
Landscape of Immune-Related Markers and Potential Therapeutic Targets in Soft Tissue Sarcoma

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
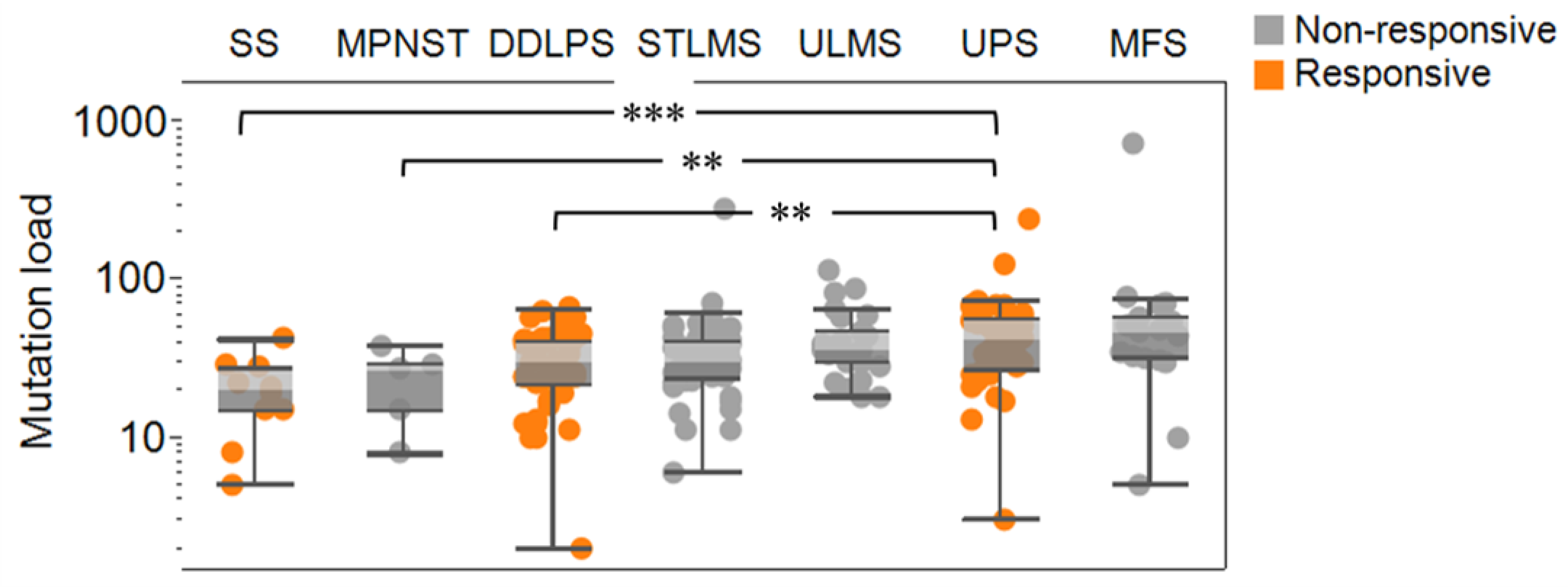
2.1. Mutational Burden Is Indicative of Immunotherapy Response in Soft Tissue Sarcomas
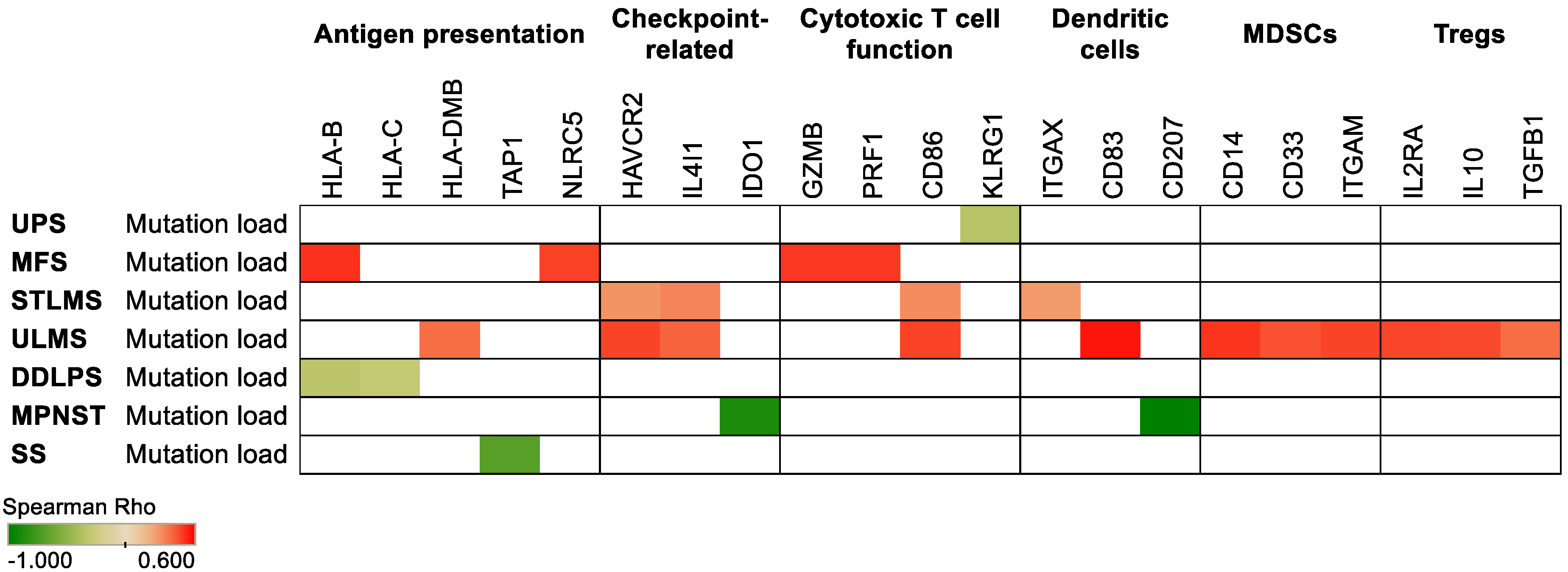
2.2. Increased Mutation Load Is Associated with the Expression of Immune-Related Genes in Soft Tissue Sarcomas
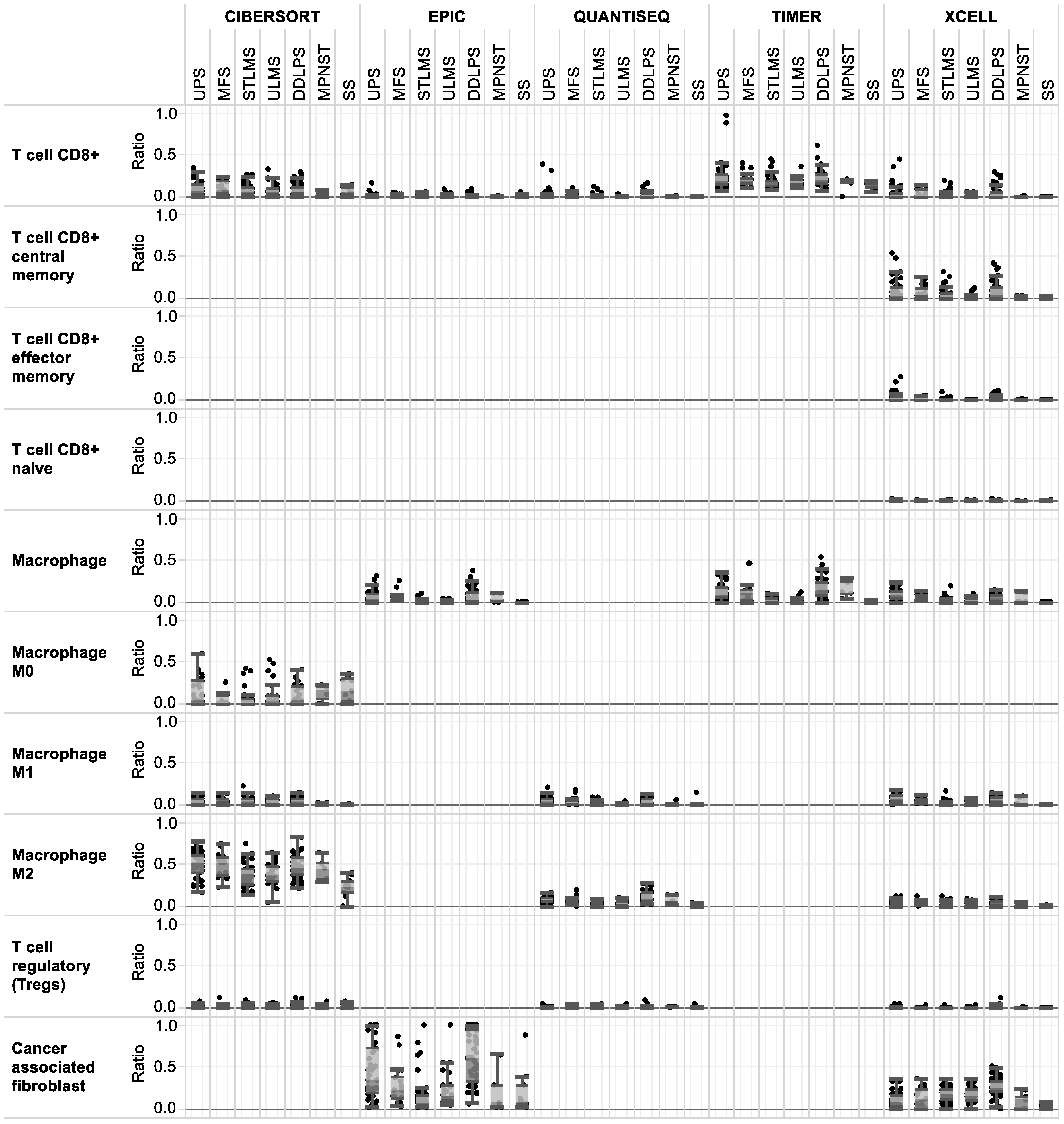
2.3. CD8+ T Cells Are Present in All Soft Tissue Sarcoma Subtypes Based on Immune Infiltrate Analyses
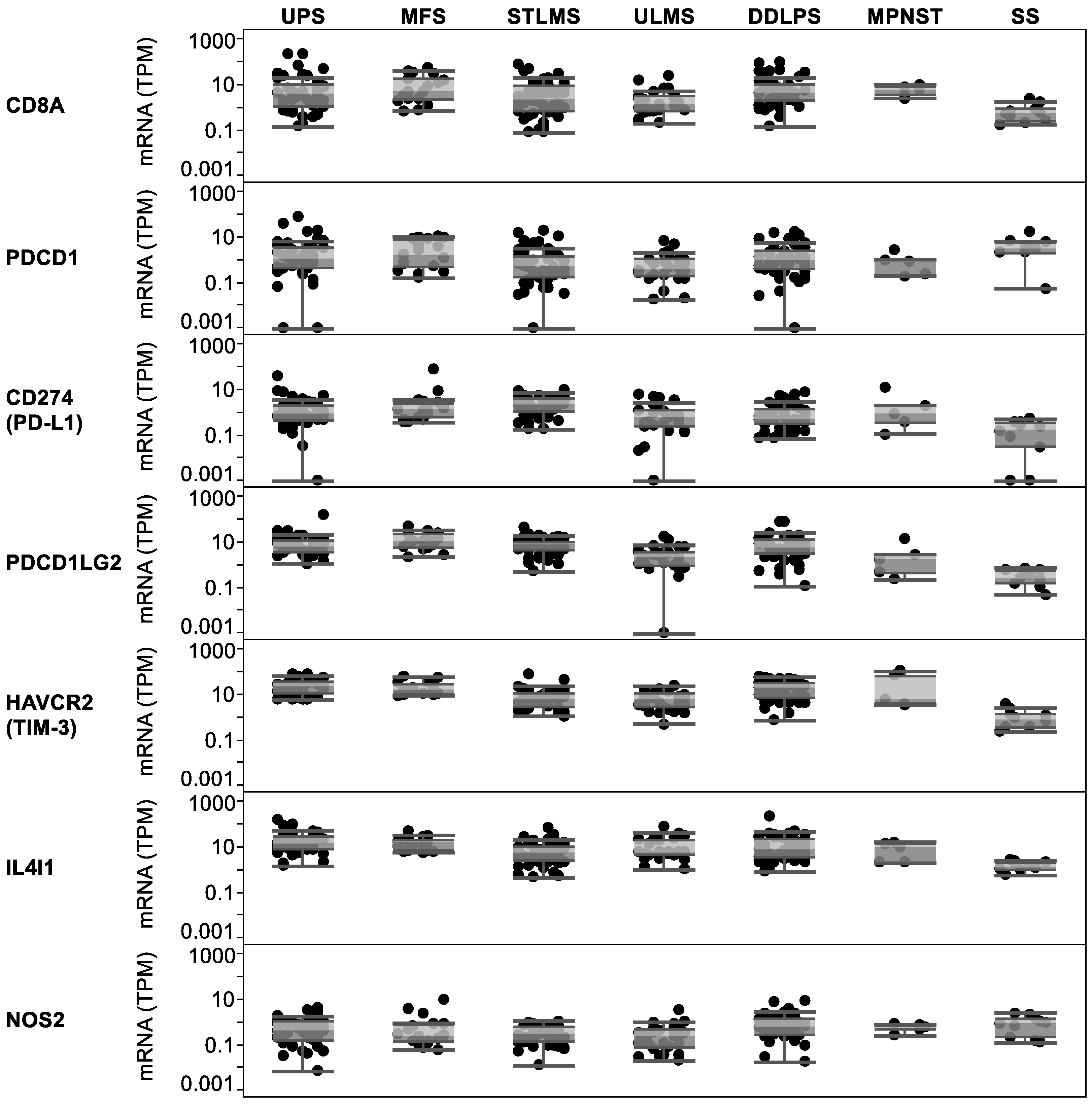
2.4. Key Immune-Related and Checkpoint GENES Are Expressed in All Sarcoma Subtypes and May Be Appropriate Therapy Targets
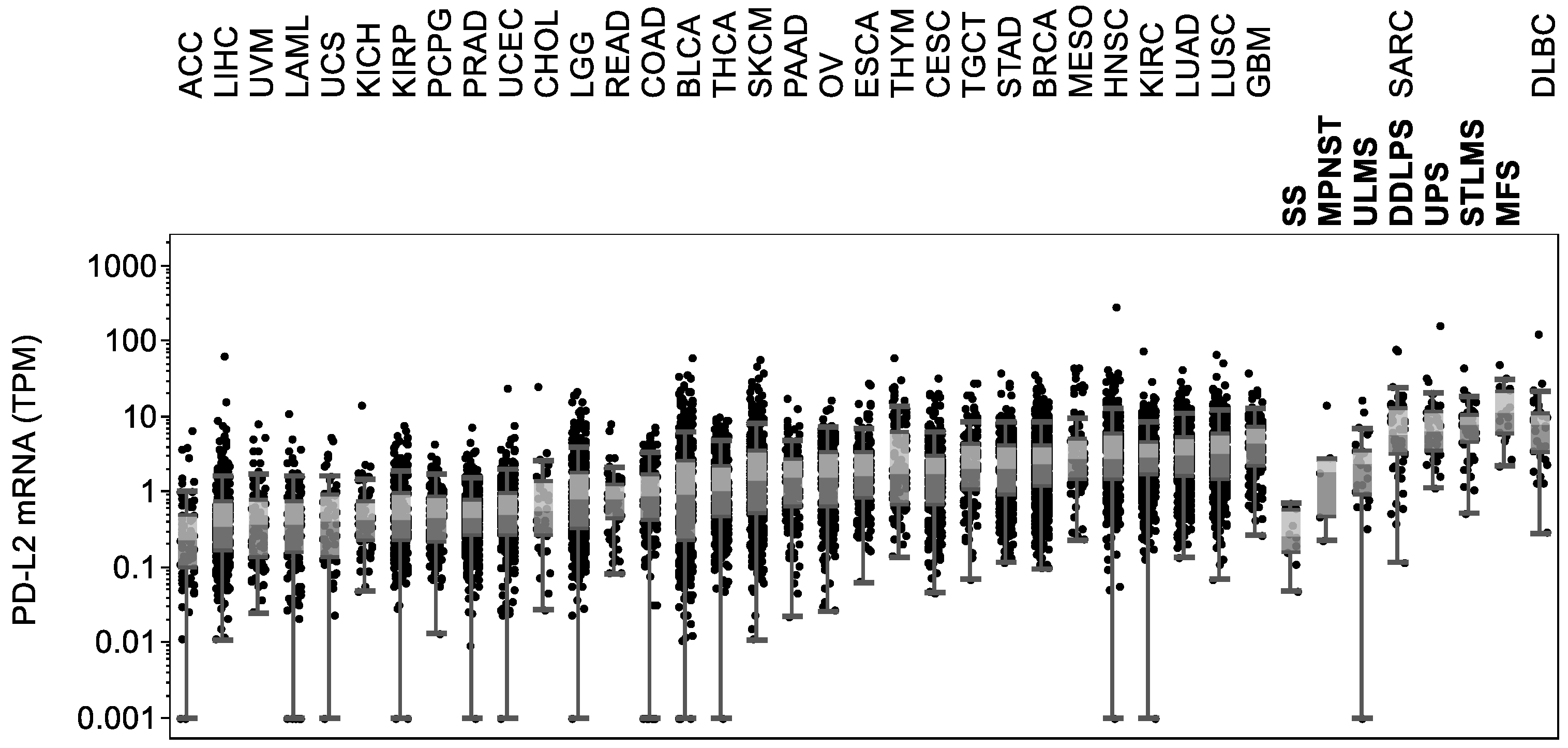
2.5. PD-L2 Expression Levels Are High in Soft Tissue Sarcomas
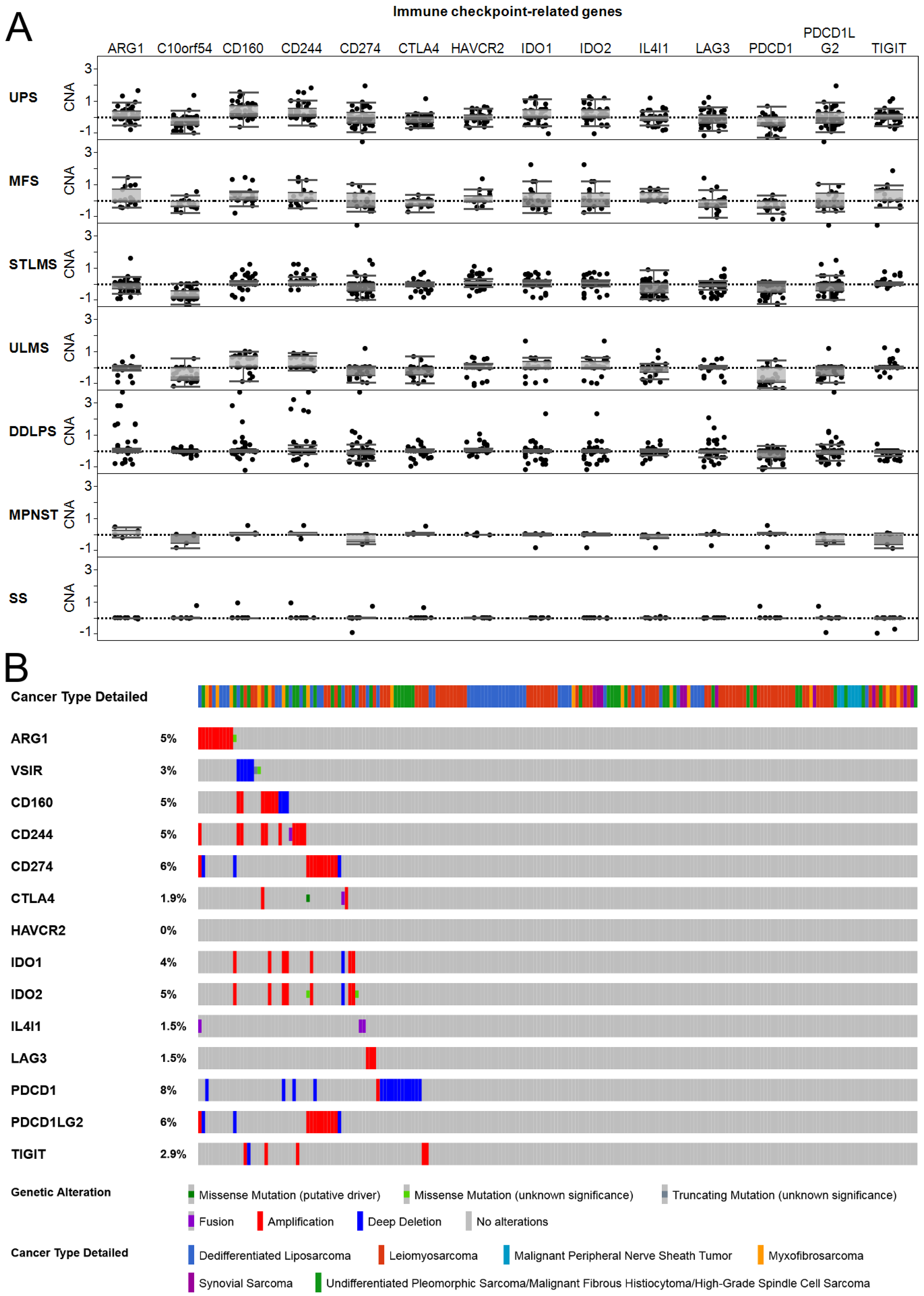
2.6. Immune Checkpoint-Related Gene Copy Number Alterations and Mutations in Soft Tissue Sarcomas
3. Discussion
4. Materials and Methods
4.1. TCGA data
4.2. Data Analysis and Visualization
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gamboa, A.C.; Gronchi, A.; Cardona, K. Soft-tissue sarcoma in adults: An update on the current state of histiotype-specific management in an era of personalized medicine. CA Cancer J. Clin. 2020, 70, 200–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roszik, J.; Wang, W.L.; Livingston, J.A.; Roland, C.L.; Ravi, V.; Yee, C.; Hwu, P.; Futreal, A.; Lazar, A.J.; Patel, S.R.; et al. Overexpressed PRAME is a potential immunotherapy target in sarcoma subtypes. Clin. Sarcoma Res. 2017, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conley, A.P.; Wang, W.L.; Livingston, J.A.; Ravi, V.; Tsai, J.W.; Ali, A.; Ingram, D.R.; Lowery, C.D.; Roland, C.L.; Somaiah, N.; et al. MAGE-A3 is a Clinically Relevant Target in Undifferentiated Pleomorphic Sarcoma/Myxofibrosarcoma. Cancers 2019, 11, 677. [Google Scholar] [CrossRef] [Green Version]
- Roszik, J.; Khan, A.; Conley, A.P.; Livingston, J.A.; Groisberg, R.; Ravi, V.; Carmagnani Pestana, R.; Sen, S.; Subbiah, V. Unique Aberrations in Intimal Sarcoma Identified by Next-Generation Sequencing as Potential Therapy Targets. Cancers 2019, 11, 1283. [Google Scholar] [CrossRef] [Green Version]
- Birdi, H.K.; Jirovec, A.; Cortes-Kaplan, S.; Werier, J.; Nessim, C.; Diallo, J.S.; Ardolino, M. Immunotherapy for sarcomas: New frontiers and unveiled opportunities. J. Immunother. Cancer 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Ayodele, O.; Razak, A.R.A. Immunotherapy in soft-tissue sarcoma. Curr. Oncol. 2020, 27, 17–23. [Google Scholar] [CrossRef]
- Burgess, M.A.; Bolejack, V.; Tine, B.A.V.; Schuetze, S.; Hu, J.; D’Angelo, S.P.; Attia, S.; Priebat, D.A.; Okuno, S.H.; Riedel, R.F.; et al. Multicenter phase II study of pembrolizumab (P) in advanced soft tissue (STS) and bone sarcomas (BS): Final results of SARC028 and biomarker analyses. J. Clin. Oncol. 2017, 35, 11008. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): A multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef]
- Conley, A.P.; Trinh, V.A.; Zobniw, C.M.; Posey, K.; Martinez, J.D.; Arrieta, O.G.; Wang, W.L.; Lazar, A.J.; Somaiah, N.; Roszik, J.; et al. Positive Tumor Response to Combined Checkpoint Inhibitors in a Patient with Refractory Alveolar Soft Part Sarcoma: A Case Report. J. Glob. Oncol. 2018, 4, 1–6. [Google Scholar] [CrossRef]
- Dancsok, A.R.; Setsu, N.; Gao, D.; Blay, J.Y.; Thomas, D.; Maki, R.G.; Nielsen, T.O.; Demicco, E.G. Expression of lymphocyte immunoregulatory biomarkers in bone and soft-tissue sarcomas. Mod. Pathol. 2019, 32, 1772–1785. [Google Scholar] [CrossRef]
- Pollack, S.M.; He, Q.; Yearley, J.H.; Emerson, R.; Vignali, M.; Zhang, Y.; Redman, M.W.; Baker, K.K.; Cooper, S.; Donahue, B.; et al. T-cell infiltration and clonality correlate with programmed cell death protein 1 and programmed death-ligand 1 expression in patients with soft tissue sarcomas. Cancer 2017, 123, 3291–3304. [Google Scholar] [CrossRef] [Green Version]
- Cancer Genome Atlas Research Network. Comprehensive and Integrated Genomic Characterization of Adult Soft Tissue Sarcomas. Cell 2017, 171, 950–965.e28. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Fu, J.; Zeng, Z.; Cohen, D.; Li, J.; Chen, Q.; Li, B.; Liu, X.S. TIMER2.0 for analysis of tumor-infiltrating immune cells. Nucleic Acids Res. 2020, 48, W509–W514. [Google Scholar] [CrossRef]
- Kim, K.; Kim, H.S.; Kim, J.Y.; Jung, H.; Sun, J.M.; Ahn, J.S.; Ahn, M.J.; Park, K.; Lee, S.H.; Choi, J.K. Predicting clinical benefit of immunotherapy by antigenic or functional mutations affecting tumour immunogenicity. Nat. Commun. 2020, 11, 951. [Google Scholar] [CrossRef]
- Potter, J.W.; Jones, K.B.; Barrott, J.J. Sarcoma-The standard-bearer in cancer discovery. Crit. Rev. Oncol. Hematol. 2018, 126, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Klempner, S.J.; Fabrizio, D.; Bane, S.; Reinhart, M.; Peoples, T.; Ali, S.M.; Sokol, E.S.; Frampton, G.; Schrock, A.B.; Anhorn, R.; et al. Tumor Mutational Burden as a Predictive Biomarker for Response to Immune Checkpoint Inhibitors: A Review of Current Evidence. Oncologist 2020, 25, e147–e159. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, S.P.; Shoushtari, A.N.; Agaram, N.P.; Kuk, D.; Qin, L.X.; Carvajal, R.D.; Dickson, M.A.; Gounder, M.; Keohan, M.L.; Schwartz, G.K.; et al. Prevalence of tumor-infiltrating lymphocytes and PD-L1 expression in the soft tissue sarcoma microenvironment. Hum. Pathol. 2015, 46, 357–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komohara, Y.; Takeya, H.; Wakigami, N.; Kusada, N.; Bekki, H.; Ishihara, S.; Takeya, M.; Nakashima, Y.; Oda, Y. Positive correlation between the density of macrophages and T-cells in undifferentiated sarcoma. Med. Mol. Morphol. 2019, 52, 44–51. [Google Scholar] [CrossRef]
- Sousa, L.M.; Almeida, J.S.; Fortes-Andrade, T.; Santos-Rosa, M.; Freitas-Tavares, P.; Casanova, J.M.; Rodrigues-Santos, P. Tumor and Peripheral Immune Status in Soft Tissue Sarcoma: Implications for Immunotherapy. Cancers 2021, 13, 3885. [Google Scholar] [CrossRef]
- Davoli, T.; Uno, H.; Wooten, E.C.; Elledge, S.J. Tumor aneuploidy correlates with markers of immune evasion and with reduced response to immunotherapy. Science 2017, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, A.M.; Shih, J.; Ha, G.; Gao, G.F.; Zhang, X.; Berger, A.C.; Schumacher, S.E.; Wang, C.; Hu, H.; Liu, J.; et al. Genomic and Functional Approaches to Understanding Cancer Aneuploidy. Cancer Cell 2018, 33, 676–689.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekmekcioglu, S.; Grimm, E.A.; Roszik, J. Targeting iNOS to increase efficacy of immunotherapies. Hum. Vaccines Immunother. 2017, 13, 1105–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miwa, S.; Nojima, T.; Alomesen, A.A.; Ikeda, H.; Yamamoto, N.; Nishida, H.; Hayashi, K.; Takeuchi, A.; Igarashi, K.; Higuchi, T.; et al. Associations of PD-L1, PD-L2, and HLA class I expression with responses to immunotherapy in patients with advanced sarcoma: Post hoc analysis of a phase 1/2 trial. Clin. Transl. Oncol. 2021, 23, 1620–1629. [Google Scholar] [CrossRef] [PubMed]
- Steggerda, S.M.; Bennett, M.K.; Chen, J.; Emberley, E.; Huang, T.; Janes, J.R.; Li, W.; MacKinnon, A.L.; Makkouk, A.; Marguier, G.; et al. Inhibition of arginase by CB-1158 blocks myeloid cell-mediated immune suppression in the tumor microenvironment. J. Immunother. Cancer 2017, 5, 101. [Google Scholar] [CrossRef] [PubMed]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [Green Version]
- Budczies, J.; Mechtersheimer, G.; Denkert, C.; Klauschen, F.; Mughal, S.S.; Chudasama, P.; Bockmayr, M.; Johrens, K.; Endris, V.; Lier, A.; et al. PD-L1 (CD274) copy number gain, expression, and immune cell infiltration as candidate predictors for response to immune checkpoint inhibitors in soft-tissue sarcoma. Oncoimmunology 2017, 6, e1279777. [Google Scholar] [CrossRef] [Green Version]
- Strickler, J.H.; Hanks, B.A.; Khasraw, M. Tumor Mutational Burden as a Predictor of Immunotherapy Response: Is More Always Better? Clin. Cancer Res. 2021, 27, 1236–1241. [Google Scholar] [CrossRef]
- Grunewald, T.G.; Alonso, M.; Avnet, S.; Banito, A.; Burdach, S.; Cidre-Aranaz, F.; Di Pompo, G.; Distel, M.; Dorado-Garcia, H.; Garcia-Castro, J.; et al. Sarcoma treatment in the era of molecular medicine. EMBO Mol. Med. 2020, 12, e11131. [Google Scholar] [CrossRef] [PubMed]
- Linch, M.; Miah, A.B.; Thway, K.; Judson, I.R.; Benson, C. Systemic treatment of soft-tissue sarcoma-gold standard and novel therapies. Nat. Rev. Clin. Oncol. 2014, 11, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Klaver, Y.; Rijnders, M.; Oostvogels, A.; Wijers, R.; Smid, M.; Grunhagen, D.; Verhoef, C.; Sleijfer, S.; Lamers, C.; Debets, R. Differential quantities of immune checkpoint-expressing CD8 T cells in soft tissue sarcoma subtypes. J. Immunother. Cancer 2020, 8. [Google Scholar] [CrossRef]
- Burgess, M.A.; Roszik, J.; Tine, B.A.V.; Hu, J.; Schuetze, S.; D’Angelo, S.P.; Attia, S.; Priebat, D.A.; Okuno, S.H.; Riedel, R.F.; et al. Correlation of circulating PD-L2 levels with outcomes of therapy with the anti-PD-1 antibody pembrolizumab (P) in patients (pts) with advanced soft tissue sarcomas (STS): Biomarker analysis of SARC028. J. Clin. Oncol. 2017, 35, 60. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| STS Subtype | Karyotype | Mutation Load | Immune Infiltrate | Immune-Related Markers |
|---|---|---|---|---|
| UPS | complex | high | CD8+ T cells; macrophages | PD-L2; PD-L1 |
| MFS | complex | high | CD8+ T cells; macrophages | PD-L2; PD-L1 |
| STLMS | complex | high | CD8+ T cells; macrophages | PD-L2; PD-L1; TIM-3; IL4I1 |
| ULMS | complex | high | CD8+ T cells; macrophages | PD-L2; PD-L1; TIM-3; IL4I1 |
| DDLPS | complex | high | CD8+ T cells; macrophages | PD-L2; PD-L1 |
| MPNST | complex | low | CD8+ T cells; macrophages | PD-L1 |
| SS | simple | low | CD8+ T cells; macrophages |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roszik, J.; Mustachio, L.M.; Livingston, J.A.; Groisberg, R.; Carmagnani Pestana, R.; Subbiah, V.; Conley, A.P. Landscape of Immune-Related Markers and Potential Therapeutic Targets in Soft Tissue Sarcoma. Cancers 2021, 13, 5249. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205249
Roszik J, Mustachio LM, Livingston JA, Groisberg R, Carmagnani Pestana R, Subbiah V, Conley AP. Landscape of Immune-Related Markers and Potential Therapeutic Targets in Soft Tissue Sarcoma. Cancers. 2021; 13(20):5249. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205249
Chicago/Turabian StyleRoszik, Jason, Lisa Maria Mustachio, John A. Livingston, Roman Groisberg, Roberto Carmagnani Pestana, Vivek Subbiah, and Anthony P. Conley. 2021. "Landscape of Immune-Related Markers and Potential Therapeutic Targets in Soft Tissue Sarcoma" Cancers 13, no. 20: 5249. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205249