
Serum Sorbitol Dehydrogenase as a Novel Prognostic Factor for Hepatocellular Carcinoma after Surgical Resection

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Baseline Characteristics
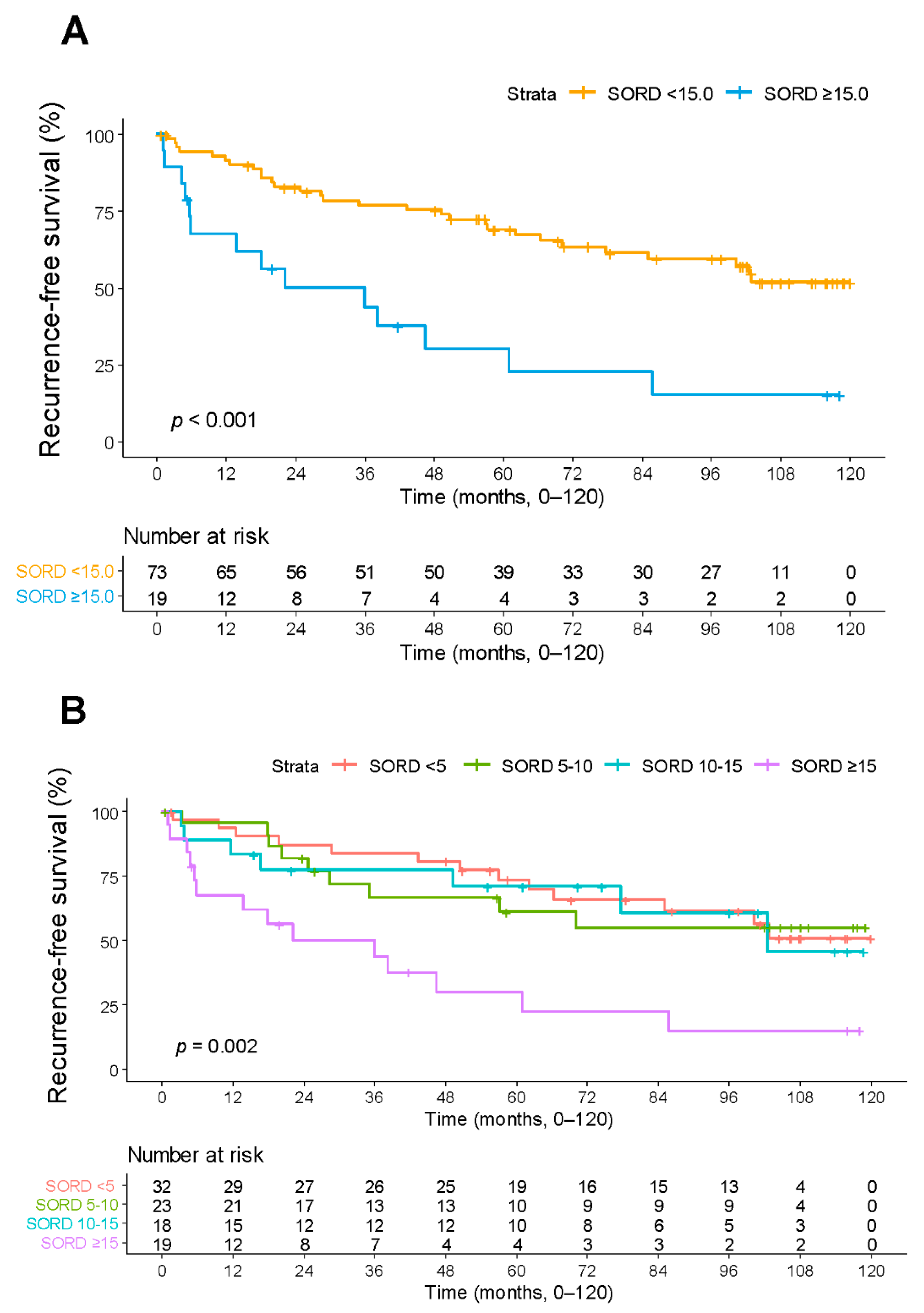
2.2. Recurrence According to SORD Level
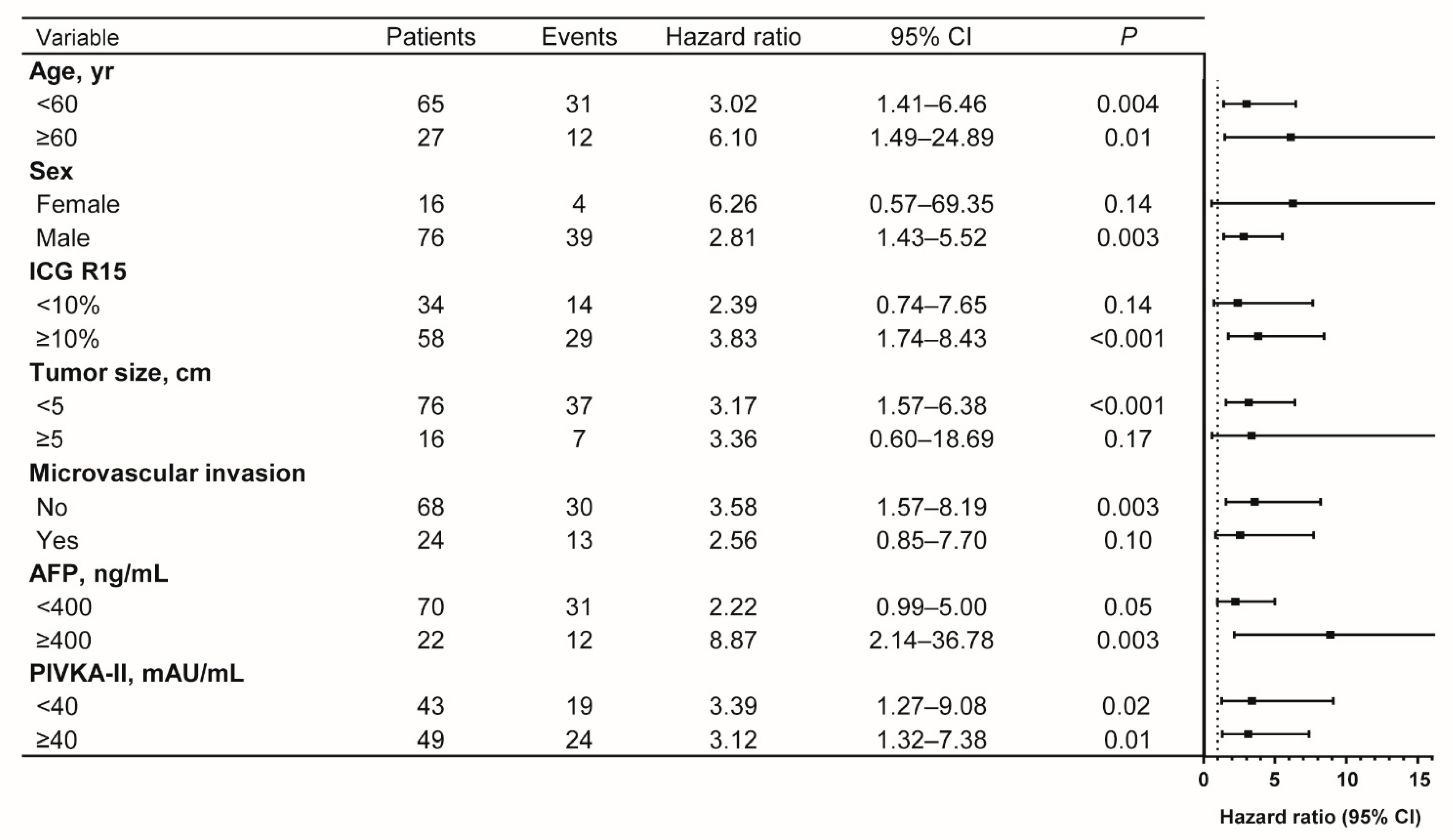
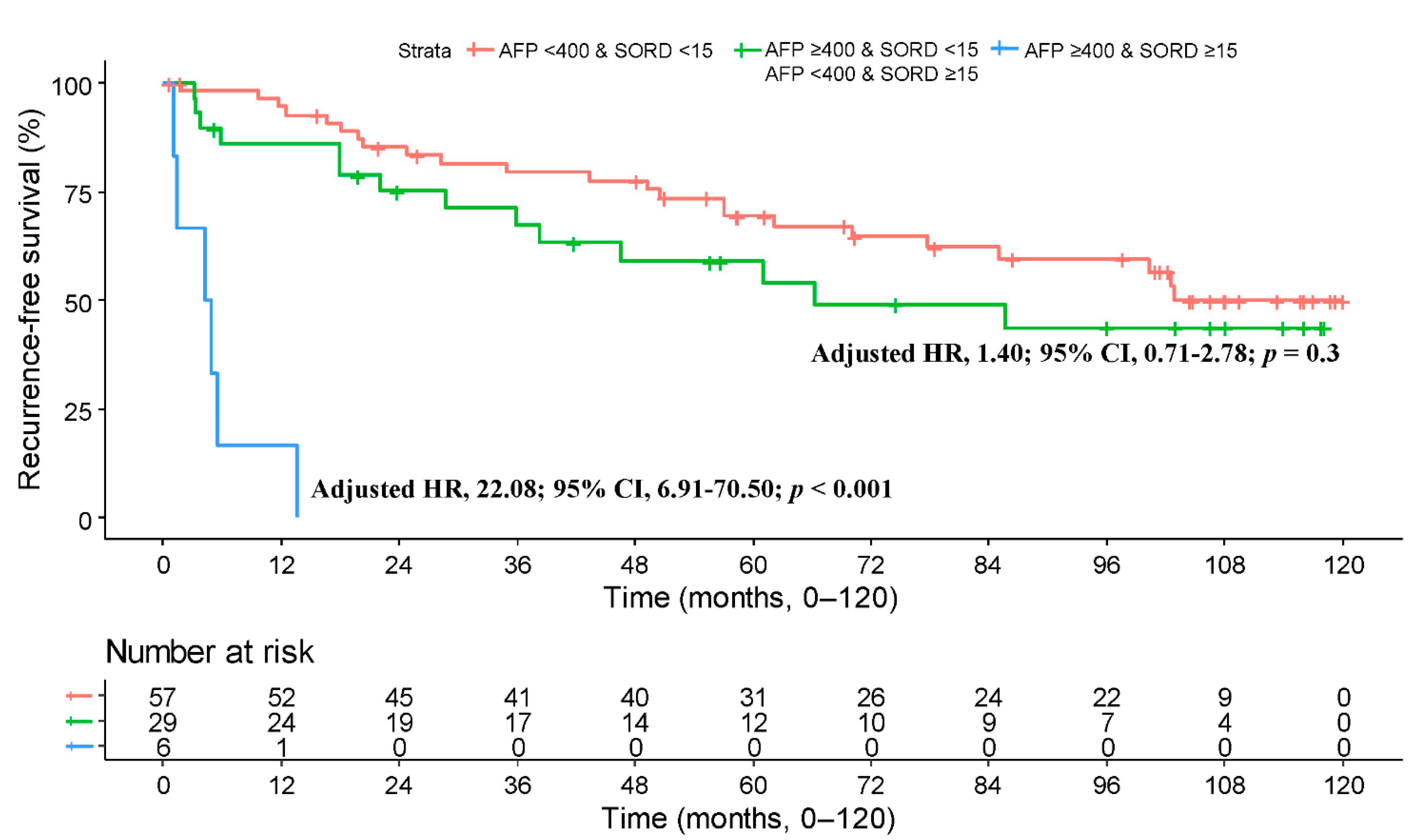
2.3. Prognostic Factors Associated with Recurrence-Free Survival
2.4. Factors Correlated with Serum SORD
3. Discussion
4. Materials and Methods
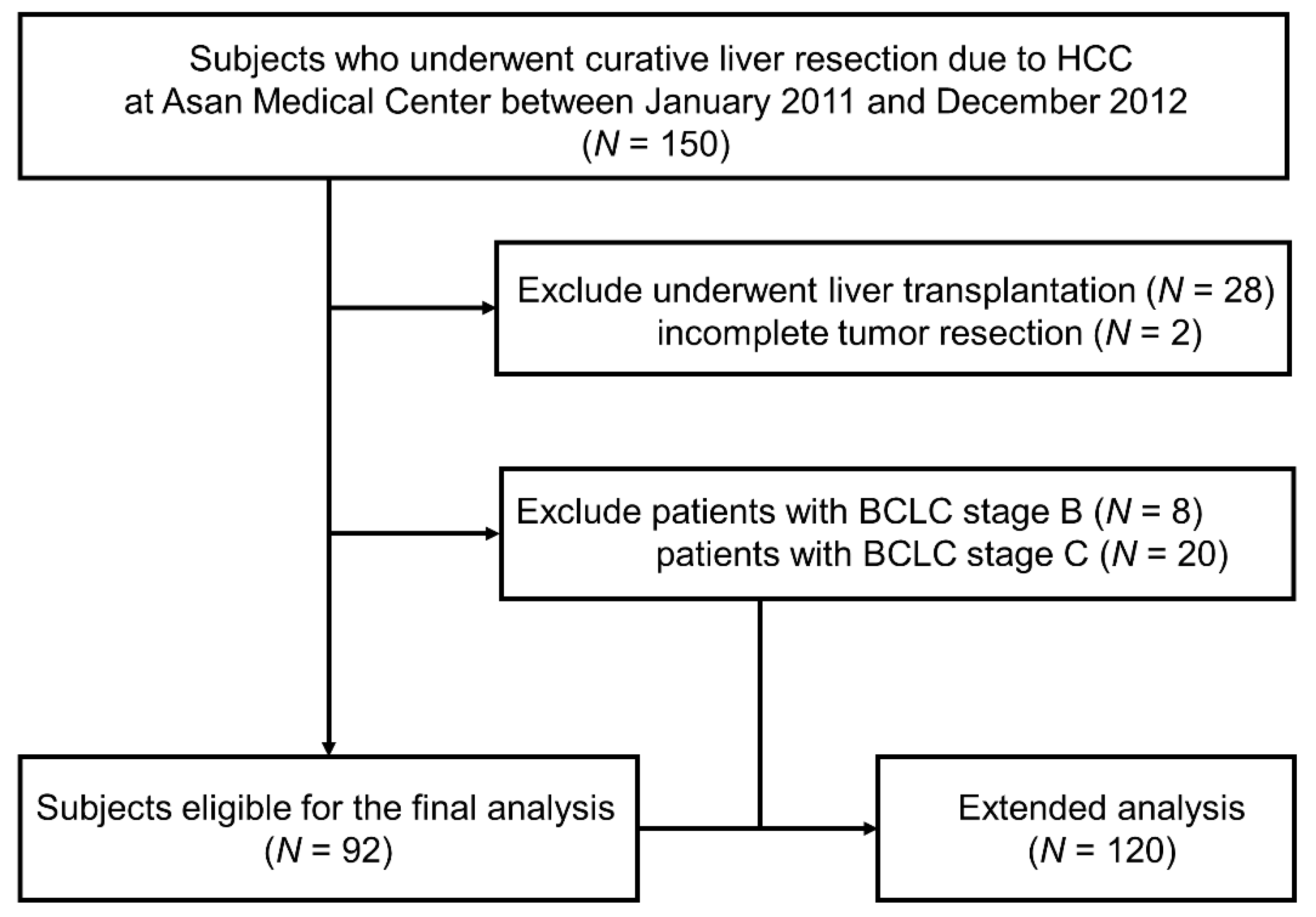
4.1. Study Design and Population
4.2. SORD Measurement
4.3. Risk Factors and Outcome
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Petrick, J.L.; Florio, A.A.; Znaor, A.; Ruggieri, D.; Laversanne, M.; Alvarez, C.S.; Ferlay, J.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in hepatocellular carcinoma incidence, 1978–2012. Int. J. Cancer 2020, 147, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Roayaie, S.; Obeidat, K.; Sposito, C.; Mariani, L.; Bhoori, S.; Pellegrinelli, A.; Labow, D.; Llovet, J.M.; Schwartz, M.; Mazzaferro, V. Resection of hepatocellular cancer ≤2 cm: Results from two Western centers. Hepatology 2013, 57, 1426–1435. [Google Scholar] [CrossRef]
- Tabrizian, P.; Jibara, G.; Shrager, B.; Schwartz, M.; Roayaie, S. Recurrence of hepatocellular cancer after resection: Patterns, treatments, and prognosis. Ann. Surg. 2015, 261, 947–955. [Google Scholar] [CrossRef]
- Lin, C.-W.; Chen, Y.-S.; Lin, C.-C.; Lee, P.-H.; Lo, G.-H.; Hsu, C.-C.; Hsieh, P.-M.; Koh, K.W.; Bair, M.-J.; Dai, C.-Y.; et al. Significant predictors of overall survival in patients with hepatocellular carcinoma after surgical resection. PLoS ONE 2018, 13, e0202650. [Google Scholar] [CrossRef]
- Rodríguez-Perálvarez, M.; Luong, T.V.; Andreana, L.; Meyer, T.; Dhillon, A.P.; Burroughs, A.K. A systematic review of microvascular invasion in hepatocellular carcinoma: Diagnostic and prognostic variability. Ann. Surg. Oncol. 2013, 20, 325–339. [Google Scholar] [CrossRef]
- Roayaie, S.; Blume, I.N.; Thung, S.N.; Guido, M.; Fiel, M.-I.; Hiotis, S.; Labow, D.M.; Llovet, J.M.; Schwartz, M.E. A system of classifying microvascular invasion to predict outcome after resection in patients with hepatocellular carcinoma. Gastroenterology 2009, 137, 850–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, K.-C.; Chow, P.K.-H.; Allen, J.C.; Chia, G.-S.; Lim, M.; Cheow, P.-C.; Chung, A.Y.; Ooi, L.L.; Tan, S.-B. Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria. Ann. Surg. 2011, 254, 108–113. [Google Scholar] [CrossRef]
- Han, J.H.; Kim, D.G.; Na, G.H.; Kim, E.Y.; Lee, S.H.; Hong, T.H.; You, Y.K. Evaluation of prognostic factors on recurrence after curative resections for hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 17132–17140. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Moris, D.; Hyer, J.M.; Bagante, F.; Ratti, F.; Marques, H.P.; Soubrane, O.; Lam, V.; Poultsides, G.A.; Popescu, I.; et al. Serum α-Fetoprotein Levels at Time of Recurrence Predict Post-Recurrence Outcomes Following Resection of Hepatocellular Carcinoma. Ann. Surg. Oncol. 2021, 28, 7673–7683. [Google Scholar] [CrossRef]
- Chan, M.Y.; She, W.H.; Dai, W.C.; Tsang, S.H.Y.; Chok, K.S.H.; Chan, A.C.Y.; Fung, J.; Lo, C.M.; Cheung, T.T. Prognostic value of preoperative alpha-fetoprotein (AFP) level in patients receiving curative hepatectomy- an analysis of 1182 patients in Hong Kong. Transl. Gastroenterol. Hepatol. 2019, 4, 52. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.H.; Jun, M.J.; Han, S.; Lee, Y.J.; Lee, S.G.; Kim, K.M.; Lim, Y.S.; Lee, H.C. Prognostic nomograms for prediction of recurrence and survival after curative liver resection for hepatocellular carcinoma. Ann. Surg. 2015, 261, 939–946. [Google Scholar] [CrossRef]
- Tateishi, R.; Yoshida, H.; Matsuyama, Y.; Mine, N.; Kondo, Y.; Omata, M. Diagnostic accuracy of tumor markers for hepatocellular carcinoma: A systematic review. Hepatol. Int. 2008, 2, 17–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blank, S.; Wang, Q.; Fiel, M.I.; Luan, W.; Kim, K.W.; Kadri, H.; Mandeli, J.; Hiotis, S.P. Assessing prognostic significance of preoperative alpha-fetoprotein in hepatitis B-associated hepatocellular carcinoma: Normal is not the new normal. Ann. Surg. Oncol. 2014, 21, 986–994. [Google Scholar] [CrossRef]
- Shim, J.H.; Yoon, D.L.; Han, S.; Lee, Y.J.; Lee, S.G.; Kim, K.M.; Lim, Y.S.; Lee, H.C.; Chung, Y.H.; Lee, Y.S. Is serum alpha-fetoprotein useful for predicting recurrence and mortality specific to hepatocellular carcinoma after hepatectomy? A test based on propensity scores and competing risks analysis. Ann. Surg. Oncol. 2012, 19, 3687–3696. [Google Scholar] [CrossRef]
- Fattovich, G.; Stroffolini, T.; Zagni, I.; Donato, F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology 2004, 127, S35–S50. [Google Scholar] [CrossRef]
- Ozer, J.; Ratner, M.; Shaw, M.; Bailey, W.; Schomaker, S. The current state of serum biomarkers of hepatotoxicity. Toxicology 2008, 245, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Harrill, A.H.; Roach, J.; Fier, I.; Eaddy, J.S.; Kurtz, C.L.; Antoine, D.J.; Spencer, D.M.; Kishimoto, T.K.; Pisetsky, D.S.; Park, B.K.; et al. The effects of heparins on the liver: Application of mechanistic serum biomarkers in a randomized study in healthy volunteers. Clin. Pharm. 2012, 92, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.; Wu, D.; Jiang, W.; Li, J.; Long, J.; Jia, C.; Zhou, T. Molecular Biomarkers in Drug-Induced Liver Injury: Challenges and Future Perspectives. Front. Pharm. 2020, 10, 1667. [Google Scholar] [CrossRef] [Green Version]
- Aulbach, A.D.; Amuzie, C.J. Chapter 17-Biomarkers in Nonclinical Drug Development. In A Comprehensive Guide to Toxicology in Nonclinical Drug Development, 2nd ed.; Faqi, A.S., Ed.; Academic Press: Cambridge, MA, USA, 2017; pp. 447–471. [Google Scholar] [CrossRef]
- Gerlach, U.; Hiby, W. Sorbitol Dehydrogenase. In Methods of Enzymatic Analysis, 2nd ed.; Bergmeyer, H.U., Ed.; Academic Press: Cambridge, MA, USA, 1974; pp. 569–573. [Google Scholar] [CrossRef]
- El-Kabbani, O.; Darmanin, C.; Chung, R.P. Sorbitol dehydrogenase: Structure, function and ligand design. Curr. Med. Chem. 2004, 11, 465–476. [Google Scholar] [CrossRef]
- Wiesner, I.S.; Rawnsley, H.M.; Brooks, F.P.; Sentor, J.R. Sorbitol dehydrogenase in the diagnosis of liver disease. Am. J. Dig. Dis. 1965, 10, 147–151. [Google Scholar] [CrossRef]
- Asada, M.; Galambos, J.T. Sorbitol Dehydrogenase and Hepatocellular Injury: An Experimental and Clinical Study. Gastroenterology 1963, 44, 578–587. [Google Scholar] [CrossRef]
- Singh, M.; Kapoor, A.; Bhatnagar, A. Physiological and Pathological Roles of Aldose Reductase. Metabolites 2021, 11, 655. [Google Scholar] [CrossRef] [PubMed]
- Schwab, A.; Siddiqui, A.; Vazakidou, M.E.; Napoli, F.; Böttcher, M.; Menchicchi, B.; Raza, U.; Saatci, Ö.; Krebs, A.M.; Ferrazzi, F.; et al. Polyol Pathway Links Glucose Metabolism to the Aggressiveness of Cancer Cells. Cancer Res. 2018, 78, 1604–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, I.T.; Fiehn, O.; Elfert, A.; Helal, M.; Salama, I.; El-Said, H. Sugar Alcohols Have a Key Role in Pathogenesis of Chronic Liver Disease and Hepatocellular Carcinoma in Whole Blood and Liver Tissues. Cancers 2020, 12, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uzozie, A.; Nanni, P.; Staiano, T.; Grossmann, J.; Barkow-Oesterreicher, S.; Shay, J.W.; Tiwari, A.; Buffoli, F.; Laczko, E.; Marra, G. Sorbitol dehydrogenase overexpression and other aspects of dysregulated protein expression in human precancerous colorectal neoplasms: A quantitative proteomics study. Mol. Cell Proteom. 2014, 13, 1198–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000140263-SORD/pathology/liver+cancer (accessed on 26 July 2021).
- Uhlen, M.; Zhang, C.; Lee, S.; Sjöstedt, E.; Fagerberg, L.; Bidkhori, G.; Benfeitas, R.; Arif, M.; Liu, Z.; Edfors, F.; et al. A pathology atlas of the human cancer transcriptome. Science 2017, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerlach, U. Sorbitol Dehydrogenase. In Methods of Enzymatic Analysis; Bergmeyer, H.-U., Ed.; Academic Press: Cambridge, MA, USA, 1965; pp. 761–764. [Google Scholar] [CrossRef]
- Korsrud, G.O.; Grice, H.G.; Goodman, T.K.; Knipfel, J.E.; McLaughlan, J.M. Sensitivity of several serum enzymes for the detection of thioacetamide-, dimethylnitrosamine- and diethanolamine-induced liver damage in rats. Toxicol. Appl. Pharm. 1973, 26, 299–313. [Google Scholar] [CrossRef]
- Smith, G.S.; Walter, G.L.; Walker, R.M. Chapter 18-Clinical Pathology in Non-Clinical Toxicology Testing. In Haschek and Rousseaux’s Handbook of Toxicologic Pathology, 3rd ed.; Haschek, W.M., Rousseaux, C.G., Wallig, M.A., Eds.; Academic Press: Cambridge, MA, USA, 2013; pp. 565–594. [Google Scholar] [CrossRef]
- Zhang, D.Y.; Friedman, S.L. Fibrosis-dependent mechanisms of hepatocarcinogenesis. Hepatology 2012, 56, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16, 1. [Google Scholar] [CrossRef]
- Harvey, R.F. Denise. Lippincott’s Illustrated Reviews: Biochemistry, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; p. 140. [Google Scholar]
- Kayali, A.G.; Austin, D.A.; Webster, N.J. Stimulation of MAPK cascades by insulin and osmotic shock: Lack of an involvement of p38 mitogen-activated protein kinase in glucose transport in 3T3-L1 adipocytes. Diabetes 2000, 49, 1783–1793. [Google Scholar] [CrossRef] [Green Version]
- Kwak, D.; Choi, S.; Jeong, H.; Jang, J.H.; Lee, Y.; Jeon, H.; Lee, M.N.; Noh, J.; Cho, K.; Yoo, J.S.; et al. Osmotic stress regulates mammalian target of rapamycin (mTOR) complex 1 via c-Jun N-terminal Kinase (JNK)-mediated Raptor protein phosphorylation. J. Biol. Chem. 2012, 287, 18398–18407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, N.; Jin, Y.; Li, Y.; Zhu, S.; Bai, H. AKR1B10 Inhibitor Epalrestat Facilitates Sorafenib-Induced Apoptosis and Autophagy Via Targeting the mTOR Pathway in Hepatocellular Carcinoma. Int. J. Med. Sci. 2020, 17, 1246–1256. [Google Scholar] [CrossRef]
- Gnoni, A.; Licchetta, A.; Memeo, R.; Argentiero, A.; Solimando, A.G.; Longo, V.; Delcuratolo, S.; Brunetti, O. Role of BRAF in Hepatocellular Carcinoma: A Rationale for Future Targeted Cancer Therapies. Medicina 2019, 55, 754. [Google Scholar] [CrossRef] [Green Version]
- Ma, W.-J.; Wang, H.-Y.; Teng, L.-S. Correlation analysis of preoperative serum alpha-fetoprotein (AFP) level and prognosis of hepatocellular carcinoma (HCC) after hepatectomy. World J. Surg. Oncol. 2013, 11, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangkijvanich, P.; Anukulkarnkusol, N.; Suwangool, P.; Lertmaharit, S.; Hanvivatvong, O.; Kullavanijaya, P.; Poovorawan, Y. Clinical Characteristics and Prognosis of Hepatocellular Carcinoma: Analysis Based on Serum Alpha-fetoprotein Levels. J. Clin. Gastroenterol. 2000, 31, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.K.; Hlaing, W.W.; Yu, R.Q.; Lee, T.W.; Ganpathi, I.S.; Madhavan, K.K. Value of alpha-foetoprotein for screening of recurrence in hepatocellular carcinoma post resection. Singap. Med. J. 2012, 53, 32–35. [Google Scholar]
- Shah, S.A.; Greig, P.D.; Gallinger, S.; Cattral, M.S.; Dixon, E.; Kim, R.D.; Taylor, B.R.; Grant, D.R.; Vollmer, C.M. Factors associated with early recurrence after resection for hepatocellular carcinoma and outcomes. J. Am. Coll. Surg. 2006, 202, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Sumie, S.; Kuromatsu, R.; Okuda, K.; Ando, E.; Takata, A.; Fukushima, N.; Watanabe, Y.; Kojiro, M.; Sata, M. Microvascular invasion in patients with hepatocellular carcinoma and its predictable clinicopathological factors. Ann. Surg. Oncol. 2008, 15, 1375–1382. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | SORD <15 ng/mL | SORD ≥15 ng/mL | p-Value |
|---|---|---|---|---|
| [N = 92] | [N = 73] | [N = 19] | ||
| Age, median [IQR], y | 55.0 [47.8, 60.3] | 54.0 [46.0, 61.0] | 57.0 [51.0, 59.5] | 0.40 |
| Male, n (%) | 76 (82.6) | 58 (79.5) | 18 (94.7) | 0.22 |
| Etiology, n (%) | 0.79 | |||
| Hepatitis B | 82 (89.1) | 65 (89.0) | 17 (89.5) | |
| Hepatitis C | 3 (3.3) | 2 (2.7) | 1 (5.3) | |
| Others | 7 (7.6) | 6 (8.2) | 1 (5.3) | |
| Diabetes, n (%) | 19 (20.7) | 12 (16.4) | 7 (36.8) | 0.10 |
| Previous TACE, n (%) | 15 (16.3) | 11 (15.1) | 4 (21.1) | 0.78 |
| AFP, ng/mL | 32.1 [6.3, 300.5] | 51.4 [6.4, 270.0] | 11.6 [7.0, 1501.5] | 0.84 |
| <400, n (%) | 70 (76.1) | 57 (78.1) | 14 (68.4) | 0.56 |
| ≥400, n (%) | 22 (23.9) | 16 (21.9) | 6 (31.6) | 0.56 |
| PIVKA-II, mAU/mL | 45.0 [21.8, 366.5] | 45.0 [23.0, 309.0] | 68.0 [19.0, 495.5] | 0.91 |
| <40, n (%) | 43 (46.7) | 34 (46.6) | 9 (47.4) | >0.99 |
| ≥40, n (%) | 49 (53.3) | 39 (53.4) | 10 (52.6) | >0.99 |
| AST, median [IQR], IU/L | 31.5 [26.8, 44.0] | 31.0 [26.0, 42.0] | 39.0 [28.0, 56.0] | 0.18 |
| ALT, median [IQR], IU/L | 33.0 [24.0, 44.5] | 32.0 [24.0, 43.0] | 38.0 [28.0, 53.0] | 0.24 |
| Platelet, median [IQR], ×103/μL | 131.50 [110.8, 175.5] | 131.0 [113.0, 178.0] | 132.0 [102.0, 159.5] | 0.53 |
| Albumin, median [IQR], g/dL | 3.9 [3.6, 4.2] | 3.9 [3.6, 4.2] | 3.7 [3.5, 4.2] | 0.32 |
| Bilirubin, median [IQR], IU/L | 0.9 [0.7, 1.1] | 0.9 [0.7, 1.1] | 0.9 [0.7, 1.2] | 0.89 |
| Creatinine, median [IQR], mg/dL | 0.8 [0.7, 0.9] | 0.8 [0.7, 0.9] | 0.8 [0.8, 1.0] | 0.64 |
| Prothrombin time, median [IQR], INR | 1.06 [1.01, 1.13] | 1.06 [1.01, 1.13] | 1.06 [1.01, 1.14] | 0.60 |
| Child-Pugh score, n (%) | 0.67 | |||
| 5 | 80 (87.0) | 63 (86.3) | 17 (89.5) | |
| 6 | 9 (9.8) | 8 (11.0) | 1 (5.3) | |
| 7 | 3 (3.3) | 2 (2.7) | 1 (5.3) | |
| ALBI grade, n (%) | 0.56 | |||
| 1 | 38 (41.3) | 31 (42.5) | 7 (36.8) | |
| 2 | 52 (56.5) | 41 (56.2) | 11 (57.9) | |
| 3 | 2 (2.2) | 1 (1.4) | 1 (5.3) | |
| ICG-R15, median [IQR], % | 11.2 [8.2, 13.8] | 11.0 [8.2, 13.4] | 13.6 [8.9, 16.8] | 0.23 |
| Cirrhosis | 81 (88.0) | 64 (87.7) | 17 (89.5) | >0.99 |
| Resection type *, n (%) | 0.01 | |||
| Major | 18 (19.6) | 10 (13.7) | 8 (42.1) | |
| Minor | 74 (80.4) | 63 (86.3) | 11 (57.9) | |
| Tumor size, median [IQR], cm | 3.0 [2.3, 4.2] | 3.0 [2.1, 4.3] | 3.3 [2.8, 3.5] | 0.32 |
| Microscopic vascular invasion, n (%) | 24 (26.1) | 16 (21.9) | 8 (42.1) | 0.14 |
| Edmondson grade, n (%) | >0.99 | |||
| I or II | 19 (20.7) | 15 (20.5) | 4 (21.1) | |
| III or IV | 73 (79.3) | 58 (79.5) | 15 (78.9) | |
| Recurrence, n (%) | 43 (46.7) | 29 (39.7) | 14 (73.7) | 0.02 |
| Follow up, median [IQR], month | 57.1 [19.8, 102.6] | 66.3 [25.7, 104.3] | 19.7 [5.3, 44.1] | 0.003 |
| Variable | Univariate Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age ≥60 y | 1.02 | 0.52–1.98 | 0.96 | — | — | — |
| Male | 2.57 | 0.92–7.18 | 0.07 | 1.93 | 0.67–5.53 | 0.22 |
| ICG R15 ≥10% | 1.71 | 0.90–3.36 | 0.10 | 1.67 | 0.87–3.18 | 0.13 |
| Cirrhosis | 3.14 | 0.76–13.0 | 0.11 | 2.82 | 0.67–11.84 | 0.16 |
| Child-Pugh score ≥6 | 0.77 | 0.30–1.97 | 0.59 | — | — | — |
| ALBI grade ≥2 | 1.37 | 0.74–2.54 | 0.31 | — | — | — |
| Tumor size ≥5 cm | 0.98 | 0.44–2.21 | 0.97 | — | — | — |
| Microscopic vascular invasion | 1.48 | 0.77–2.83 | 0.24 | — | — | — |
| AFP ≥400 ng/mL | 1.68 | 0.86–3.27 | 0.13 | 2.08 | 1.04–4.17 | 0.04 |
| PIVKA-II ≥40 mAU/mL | 1.24 | 0.68–2.27 | 0.48 | — | — | — |
| SORD ≥15 ng/mL | 3.29 | 1.72–6.28 | <0.001 * | 3.24 | 1.64–6.37 | <0.001 |
| Major hepatectomy * | 1.63 | 0.80–3.30 | 0.18 | — | — | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, D.; Choi, W.-M.; Kim, J.-S.; Jung, Y.; Lee, S.-Y.; Seo, H.R.; Kim, K.M. Serum Sorbitol Dehydrogenase as a Novel Prognostic Factor for Hepatocellular Carcinoma after Surgical Resection. Cancers 2021, 13, 6143. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236143
Jeon D, Choi W-M, Kim J-S, Jung Y, Lee S-Y, Seo HR, Kim KM. Serum Sorbitol Dehydrogenase as a Novel Prognostic Factor for Hepatocellular Carcinoma after Surgical Resection. Cancers. 2021; 13(23):6143. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236143
Chicago/Turabian StyleJeon, Dongsub, Won-Mook Choi, Jin-Sun Kim, Yusun Jung, Su-Yeon Lee, Haeng Ran Seo, and Kang Mo Kim. 2021. "Serum Sorbitol Dehydrogenase as a Novel Prognostic Factor for Hepatocellular Carcinoma after Surgical Resection" Cancers 13, no. 23: 6143. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236143