
Adverse Event Reporting with Immune Checkpoint Inhibitors in Older Patients: Age Subgroup Disproportionality Analysis in VigiBase

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. VigiBase
2.2. Study Design
2.3. Disproportionality Analysis
2.4. Safety Assessment of Signals of Disproportionate Reporting in Specific Age Subgroups
3. Results
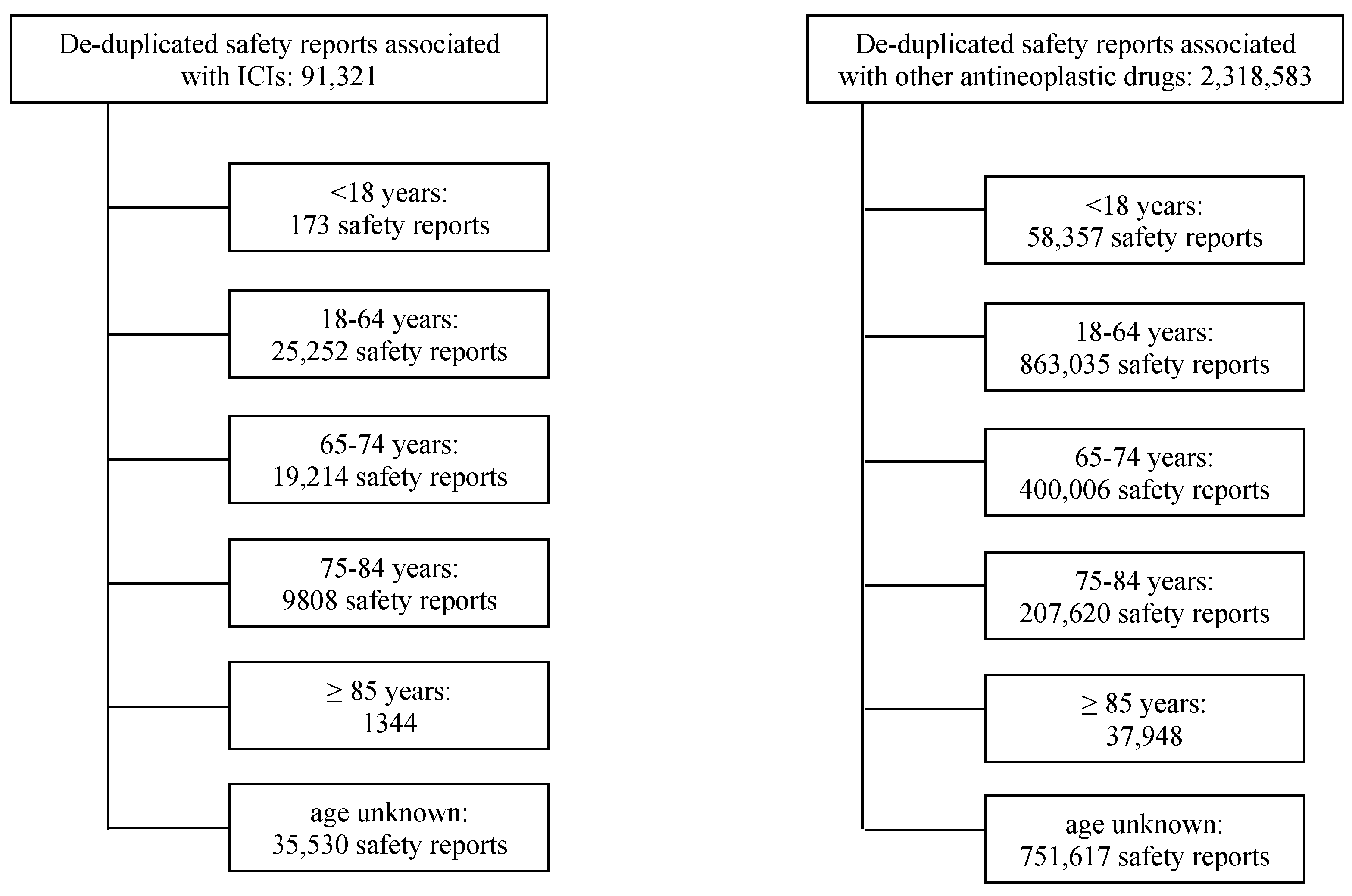
3.1. Descriptive Analysis of ICI-Related Safety Reports by Age Subgroups
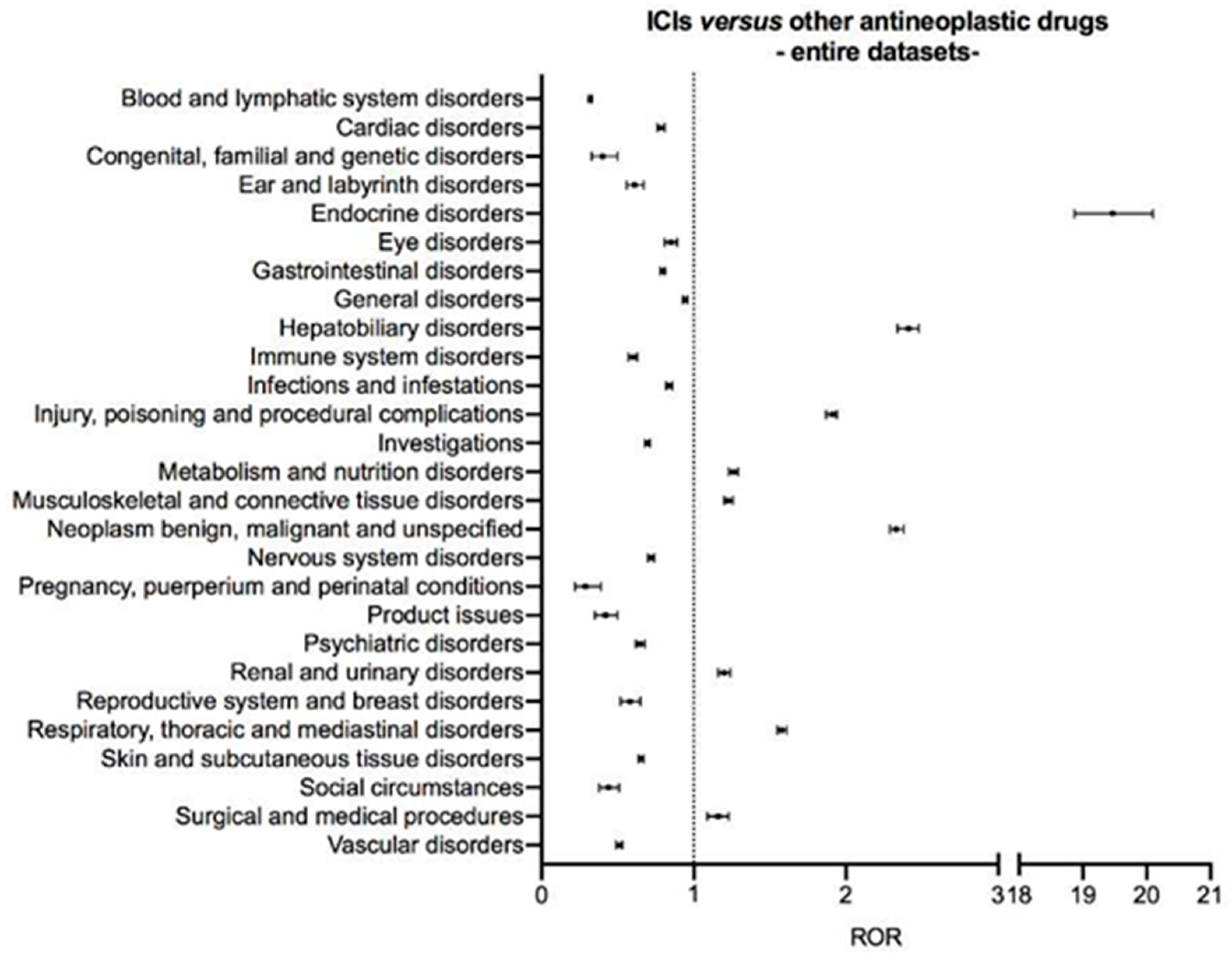
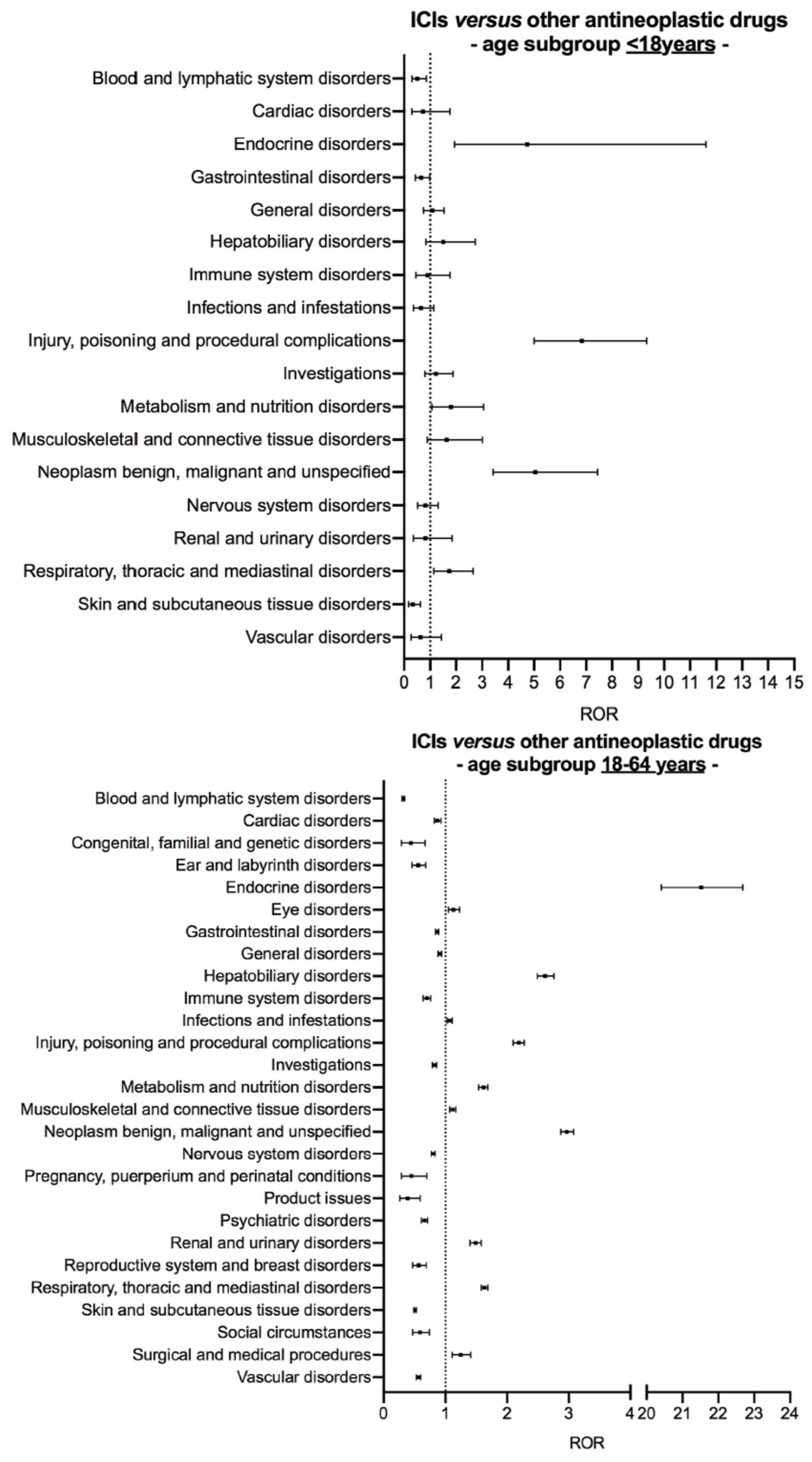
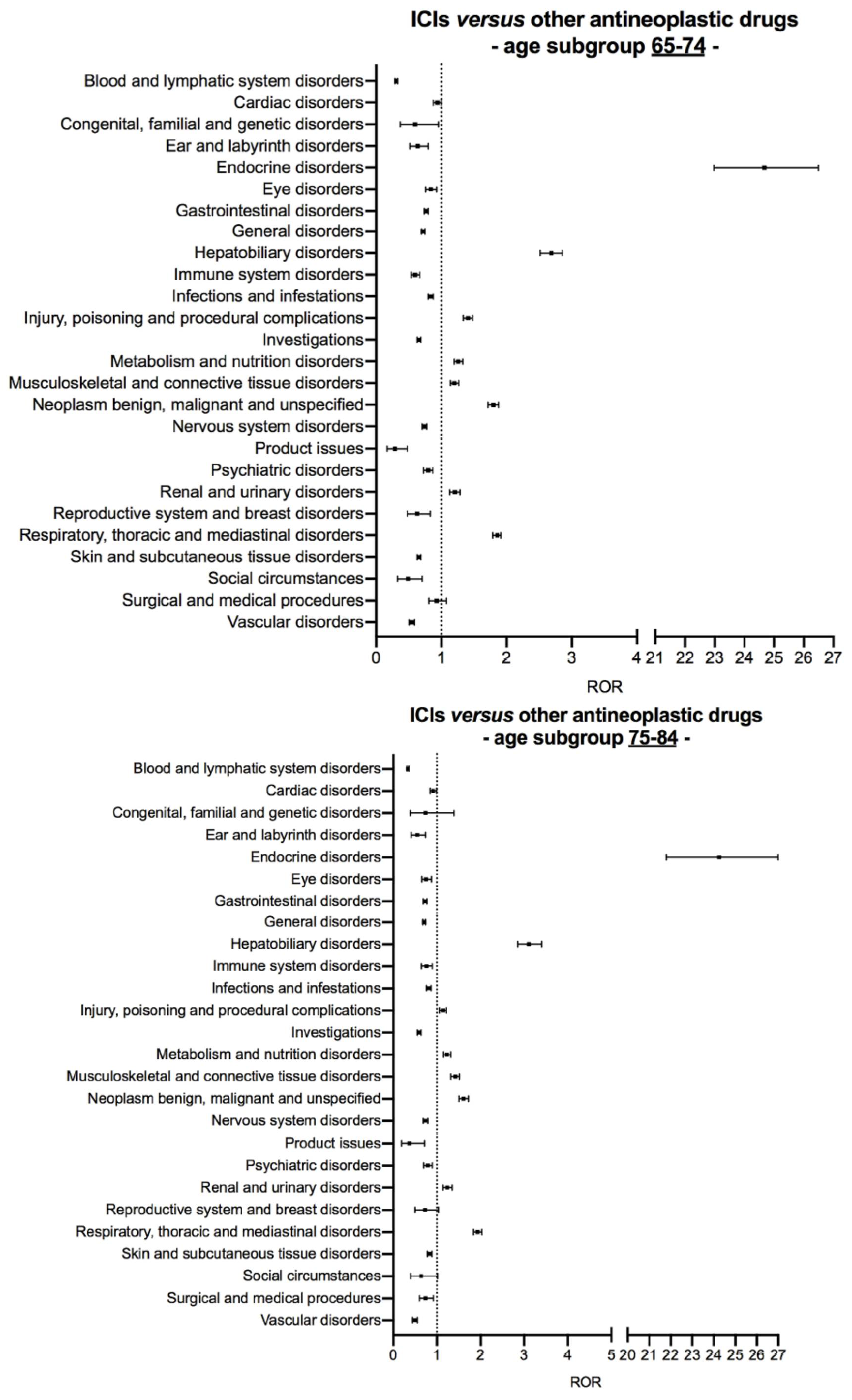
3.2. Disproportionality Analysis
3.3. Signal of Disproportionate Reporting for ICI-Related Eye Disorders in the Age Subgroup 18–64 Years
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ribas, A.; Wolchok, J.D. Cancer Immunotherapy Using Checkpoint Blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in Previously Untreated Melanoma without BRAF Mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Casals, M.; Brahmer, J.R.; Callahan, M.K.; Flores-Chávez, A.; Keegan, N.; Khamashta, M.A.; Lambotte, O.; Mariette, X.; Prat, A.; Suárez-Almazor, M.E. Immune-related Adverse Events of Checkpoint Inhibitors. Nat. Rev. Dis. Primers. 2020, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Fulop, T.; Larbi, A.; Dupuis, G.; Le Page, A.; Frost, E.H.; Cohen, A.A.; Witkowski, J.M.; Franceschi, C. Immunosenescence and Inflamm-aging as Two Sides of the Same Coin: Friends or Foes? Front. Immunol. 2018, 8, 1960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, J.M.; Fessele, K.L.; Steiner, J.; Seidl-Rathkopf, K.; Carson, K.R.; Nussbaum, N.C.; Yin, E.S.; Adelson, K.B.; Presley, C.J.; Chiang, A.C.; et al. Speed of Adoption of Immune Checkpoint Inhibitors of Programmed Cell Death 1 Protein and Comparison of Patient Ages in Clinical Practice Versus Pivotal Clinical Trials. JAMA Oncol. 2018, 4, e180798. [Google Scholar] [CrossRef] [PubMed]
- Dunn, C.; Wilson, A.; Sitas, F. Older Cancer Patients in Cancer Clinical Trials are Underrepresented. Systematic Literature Review of Almost 5000 Meta- and Pooled Analyses of Phase III Randomized Trials of Survival from Breast, Prostate and Lung Cancer. Cancer Epidemiol. 2017, 51, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Rai, R.; McQuade, J.L.; Wang, D.Y.; Park, J.J.; Nahar, K.; Sosman, J.A.; Beckermann, K.E.; Haydu, L.E.; Lo, S.; Rubinstein, S.; et al. 1113PD - Safety and Efficacy of Anti-PD-1 Antibodies in Elderly Patients with Metastatic Melanoma. Ann. Oncol. 2016, 27, 379–400. [Google Scholar] [CrossRef] [Green Version]
- Spigel, D.R.; McCleod, M.; Jotte, R.M.; Einhorn, L.; Horn, L.; Waterhouse, D.M.; Creelan, B.; Babu, S.; Leighl, N.B.; Chandler, J.C.; et al. Safety, Efficacy, and Patient-reported Health-related Quality of Life and Symptom Burden with Nivolumab in Patients with Advanced Non-small Cell Lung Cancer, Including Patients Aged 70 Years or Older or with Poor Performance Status (CheckMate 153). J. Thorac. Oncol. 2019, 14, 1628–1639. [Google Scholar] [CrossRef]
- Betof, A.S.; Nipp, R.D.; Giobbie-Hurder, A.; Johnpulle, R.A.N.; Rubin, K.; Rubinstein, S.M.; Flaherty, K.T.; Lawrence, D.P.; Johnson, D.B.; Sullivan, R.J. Impact of Age on Outcomes with Immunotherapy for Patients with Melanoma. Oncologist 2017, 22, 963–971. [Google Scholar] [CrossRef] [Green Version]
- Archibald, W.J.; Victor, A.I.; Strawderman, M.S.; Maggiore, R.J. Immune Checkpoint Inhibitors in Older Adults with Melanoma or Cutaneous Malignancies: The Wilmot Cancer Institute Experience. J. Geriatr. Oncol. 2020, 11, 496–502. [Google Scholar] [CrossRef]
- Samani, A.; Zhang, S.; Spiers, L.; Mohamed, A.A.; Merrick, S.; Tippu, Z.; Payne, M.; Faust, G.; Papa, S.; Fields, P.; et al. Impact of Age on the Toxicity of Immune Checkpoint Inhibition. J. Immunother. Cancer. 2020, 8, e000871. [Google Scholar] [CrossRef] [PubMed]
- Ridolfi, L.; De Rosa, F.; Petracci, E.; Tanda, E.T.; Marra, E.; Pigozzo, J.; Marconcini, R.; Guida, M.; Cappellini, G.C.A.; Gallizzi, G.; et al. Anti-PD1 Antibodies in Patients Aged ≥ 75 Years with Metastatic Melanoma: A Retrospective Multicentre Study. J. Geriatr. Oncol. 2020, 11, 515–522. [Google Scholar] [CrossRef]
- van Holstein, Y.; Kapiteijn, E.; Bastiaannet, E.; van den Bos, F.; Portielje, J.; de Glas, N.A. Efficacy and Adverse Events of Immunotherapy with Checkpoint Inhibitors in Older Patients with Cancer. Drugs Aging. 2019, 36, 927–938. [Google Scholar] [CrossRef] [Green Version]
- Baldini, C.; Romano, P.M.; Voisin, A.L.; Danlos, F.X.; Champiat, S.; Laghouati, S.; Kfoury, M.; Vincent, H.; Postel-Vinay, S.; Varga, A.; et al. Impact of Aging on Immune-related Adverse Events Generated by Anti-programmed Death (Ligand)PD-(L)1 Therapies. Eur. J. Cancer. 2020, 129, 71–79. [Google Scholar] [CrossRef]
- Raschi, E.; Mazzarella, A.; Antonazzo, I.C.; Bendinelli, N.; Forcesi, E.; Tuccori, M.; Moretti, U.; Poluzzi, E.; De Ponti, F. Toxicities with Immune Checkpoint Inhibitors: Emerging Priorities from Disproportionality Analysis of the FDA Adverse Event Reporting System. Target Oncol. 2019, 14, 205–221. [Google Scholar] [CrossRef]
- Sandberg, L.; Taavola, H.; Aoki, Y.; Chandler, R.; Norén, G.N. Risk Factor Considerations in Statistical Signal Detection: Using Subgroup Disproportionality to Uncover Risk Groups for Adverse Drug Reactions in VigiBase. Drug Saf. 2020, 43, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, M. VigiBase, the WHO Global ICSR Database System: Basic Facts. Drug Inf. J. 2008, 42, 409–419. [Google Scholar] [CrossRef]
- Califano, R.; Gomes, F.; Ackermann, C.J.; Rafee, S.; Tsakonas, G.; Ekman, S. Immune Checkpoint Blockade for Non-small Cell Lung Cancer: What is the Role in the Special Populations? Eur. J. Cancer. 2020, 125, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Gatti, M.; Gelsomino, F.; Ardizzoni, A.; Poluzzi, E.; De Ponti, F. Lessons to be Learnt from Real-world Studies on Immune-related Adverse Events with Checkpoint Inhibitors: A Clinical Perspective from Pharmacovigilance. Target Oncol. 2020, 15, 449–466. [Google Scholar] [CrossRef]
- Del Castillo, M.; Romero, F.A.; Argüello, E.; Kyi, C.; Postow, M.A.; Redelman-Sidi, G. The Spectrum of Serious Infections Among Patients Receiving Immune Checkpoint Blockade for the Treatment of Melanoma. Clin. Infect. Dis. 2016, 63, 1490–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redelman-Sidi, G.; Michielin, O.; Cervera, C.; Ribi, C.; Aguado, J.M.; Fernández-Ruiz, M.; Manuel, O. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the Safety of Targeted and Biological Therapies: An Infectious Diseases Perspective (Immune Checkpoint Inhibitors, Cell Adhesion Inhibitors, Sphingosine-1-phosphate Receptor Modulators and Proteasome Inhibitors). Clin. Microbiol. Infect. 2018, 24 (Suppl. 2), S95–S107. [Google Scholar]
- Kim, Y.J.; Lee, J.S.; Lee, J.; Lee, S.C.; Kim, T.I.; Byeon, S.H.; Lee, C.S. Factors Associated with Ocular Adverse Event after Immune Checkpoint Inhibitor Treatment. Cancer Immunol. Immunother. 2020, 69, 2441–2452. [Google Scholar] [CrossRef]
- Noble, C.W.; Gangaputra, S.S.; Thompson, I.A.; Yuan, A.; Apolo, A.B.; Lee, J.M.; Papaliodis, G.N.; Kodati, S.; Bishop, R.; Magone, M.T.; et al. Ocular Adverse Events Following Use of Immune Checkpoint Inhibitors for Metastatic Malignancies. Ocul. Immunol. Inflamm. 2020, 28, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Dow, E.R.; Yung, M.; Tsui, E. Immune Checkpoint Inhibitor-associated Uveitis: Review of Treatments and Outcomes. Ocul. Immunol. Inflamm. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fang, T.; Maberley, D.A.; Etminan, M. Ocular Adverse Events with Immune Checkpoint Inhibitors. J. Curr. Ophthalmol. 2019, 31, 319–322. [Google Scholar] [CrossRef]
- Seabroke, S.; Candore, G.; Juhlin, K.; Quarcoo, N.; Wisniewski, A.; Arani, R.; Painter, J.; Tregunno, P.; Norén, G.N.; Slattery, J. Performance of Stratified and Subgrouped Disproportionality Analyses in Spontaneous Databases. Drug Saf. 2016, 39, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Pearson, R.K.; Hauben, M.; Goldsmith, D.I.; Gould, A.L.; Madigan, D.; O’Hara, D.J.; Reisinger, S.J.; Hochberg, A.M. Influence of the MedDRA Hierarchy on Pharmacovigilance Data Mining Results. Int. J. Med. Inform. 2009, 78, e97–e103. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | <18 Years (N = 173) | 18–64 Years (N = 25,252) | 65–74 Years (N = 19,214) | 75–84 Years (N = 9808) | ≥85 Years (N = 1344) |
|---|---|---|---|---|---|
| Median age (IQR), years | 12 (5–15) | 56 (49–61) | 69 (67–72) | 78 (76–80) | 87 (85–88) |
| Patient sex | |||||
| Male | 94 (54.3) | 14,530 (57.5) | 12,850 (66.9) | 6627 (67.6) | 828 (61.6) |
| Female | 74 (42.8) | 10,236 (40.5) | 6038 (31.4) | 3009 (30.7) | 486 (36.2) |
| Not reported | 5 (2.9) | 486 (1.9) | 326 (1.7) | 172 (1.8) | 30 (2.2) |
| Reporting country | |||||
| North America | 84 (48.6) | 9830 (38.9) | 6005 (31.3) | 2991 (30.5) | 586 (43.6) |
| South America | 16 (9.2) | 379 (1.5) | 215 (1.1) | 97 (1.0) | 17 (1.3) |
| Europe | 50 (28.9) | 9042 (35.8) | 6416 (33.4) | 3238 (33.0) | 413 (30.7) |
| Asia | 18 (10.4) | 5107 (20.2) | 5963 (31.0) | 3186 (32.5) | 278 (20.7) |
| Oceania | 3 (1.7) | 734 (2.9) | 564 (2.9) | 282 (2.9) | 49 (3.6) |
| Africa | 2 (1.2) | 160 (0.6) | 51 (0.3) | 14 (0.1) | 1 (0.1) |
| Reporting year | |||||
| 2008 | - | 8 (0) | - | - | - |
| 2009 | - | 26 (0.1) | 1 (0) | 3 (0) | - |
| 2010 | - | 32 (0.1) | 5 (0) | 3 (0) | - |
| 2011 | - | 114 (0.5) | 46 (0.2) | 18 (0.2) | 1 (0.1) |
| 2012 | 5 (2.9) | 397 (1.6) | 185 (1.0) | 92 (0.9) | 14 (1.0) |
| 2013 | 1 (0.6) | 311 (1.2) | 163 (0.8) | 59 (0.6) | 8 (0.6) |
| 2014 | 8 (4.6) | 696 (2.8) | 299 (1.6) | 177 (1.8) | 29 (2.2) |
| 2015 | 9 (5.2) | 1597 (6.3) | 910 (4.7) | 397 (4.0) | 60 (4.5) |
| 2016 | 14 (8.1) | 2415 (9.6) | 1623 (8.4) | 766 (7.8) | 100 (7.4) |
| 2017 | 32 (18.5) | 4090 (16.2) | 3245 (16.9) | 1627 (16.6) | 220 (16.4) |
| 2018 | 42 (24.3) | 5790 (22.9) | 4792 (24.9) | 2435 (24.8) | 334 (24.9) |
| 2019 | 34 (19.7) | 6613 (26.2) | 5739 (29.9) | 3092 (31.5) | 402 (29.9) |
| 2020 (up to 30 August) | 28 (16.2) | 3163 (12.5) | 2206 (11.5) | 1139 (11.6) | 176 (13.1) |
| Reporter qualification | |||||
| Physician | 71 (41.0) | 13,175 (52.2) | 11,624 (60.5) | 6066 (61.8) | 732 (54.5) |
| Other Health Professional | 59 (34.1) | 6227 (24.7) | 3705 (19.3) | 1766 (18.0) | 231 (17.2) |
| Consumer/Non Health Professional | 27 (15.6) | 3457 (13.7) | 1985 (10.3) | 958 (9.8) | 225 (16.7) |
| Pharmacist | 11 (6.4) | 1668 (6.6) | 1380 (7.2) | 755 (7.7) | 112 (8.3) |
| Lawyer | - | 10 (0) | 6 (0) | 2 (0) | - |
| Not reported | 5 (2.9) | 715 (2.8) | 514 (2.7) | 261 (2.7) | 44 (3.3) |
| Seriousness | |||||
| Yes | 135 (78.0) | 20,291 (80.4) | 15,630 (81.3) | 7985 (81.4) | 1046 (77.8) |
| Caused/prolonged hospitalization | 42 (24.3) | 8541 (33.8) | 6958 (36.2) | 3491 (35.6) | 406 (30.2) |
| Death | 29 (16.8) | 4214 (16.7) | 3226 (16.8) | 1838 (18.7) | 290 (21.6) |
| Disabling/incapacitating | 2 (1.2) | 185 (0.7) | 178 (0.9) | 84 (0.9) | 12 (0.9) |
| Life threatening | 11 (6.4) | 1054 (4.2) | 873 (4.5) | 438 (4.5) | 47 (3.5) |
| Congenital anomaly/birth defect | - | 8 (0) | - | 1 (0) | - |
| Other medically important condition | 51 (29.5) | 6264 (24.8) | 4386 (22.8) | 2132 (21.7) | 290 (21.6) |
| Unknown | - | 25 (0.1) | 9 (0) | 1 (0) | 1 (0.1) |
| No | 34 (19.7) | 4445 (17.6) | 3203 (16.7) | 1642 (16.7) | 265 (19.7) |
| Not reported | 4 (2.3) | 516 (2.0) | 381 (2.0) | 181 (1.8) | 33 (2.5) |
| Suspected ICI(s) | |||||
| Anti-CTLA-4 monotherapy | |||||
| ipilimumab | 20 (11.6) | 3382 (13.4) | 1698 (8.8) | 839 (8.6) | 119 (8.9) |
| Anti-PD-1 monotherapy | |||||
| nivolumab | 71 (41.0) | 8960 (35.5) | 7247 (37.7) | 3548 (36.2) | 442 (32.9) |
| pembrolizumab | 49 (28.3) | 6591 (26.1) | 5748 (29.9) | 3379 (34.5) | 540 (40.2) |
| cemiplimab | - | 33 (0.1) | 47 (0.2) | 75 (0.8) | 48 (3.6) |
| Anti-PD-L1 monotherapy | |||||
| atezolizumab | 8 (4.6) | 1993 (7.9) | 1674 (8.7) | 777 (7.9) | 88 (6.5) |
| avelumab | 1 (0.6) | 215 (0.9) | 214 (1.1) | 142 (1.4) | 22 (1.6) |
| durvalumab | 2 (1.2) | 912 (3.6) | 894 (4.7) | 380 (3.9) | 18 (1.3) |
| Combination of anti-PD-1 and anti-CTLA-4 | 13 (7.5) | 1826 (7.2) | 1039 (5.4) | 397 (4.0) | 35 (2.6) |
| ≥2 suspected ICIs but regimen not definable # | 9 (5.2) | 1340 (5.3) | 653 (3.4) | 271 (2.8) | 32 (2.4) |
| Cancer type | |||||
| Lung cancer | 11 (6.4) | 7740 (30.7) | 8127 (42.3) | 3933 (40.1) | 375 (27.9) |
| Malignant melanoma | 31 (17.9) | 6526 (25.8) | 3502 (18.2) | 2137 (21.8) | 418 (31.1) |
| Renal cell carcinoma | 11 (6.4) | 1585 (6.3) | 1299 (6.8) | 570 (5.8) | 62 (4.6) |
| Urothelial carcinoma | 2 (1.2) | 708 (2.8) | 961 (5.0) | 685 (7.0) | 85 (6.3) |
| Squamous cell carcinoma of head and neck | - | 557 (2.2) | 370 (1.9) | 154 (1.6) | 11 (0.8) |
| Breast cancer | 1 (0.6) | 530 (2.1) | 108 (0.6) | 37 (0.4) | 6 (0.4) |
| Cancer of the female reproductive system | 1 (0.6) | 454 (1.8) | 261 (1.4) | 98 (1.0) | 6 (0.4) |
| Haematological malignancy | 31 (17.9) | 722 (2.9) | 335 (1.7) | 172 (1.8) | 26 (1.9) |
| Gastrointestinal tract cancer | 7 (4.0) | 1080 (4.3) | 833 (4.3) | 356 (3.6) | 47 (3.5) |
| Skin cancer | - | 70 (0.3) | 50 (0.3) | 98 (1.0) | 73 (5.4) |
| Cancer of the male reproductive system | - | 104 (0.4) | 142 (0.7) | 86 (0.9) | 15 (1.1) |
| Brain cancer | 18 (10.4) | 225 (0.9) | 84 (0.4) | 18 (0.2) | 3 (0.2) |
| Colon cancer | - | 143 (0.6) | 49 (0.3) | 38 (0.4) | - |
| Sarcoma | 12 (6.9) | 132 (0.5) | 36 (0.2) | 17 (0.2) | 1 (0.1) |
| Thyroid cancer/parathyroid gland cancer | - | 74 (0.3) | 32 (0.2) | 17 (0.2) | 5 (0.4) |
| Mesothelioma | - | 64 (0.3) | 86 (0.4) | 43 (0.4) | 6 (0.4) |
| Neuroendocrine carcinoma | 1 (0.6) | 47 (0.2) | 79 (0.4) | 4 (0) | 8 (0.6) |
| Other ῀ | 1 (0.6) | 305 (1.2) | 231 (1.2) | 139 (1.4) | 13 (1.0) |
| Not reported | 46 (26.6) | 4186 (16.6) | 2629 (13.7) | 1206 (12.3) | 184 (13.7) |
| ICI-Related Safety Reports of Eye Disorders | Anti-CTLA-4 Monotherapy (N = 121) | Anti-PD-1/PD-L1 Monotherapy (N = 411) | Combination of Anti-PD-1 and Anti-CTLA-4 (N = 65) | ≥2 Suspected ICIs but Regimen Not Definable * (N = 37) |
|---|---|---|---|---|
| Median age (IQR), years | 52 (46–58) | 55 (48–60) | 54 (47–59) | 56 (52–60) |
| Patient sex | ||||
| Male | 65 (53.7) | 210 (51.1) | 35 (53.8) | 21 (56.8) |
| Female | 55 (45.5) | 196 (47.7) | 30 (46.2) | 16 (43.2) |
| Unknown | 1 (0.8) | 5 (1.2) | - | - |
| Cancer type | ||||
| Lung cancer | - | 127 (30.9) | 2 (3.1) | 1 (2.7) |
| Malignant melanoma | 94 (77.7) | 120 (29.2) | 42 (64.6) | 27 (73.0) |
| Renal cell carcinoma | - | 33 (8.0) | 7 (10.8) | 1 (2.7) |
| Urothelial carcinoma | - | 9 (2.2) | - | - |
| Squamous cell carcinoma of head and neck | - | 9 (2.2) | - | - |
| Breast cancer | - | 9 (2.2) | - | - |
| Cancer of the female reproductive system | - | 11 (2.7) | 3 (4.6) | 1 (2.7) |
| Haematological malignancy | 3 (2.5) | 8 (1.9) | 1 (1.5) | - |
| Gastrointestinal tract cancer | - | 6 (1.5) | 2 (3.1) | - |
| Cancer of the male reproductive system | - | 2 (0.5) | - | - |
| Brain cancer | 1 (0.8) | 6 (1.5) | 1 (1.5) | - |
| Colon cancer | - | 4 (1.0) | - | - |
| Sarcoma | - | 2 (0.5) | - | 1 (2.7) |
| Thyroid cancer/parathyroid gland cancer | - | 1 (0.2) | - | - |
| Mesothelioma | - | 1 (0.2) | - | - |
| Neuroendocrine carcinoma | - | 2 (0.5) | - | - |
| Nasopharyngeal cancer | - | 5 (1.2) | - | - |
| Salivary gland cancer | - | 2 (0.5) | - | - |
| Thymoma | - | 1 (0.2) | - | - |
| Not reported | 23 (19.0) | 53 (13.0) | 7 (10.8) | 6 (16.2) |
| Safety reports with co-reported ICI-related toxicities | 98 (81.0) | 293 (71.3) | 52 (81.3) | 28 (75.7) |
| Safety reports with co-suspected drugs | 15 (12.4) | 62 (15.1) | 10 (15.4) | 1 (2.7) |
| of which antineoplastic drugs (ATC L01) | 4 (3.3) | 44 (10.7) | 6 (9.2) | 1 (2.7) |
| Eye Disorders # | with Anti-CTLA-4 Monotherapy (N = 185) | with Anti-PD-1/PD-L1 Monotherapy (N = 549) | with Combination of Anti-PD-1 and Anti-CTLA-4 (N = 82) | with ≥2 Suspected ICIs but Regimen Not Definable * (N = 50) |
|---|---|---|---|---|
| Spectrum + | ||||
| Uveitis/autoimmune uveitis | 19 | 78 | 9 | 5 |
| Visual impairment | 16 | 48 | 8 | 1 |
| Vision blurred | 14 | 45 | 10 | 2 |
| Dry eye | 1 | 25 | 6 | 2 |
| Diplopia | 12 | 16 | 4 | 1 |
| Iridocyclitis | 6 | 14 | 2 | 8 |
| Ocular hyperaemia | 11 | 12 | 3 | - |
| Blindness | 5 | 16 | 2 | 1 |
| Visual acuity reduced | 7 | 16 | 1 | - |
| Eyelid ptosis | 2 | 19 | 2 | - |
| Eye pain | 4 | 9 | 9 | - |
| Vogt-Koyanagi-Harada disease | 3 | 15 | 1 | 2 |
| Papilloedema | 3 | 7 | 1 | 5 |
| Lacrimation increased | 4 | 10 | 1 | - |
| Photophobia | 5 | 7 | 1 | 1 |
| Retinal detachment | 2 | 7 | - | 2 |
| Eye irritation | 2 | 6 | 1 | 1 |
| Eye swelling | 2 | 6 | 1 | 1 |
| Cataract | 2 | 5 | 2 | - |
| Time to onset | 29 (15.7) | 104 (18.9) | 12 (14.6) | |
| Median (IQR), weeks | 7.6 (2.6–12.9) | 5.8 (2.1–14.0) | 5.3 (3.1–8.4) | - |
| Outcome | ||||
| Recovered/recovering | 77 (41.6) | 202 (36.8) | 30 (36.6) | 18 (36.0) |
| Recovered with sequelae | 3 (1.6) | 11 (2.0) | 1 (1.2) | 1 (2.0) |
| Not recovered | 13 (7.0) | 98 (17.9) | 11 (13.4) | 5 (10.0) |
| Fatal | - | 3 (0.5) | - | - |
| Not reported | 92 (49.7) | 235 (42.8) | 40 (48.8) | 26 (52.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noseda, R.; Bonaldo, G.; Motola, D.; Stathis, A.; Ceschi, A. Adverse Event Reporting with Immune Checkpoint Inhibitors in Older Patients: Age Subgroup Disproportionality Analysis in VigiBase. Cancers 2021, 13, 1131. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051131
Noseda R, Bonaldo G, Motola D, Stathis A, Ceschi A. Adverse Event Reporting with Immune Checkpoint Inhibitors in Older Patients: Age Subgroup Disproportionality Analysis in VigiBase. Cancers. 2021; 13(5):1131. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051131
Chicago/Turabian StyleNoseda, Roberta, Giulia Bonaldo, Domenico Motola, Anastasios Stathis, and Alessandro Ceschi. 2021. "Adverse Event Reporting with Immune Checkpoint Inhibitors in Older Patients: Age Subgroup Disproportionality Analysis in VigiBase" Cancers 13, no. 5: 1131. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051131