
Can the Six-Minute Walk Test Be Used to Individualize Physical Activity Intensity in Patients with Breast Cancer?

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
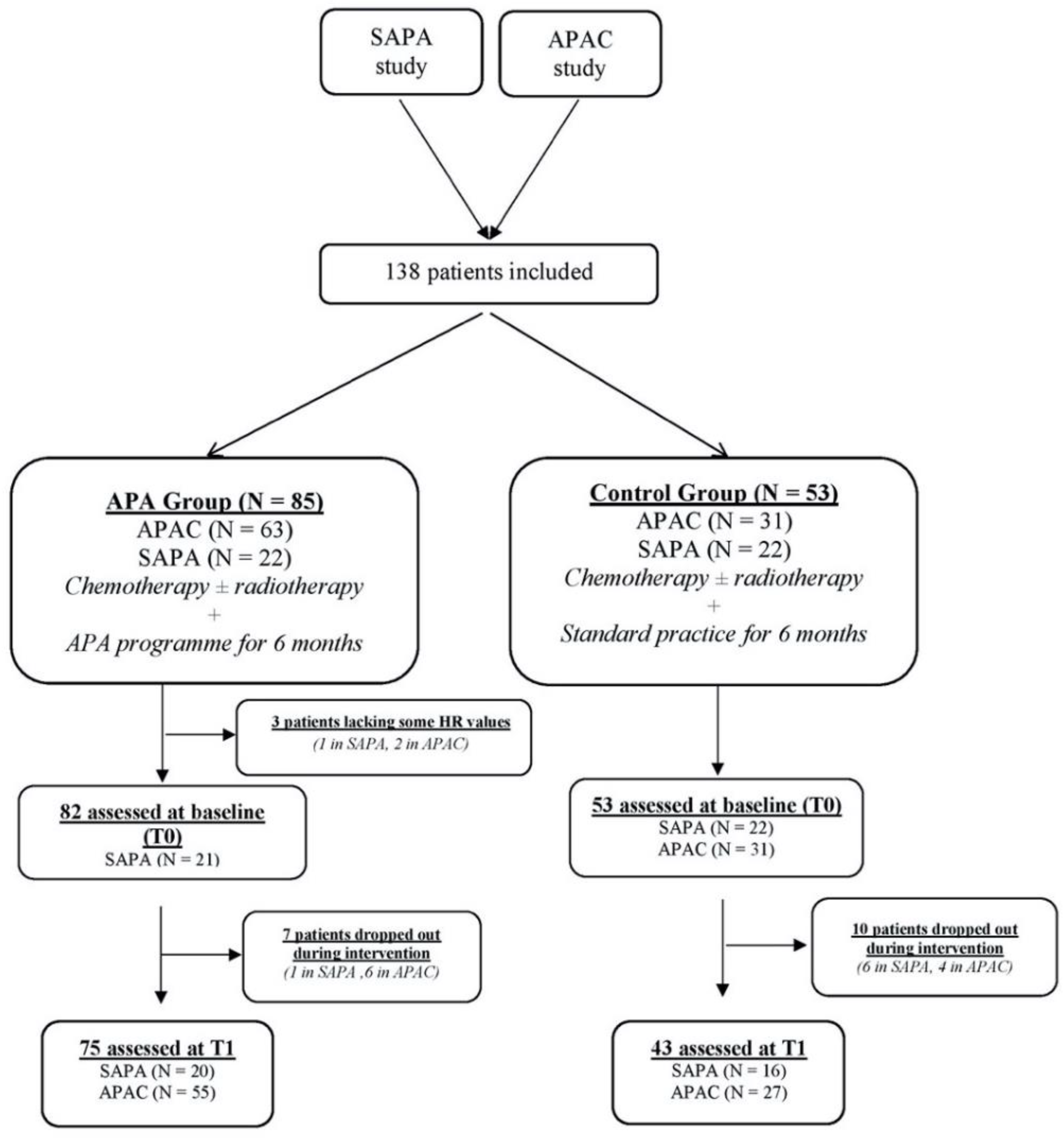
2.1. Setting and Participants
2.2. Study Design
- Group A performed 6-month home-based APA during adjuvant therapy.
- Group B received conventional management during adjuvant therapy.
- Group A performed 6-month home-based APA during adjuvant or neoadjuvant therapy.
- Group B performed 6-month home-based APA after adjuvant or neoadjuvant therapy.
- Group C performed 12-month home-based APA during and after adjuvant or neoadjuvant therapy.
2.3. Study Outcomes
2.4. The Tests Used in the SAPA and APAC Trials
2.4.1. Cardiopulmonary Exercise Test
2.4.2. Six-Minute Walk Test
2.4.3. Body Composition
2.5. Exercise Training
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics at Baseline
3.2. HR at Baseline
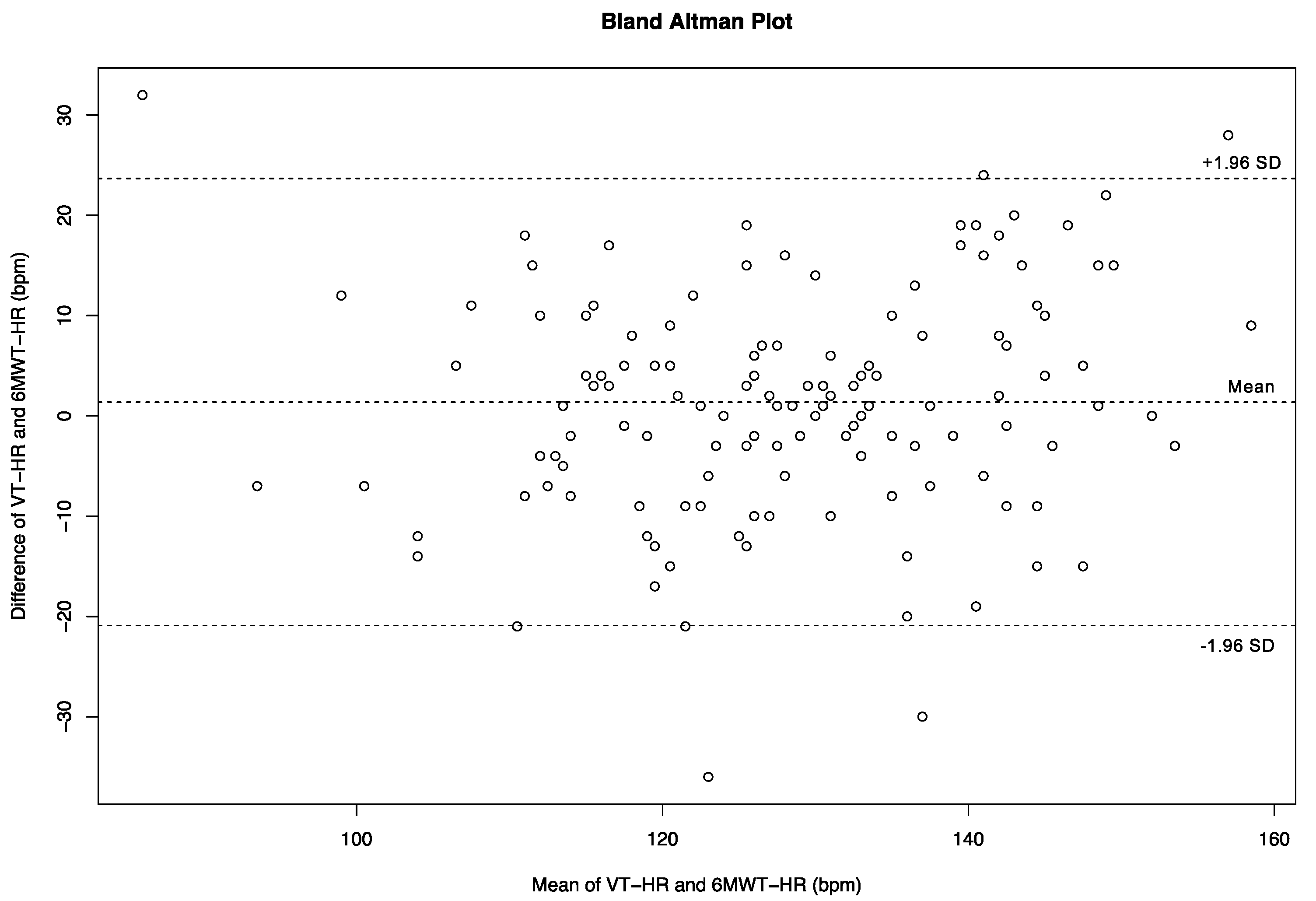
3.3. Relationship between the 6MWT-HR and VT-HR at Baseline
3.4. Impact of APA during Adjuvant Treatment on the 6MWT-HR and VT-HR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Visovsky, C. Muscle strength, body composition, and physical activity in women receiving chemotherapy for breast cancer. Integr. Cancer Ther. 2006, 5, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Klassen, O.; Schmidt, M.E.; Scharhag-Rosenberger, F.; Sorkin, M.; Ulrich, C.M.; Schneeweiss, A.; Potthoff, K.; Steindorf, K.; Wiskemann, J. Cardiorespiratory fitness in breast cancer patients undergoing adjuvant therapy. Acta Oncol. 2014, 53, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Bergh, J.; Jonsson, P.E.; Glimelius, B.; Nygren, P.; SBU-group. Swedish Council of Technology Assessment in Health Care: A systematic overview of chemotherapy effects in breast cancer. Acta Oncol. 2001, 40, 253–281. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.L. Physical activity interventions for cancer survivors. Br. J. Sports Med. 2009, 43, 32–38. [Google Scholar] [CrossRef]
- Courneya, K.S.; Karvinen, K.H. Exercise Motivation VJK. Behavior Change; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Schneider, C.M.; Hsieh, C.C.; Sprod, L.K.; Carter, S.D.; Hayward, R. Effects of supervised exercise training on cardiopulmonary function and fatigue in breast cancer survivors during and after treatment. Cancer 2007, 110, 918–925. [Google Scholar] [CrossRef]
- Witlox, L.; Velthuis, M.J.; Boer, J.H.; Steins Bisschop, C.N.; Wall, E.V.; Meulen, W.; Schroder, C.D.; Peeters, P.H.M.; May, A.M. Attendance and compliance with an exercise program during localized breast cancer treatment in a randomized controlled trial: The PACT study. PLoS ONE 2019, 14, e0215517. [Google Scholar] [CrossRef]
- Segal, R.; Evans, W.; Johnson, D.; Smith, J.; Colletta, S.; Gayton, J.; Woodard, S.; Wells, G.; Reid, R. Structured exercise improves physical functioning in women with stages I and II breast cancer: Results of a randomized controlled trial. J. Clin. Oncol. 2001, 19, 657–665. [Google Scholar] [CrossRef]
- Courneya, K.S.; Mackey, J.R.; Bell, G.J.; Jones, L.W.; Field, C.J.; Fairey, A.S. Randomized controlled trial of exercise training in postmenopausal breast cancer survivors: Cardiopulmonary and quality of life outcomes. J. Clin. Oncol. 2003, 21, 1660–1668. [Google Scholar] [CrossRef]
- van Waart, H.; Buffart, L.M.; Stuiver, M.M.; van Harten, W.H.; Sonke, G.S.; Aaronson, N.K. Adherence to and satisfaction with low-intensity physical activity and supervised moderate-high intensity exercise during chemotherapy for breast cancer. Supportive Care Cancer 2020, 28, 2115–2126. [Google Scholar] [CrossRef]
- Cornette, T.; Vincent, F.; Mandigout, S.; Antonini, M.T.; Leobon, S.; Labrunie, A.; Venat, L.; Lavau-Denes, S.; Tubiana-Mathieu, N. Effects of home-based exercise training on VO2 in breast cancer patients under adjuvant or neoadjuvant chemotherapy (SAPA): A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2016, 52, 223–232. [Google Scholar]
- Zhao, M.; Veeranki, S.P.; Magnussen, C.G.; Xi, B. Recommended physical activity and all cause and cause specific mortality in US adults: Prospective cohort study. BMJ 2020, 370. [Google Scholar] [CrossRef]
- Fletcher, G.F. How to implement physical activity in primary and secondary prevention. A statement for healthcare-professionals from the Task Force on Risk-reduction, American Heart Association. Circulation 1997, 96, 355–357. [Google Scholar] [CrossRef]
- McConnell, T.R.; Clark, B.A., III; Conlin, N.C.; Haas, J.H. Gas Exchange Anaerobic Threshold: Implications for Prescribing Exercise in Cardiac Rehabilitation. J. Cardiopulm. Rehabil. 1993, 13, 31–36. [Google Scholar] [CrossRef]
- Brun, J.F.; Bordenave, S.; Mercier, J.; Jaussent, A.; Picot, M.C.; Prefaut, C. Cost-sparing effect of twice-weekly targeted endurance training in type 2 diabetics: A one-year controlled randomized trial. Diabetes Metab. 2008, 34, 258–265. [Google Scholar] [CrossRef]
- Besnier, F.; Laruelle, E.; Genestier, S.; Gie, S.; Vigneau, C.; Carre, F. Effects of exercise training on ergocycle during hemodialysis in patients with end stage renal disease: Relevance of the anaerobic threshold intensity. Nephrol. Ther. 2012, 8, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef]
- Solway, S.; Brooks, D.; Lacasse, Y.; Thomas, S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest 2001, 119, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Gayda, M.; Temfemo, A.; Choquet, D.; Ahmaidi, S. Cardiorespiratory requirements and reproducibility of the six-minute walk test in elderly patients with coronary artery disease. Arch. Phys. Med. Rehabil. 2004, 85, 1538–1543. [Google Scholar] [CrossRef]
- Gremeaux, M.; Hannequin, A.; Laurent, Y.; Laroche, D.; Casillas, J.M.; Gremeaux, V. Usefulness of the 6-minute walk test and the 200-metre fast walk test to individualize high intensity interval and continuous exercise training in coronary artery disease patients after acute coronary syndrome: A pilot controlled clinical study. Clin. Rehabil. 2011, 25, 844–855. [Google Scholar] [CrossRef]
- Kervio, G.; Carre, F.; Ville, N.S. Reliability and intensity of the six-minute walk test in healthy elderly subjects. Med. Sci. Sports Exerc. 2003, 35, 169–174. [Google Scholar] [CrossRef]
- Haykowsky, M.J.; Beaudry, R.; Brothers, R.M.; Nelson, M.D.; Sarma, S.; La Gerche, A. Pathophysiology of exercise intolerance in breast cancer survivors with preserved left ventricular ejection fraction. Clin. Sci. 2016, 130, 2239–2244. [Google Scholar] [CrossRef]
- Vincent, F.; Deluche, E.; Bonis, J.; Leobon, S.; Antonini, M.T.; Laval, C.; Favard, F.; Dobbels, E.; Lavau-Denes, S.; Labrunie, A.; et al. Home-Based Physical Activity in Patients with Breast Cancer: During and/or after Chemotherapy? Impact on Cardiorespiratory Fitness. A 3-Arm Randomized Controlled Trial (APAC). Integr. Cancer Ther. 2020, 19, 1534735420969818. [Google Scholar] [CrossRef]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDonald, A.; Russi, G.D.; Moudgil, V.K. Longitudinal modeling of the relationship between age and maximal heart rate. Med. Sci. Sports Exerc. 2007, 39, 822–829. [Google Scholar] [CrossRef]
- Jones, L.W.; Eves, N.D.; Haykowsky, M.; Joy, A.A.; Douglas, P.S. Cardiorespiratory exercise testing in clinical oncology research: Systematic review and practice recommendations. Lancet Oncol. 2008, 9, 757–765. [Google Scholar] [CrossRef]
- Wasserman, K.H.; James, E.; Sue Daryl, Y.; Whipp Brian, J.; Froelicher Victor, F. Principles of Exercise Testing and Interpretation. J. Cardiopulm. Rehabil. 1987, 7, 189. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Sullivan, M.J.; Thompson, P.J.; Fallen, E.L.; Pugsley, S.O.; Taylor, D.W.; Berman, L.B. The 6-minute walk: A new measure of exercise capacity in patients with chronic heart failure. Can. Med. Assoc. J. 1985, 132, 919–923. [Google Scholar]
- Reis, A.D.; Pereira, P.; Diniz, R.R.; de Castro Filha, J.G.L.; Dos Santos, A.M.; Ramallo, B.T.; Filho, F.A.A.; Navarro, F.; Garcia, J.B.S. Effect of exercise on pain and functional capacity in breast cancer patients. Health Qual. Life Outcomes 2018, 16, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity for women with breast cancer after adjuvant therapy. Cochrane Database Syst. Rev. 2018, 1, CD011292. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.L.; Cartmel, B.; Gross, C.P.; Ercolano, E.; Li, F.; Yao, X.; Fiellin, M.; Capozza, S.; Rothbard, M.; Zhou, Y.; et al. Randomized exercise trial of aromatase inhibitor-induced arthralgia in breast cancer survivors. J. Clin. Oncol. 2015, 33, 1104–1111. [Google Scholar] [CrossRef]
- Daley, A.J.; Crank, H.; Saxton, J.M.; Mutrie, N.; Coleman, R.; Roalfe, A. Randomized trial of exercise therapy in women treated for breast cancer. J. Clin. Oncol. 2007, 25, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Cadmus, L.A.; Salovey, P.; Yu, H.; Chung, G.; Kasl, S.; Irwin, M.L. Exercise and quality of life during and after treatment for breast cancer: Results of two randomized controlled trials. Psychooncology 2009, 18, 343–352. [Google Scholar] [CrossRef]
- Do, J.; Cho, Y.; Jeon, J. Effects of a 4-week multimodal rehabilitation program on quality of life, cardiopulmonary function, and fatigue in breast cancer patients. J. Breast Cancer 2015, 18, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolan, L.B.; Campbell, K.; Gelmon, K.; Neil-Sztramko, S.; Holmes, D.; McKenzie, D.C. Interval versus continuous aerobic exercise training in breast cancer survivors—A pilot RCT. Supportive Care Cancer 2016, 24, 119–127. [Google Scholar] [CrossRef]
- Bhatia, C.; Kayser, B. Preoperative high-intensity interval training is effective and safe in deconditioned patients with lung cancer: A randomized clinical trial. J. Rehabil. Med. 2019, 51, 712–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morard, M.D.; Bosquet, L.; Laroche, D.; Joussain, C.; Besson, D.; Deley, G.; Casillas, J.M.; Gremeaux, V. Are first ventilatory threshold and 6-minute walk test heart rate interchangeable? A pilot study in healthy elderlies and cardiac patients. Ann. Phys. Rehabil. Med. 2015, 58, 92–97. [Google Scholar] [CrossRef]
- Kervio, G.; Ville, N.S.; Leclercq, C.; Daubert, J.C.; Carre, F. Intensity and daily reliability of the six-minute walk test in moderate chronic heart failure patients. Arch. Phys. Med. Rehabil. 2004, 85, 1513–1518. [Google Scholar] [CrossRef]
- Irwin, M.L.; McTiernan, A.; Manson, J.E.; Thomson, C.A.; Sternfeld, B.; Stefanick, M.L.; Wactawski-Wende, J.; Craft, L.; Lane, D.; Martin, L.W.; et al. Physical activity and survival in postmenopausal women with breast cancer: Results from the women’s health initiative. Cancer Prev. Res. 2011, 4, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Sternfeld, B.; Weltzien, E.; Quesenberry, C.P., Jr.; Castillo, A.L.; Kwan, M.; Slattery, M.L.; Caan, B.J. Physical activity and risk of recurrence and mortality in breast cancer survivors: Findings from the LACE study. Cancer Epidemiol. Biomark. Prev. 2009, 18, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Patient Characteristics |
All Patients (N = 138) |
APA Group
(N = 85) |
Control Group
(N = 53) |
|---|---|---|---|
| Age (years), median (min–max) | 52 (29–74) | 51 (29–74) | 50 (37–72) |
| BMI (kg/m²), mean ± SD | 25.6 ± 4.8 | 25.4 ± 5.2 | 25.8 ± 4.2 |
| BMI (kg/m²), n (%) | |||
| Thin (<18.5) | 3 (2.2) | 3 (3.5) | 3 (2.2) |
| Normal (≥18.5, <25) | 70 (50.7) | 44 (51.8) | 70 (50.7) |
| Overweight (≥25, <30) | 46 (33.3) | 27 (31.8) | 46 (33.3) |
| Obese (≥30) | 19 (13.8) | 11 (12.9) | 19 (13.8) |
| Cancer stage, n (%) | |||
| I | 23 (16.8) | 19 (22.6) | 23 (16.8) |
| II | 97 (70.8) | 54 (64.3) | 97 (70.8) |
| III | 17 (12.4) | 11 (13.1) | 17 (12.4) |
| Bilateral, n (%) | 6 (4.5) | 4 (4.8) | 2 (4.0) |
| Mastectomy, n (%) | 40 (29.9) | 25 (29.8) | 15 (30.0) |
| Lumpectomy, n (%) | 95 (70.9) | 60 (71.4) | 35 (70.0) |
| Axillary dissection, n (%) | 70 (51.1) | 42 (49.4) | 28 (53.8) |
| Comorbidities, n (%) | 22 (15.9) | 13 (15.3) | 9 (17.0) |
| Hypertension | 19 (13.8) | 12 (14.1) | 7 (13.2) |
| Stroke | 2 (1.5) | 0 (0) | 2 (3.7) |
| Phlebitis | 2 (1.5) | 1 (1.2) | 1 (1.9) |
| Hemoglobin (g/L), mean ± SD | 12.8 ± 0.8 | 12.7 ± 0.9 | 13.3 ± 0.4 |
| Tests Characteristics | No. of Patients | Mean | SD | Range |
|---|---|---|---|---|
| 6MWT | ||||
| 6MWT-HR (bpm) | 137 | 129.3 | 15.5 | 90.0–171.0 |
| CPET | ||||
| VT-HR (bpm) | 136 | 127.8 | 14.0 | 70.0–162.0 |
| HRpeak (bpm) | 137 | 154.1 | 15.7 | 107.0–187.0 |
| Calculated variables | ||||
| Predicted HRmax (bpm) | 138 | 172.0 | 8.0 | 153.2–185.6 |
| % VT-HR/predicted HRmax | 136 | 74.3 | 7.6 | 40.7–95.5 |
| % 6MWT-HR/predicted HRmax | 137 | 75.2 | 8.5 | 57.2–97.3 |
| % VT-HR/HRpeak | 136 | 83.2 | 6.4 | 47.0–107.3 |
| % 6MWT-HR/HRpeak | 136 | 84.3 | 8.6 | 64.4–111.9 |
| Tests Characteristics | r | IC0.95 | p-Value |
|---|---|---|---|
| 6MWT-HR vs. age | −0.37 | (−0.50, −0.21) | <0.001 |
| 6MWT-HR vs. BMI | −0.12 | (−0.28, −0.05) | 0.170 |
| VT-HR vs. age | −0.38 | (−0.52, −0.23) | <0.001 |
| VT-HR vs. BMI | −0.12 | (−0.29, 0.04) | 0.149 |
| 6MWT-HR vs. VT-HR | 0.70 | (0.60, 0.77) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tubiana-Mathieu, N.; Cornette, T.; Mandigout, S.; Leobon, S.; Vincent, F.; Venat, L.; Deluche, E. Can the Six-Minute Walk Test Be Used to Individualize Physical Activity Intensity in Patients with Breast Cancer? Cancers 2021, 13, 5851. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225851
Tubiana-Mathieu N, Cornette T, Mandigout S, Leobon S, Vincent F, Venat L, Deluche E. Can the Six-Minute Walk Test Be Used to Individualize Physical Activity Intensity in Patients with Breast Cancer? Cancers. 2021; 13(22):5851. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225851
Chicago/Turabian StyleTubiana-Mathieu, Nicole, Thibault Cornette, Stephane Mandigout, Sophie Leobon, François Vincent, Laurence Venat, and Elise Deluche. 2021. "Can the Six-Minute Walk Test Be Used to Individualize Physical Activity Intensity in Patients with Breast Cancer?" Cancers 13, no. 22: 5851. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225851