
Interventions Facilitating Family Communication of Genetic Testing Results and Cascade Screening in Hereditary Breast/Ovarian Cancer or Lynch Syndrome: A Systematic Review and Meta-Analysis



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
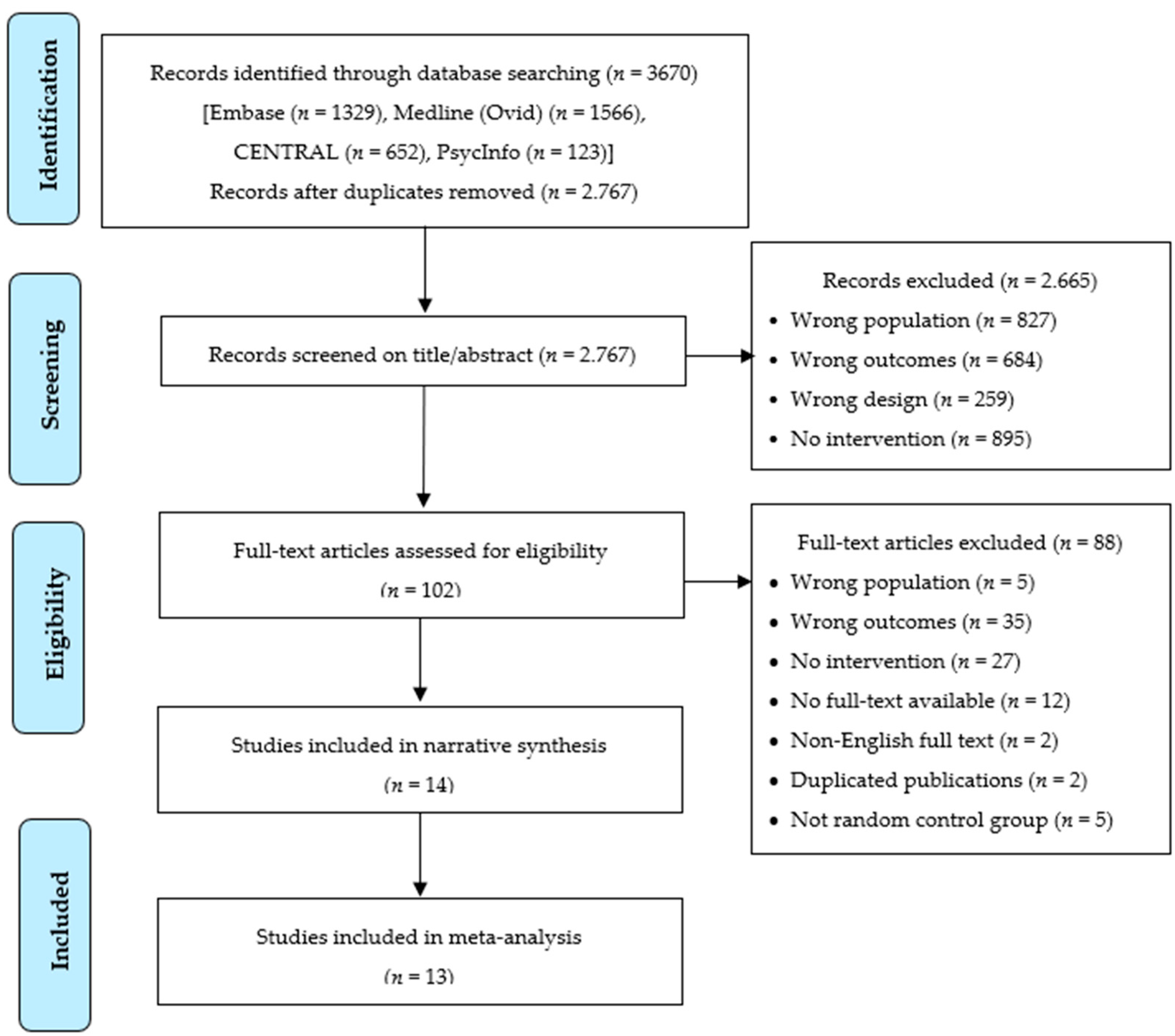
2.1. Literature Extraction
2.2. Screening, Inclusion, and Exclusion Criteria
2.3. Data Extraction
2.4. Statistical Analyses
3. Results
3.1. Characteristics and Content of Interventions
3.2. Intervention Mode of Delivery and Intervener
3.3. Intervention Dose and Duration
3.4. Characteristics of Samples
3.5. Effect Sizes Obtained for Outcomes
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A.
Search Strategies
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in Globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Allemani, C.; Weir, H.K.; Carreira, H.; Harewood, R.; Spika, D.; Wang, X.S.; Bannon, F.; Ahn, J.V.; Johnson, C.J.; Bonaventure, A.; et al. Global surveillance of cancer survival 1995–2009: Analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (Concord-2). Lancet 2015, 385, 977–1010. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A population-based study of genes previously implicated in breast cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Chubb, D.; Broderick, P.; Frampton, M.; Kinnersley, B.; Sherborne, A.; Penegar, S.; Lloyd, A.; Ma, Y.P.; Dobbins, S.E.; Houlston, R.S. Genetic diagnosis of high-penetrance susceptibility for colorectal cancer (CRC) is achievable for a high proportion of familial CRC by exome sequencing. J. Clin. Oncol. 2015, 33, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Casadei, S.; Lee, M.K.; Pennil, C.C.; Nord, A.S.; Thornton, A.M.; Roeb, W.; Agnew, K.J.; Stray, S.M.; Wickramanayake, A.; et al. Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Proc. Natl. Acad. Sci. USA 2011, 108, 18032–18037. [Google Scholar] [CrossRef] [Green Version]
- Couch, F.J.; Nathanson, K.L.; Offit, K. Two decades after BRCA: Setting paradigms in personalized cancer care and prevention. Science 2014, 343, 1466–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavaddat, N.; Peock, S.; Frost, D.; Ellis, S.; Platte, R.; Fineberg, E.; Evans, D.G.; Izatt, L.; Eeles, R.A.; Adlard, J.; et al. Cancer risks for BRCA1 and BRCA2 mutation carriers: Results from prospective analysis of embrace. J. Natl. Cancer Inst. 2013, 105, 812–822. [Google Scholar] [CrossRef] [Green Version]
- Giardiello, F.M.; Allen, J.I.; Axilbund, J.E.; Boland, C.R.; Burke, C.A.; Burt, R.W.; Church, J.M.; Dominitz, J.A.; Johnson, D.A.; Kaltenbach, T.; et al. Guidelines on genetic evaluation and management of lynch syndrome: A consensus statement by the us multi-society task force on colorectal cancer. Am. J. Gastroenterol. 2014, 109, 1159–1179. [Google Scholar] [CrossRef]
- Bellcross, C.A.; Bedrosian, S.R.; Daniels, E.; Duquette, D.; Hampel, H.; Jasperson, K.; Joseph, D.A.; Kaye, C.; Lubin, I.; Meyer, L.J.; et al. Implementing screening for Lynch syndrome among patients with newly diagnosed colorectal cancer: Summary of a public health/clinical collaborative meeting. Genet. Med. 2012, 14, 152–162. [Google Scholar] [CrossRef] [Green Version]
- Syngal, S.; Brand, R.E.; Church, J.M.; Giardiello, F.M.; Hampel, H.L.; Burt, R.W. Acg clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am. J. Gastroenterol. 2015, 110, 223–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W., Jr.; Garcia, F.A.; Gillman, M.W.; Harper, D.M.; Kemper, A.R.; Krist, A.H.; et al. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA 2016, 315, 2564–2575. [Google Scholar] [PubMed]
- Greenberg, S.; Buys, S.S.; Edwards, S.L.; Espinel, W.; Fraser, A.; Gammon, A.; Hafen, B.; Herget, K.A.; Kohlmann, W.; Roundy, C.; et al. Population prevalence of individuals meeting criteria for hereditary breast and ovarian cancer testing. Cancer Med. 2019, 8, 6789–6798. [Google Scholar] [CrossRef]
- Grosse, S.D.; Rogowski, W.H.; Ross, L.F.; Cornel, M.C.; Dondorp, W.J.; Khoury, M.J. Population screening for genetic disorders in the 21st century: Evidence, economics, and ethics. Public Health Genom. 2010, 13, 106–115. [Google Scholar] [CrossRef]
- Clain, E.; Trosman, J.R.; Douglas, M.P.; Weldon, C.B.; Phillips, K.A. Availability and payer coverage of BRCA1/2 tests and gene panels. Nat. Biotechnol. 2015, 33, 900–902. [Google Scholar] [CrossRef] [Green Version]
- Hampel, H. Genetic counseling and cascade genetic testing in Lynch syndrome. Fam. Cancer 2016, 15, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Khoury, M.J.; Evans, J.P. A public health perspective on a national precision medicine cohort: Balancing long-term knowledge generation with early health benefit. JAMA 2015, 313, 2117–2118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, L.; Bramald, S.; Chapman, C.; Chu, C.; Cornelius, V.; Douglas, F.; Lucassen, A.; Nehammer, A.; Sutton, S.; Trivella, M.; et al. What motivates interest in attending a familial cancer genetics clinic? Fam. Cancer 2003, 2, 159–168. [Google Scholar] [CrossRef]
- Van den Heuvel, M.L.; Stemkens, D.; van Zelst-Stams, W.A.G.; Willeboordse, F.; Christiaans, I. How to inform at-risk relatives? Attitudes of 1379 Dutch patients, relatives, and members of the general population. J. Genet. Couns. 2020, 29, 786–799. [Google Scholar] [CrossRef] [Green Version]
- Daly, M.B.; Montgomery, S.; Bingler, R.; Ruth, K. Communicating genetic test results within the family: Is it lost in translation? A survey of relatives in the randomized six-step study. Fam. Cancer 2016, 15, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Taber, J.M.; Chang, C.Q.; Lam, T.K.; Gillanders, E.M.; Hamilton, J.G.; Schully, S.D. Prevalence and correlates of receiving and sharing high-penetrance cancer genetic test results: Findings from the health information national trends survey. Public Health Genom. 2015, 18, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Fadda, M.; Chappuis, P.O.; Katapodi, M.C.; Pagani, O.; Monnerat, C.; Membrez, V.; Unger, S.; Caiata Zufferey, M. Physicians communicating with women at genetic risk of breast and ovarian cancer: Are we in the middle of the ford between contradictory messages and unshared decision making? PLoS ONE 2020, 15, e0240054. [Google Scholar] [CrossRef] [PubMed]
- Bowen, D.J.; Hyams, T.; Laurino, M.; Woolley, T.; Cohen, S.; Leppig, K.A.; Jarvik, G. Development of FamilyTalk: An intervention to support communication and educate families about colorectal cancer risk. J. Cancer Educ. 2019, 35, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Birch, P.H. Interactive e-counselling for genetics pre-test decisions: Where are we now? Clin. Genet. 2015, 87, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Syrowatka, A.; Krömker, D.; Meguerditchian, A.N.; Tamblyn, R. Features of computer-based decision aids: Systematic review, thematic synthesis, and meta-analyses. J. Med. Internet Res. 2016, 18, e20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biesecker, B.B.; Lewis, K.L.; Umstead, K.L.; Johnston, J.J.; Turbitt, E.; Fishler, K.P.; Patton, J.H.; Miller, I.M.; Heidlebaugh, A.R.; Biesecker, L.G. Web platform vs. in-person genetic counselor for return of carrier results from exome sequencing: A randomized clinical trial. JAMA Intern. Med. 2018, 178, 338–346. [Google Scholar] [CrossRef] [Green Version]
- Otten, E.; Birnie, E.; Ranchor, A.V.; van Langen, I.M. Telegenetics use in presymptomatic genetic counselling: Patient evaluations on satisfaction and quality of care. Eur. J. Hum. Genet. 2016, 24, 513. [Google Scholar] [CrossRef]
- Buchanan, A.H.; Datta, S.K.; Skinner, C.S.; Hollowell, G.P.; Beresford, H.F.; Freeland, T.; Rogers, B.; Boling, J.; Marcom, P.K.; Adams, M.B. Randomized trial of telegenetics vs. in-person cancer genetic counseling: Cost, patient satisfaction and attendance. J. Genet. Couns. 2015, 24, 961–970. [Google Scholar] [CrossRef] [Green Version]
- Gaieski, J.B.; Patrick-Miller, L.; Egleston, B.L.; Maxwell, K.N.; Walser, S.; DiGiovanni, L.; Brower, J.; Fetzer, D.; Ganzak, A.; McKenna, D.; et al. Research participants’ experiences with return of genetic research results and preferences for web-based alternatives. Mol. Genet. Genom. Med. 2019, 7, e898. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, C.; Manheimer, E.; Glanville, J. Chapter 6: Searching for studies. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated 11); Higgins, J., Green, S., Eds.; The Cochrane Collaboration, 2011. Available online: www.cochrane-handbook.org.
- CADTH database search filters (Internet). Ottawa: CADTH; 2016. Available online: https://www.cadth.ca/resources/finding-evidence (accessed on 31 January 2021).
- Endnote,Version EndNote X9; Clarivate: Philadelphia, PA, USA, 2018.
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote [published correction appears in J Med Libr Assoc. 2017 Jan;105(1):111]. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 25 August 2020).
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions, Version 5.2.0; Cochrane: London, UK, 2017. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: Hoboken, NJ, USA, 2009; pp. 1–421. [Google Scholar]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Rosenthal, R. Meta-Analytic Procedures for Social Research; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Comprehensive Meta-Analysis, Version 3; Biostat Inc.: Englewood, NJ, USA, 2020.
- McInerney, L.A.; Biesecker, B.B.; Hadley, D.W.; Kase, R.G.; Giambarresi, T.R.; Johnson, E.; Lerman, C.; Struewing, J.P. BRCA1/2 testing in hereditary breast and ovarian cancer families: Effectiveness of problem-solving training as a counseling intervention. Am. J. Med. Genet. A 2004, 130a, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Katapodi, M.C.; Jung, M.; Schafenacker, A.M.; Milliron, K.J.; Mendelsohn-Victor, K.E.; Merajver, S.D.; Northouse, L.L. Development of a family-based intervention for BRCA carriers and their at-risk relatives: Focus groups, usability, and feasibility testing. JMIR Cancer 2018, 4, e7. [Google Scholar] [CrossRef]
- Lobb, E.; Butow, P.; Meiser, B.; Barratt, A.; Kirk, J.; Gattas, M.; Haan, E.; Tucker, K. The use of audiotapes in consultations with women from high risk breast cancer families: A randomised trial. J. Med. Genet. 2002, 39, 697–703. [Google Scholar] [CrossRef]
- Montgomery, S.V.; Barsevick, A.M.; Egleston, B.L.; Bingler, R.; Ruth, K.; Miller, S.M.; Malick, J.; Cescon, T.P.; Daly, M.B. preparing individuals to communicate genetic test results to their relatives: Report of a randomized control trial. Fam. Cancer 2013, 12, 537–546. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, C.E.; Meiser, B.; Homewood, J.; Peate, M.; Taylor, A.; Lobb, E.; Kirk, J.; Young, M.A.; Williams, R.; Dudding, T.; et al. A randomized controlled trial of a decision aid for women considering genetic testing for breast and ovarian cancer risk. Breast Cancer Res. Treat. 2008, 107, 289–301. [Google Scholar] [CrossRef]
- Bodurtha, J.N.; McClish, D.; Gyure, M.; Corona, R.; Krist, A.H.; Rodríguez, V.M.; Maibauer, A.M.; Borzelleca, J., Jr.; Bowen, D.J.; Quillin, J.M. The kinfact intervention—A randomized controlled trial to increase family communication about cancer history. J. Womens Health 2014, 23, 806–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eijzenga, W.; de Geus, E.; Aalfs, C.M.; Menko, F.H.; Sijmons, R.H.; de Haes, H.C.J.M.; Smets, E.M.A. How to support cancer genetics counselees in informing at-risk relatives? Lessons from a randomized controlled trial. Patient Educ. Couns. 2018, 101, 1611–1619. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, J.; Metcalfe, S.; Gaff, C.; Donath, S.; Delatycki, M.B.; Winship, I.; Skene, L.; Aitken, M.A.; Halliday, J. Outcomes of a randomised controlled trial of a complex genetic counselling intervention to improve family communication. Eur. J. Human Genet. 2016, 24, 356–360. [Google Scholar] [CrossRef] [Green Version]
- Roshanai, A.H.; Rosenquist, R.; Lampic, C.; Nordin, K. Does enhanced information at cancer genetic counseling improve counselees’ knowledge, risk perception, satisfaction and negotiation of information to at-risk relatives?—A randomized study. Acta Oncologica 2009, 48, 999–1009. [Google Scholar] [CrossRef]
- Dekker, N.; Hermens, R.P.; de Wilt, J.H.; van Zelst-Stams, W.A.; Hoogerbrugge, N.; Nagengast, F.; Elwyn, G.; Ligtenberg, M.; van Krieken, J.; Adang, E.; et al. Improving recognition and referral of patients with an increased familial risk of colorectal cancer: Results from a randomized controlled trial. Colorectal Dis. 2015, 17, 499–510. [Google Scholar] [CrossRef]
- Loader, S.; Shields, C.; Levenkron, J.C.; Fishel, R.; Rowley, P.T. Patient vs. physician as the target of educational outreach about screening for an inherited susceptibility to colorectal cancer. Genet. Test. 2002, 6, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Amendola, L.M.; Hart, R.; Bennette, C.S.; Heagerty, P.; Horike-Pyne, M.; Trinidad, S.B.; Rosenthal, E.A.; Comstock, B.; Nefcy, C.; et al. Clinical exome sequencing vs. usual care for hereditary colorectal cancer diagnosis: A pilot comparative effectiveness study. Contemp. Clin. Trials 2019, 84, 105820. [Google Scholar] [CrossRef] [PubMed]
- Tiller, K.; Meiser, B.; Gaff, C.; Kirk, J.; Dudding, T.; Phillips, K.A.; Friedlander, M.; Tucker, K. A randomized controlled trial of a decision aid for women at increased risk of ovarian cancer. Med. Decis. Mak. 2006, 26, 360–372. [Google Scholar] [CrossRef] [PubMed]
- Vogel, R.I.; Niendorf, K.; Petzel, S.; Lee, H.; Teoh, D.; Blaes, A.H.; Argenta, P.; Rivard, C.; Winterhoff, B.; Lee, H.Y.; et al. A patient-centered mobile health application to motivate use of genetic counseling among women with ovarian cancer: A pilot randomized controlled trial. Gynecol. Oncol. 2019, 153, 100–107. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Speilberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. State-Trait Anxiety Inventory for Adults; Mind Garden, Inc.: Redwood City, CA, USA, 1983. [Google Scholar]
- Radloff, L.S. The Ces-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Caswell-Jin, J.L.; Zimmer, A.D.; Stedden, W.; Kingham, K.E.; Zhou, A.Y.; Kurian, A.W. Cascade genetic testing of relatives for hereditary cancer risk: Results of an online initiative. J. Natl. Cancer Inst. 2019, 111, 95–98. [Google Scholar] [CrossRef]
- Peshkin, B.N.; Ladd, M.K.; Isaacs, C.; Segal, H.; Jacobs, A.; Taylor, K.L.; Graves, K.D.; O’Neill, S.C.; Schwartz, M.D. The genetic education for men (Gem) trial: Development of web-based education for untested men in BRCA1/2-positive families. J. Cancer Educ. 2019, 11, 11. [Google Scholar]
- Courtney, E.; Chok, A.K.; Ting Ang, Z.L.; Shaw, T.; Li, S.T.; Yuen, J.; Ngeow, J. Impact of free cancer predisposition cascade genetic testing on uptake in Singapore. NPJ Genom. Med. 2019, 4, 22. [Google Scholar] [CrossRef]
- Forrest, L.E.; Burke, J.; Bacic, S.; Amor, D.J. Increased genetic counseling support improves communication of genetic information in families. Genet. Med. 2008, 10, 167–172. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, S.C.; Evans, C.; Hamilton, R.J.; Peshkin, B.N.; Isaacs, C.; Friedman, S.; Tercyak, K.P. Information and support needs of young women regarding breast cancer risk and genetic testing: Adapting effective interventions for a novel population. Fam. Cancer 2018, 17, 351–360. [Google Scholar] [CrossRef]
- Evans, D.G.R.; Binchy, A.; Shenton, A.; Hopwood, P.; Craufurd, D. Comparison of proactive and usual approaches to offering predictive testing for BRCA1/2 mutations in unaffected relatives. Clin. Genet. 2009, 75, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Frey, M.K.; Kahn, R.M.; Chapman-Davis, E.; Tubito, F.; Pires, M.; Christos, P.; Anderson, S.; Mukherjee, S.; Jordan, B.; Blank, S.V.; et al. Prospective feasibility trial of a novel strategy of facilitated cascade genetic testing using telephone counseling. J. Clin. Oncol. 2020, 38, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Kardashian, A.; Fehniger, J.; Creasman, J.; Cheung, E.; Beattie, M.S. A pilot study of the sharing risk information tool (Sharit) for families with hereditary breast and ovarian cancer syndrome. Hered. Cancer Clin. Pract. 2012, 10, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrečar, I.; Hristovski, D.; Peterlin, B. Telegenetics: An update on availability and use of telemedicine in clinical genetics service. J. Med. Syst. 2017, 41, 21. [Google Scholar] [CrossRef]
- Dheensa, S.; Fenwick, A.; Shkedi-Rafid, S.; Crawford, G.; Lucassen, A. Health-care professionals’ responsibility to patients’ relatives in genetic medicine: A systematic review and synthesis of empirical research. Genet. Med. 2016, 18, 290–301. [Google Scholar] [CrossRef] [Green Version]
- Griffin, N.E.; Buchanan, T.R.; Smith, S.H.; Leon, A.A.; Meyer, M.F.; Liu, J.; Tabak, R.G.; Fuh, K.C.; Thaker, P.H.; Powell, M.A. Low rates of cascade genetic testing among families with hereditary gynecologic cancer: An opportunity to improve cancer prevention. Gynecol. Oncol. 2020, 156, 140–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menko, F.H.; ter Stege, J.A.; van der Kolk, L.E.; Jeanson, K.N.; Schats, W.; Ait Moha, D.; Bleiker, E.M.A. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: A systematic review of the literature and implications for clinical practice. Fam. Cancer 2019, 18, 127–135. [Google Scholar] [CrossRef]
- Unger, S.; Simond, E.; Davoine, E.; Katapodi, M.C. Dissemination of Genetic Information in Swiss Families with Lynch Syndrome: A Qualitative Exploratory Study. Clin. Oncol. Res. 2020, 2020, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Edwards, A.; Gray, J.; Clarke, A.; Dundon, J.; Elwyn, G.; Gaff, C.; Hood, K.; Iredale, R.; Sivell, S.; Shaw, C.; et al. Interventions to improve risk communication in clinical genetics: Systematic review. Patient Educ. Couns. 2008, 71, 4–25. [Google Scholar] [CrossRef]
- Pedrazzani, C.; Caiata-Zufferey, M.; Kaiser-Grolimund, A.; Bürki, N.; Pagani, O.; Katapodi, M.C. CN115 communication of genetic information to family members in hereditary cancers and healthcare providers’ role. Ann. Oncol. 2019, 30, v848. [Google Scholar] [CrossRef]
- Aceti, M.; Kaiser-Grolimund, A.; Pedrazzani, C.; Rudaz, M.; Baroutsou, V.; Bürki, N.; Chappuis, P.; Graffeo, R.; Monnerat, C.; Rabaglio, M.; et al. Bottom-up approach: Soliciting participants’ input for developing a digital platform to support cancer coping and family communication about hereditary cancer risks in Switzerland and Korea. In Proceedings of the 5th Annual Meeting on Personalized Breast Cancer Treatments, Basel, Switzerland, 12–13 November 2020. [Google Scholar]
- Hampel, H.; Frankel, W.L.; Martin, E.; Arnold, M.; Khanduja, K.; Kuebler, P.; Clendenning, M.; Sotamaa, K.; Prior, T.; Westman, J.A.; et al. Feasibility of screening for Lynch syndrome among patients with colorectal cancer. J. Clin. Oncol. 2008, 26, 5783–5788. [Google Scholar] [CrossRef] [PubMed]
- Hampel, H.; Frankel, W.L.; Martin, E.; Arnold, M.; Khanduja, K.; Kuebler, P.; Nakagawa, H.; Sotamaa, K.; Prior, T.W.; Westman, J. Screening for the Lynch syndrome (hereditary nonpolyposis colorectal cancer). New Engl. J. Med. 2005, 352, 1851–1860. [Google Scholar] [CrossRef] [Green Version]
- Win, A.K.; Jenkins, M.A.; Dowty, J.G.; Antoniou, A.C.; Lee, A.; Giles, G.G.; Buchanan, D.D.; Clendenning, M.; Rosty, C.; Ahnen, D.J. Prevalence and penetrance of major genes and polygenes for colorectal cancer. Cancer Epidemiol. Prev. Biomark. 2017, 26, 404–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haraldsdottir, S.; Rafnar, T.; Frankel, W.L.; Einarsdottir, S.; Sigurdsson, A.; Hampel, H.; Snaebjornsson, P.; Masson, G.; Weng, D.; Arngrimsson, R. Comprehensive population-wide analysis of Lynch syndrome in Iceland reveals founder mutations in Msh6 and Pms2. Nat. Commun. 2017, 8, 1–11. [Google Scholar] [CrossRef]
- Departments of Labor, Health and Human Services and the Treasury Genetic Information Nondiscrimination Act of 2008. Available online: https://www.dol.gov/agencies/ebsa/laws-and-regulations/laws/gina (accessed on 27 January 2021).
- Schwiter, R.; Kulchak Rahm, A.; Williams, J.L.; Curry Sturm, A. How can we reach at-risk relatives? Efforts to enhance communication and cascade testing uptake: A mini-review. Curr. Genet. Med. Rep. 2018, 6, 21–27. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Syndrome/Outcomes * | Intervention | Control | Theoretical Framework | Mode of Delivery | Intervener | Dose | Duration | Fidelity |
|---|---|---|---|---|---|---|---|---|---|
| Bodurtha et al., 2014 [46], KinFact | Both/Communication | Booklet (27-page personalized information for family communication about cancer and cancer genetics) | Pamphlet—breast, colon cancer risks, screening, services | Health Belief Model; Buckman’s 6-step strategy Breaking Bad News | Booklet/PamphletFace-to-face One-on-one | Trained Personnel | Once | 20-min | NR~ |
| Dekker et al., 2015 [50] | CRC **/Communication Cascade testing Knowledge | Website (CRC risk, risk calculators, decision aid) + Brochure (familial CRC risk, prevention) + 30-min Clinician education + Referral cards (criteria) | Usual care | NR | Website + Brochure | Self-administered | NR | NR | 67% used website |
| Eijzenga et al., 2018 [47] | Both/Communication Knowledge Perceived risk | Standard genetic counseling + Phone call—motivational interviewing (enhance family communication, knowledge, motivation, self-efficacy, solutions) | Standard genetic counseling | Motivational interviewing | Telephone | Psychosocial Worker | Once | NR | 33% random check interview recording |
| Hodgson et al., 2016 [48] | Multiple incl. HBOC + LSCascade testing | Enhanced genetic counseling over telephone with emphasis on family communication + Pedigree | Pedigree | NR | Telephone One-on-one | Genetic Counselors | 2–3 times | 12 months | NR |
| Katapodi et al., 2018 [42] Family Gene Toolkit | HBOC/CommunicationKnowledge Perceived risk | Webinar (power point, live presentations about cancer genetics, risk, genetic counseling, coping, family communication) + Decision aid + Communication skills building + Phone call | Wait-listed control | Theory of Stress and Coping | Web-based + Telephone Face-to-face One-on-family + One-on-one | Genetic Counselor + Master’s Oncology Nurse | 2 webinars 45–60 min per webinar + 20 min phone call | 3 weeks 110–140 min | 71% completion rate |
| Loader et al., 2002 [51] | CRC/Cascade testing | Brochure (hereditary cancer, risk factors, prevention, genetic testing, family communication) + Invitation to counseling + Letter genetic counseling | Physician education (CRC risk, information about referrals to counseling) | NR | Brochure + Letter Face-to-face One-on-one | Mail, Self-administered | Once | NR | 47% counseled |
| Lobb et al., 2002 [43] | HBOC/Anxiety Depression | Audio-recording of genetic consultation | Usual care | NR | Audiotapes | Self-administered | NR | NR | 51% listened tape once |
| McInerney-Leo et al., 2004 *** [41] | HBOC | Family education + Problem Solving Training (expectations, concerns, feelings) for task- and emotional-focused coping and problem solving + Telephone interview | Family education + Client-centered counseling + Telephone interview | Cognitive–Behavioral Theory | Face-to-face or TelephoneOne-on-family + One-on-one | Trained Provider | Once | 60 min | Standardized protocol |
| Montgomery et al., 2013 [44] | HBOC/Communication Depression | Counseling (risk factors, personal risk, pedigree) + Communication skills building (who, how, extent willing to know, share results, emotional responses, resources) | Wellness education (nutrition, exercise) + List of nutrition websites | Buckman’s 6-step strategy Breaking Bad News + Theory of Planned Behavior | Face-to-face One-on-one | Genetic Counselor + Research Staff | NR | NR | NR |
| Niu et al., 2019 [52] | CRC/Communication Anxiety Depression | Genetic counseling + Clinical exome sequencing (21 to >50 actionable genes) + Additional genetic information | Counseling + Tumor testing OR panel testing + Review family history | NR | Telephone or Face-to-faceOne-on-one | Genetic Counselor or Geneticist | NR | NR | NR |
| Roshanai et al., 2009 [49] | Both/Communication Knowledge Anxiety DepressionPerceived risk | Genetic counseling + Extended meeting nurse specialist (pedigree, cancer risk, 6-step strategy for family communication) + Pamphlet + Videotape of counseling + Copies pedigree, medical records | Genetic counseling + Short meeting nurse specialist (intention inform relatives) + Videotape of counseling | Buckman’s 6-step strategy Breaking Bad News | Clinical settingFace-to-face One-on-one | Genetic Counselor + Nurse Specialist | Once | NR | 19-item survey counselees |
| Tiller et al., 2006 [53] | Ovarian Cancer/Knowledge Anxiety | Decision aid (booklet on risk factors, family history and risk, genetic testing, prevention) + Values clarification | General education pamphlet | Ottawa Decision Support Framework | Pamphlet | Self-administered | Once | NR | 88% review booklet |
| Vogel et al., 2019 [54]mAGIC | Ovarian cancer/Communication Cascade testing Knowledge | Mobile app tailored messages (motivation, positive feedback, triggers) + Videos (genetic counseling, testing, personal health, cancer genetics, self-care, self-efficacy) + Training how to use mAGIC + Pamphlet (ovarian cancer risk, counseling, services) | Usual care + Pamphlet (hereditary cancer risk, counseling, services) | Health Belief Model + Fogg Behavioral Model of Mobile Persuasion | Mobile app + Pamphlet | Self-administered | Once per day10–15 min per day | 7 days70–90 min | NR |
| Wakefield et al., 2008 [45] | HBOC/Cascade testing Knowledge | Decision aid (40-page booklet, hereditary cancer, testing, impact on individual and family) + Values clarification | Pamphlet (4-page education about HBOC genetic testing) | Ottawa Decision Support Framework | Brochure/Pamphlet | Self-administered | NR | NR | 70% intervention read booklet |
| Author/Year Country | Setting | Sample N | Cancer Type/Stage/PDx * | Carrier of PV ** or FH *** | Age Mean ± SD or Range | Sex | Race | Education% ≤ HS^ | Enrollment | Attrition |
|---|---|---|---|---|---|---|---|---|---|---|
| Bodurtha et., al 2014 [46], USA | Outpatient | 490 | Stage/type NR: HBOC or CRC risk | 75% FDR+ any cancer 10% FH breast or CRC | 33.4 ± 11.9 | 100% female | 59% Black 33% White 8% Other/Multiple | 41% 16% missing | 61% | 42% |
| Dekker et al., 2015 [50], Netherlands | Hospital | 384 | 100% CRC I: 86.4% Stage I–III C: 86.55 Stage I–III | I: 9% high risk C:13% high risk | I: 60 ± 8.2 C: 59 ± 7.5 | I: 71% male C: 66% male | NR~ | NR | 55% | 59% |
| Eijzenga et al., 2018 [47], Netherlands | Hospital | 305 | Stage/type NR; HBOC or CRC risk I: 70% PDx C: 73% PDx | I: 9% PV C: 12% PV | I: 53.1 ± 10.1 C: 54.4 ± 12.4 | I: 75% female C:75% female | NR | I: 36%C: 30% | 90% | 21% |
| Hodgson et al., 2016 [48], Australia | Hospital and Genetic Clinic | 95 | Stage/type NR; HBOC and LS | I: 57.8% “actionable” groupC: 50.0% “actionable” group | I: 49.5 ± 14.9 C: 45.8 ± 13.9 | I: 50% female C:48% female | NR | NR | 57% | 53% |
| Katapodi et al., 2018 [42], USA | Outpatient | 24 | Stage/type NR: HBOC 40% PDx Breast 10% PDx Ovarian 20% PDx Other | 12 PV | 41 ± 13 | 100% female | 100% White | NR | 23% | 29% |
| Loader et al., 2002 [51], USA | Cancer Registry | 101 | 100% PDxCRC; stage NR | 100% ≥1 FDR or SDR++ CRC | Not Counseled: 57.3 ± 6.9 Counseled:59.2 ± 6.5 | 53% female | 93% White | NR | 71% | 13% |
| Lobb et al., 2002 [43], Australia | Outpatient | 193 | Stage/type NR; HBOC I: 42% PDx C: 45% PDx | NR | I: 45 C: 44 | 100% female | NR | I: 47% C: 50% | 88% | 18% |
| McInerney-Leo et al., 2004 [41], USA | NR | 262 | Stage/type NR; HBOC families | 26% PV 85% genetic testing | 55% ≥ 40 | 65% female | Mostly White | NR | 47% | 19% |
| Montgomery et al., 2013 [44], USA | Outpatient | 422 | Stage/type NR; HBOC | NR | 48.5 ± 11.0 | 100% female | 95% White | 77% | 96% | 41% |
| Niu et al., 2019 [52], USA | Outpatient | 190 | I: 33.68% CRC PDx C: 36.84% CRC PDx | NR | I: 53.4 ± 12.5 C: 51.8 ± 14.0 | I: 46% female C:57% female | I: 81% White C: 84% White | NR | NR | 26% |
| Roshanai et al., 2009 [49], Sweden | Outpatient | 147 | HBOC, CRC riskI: 38.36% PDxC: 35.14% PDx | I: 77% No PDx >20%risk 79% PDx >20% risk C:81% No PDx >20% risk 70% PDx >20% risk | 56 (23-84) | I: 92% female C: 89% female | NR | NR | 66% | 15% |
| Tiller et al., 2006 [53], Australia | Outpatient | 131 | Ovarian cancer I: 51.5% PDx C: 52.4% PDx | I: 74.2% FH C: 71.4% FH | I: 45.8 C: 46.3 | 100% female | NR | I: 29% C:29% | 92% | 17% |
| Vogel et al., 2019 [54], USA | Outpatient | 104 | Ovarian cancer 100% PDx I: ≥74% Stage III C: ≥75% Stage III | NR | I: 60.9 ± 10.7 C: 61 ± 12 | 100% female | I: 91% White C: 88% White | I: 20.8% C: 18% | 82% | 13% |
| Wakefield et., al 2008 [45], Australia | Outpatient | 120 | Type NR; HBOC I:56.1% PDx C:65.1% PDx | 100% FH HBOC—cancer | I: 45.8 (21–73) C: 49.6 (22–75) | 100% female | NR | I: 26.3% C: 36.5% | 94% | 17% |
| Outcomes | Number of Trials | Overall Sample N | Pooled Effect Size Hedges’ g (95% CI) | Q for Heterogeneity | Egger’s t-Test for Publication Bias |
|---|---|---|---|---|---|
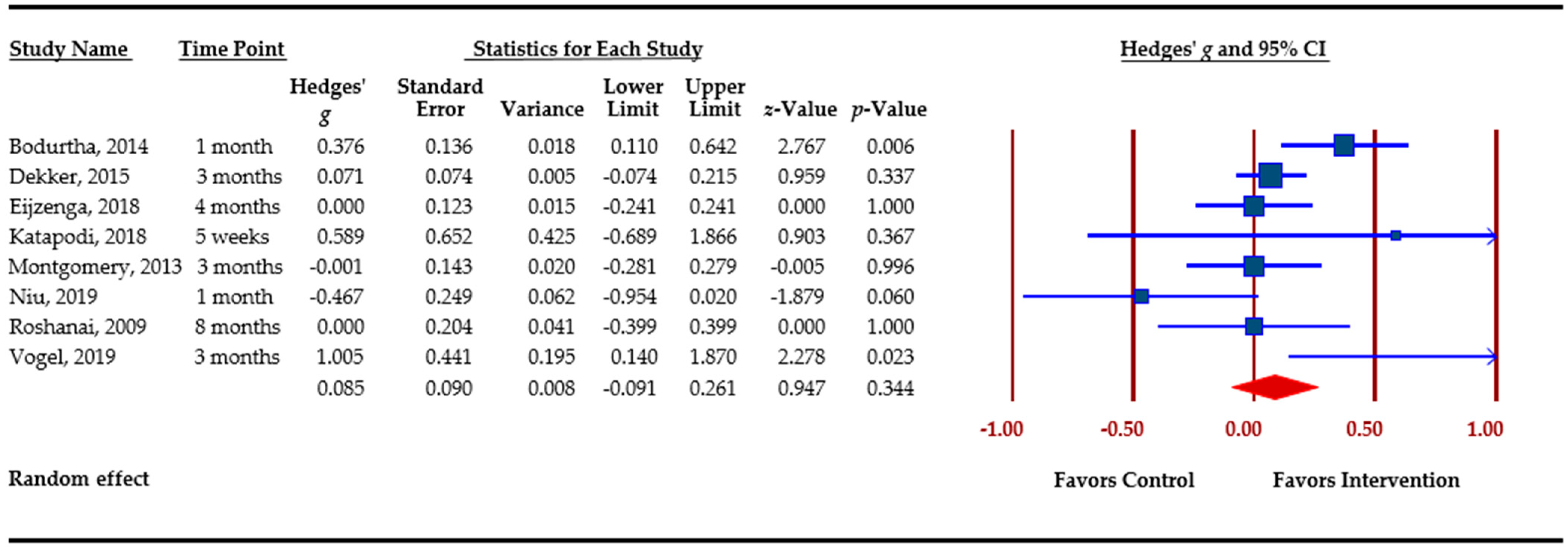
| Family communication | 8 | 2066 | 0.085 (−0.091 – 0.261) | 15.50* | 0.53 |
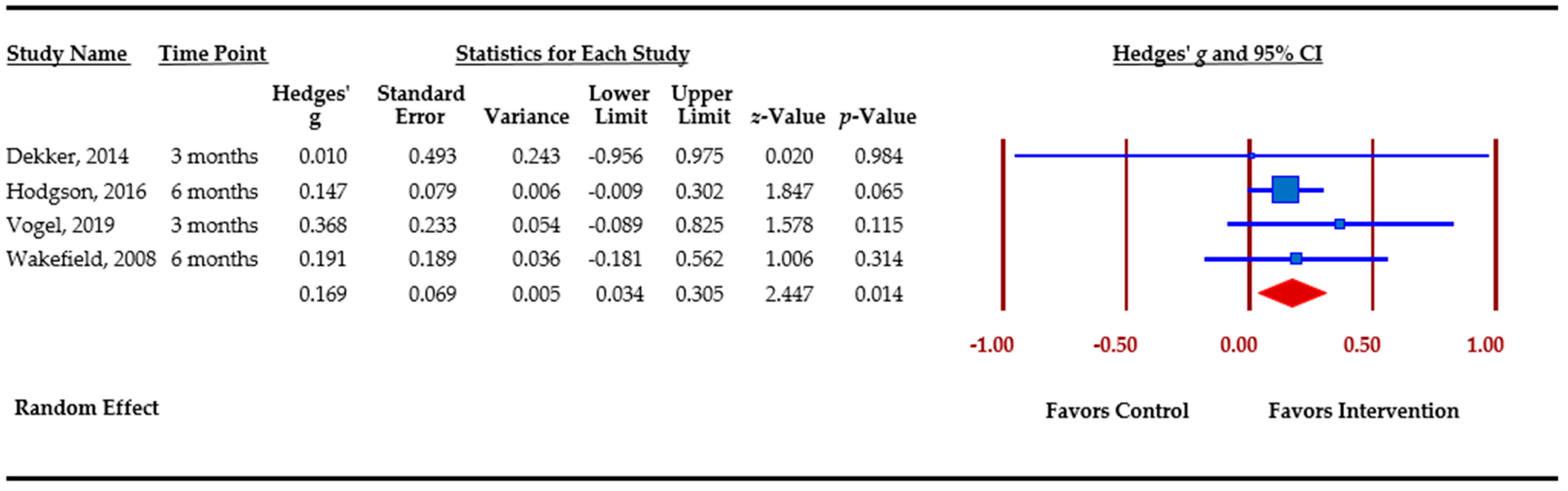
| Cascade genetic testing | 4 | 703 | 0.169 (0.034 – 0.305)* | 0.93 | −0.66 |
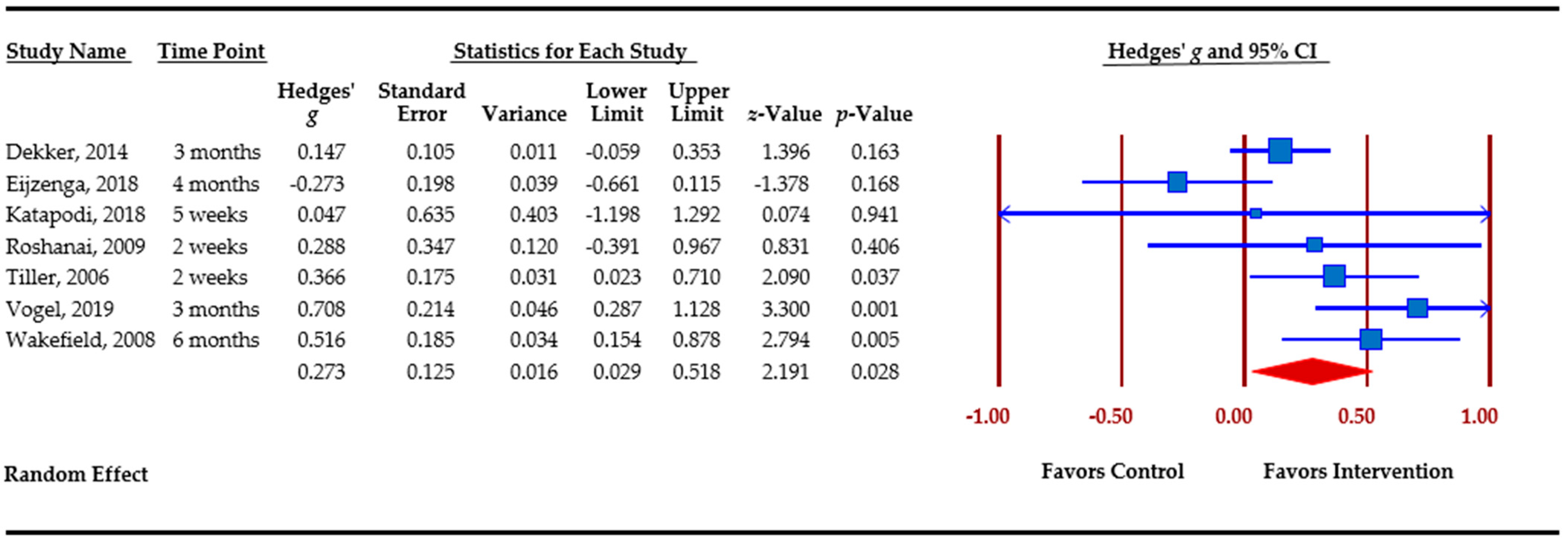
| Knowledge | 7 | 1215 | 0.244 (0.109 – 0.379)* | 15.10 * | 0.50 |
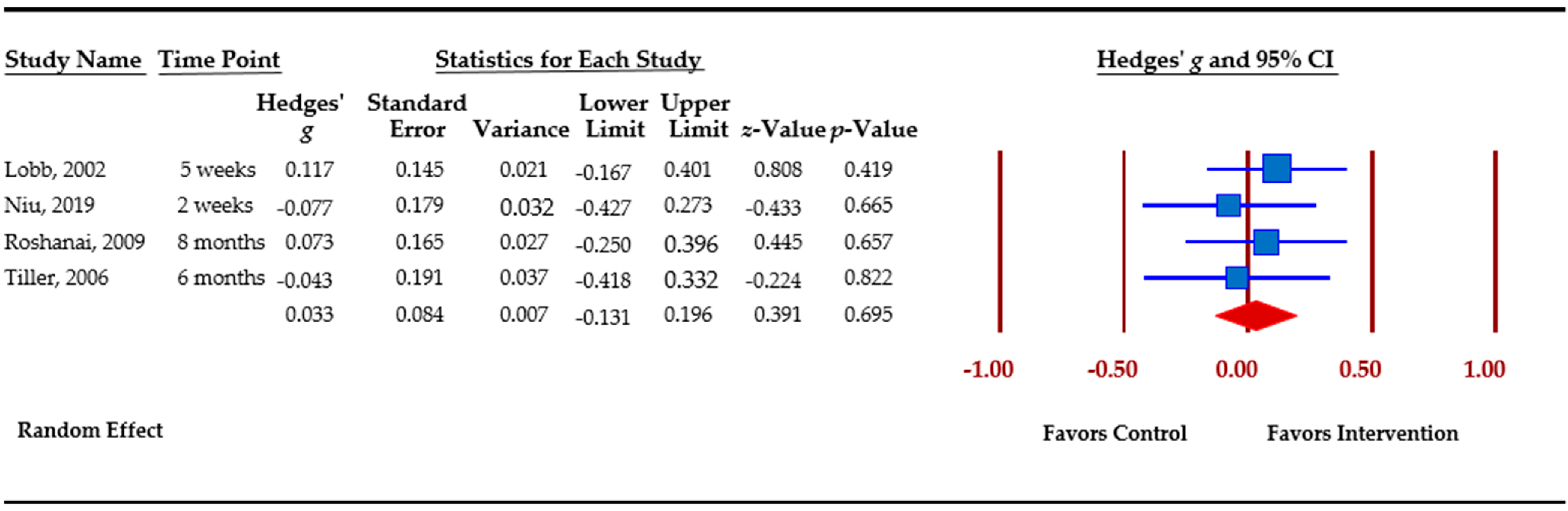
| Anxiety | 4 | 661 | 0.033 (−0.132 – 0.198) | 6.14 | −4.17* |
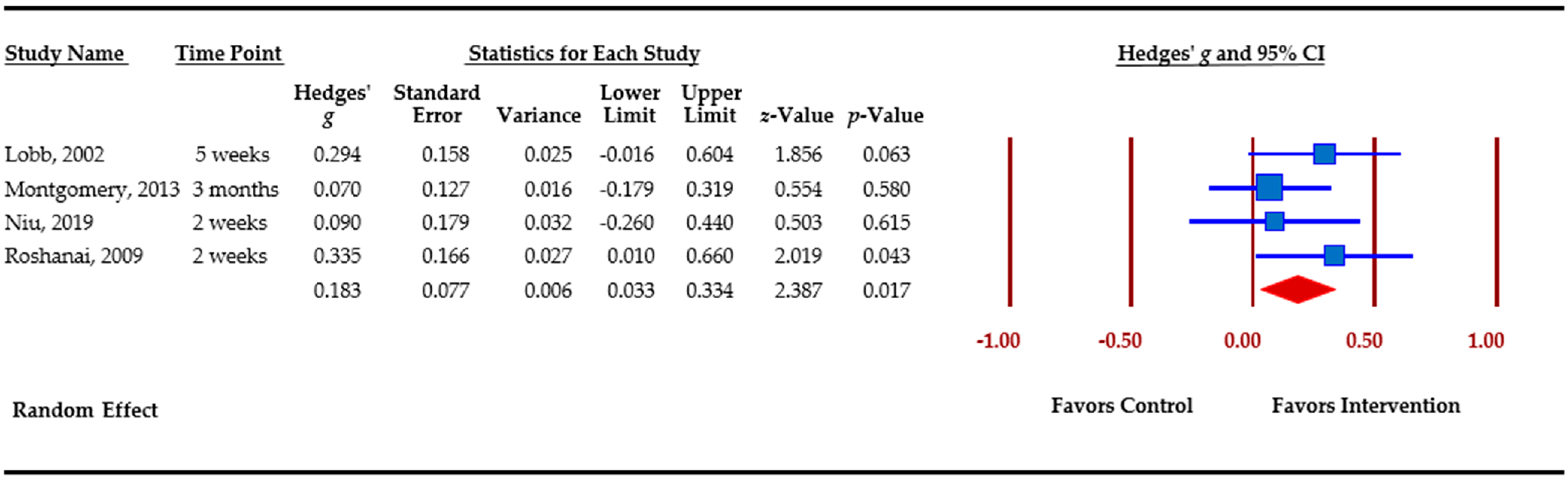
| Depression | 4 | 952 | 0.183 (0.033 – 0.334)* | 2.39 | 2.89 |
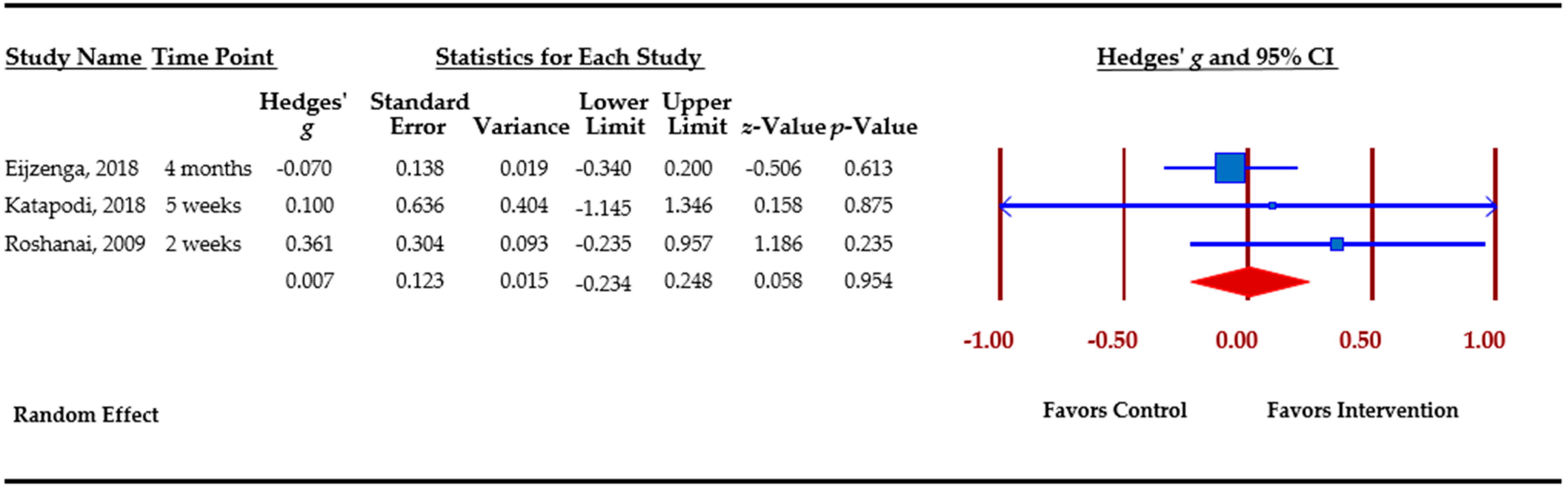
| Risk perception | 3 | 476 | 0.007 (−0.230 – 0.250) | 1.69 | 0.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baroutsou, V.; Underhill-Blazey, M.L.; Appenzeller-Herzog, C.; Katapodi, M.C. Interventions Facilitating Family Communication of Genetic Testing Results and Cascade Screening in Hereditary Breast/Ovarian Cancer or Lynch Syndrome: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 925. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040925
Baroutsou V, Underhill-Blazey ML, Appenzeller-Herzog C, Katapodi MC. Interventions Facilitating Family Communication of Genetic Testing Results and Cascade Screening in Hereditary Breast/Ovarian Cancer or Lynch Syndrome: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(4):925. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040925
Chicago/Turabian StyleBaroutsou, Vasiliki, Meghan L. Underhill-Blazey, Christian Appenzeller-Herzog, and Maria C. Katapodi. 2021. "Interventions Facilitating Family Communication of Genetic Testing Results and Cascade Screening in Hereditary Breast/Ovarian Cancer or Lynch Syndrome: A Systematic Review and Meta-Analysis" Cancers 13, no. 4: 925. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040925