Yoon, J.-H.; Lee, S.-E.; Eom, K.-S.; et al. Prognostic Impacts of D816V KIT Mutation and Peri-Transplant RUNX1–RUNX1T1 MRD Monitoring on Acute Myeloid Leukemia with RUNX1–RUNX1T1. Cancers 2021, 13, 336. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13020336
Cho B-S, Min G-J, Park S-S, Park S, Jeon Y-W, Shin S-H, Yahng S-A, Yoon J-H, Lee S-E, Eom K-S, et al. Prognostic Impacts of D816V KIT Mutation and Peri-Transplant RUNX1–RUNX1T1 MRD Monitoring on Acute Myeloid Leukemia with RUNX1–RUNX1T1. Cancers. 2021; 13(2):336. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13020336
Chicago/Turabian StyleCho, Byung-Sik, Gi-June Min, Sung-Soo Park, Silvia Park, Young-Woo Jeon, Seung-Hwan Shin, Seung-Ah Yahng, Jae-Ho Yoon, Sung-Eun Lee, Ki-Seong Eom, and et al. 2021. "Prognostic Impacts of D816V KIT Mutation and Peri-Transplant RUNX1–RUNX1T1 MRD Monitoring on Acute Myeloid Leukemia with RUNX1–RUNX1T1" Cancers 13, no. 2: 336. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13020336