
An Extensive Quality Control and Quality Assurance (QC/QA) Program Significantly Improves Inter-Laboratory Concordance Rates of Flow-Cytometric Minimal Residual Disease Assessment in Acute Lymphoblastic Leukemia: An I-BFM-FLOW-Network Report

 , , , , , , , , , , , , , , ,
, , , , , , , , , , , , , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Samples
Sample Preparation
2.2. I-BFM-FLOW Twinning and Maturation Program
2.3. External Quality Assessment (EQA)
2.4. List-Mode-Data File Ring Trials (LMD Ring Trial)
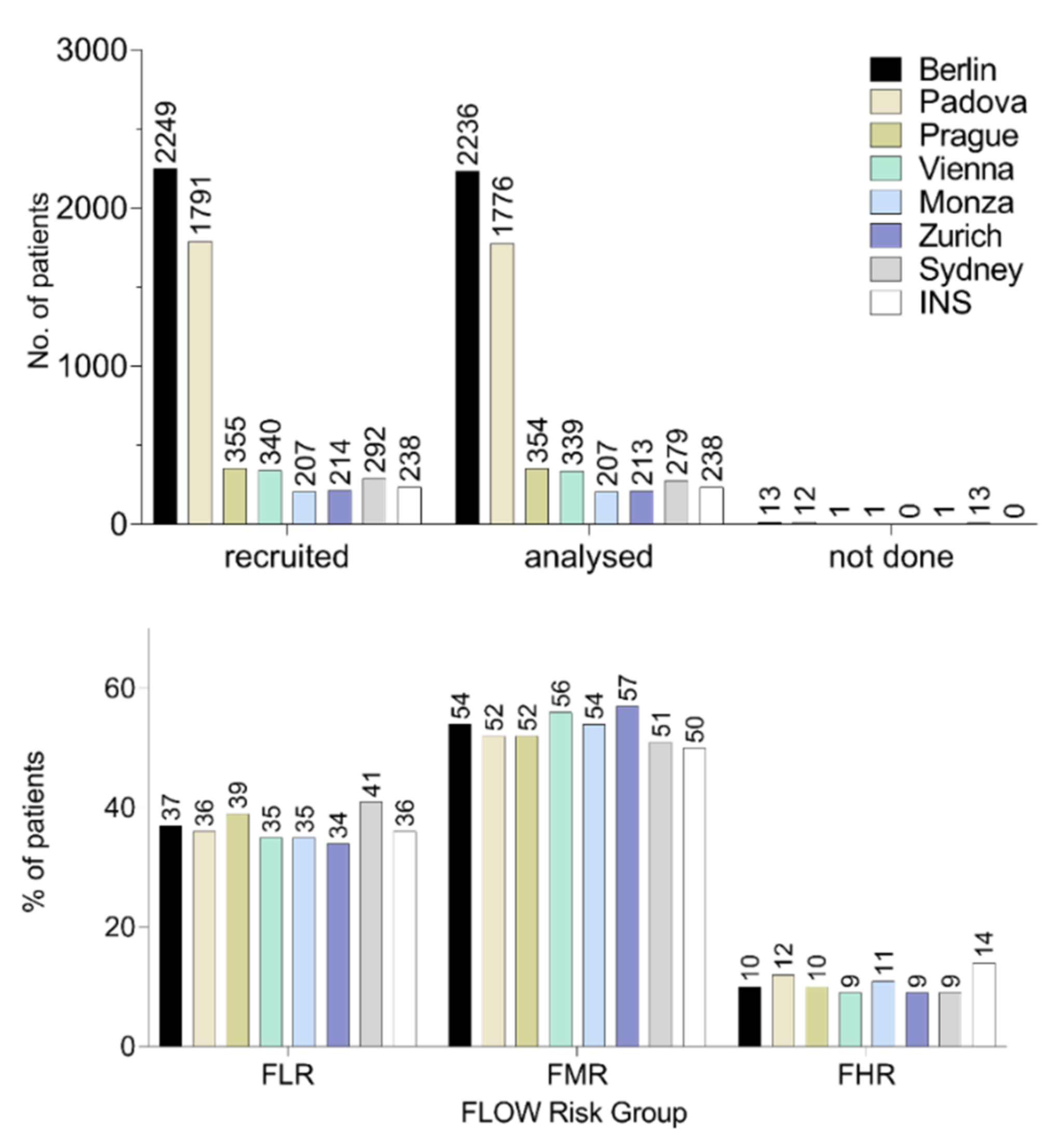
2.5. Independent Data Survey
2.6. Statistical Analysis
3. Results
3.1. Twinning Maturation Program
3.2. External Quality Assessment
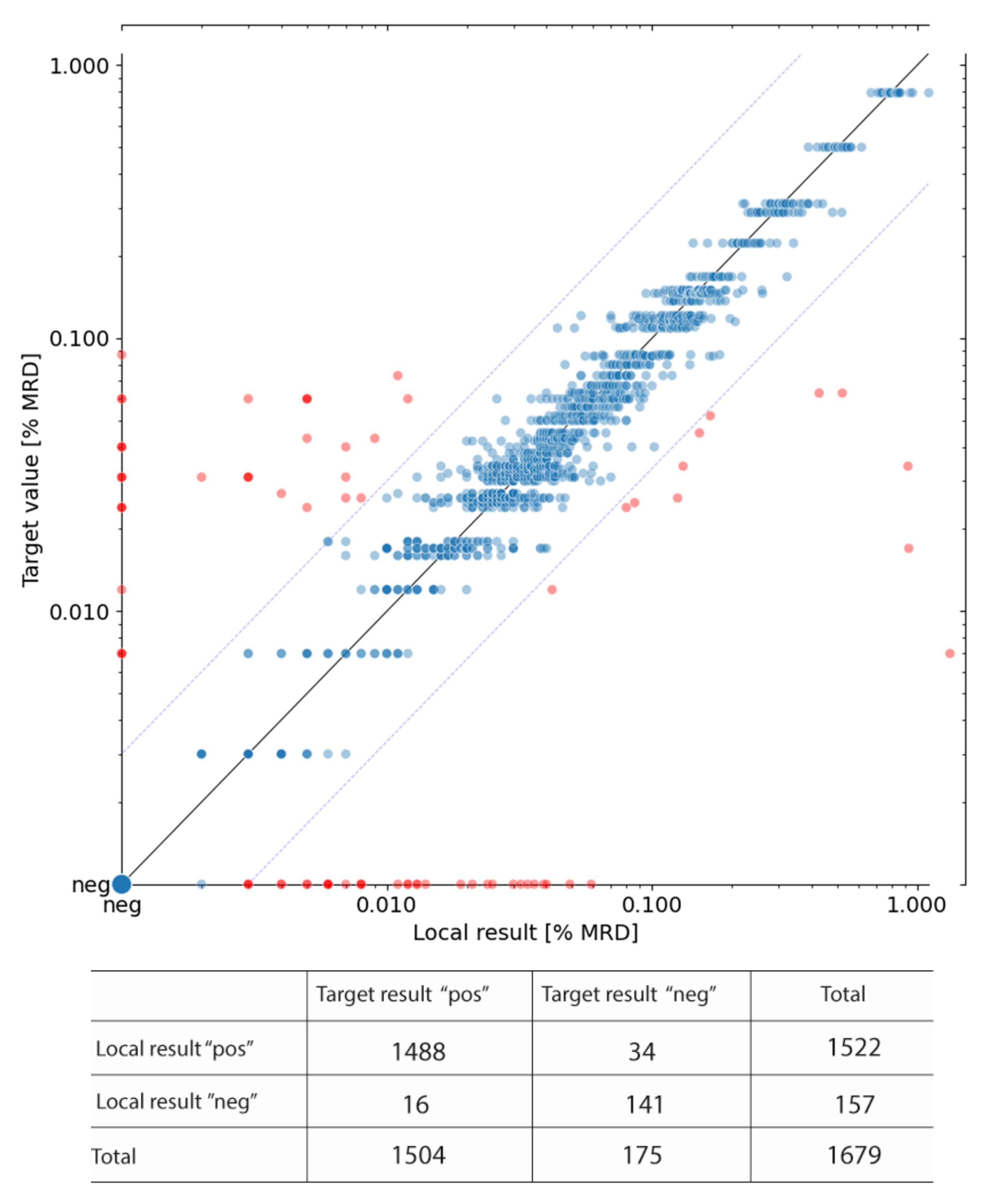
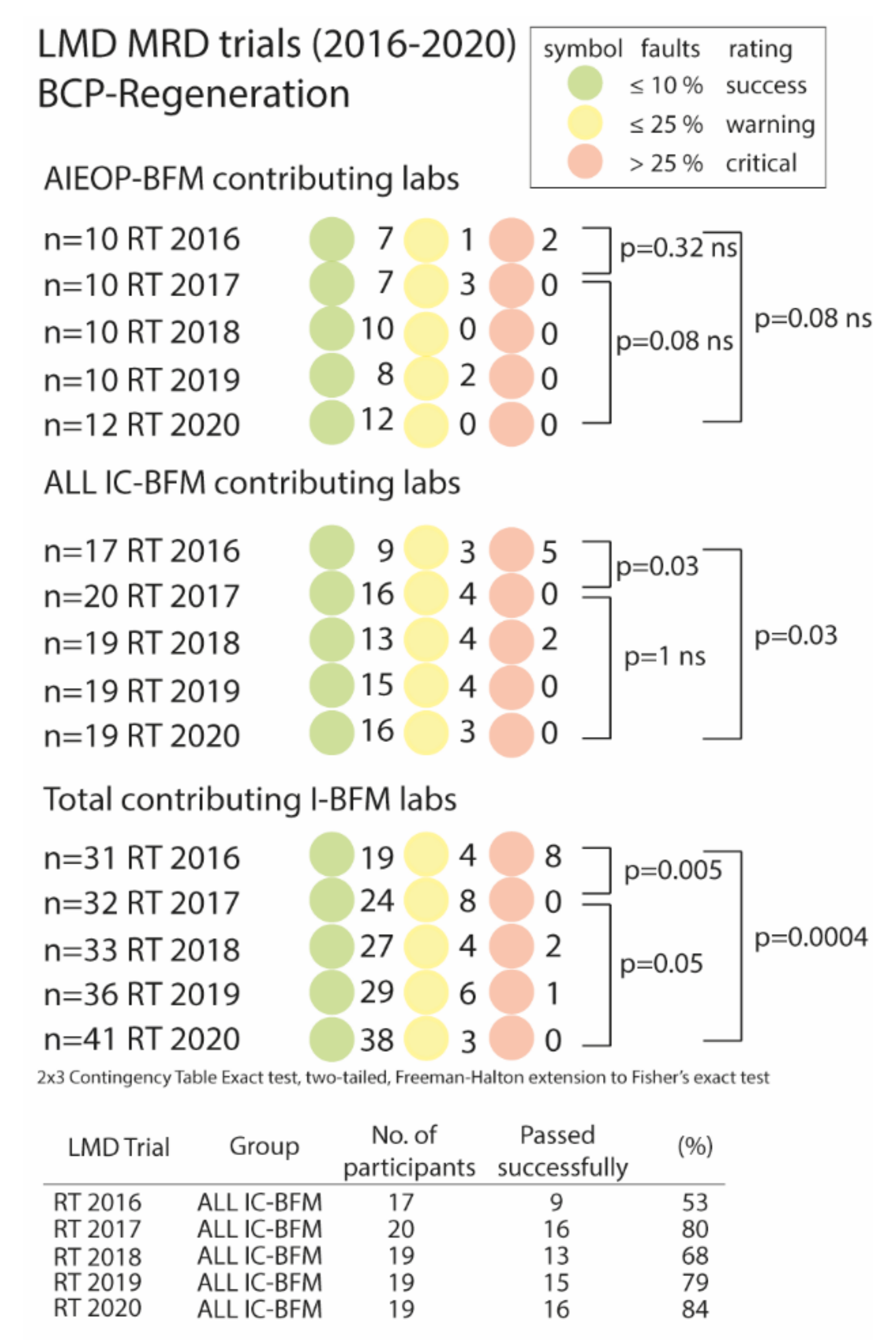
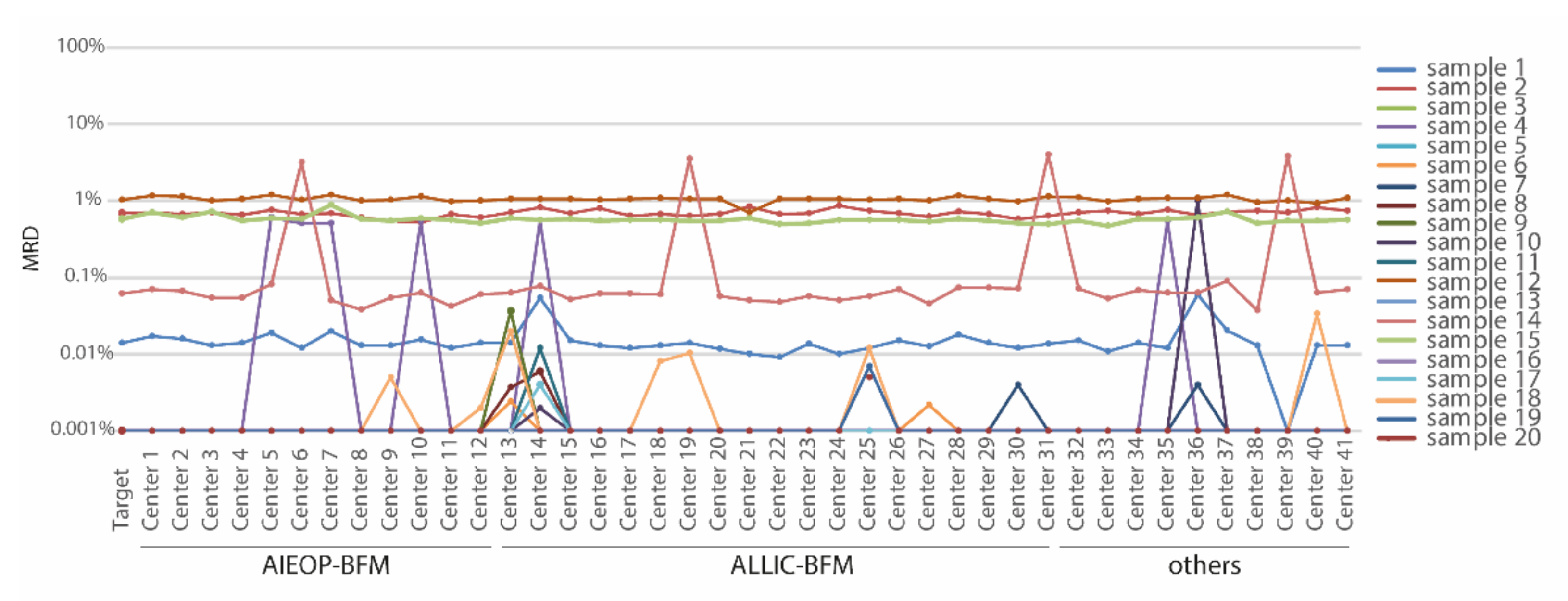
3.3. List Mode Data File Ring Trials (LMD Ring Trial)
3.4. Independent Data Concordance: A Retrospective Quality Control Measure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gaipa, G.; Buracchi, C.; Biondi, A. Flow cytometry for minimal residual disease testing in acute leukemia: Opportunities and challenges. Expert Rev. Mol. Diagn. 2018, 18, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Coustan-Smith, E.; Behm, F.G.; Sanchez, J.; Boyett, J.M.; Hancock, M.L.; Raimondi, S.C.; E Rubnitz, J.; Rivera, G.K.; Sandlund, J.T.; Pui, C.-H.; et al. Immunological detection of minimal residual disease in children with acute lymphoblastic leukaemia. Lancet 1998, 351, 550–554. [Google Scholar] [CrossRef]
- Borowitz, M.J.; Devidas, M.; Hunger, S.P.; Bowman, W.P.; Carroll, A.J.; Carroll, W.L.; Linda, S.; Martin, P.L.; Pullen, D.J.; Viswanatha, D.; et al. Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia and its relationship to other prognostic factors: A Children’s Oncology Group study. Blood 2008, 111, 5477–5485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dworzak, M.N.; Fröschl, G.; Printz, D.; Mann, G.; Pötschger, U.; Mühlegger, N.; Fritsch, G.; Gadner, H.G. Austrian Berlin-Frankfurt-Munster Study, Prognostic significance and modalities of flow cytometric minimal residual disease detection in childhood acute lymphoblastic leukemia. Blood 2002, 99, 1952–1958. [Google Scholar] [CrossRef] [Green Version]
- Brüggemann, M.; Schrauder, A.; Raff, T.; Pfeifer, H.; Dworzak, M.; Ottmann, O.G.; Asnafi, V.; Baruchel, A.; Bassan, R.; Benoit, Y.; et al. Standardized MRD quantification in European ALL trials. In Proceedings of the Second International Symposium on MRD Assessment, Kiel, Germany, 18–20 September 2008. [Google Scholar]
- Basso, G.; Veltroni, M.; Valsecchi, M.G.; Dworzak, M.N.; Ratei, R.; Silvestri, D.; Benetello, A.; Buldini, B.; Maglia, O.; Masera, G.; et al. Risk of Relapse of Childhood Acute Lymphoblastic Leukemia Is Predicted By Flow Cytometric Measurement of Residual Disease on Day 15 Bone Marrow. J. Clin. Oncol. 2009, 27, 5168–5174. [Google Scholar] [CrossRef]
- Irving, J.; Jesson, J.; Virgo, P.; Case, M.; Minto, L.; Eyre, L.; Noel, N.; Johansson, U.; Macey, M.; Knotts, L.; et al. Establishment and validation of a standard protocol for the detection of minimal residual disease in B lineage childhood acute lymphoblastic leukemia by flow cytometry in a multi-center setting. Haematologica 2009, 94, 870–874. [Google Scholar] [CrossRef] [Green Version]
- Björklund, E.; Matinlauri, I.; Tierens, A.; Axelsson, S.; Forestier, E.; Jacobsson, S.; Ahlberg, A.J.; Kauric, G.; Mäntymaa, P.; Osnes, L.; et al. Quality Control of Flow Cytometry Data Analysis for Evaluation of Minimal Residual Disease in Bone Marrow from Acute Leukemia Patients during Treatment. J. Pediatr. Hematol. Oncol. 2009, 31, 406–415. [Google Scholar] [CrossRef]
- Dworzak, M.N.; Gaipa, G.; Ratei, R.; Veltroni, M.; Schumich, A.; Maglia, O.; Karawajew, L.; Benetello, A.; Pötschger, U.; Husak, Z.; et al. Standardization of flow cytometric minimal residual disease evaluation in acute lymphoblastic leukemia: Multicentric assessment is feasible. Cytom. Part B Clin. Cytom. 2008, 74, 331–340. [Google Scholar] [CrossRef]
- Theunissen, P.; Mejstrikova, E.; Sędek, L.; Van Der Sluijs-Gelling, A.J.; Gaipa, G.; Bartels, M.; da Costa, E.S.; Kotrová, M.; Novakova, M.; Sonneveld, E.; et al. Standardized flow cytometry for highly sensitive MRD measurements in B-cell acute lymphoblastic leukemia. Blood 2017, 129, 347–357. [Google Scholar] [CrossRef]
- Lorenzana, R.; Coustan-Smith, E.; Antillon, F.; Ribeiro, R.; Campana, D. Simple methods for the rapid exchange of flow cytometric data between remote centers. Leukemia 2000, 14, 336–337. [Google Scholar] [CrossRef] [Green Version]
- Keeney, M.; Wood, B.L.; Hedley, B.D.; DiGiuseppe, J.A.; Stetler-Stevenson, M.; Paietta, E.; Lozanski, G.; Seegmiller, A.C.; Greig, B.W.; Shaver, A.C.; et al. A QA Program for MRD Testing Demonstrates That Systematic Education Can Reduce Discordance Among Experienced Interpreters. Cytom. Part B Clin. Cytom. 2018, 94, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Dworzak, M.N.; Fritsch, G.; Fleischer, C.; Printz, D.; Fröschl, G.; Buchinger, P.; Mann, G.; Gadner, H. Multiparameter phenotype mapping of normal and post-chemotherapy B lymphopoiesis in pediatric bone marrow. Leukemia 1997, 11, 1266–1273. [Google Scholar] [CrossRef] [Green Version]
- Bainbridge, J.; Rountree, W.; Louzao, R.; Wong, J.; Whitby, L.; Denny, T.N.; Barnett, D. Laboratory Accuracy Improvement in the UK NEQAS Leucocyte Immunophenotyping Immune Monitoring Program: An Eleven-Year Review via Longitudinal Mixed Effects Modeling. Cytom. Part B Clin. Cytom. 2017, 94, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Freeman, G.H.; Halton, J.H. Note on an Exact Treatment of Contingency, Goodness of Fit and Other Problems of Significance. Biometrika 1951, 38, 141–149. [Google Scholar] [CrossRef]
- Soper, D. 2 × 3 Contingency Table Exact Test Calculator. 2020. Available online: http://www.analyticscalculators.com (accessed on 20 November 2021).
- Reiter, M.; Diem, M.; Schumich, A.; Maurer-Granofszky, M.; Karawajew, L.; Rossi, J.G.; Ratei, R.; Groeneveld-Krentz, S.; Sajaroff, E.O.; Suhendra, S.; et al. Automated Flow Cytometric MRD Assessment in Childhood Acute B-Lymphoblastic Leukemia Using Supervised Machine Learning. Cytom. Part A 2019, 95, 966–975. [Google Scholar] [CrossRef]
- Denys, B.; Van Der Sluijs-Gelling, A.J.; Homburg, C.; Van Der Schoot, C.E.; De Haas, V.; Philippé, J.; Pieters, R.; Van Dongen, J.; Van Der Velden, V.H.J. Improved flow cytometric detection of minimal residual disease in childhood acute lymphoblastic leukemia. Leukemia 2012, 27, 635–641. [Google Scholar] [CrossRef]
- Karawajew, L.; Dworzak, M.; Ratei, R.; Rhein, P.; Gaipa, G.; Buldini, B.; Basso, G.; Hrusak, O.; Ludwig, W.-D.; Henze, G.; et al. Minimal residual disease analysis by eight-color flow cytometry in relapsed childhood acute lymphoblastic leukemia. Haematologica 2015, 100, 935–944. [Google Scholar] [CrossRef]
- Bouriche, L.; Bernot, D.; Nivaggioni, V.; Arnoux, I.; Loosveld, M. Detection of Minimal Residual Disease in B Cell Acute Lymphoblastic Leukemia Using an Eight-Color Tube with Dried Antibody Reagents. Cytom. Part B Clin. Cytom. 2019, 96, 158–163. [Google Scholar] [CrossRef]
- Tembhare, P.R.; Pg, P.G.S.; Ghogale, S.; Chatterjee, G.; Patkar, N.; Gupta, A.; Shukla, R.; Badrinath, Y.; Deshpande, N.; Narula, G.; et al. A High-Sensitivity 10-Color Flow Cytometric Minimal Residual Disease Assay in B-Lymphoblastic Leukemia/Lymphoma Can Easily Achieve the Sensitivity of 2-in-10 6 and Is Superior to Standard Minimal Residual Disease Assay: A Study of 622 Patients. Cytom. Part B Clin. Cytom. 2019, 98, 57–67. [Google Scholar] [CrossRef]
- Van Gassen, S.; Callebaut, B.; Van Helden, M.J.; Lambrecht, B.N.; Demeester, P.; Dhaene, T.; Saeys, Y. FlowSOM: Using self-organizing maps for visualization and interpretation of cytometry data. Cytom. Part A 2015, 87, 636–645. [Google Scholar] [CrossRef]
- Ni, W.; Hu, B.; Zheng, C.; Tong, Y.; Wang, L.; Li, Q.-Q.; Tong, X.; Han, Y. Automated analysis of acute myeloid leukemia minimal residual disease using a support vector machine. Oncotarget 2016, 7, 71915–71921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrad, V.K.; Dubay, C.J.; Malek, M.; Brinkman, R.R.; Koguchi, Y.; Redmond, W.L. Implementation and Validation of an Automated Flow Cytometry Analysis Pipeline for Human Immune Profiling. Cytom. Part A 2019, 95, 183–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overview | |
|---|---|
| Nº of trainee labs § | 22 |
| Nº of expert trainer labs * | 7 |
| Nº of samples reviewed | 682 |
| Nº of samples required for maturation/lab | 25 |
| Median needed [range] | 28 (25–57) |
| Mean needed [SD] | 31 (8.8) |
| All 22 Trainee Laboratories | ||||
|---|---|---|---|---|
| Main Sample Set (Sample 1–25) | Series 1 (Sample 1–13) | Series 2 (Sample 14–25) | Series 3 (Sample 14–pX) § | |
| Total Nº of reported results | 550 | 286 | 264 | 396 |
| Nº of failures | 67 | 42 | 25 | 37 |
| Failures [%] | 12.2 | 14.7 | 9.5 | 9.3 |
| All samples (sample 1–57) | ||||
| Total Nº of reported results | 682 | |||
| Nº of failures | 79 | |||
| Failures [%] | 11.6 | |||
| Participation | |||
| Nº of issued trials a | 29 | ||
| Nº of participating laboratories | 29–38 | ||
| Nº of possible results | 1925 | ||
| Nº of submitted results | 1679 | ||
| Performance | |||
| AIEOP-BFM | ALL IC-BFM/others | Total | |
| Nº of submitted results | 487 | 1192 | 1679 |
| Nº of Outliers b | 11 | 67 | 78 |
| Outliers b [%] | 2.3 | 5.6 | 4.6 |
| p = 0.0043 c | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maurer-Granofszky, M.; Schumich, A.; Buldini, B.; Gaipa, G.; Kappelmayer, J.; Mejstrikova, E.; Karawajew, L.; Rossi, J.; Suzan, A.Ç.; Agriello, E.; et al. An Extensive Quality Control and Quality Assurance (QC/QA) Program Significantly Improves Inter-Laboratory Concordance Rates of Flow-Cytometric Minimal Residual Disease Assessment in Acute Lymphoblastic Leukemia: An I-BFM-FLOW-Network Report. Cancers 2021, 13, 6148. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236148
Maurer-Granofszky M, Schumich A, Buldini B, Gaipa G, Kappelmayer J, Mejstrikova E, Karawajew L, Rossi J, Suzan AÇ, Agriello E, et al. An Extensive Quality Control and Quality Assurance (QC/QA) Program Significantly Improves Inter-Laboratory Concordance Rates of Flow-Cytometric Minimal Residual Disease Assessment in Acute Lymphoblastic Leukemia: An I-BFM-FLOW-Network Report. Cancers. 2021; 13(23):6148. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236148
Chicago/Turabian StyleMaurer-Granofszky, Margarita, Angela Schumich, Barbara Buldini, Giuseppe Gaipa, Janos Kappelmayer, Ester Mejstrikova, Leonid Karawajew, Jorge Rossi, Adın Çınar Suzan, Evangelina Agriello, and et al. 2021. "An Extensive Quality Control and Quality Assurance (QC/QA) Program Significantly Improves Inter-Laboratory Concordance Rates of Flow-Cytometric Minimal Residual Disease Assessment in Acute Lymphoblastic Leukemia: An I-BFM-FLOW-Network Report" Cancers 13, no. 23: 6148. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236148