
Oncological Treatment-Related Fatigue in Oncogeriatrics: A Scoping Review

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Fatigue during Breast Cancer Treatment
3.2. Fatigue during Ovarian Cancer Treatments
3.3. Fatigue during Prostate Cancer Treatments
3.4. Fatigue during Urothelial Cancer Treatments
3.5. Fatigue during Colorectal Cancer Treatments
3.6. Fatigue during Lung Cancer Treatments
3.7. Fatigue during Treatments for Non-Hodgkin’s and Follicular Lymphoma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- PDQ Supportive and Palliative Care Editorial Board Fatigue (PDQ®): Health Professional Version. In PDQ Cancer Information Summaries; National Cancer Institute (US): Bethesda, MD, USA, 2002.
- Zengarini, E.; Ruggiero, C.; Pérez-Zepeda, M.U.; Hoogendijk, E.O.; Vellas, B.; Mecocci, P.; Cesari, M. Fatigue: Relevance and Implications in the Aging Population. Exp. Gerontol. 2015, 70, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.P.; Kupelnick, B.; Miller, K.; Devine, D.; Lau, J. Evidence Report on the Occurrence, Assessment, and Treatment of Fatigue in Cancer Patients. J. Natl. Cancer Inst. Monogr. 2004, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Vogelzang, N.J.; Breitbart, W.; Cella, D.; Curt, G.A.; Groopman, J.E.; Horning, S.J.; Itri, L.M.; Johnson, D.H.; Scherr, S.L.; Portenoy, R.K. Patient, Caregiver, and Oncologist Perceptions of Cancer-Related Fatigue: Results of a Tripart Assessment Survey. The Fatigue Coalition. Semin. Hematol. 1997, 34, 4–12. [Google Scholar]
- Abrahams, H.J.G.; Gielissen, M.F.M.; Schmits, I.C.; Verhagen, C.A.H.H.V.M.; Rovers, M.M.; Knoop, H. Risk Factors, Prevalence, and Course of Severe Fatigue after Breast Cancer Treatment: A Meta-Analysis Involving 12 327 Breast Cancer Survivors. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Langston, B.; Armes, J.; Levy, A.; Tidey, E.; Ream, E. The Prevalence and Severity of Fatigue in Men with Prostate Cancer: A Systematic Review of the Literature. Support. Care Cancer 2013, 21, 1761–1771. [Google Scholar] [CrossRef] [PubMed]
- PDQ Supportive and Palliative Care Editorial Board Fatigue (PDQ®); National Cancer Institute: Bethesda, MD, USA, 2014.
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Respini, D.; Jacobsen, P.B.; Thors, C.; Tralongo, P.; Balducci, L. The Prevalence and Correlates of Fatigue in Older Cancer Patients. Crit. Rev. Oncol. Hematol. 2003, 47, 273–279. [Google Scholar] [CrossRef]
- Luciani, A.; Jacobsen, P.B.; Extermann, M.; Foa, P.; Marussi, D.; Overcash, J.A.; Balducci, L. Fatigue and Functional Dependence in Older Cancer Patients. Am. J. Clin. Oncol. 2008, 31, 424–430. [Google Scholar] [CrossRef]
- Luctkar-Flude, M.; Groll, D.; Woodend, K.; Tranmer, J. Fatigue and Physical Activity in Older Patients with Cancer: A Six-Month Follow-up Study. Oncol. Nurs. Forum 2009, 36, 194–202. [Google Scholar] [CrossRef]
- Cella, D.; Lai, J.-S.; Chang, C.-H.; Peterman, A.; Slavin, M. Fatigue in Cancer Patients Compared with Fatigue in the General United States Population. Cancer 2002, 94, 528–538. [Google Scholar] [CrossRef]
- Gupta, D.; Braun, D.P.; Staren, E.D. Prognostic Value of Changes in Quality of Life Scores in Prostate Cancer. BMC Urol. 2013, 13, 32. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus Sunitinib in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Common Terminology Criteria for Adverse Events (CTCAE); Version 4; National Cancer Institute: Bethesda, MD, USA, 2009.
- Common Terminology Criteria for Adverse Events (CTCAE); Version 3; National Cancer Institute: Bethesda, MD, USA, 2006.
- Common Terminology Criteria for Adverse Events (CTCAE); Version 5; National Cancer Institute: Bethesda, MD, USA, 2017; p. 155.
- Agnihotri, P.; Telfer, M.; Butt, Z.; Jella, A.; Cella, D.; Kozma, C.M.; Ahuja, M.; Riaz, S.; Akamah, J. Chronic Anemia and Fatigue in Elderly Patients: Results of a Randomized, Double-Blind, Placebo-Controlled, Crossover Exploratory Study with Epoetin Alfa. J. Am. Geriatr. Soc. 2007, 55, 1557–1565. [Google Scholar] [CrossRef]
- Silva, J.C.; de Moraes, Z.V.; Silva, C.; de Barros Mazon, S.; Guariento, M.E.; Neri, A.L.; Fattori, A. Understanding Red Blood Cell Parameters in the Context of the Frailty Phenotype: Interpretations of the FIBRA (Frailty in Brazilian Seniors) Study. Arch. Gerontol. Geriatr. 2014, 59, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Penninx, B.W.J.H.; Lauretani, F.; Russo, C.R.; Carter, C.; Bandinelli, S.; Atkinson, H.; Onder, G.; Pahor, M.; Ferrucci, L. Hemoglobin Levels and Skeletal Muscle: Results from the InCHIANTI Study. J. Gerontol. A. Biol. Sci. Med. Sci. 2004, 59, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aapro, M.S.; Bohlius, J.; Cameron, D.A.; Lago, L.D.; Donnelly, J.P.; Kearney, N.; Lyman, G.H.; Pettengell, R.; Tjan-Heijnen, V.C.; Walewski, J.; et al. 2010 Update of EORTC Guidelines for the Use of Granulocyte-Colony Stimulating Factor to Reduce the Incidence of Chemotherapy-Induced Febrile Neutropenia in Adult Patients with Lymphoproliferative Disorders and Solid Tumours. Eur. J. Cancer 2011, 47, 8–32. [Google Scholar] [CrossRef]
- Hesketh, P.J.; Kris, M.G.; Basch, E.; Bohlke, K.; Barbour, S.Y.; Clark-Snow, R.A.; Danso, M.A.; Dennis, K.; Dupuis, L.L.; Dusetzina, S.B.; et al. Antiemetics: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 3240–3261. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Wiskemann, J.; Schneeweiss, A.; Potthoff, K.; Ulrich, C.M.; Steindorf, K. Determinants of Physical, Affective, and Cognitive Fatigue during Breast Cancer Therapy and 12 Months Follow-Up. Int. J. Cancer 2018, 142, 1148–1157. [Google Scholar] [CrossRef] [Green Version]
- Di Meglio, A.; Havas, J.; Soldato, D.; Presti, D.; Martin, E.; Pistilli, B.; Menvielle, G.; Dumas, A.; Charles, C.; Everhard, S.; et al. Development and Validation of a Predictive Model of Severe Fatigue After Breast Cancer Diagnosis: Toward a Personalized Framework in Survivorship Care. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, JCO2101252. [Google Scholar] [CrossRef]
- Masuda, N.; Lee, S.-J.; Ohtani, S.; Im, Y.-H.; Lee, E.-S.; Yokota, I.; Kuroi, K.; Im, S.-A.; Park, B.-W.; Kim, S.-B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Jones, S.E.; Savin, M.A.; Holmes, F.A.; O’Shaughnessy, J.A.; Blum, J.L.; Vukelja, S.; McIntyre, K.J.; Pippen, J.E.; Bordelon, J.H.; Kirby, R.; et al. Phase III Trial Comparing Doxorubicin plus Cyclophosphamide with Docetaxel plus Cyclophosphamide as Adjuvant Therapy for Operable Breast Cancer. J. Clin. Oncol. 2006, 24, 5381–5387. [Google Scholar] [CrossRef] [Green Version]
- Tolaney, S.M.; Barry, W.T.; Dang, C.T.; Yardley, D.A.; Moy, B.; Marcom, P.K.; Albain, K.S.; Rugo, H.S.; Ellis, M.; Shapira, I.; et al. Adjuvant Paclitaxel and Trastuzumab for Node-Negative, HER2-Positive Breast Cancer. N. Engl. J. Med. 2015, 372, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Reinisch, M.; von Minckwitz, G.; Harbeck, N.; Janni, W.; Kümmel, S.; Kaufmann, M.; Elling, D.; Nekljudova, V.; Loibl, S. Side Effects of Standard Adjuvant and Neoadjuvant Chemotherapy Regimens According to Age Groups in Primary Breast Cancer. Breast Care 2013, 8, 60–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouridsen, H.; Gershanovich, M.; Sun, Y.; Pérez-Carrión, R.; Boni, C.; Monnier, A.; Apffelstaedt, J.; Smith, R.; Sleeboom, H.P.; Jänicke, F.; et al. Superior Efficacy of Letrozole versus Tamoxifen as First-Line Therapy for Postmenopausal Women with Advanced Breast Cancer: Results of a Phase III Study of the International Letrozole Breast Cancer Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 2596–2606. [Google Scholar] [CrossRef] [PubMed]
- Ohno, S. Tolerability of Therapies Recommended for the Treatment of Hormone Receptor-Positive Locally Advanced or Metastatic Breast Cancer. Clin. Breast Cancer 2016, 16, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Bonneterre, J.; Buzdar, A.; Nabholtz, J.M.; Robertson, J.F.; Thurlimann, B.; von Euler, M.; Sahmoud, T.; Webster, A.; Steinberg, M. Anastrozole Is Superior to Tamoxifen as First-Line Therapy in Hormone Receptor Positive Advanced Breast Carcinoma. Cancer 2001, 92, 2247–2258. [Google Scholar] [CrossRef]
- Goss, P.E.; Ingle, J.N.; Martino, S.; Robert, N.J.; Muss, H.B.; Piccart, M.J.; Castiglione, M.; Tu, D.; Shepherd, L.E.; Pritchard, K.I.; et al. A Randomized Trial of Letrozole in Postmenopausal Women after Five Years of Tamoxifen Therapy for Early-Stage Breast Cancer. N. Engl. J. Med. 2003, 349, 1793–1802. [Google Scholar] [CrossRef]
- Muss, H.B.; Tu, D.; Ingle, J.N.; Martino, S.; Robert, N.J.; Pater, J.L.; Whelan, T.J.; Palmer, M.J.; Piccart, M.J.; Shepherd, L.E.; et al. Efficacy, Toxicity, and Quality of Life in Older Women with Early-Stage Breast Cancer Treated with Letrozole or Placebo after 5 Years of Tamoxifen: NCIC CTG Intergroup Trial MA.17. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 1956–1964. [Google Scholar] [CrossRef]
- Coombes, R.C.; Hall, E.; Gibson, L.J.; Paridaens, R.; Jassem, J.; Delozier, T.; Jones, S.E.; Alvarez, I.; Bertelli, G.; Ortmann, O.; et al. A Randomized Trial of Exemestane after Two to Three Years of Tamoxifen Therapy in Postmenopausal Women with Primary Breast Cancer. N. Engl. J. Med. 2004, 350, 1081–1092. [Google Scholar] [CrossRef] [Green Version]
- Nabholtz, J.-M.; Falkson, C.; Campos, D.; Szanto, J.; Martin, M.; Chan, S.; Pienkowski, T.; Zaluski, J.; Pinter, T.; Krzakowski, M.; et al. Docetaxel and Doxorubicin Compared with Doxorubicin and Cyclophosphamide as First-Line Chemotherapy for Metastatic Breast Cancer: Results of a Randomized, Multicenter, Phase III Trial. J. Clin. Oncol. 2003, 21, 968–975. [Google Scholar] [CrossRef]
- Citron, M.L.; Berry, D.A.; Cirrincione, C.; Hudis, C.; Winer, E.P.; Gradishar, W.J.; Davidson, N.E.; Martino, S.; Livingston, R.; Ingle, J.N.; et al. Randomized Trial of Dose-Dense versus Conventionally Scheduled and Sequential versus Concurrent Combination Chemotherapy as Postoperative Adjuvant Treatment of Node-Positive Primary Breast Cancer: First Report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 1431–1439. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Raab, G.; Caputo, A.; Schütte, M.; Hilfrich, J.; Blohmer, J.U.; Gerber, B.; Costa, S.D.; Merkle, E.; Eidtmann, H.; et al. Doxorubicin with Cyclophosphamide Followed by Docetaxel Every 21 Days Compared with Doxorubicin and Docetaxel Every 14 Days As Preoperative Treatment in Operable Breast Cancer: The GEPARDUO Study of the German Breast Group. J. Clin. Oncol. 2005, 23, 2676–2685. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Geeraerts, L.; Suman, V.J.; Adjei, A.A.; Baron, A.T.; Hatfield, A.K.; Maihle, N.; Michalak, J.C.; Kuross, S.A.; Kugler, J.W.; et al. A Randomized Phase II Study of Sequential Docetaxel and Doxorubicin/Cyclophosphamide in Patients with Metastatic Breast Cancer. Ann. Oncol. 2002, 13, 1225–1235. [Google Scholar] [CrossRef] [PubMed]
- Alba, E.; Martín, M.; Ramos, M.; Adrover, E.; Balil, A.; Jara, C.; Barnadas, A.; Fernández-Aramburo, A.; Sánchez-Rovira, P.; Amenedo, M.; et al. Multicenter Randomized Trial Comparing Sequential with Concomitant Administration of Doxorubicin and Docetaxel as First-Line Treatment of Metastatic Breast Cancer: A Spanish Breast Cancer Research Group (GEICAM-9903) Phase III Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 2587–2593. [Google Scholar] [CrossRef]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant Trastuzumab in HER2-Positive Breast Cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Biganzoli, L.; Cufer, T.; Bruning, P.; Coleman, R.; Duchateau, L.; Calvert, A.H.; Gamucci, T.; Twelves, C.; Fargeot, P.; Epelbaum, R.; et al. Doxorubicin and Paclitaxel versus Doxorubicin and Cyclophosphamide as First-Line Chemotherapy in Metastatic Breast Cancer: The European Organization for Research and Treatment of Cancer 10961 Multicenter Phase III Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2002, 20, 3114–3121. [Google Scholar] [CrossRef]
- Martin, M.; Pienkowski, T.; Mackey, J.; Pawlicki, M.; Guastalla, J.-P.; Weaver, C.; Tomiak, E.; Al-Tweigeri, T.; Chap, L.; Juhos, E.; et al. Adjuvant Docetaxel for Node-Positive Breast Cancer. N. Engl. J. Med. 2005, 352, 2302–2313. [Google Scholar] [CrossRef] [Green Version]
- Therasse, P.; Mauriac, L.; Welnicka-Jaskiewicz, M.; Bruning, P.; Cufer, T.; Bonnefoi, H.; Tomiak, E.; Pritchard, K.I.; Hamilton, A.; Piccart, M.J. Final Results of a Randomized Phase III Trial Comparing Cyclophosphamide, Epirubicin, and Fluorouracil with a Dose-Intensified Epirubicin and Cyclophosphamide + Filgrastim as Neoadjuvant Treatment in Locally Advanced Breast Cancer: An EORTC-NCIC-SAKK Multicenter Study. J. Clin. Oncol. 2003, 21, 843–850. [Google Scholar] [CrossRef]
- Brain, E.G.C.; Mertens, C.; Girre, V.; Rousseau, F.; Blot, E.; Abadie, S.; Uwer, L.; Bourbouloux, E.; Van Praagh-Doreau, I.; Mourey, L.; et al. Impact of Liposomal Doxorubicin-Based Adjuvant Chemotherapy on Autonomy in Women over 70 with Hormone-Receptor-Negative Breast Carcinoma: A French Geriatric Oncology Group (GERICO) Phase II Multicentre Trial. Crit. Rev. Oncol. Hematol. 2011, 80, 160–170. [Google Scholar] [CrossRef]
- Martín, M.; Ruiz, A.; Ruiz Borrego, M.; Barnadas, A.; González, S.; Calvo, L.; Margelí Vila, M.; Antón, A.; Rodríguez-Lescure, A.; Seguí-Palmer, M.A.; et al. Fluorouracil, Doxorubicin, and Cyclophosphamide (FAC) versus FAC Followed by Weekly Paclitaxel as Adjuvant Therapy for High-Risk, Node-Negative Breast Cancer: Results from the GEICAM/2003-02 Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 2593–2599. [Google Scholar] [CrossRef]
- Jassem, J.; Pieńkowski, T.; Płuzańska, A.; Jelic, S.; Gorbunova, V.; Mrsic-Krmpotic, Z.; Berzins, J.; Nagykalnai, T.; Wigler, N.; Renard, J.; et al. Doxorubicin and Paclitaxel versus Fluorouracil, Doxorubicin, and Cyclophosphamide as First-Line Therapy for Women with Metastatic Breast Cancer: Final Results of a Randomized Phase III Multicenter Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 1707–1715. [Google Scholar] [CrossRef] [PubMed]
- Bontenbal, M.; Creemers, G.-J.; Braun, H.J.; de Boer, A.C.; Janssen, J.T.; Leys, R.B.; Ruit, J.B.; Goey, S.H.; van der Velden, P.C.; Kerkhofs, L.G.; et al. Phase II to III Study Comparing Doxorubicin and Docetaxel with Fluorouracil, Doxorubicin, and Cyclophosphamide As First-Line Chemotherapy in Patients with Metastatic Breast Cancer: Results of a Dutch Community Setting Trial for the Clinical Trial Group of the Comprehensive Cancer Centre. J. Clin. Oncol. 2005, 23, 7081–7088. [Google Scholar] [CrossRef] [PubMed]
- French Adjuvant Study Group Benefit of a High-Dose Epirubicin Regimen in Adjuvant Chemotherapy for Node-Positive Breast Cancer Patients with Poor Prognostic Factors: 5-Year Follow-up Results of French Adjuvant Study Group 05 Randomized Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 602–611. [CrossRef] [PubMed]
- Zielinski, C.; Beslija, S.; Mrsic-Krmpotic, Z.; Welnicka-Jaskiewicz, M.; Wiltschke, C.; Kahan, Z.; Grgic, M.; Tzekova, V.; Inbar, M.; Cervek, J.; et al. Gemcitabine, Epirubicin, and Paclitaxel Versus Fluorouracil, Epirubicin, and Cyclophosphamide As First-Line Chemotherapy in Metastatic Breast Cancer: A Central European Cooperative Oncology Group International, Multicenter, Prospective, Randomized Phase III Trial. J. Clin. Oncol. 2005, 23, 1401–1408. [Google Scholar] [CrossRef]
- Tannock, I.F.; Boyd, N.F.; DeBoer, G.; Erlichman, C.; Fine, S.; Larocque, G.; Mayers, C.; Perrault, D.; Sutherland, H. A Randomized Trial of Two Dose Levels of Cyclophosphamide, Methotrexate, and Fluorouracil Chemotherapy for Patients with Metastatic Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1988, 6, 1377–1387. [Google Scholar] [CrossRef]
- Ron, I.G.; Wigler, N.; Borovik, R.; Brufman, G.; Rizel, S.; Shani, A.; Brenner, J.; Farbstein, H.; Dale, A.; Inbar, M.J.; et al. CMF (Cyclophosphamide, Methotrexate, 5-Fluorouracil) versus Cnf (Cyclophosphamide, Mitoxantrone, 5-Fluorouracil) as Adjuvant Chemotherapy for Stage II Lymph-Node Positive Breast Cancer: A Phase III Randomized Multicenter Study. Am. J. Clin. Oncol. 2001, 24, 323–327. [Google Scholar] [CrossRef]
- Levine, M.N.; Bramwell, V.H.; Pritchard, K.I.; Norris, B.D.; Shepherd, L.E.; Abu-Zahra, H.; Findlay, B.; Warr, D.; Bowman, D.; Myles, J.; et al. Randomized Trial of Intensive Cyclophosphamide, Epirubicin, and Fluorouracil Chemotherapy Compared with Cyclophosphamide, Methotrexate, and Fluorouracil in Premenopausal Women with Node-Positive Breast Cancer. National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1998, 16, 2651–2658. [Google Scholar]
- Jones, S.E.; Collea, R.; Paul, D.; Sedlacek, S.; Favret, A.M.; Gore, I.; Lindquist, D.L.; Holmes, F.A.; Allison, M.A.K.; Brooks, B.D.; et al. Adjuvant Docetaxel and Cyclophosphamide plus Trastuzumab in Patients with HER2-Amplified Early Stage Breast Cancer: A Single-Group, Open-Label, Phase 2 Study. Lancet Oncol. 2013, 14, 1121–1128. [Google Scholar] [CrossRef]
- Breast International Group (BIG) 1-98 Collaborative Group; Thürlimann, B.; Keshaviah, A.; Coates, A.S.; Mouridsen, H.; Mauriac, L.; Forbes, J.F.; Paridaens, R.; Castiglione-Gertsch, M.; Gelber, R.D.; et al. A Comparison of Letrozole and Tamoxifen in Postmenopausal Women with Early Breast Cancer. N. Engl. J. Med. 2005, 353, 2747–2757. [Google Scholar] [CrossRef] [Green Version]
- Seidman, A.D.; Berry, D.; Cirrincione, C.; Harris, L.; Muss, H.; Marcom, P.K.; Gipson, G.; Burstein, H.; Lake, D.; Shapiro, C.L.; et al. Randomized Phase III Trial of Weekly Compared with Every-3-Weeks Paclitaxel for Metastatic Breast Cancer, with Trastuzumab for All HER-2 Overexpressors and Random Assignment to Trastuzumab or Not in HER-2 Nonoverexpressors: Final Results of Cancer and Leukemia Group B Protocol 9840. J. Clin. Oncol. 2008, 26, 1642–1649. [Google Scholar] [CrossRef] [Green Version]
- Gradishar, W.J. The Place for Eribulin in the Treatment of Metastatic Breast Cancer. Curr. Oncol. Rep. 2011, 13, 11–16. [Google Scholar] [CrossRef]
- Miller, K.; Wang, M.; Gralow, J.; Dickler, M.; Cobleigh, M.; Perez, E.A.; Shenkier, T.; Cella, D.; Davidson, N.E. Paclitaxel plus Bevacizumab versus Paclitaxel Alone for Metastatic Breast Cancer. N. Engl. J. Med. 2007, 357, 2666–2676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneeweiss, A.; Förster, F.; Tesch, H.; Aktas, B.; Gluz, O.; Geberth, M.; Hertz-Eichenrode, M.M.; Schönegg, W.; Schumacher, C.; Kutscheidt, A.; et al. First-Line Bevacizumab-Containing Therapy for HER2-Negative Metastatic Breast Cancer: Final Results from a Prospective German Study. Anticancer Res. 2016, 36, 967–974. [Google Scholar]
- O’Shaughnessy, J.; Miles, D.; Vukelja, S.; Moiseyenko, V.; Ayoub, J.-P.; Cervantes, G.; Fumoleau, P.; Jones, S.; Lui, W.-Y.; Mauriac, L.; et al. Superior Survival with Capecitabine plus Docetaxel Combination Therapy in Anthracycline-Pretreated Patients with Advanced Breast Cancer: Phase III Trial Results. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2002, 20, 2812–2823. [Google Scholar] [CrossRef] [PubMed]
- Harvey, V.; Mouridsen, H.; Semiglazov, V.; Jakobsen, E.; Voznyi, E.; Robinson, B.A.; Groult, V.; Murawsky, M.; Cold, S. Phase III Trial Comparing Three Doses of Docetaxel for Second-Line Treatment of Advanced Breast Cancer. J. Clin. Oncol. 2006, 24, 4963–4970. [Google Scholar] [CrossRef] [PubMed]
- Joensuu, H.; Sailas, L.; Alanko, T.; Sunela, K.; Huuhtanen, R.; Utriainen, M.; Kokko, R.; Bono, P.; Wigren, T.; Pyrhönen, S.; et al. Docetaxel versus Docetaxel Alternating with Gemcitabine as Treatments of Advanced Breast Cancer: Final Analysis of a Randomised Trial. Ann. Oncol. 2010, 21, 968–973. [Google Scholar] [CrossRef]
- Young, S.D.; Lafrenie, R.M.; Clemons, M.J. Phase II Trial of a Metronomic Schedule of Docetaxel and Capecitabine with Concurrent Celecoxib in Patients with Prior Anthracycline Exposure for Metastatic Breast Cancer. Curr. Oncol. 2012, 19, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Martín, M.; Ruiz, A.; Muñoz, M.; Balil, A.; García-Mata, J.; Calvo, L.; Carrasco, E.; Mahillo, E.; Casado, A.; García-Saenz, J.Á.; et al. Gemcitabine plus Vinorelbine versus Vinorelbine Monotherapy in Patients with Metastatic Breast Cancer Previously Treated with Anthracyclines and Taxanes: Final Results of the Phase III Spanish Breast Cancer Research Group (GEICAM) Trial. Lancet Oncol. 2007, 8, 219–225. [Google Scholar] [CrossRef]
- O’Shaughnessy, J.A. Pegylated Liposomal Doxorubicin in the Treatment of Breast Cancer. Clin. Breast Cancer 2003, 4, 318–328. [Google Scholar] [CrossRef]
- Falandry, C.; Brain, E.; Bonnefoy, M.; Mefti, F.; Jovenin, N.; Rigal, O.; Guillem, O.; El Kouri, C.; Uwer, L.; Abadie-Lacourtoisie, S.; et al. Impact of Geriatric Risk Factors on Pegylated Liposomal Doxorubicin Tolerance and Efficacy in Elderly Metastatic Breast Cancer Patients: Final Results of the DOGMES Multicentre GINECO Trial. Eur. J. Cancer 2013, 49, 2806–2814. [Google Scholar] [CrossRef]
- Norris, B.; Pritchard, K.I.; James, K.; Myles, J.; Bennett, K.; Marlin, S.; Skillings, J.; Findlay, B.; Vandenberg, T.; Goss, P.; et al. Phase III Comparative Study of Vinorelbine Combined with Doxorubicin versus Doxorubicin Alone in Disseminated Metastatic/Recurrent Breast Cancer: National Cancer Institute of Canada Clinical Trials Group Study MA8. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2000, 18, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Blum, J.L.; Jones, S.E.; Buzdar, A.U.; LoRusso, P.M.; Kuter, I.; Vogel, C.; Osterwalder, B.; Burger, H.U.; Brown, C.S.; Griffin, T. Multicenter Phase II Study of Capecitabine in Paclitaxel-Refractory Metastatic Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1999, 17, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Blum, J.L.; Dieras, V.; Lo Russo, P.M.; Horton, J.; Rutman, O.; Buzdar, A.; Osterwalder, B. Multicenter, Phase II Study of Capecitabine in Taxane-Pretreated Metastatic Breast Carcinoma Patients. Cancer 2001, 92, 1759–1768. [Google Scholar] [CrossRef]
- Reichardt, P.; von Minckwitz, G.; Thuss-Patience, P.C.; Jonat, W.; Kölbl, H.; Jänicke, F.; Kieback, D.G.; Kuhn, W.; Schindler, A.E.; Mohrmann, S.; et al. Multicenter Phase II Study of Oral Capecitabine (Xeloda“) in Patients with Metastatic Breast Cancer Relapsing after Treatment with a Taxane-Containing Therapy. Ann. Oncol. 2003, 14, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Walko, C.M.; Lindley, C. Capecitabine: A Review. Clin. Ther. 2005, 27, 23–44. [Google Scholar] [CrossRef] [PubMed]
- Welt, A.; Marschner, N.; Lerchenmueller, C.; Decker, T.; Steffens, C.-C.; Koehler, A.; Depenbusch, R.; Busies, S.; Hegewisch-Becker, S. Capecitabine and Bevacizumab with or without Vinorelbine in First-Line Treatment of HER2/Neu-Negative Metastatic or Locally Advanced Breast Cancer: Final Efficacy and Safety Data of the Randomised, Open-Label Superiority Phase 3 CARIN Trial. Breast Cancer Res. Treat. 2016, 156, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Blackstein, M.; Vogel, C.L.; Ambinder, R.; Cowan, J.; Iglesias, J.; Melemed, A. Gemcitabine as First-Line Therapy in Patients with Metastatic Breast Cancer: A Phase II Trial. Oncology 2002, 62, 2–8. [Google Scholar] [CrossRef]
- Swami, U.; Chaudhary, I.; Ghalib, M.H.; Goel, S. Eribulin—A Review of Preclinical and Clinical Studies. Crit. Rev. Oncol. Hematol. 2012, 81, 163–184. [Google Scholar] [CrossRef] [Green Version]
- Cortes, J.; Hudgens, S.; Twelves, C.; Perez, E.A.; Awada, A.; Yelle, L.; McCutcheon, S.; Kaufman, P.A.; Forsythe, A.; Velikova, G. Health-Related Quality of Life in Patients with Locally Advanced or Metastatic Breast Cancer Treated with Eribulin Mesylate or Capecitabine in an Open-Label Randomized Phase 3 Trial. Breast Cancer Res. Treat. 2015, 154, 509–520. [Google Scholar] [CrossRef]
- Swain, S.M.; Miles, D.; Kim, S.-B.; Im, Y.-H.; Im, S.-A.; Semiglazov, V.; Ciruelos, E.; Schneeweiss, A.; Loi, S.; Monturus, E.; et al. Pertuzumab, Trastuzumab, and Docetaxel for HER2-Positive Metastatic Breast Cancer (CLEOPATRA): End-of-Study Results from a Double-Blind, Randomised, Placebo-Controlled, Phase 3 Study. Lancet Oncol. 2020, 21, 519–530. [Google Scholar] [CrossRef]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of Chemotherapy plus a Monoclonal Antibody against HER2 for Metastatic Breast Cancer That Overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Farhat, F.; Kattan, J.G.; Ghosn, M. Oral Vinorelbine in Combination with Trastuzumab as a First-Line Therapy of Metastatic or Locally Advanced HER2-Positive Breast Cancer. Cancer Chemother. Pharmacol. 2016, 77, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- André, F.; O’Regan, R.; Ozguroglu, M.; Toi, M.; Xu, B.; Jerusalem, G.; Masuda, N.; Wilks, S.; Arena, F.; Isaacs, C.; et al. Everolimus for Women with Trastuzumab-Resistant, HER2-Positive, Advanced Breast Cancer (BOLERO-3): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet Oncol. 2014, 15, 580–591. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.-Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [Green Version]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A.; Lin, N.U.; Borges, V.; Abramson, V.; Anders, C.; et al. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2020, 382, 597–609. [Google Scholar] [CrossRef]
- Bachelot, T.; Ciruelos, E.; Schneeweiss, A.; Puglisi, F.; Peretz-Yablonski, T.; Bondarenko, I.; Paluch-Shimon, S.; Wardley, A.; Merot, J.-L.; du Toit, Y.; et al. Preliminary Safety and Efficacy of First-Line Pertuzumab Combined with Trastuzumab and Taxane Therapy for HER2-Positive Locally Recurrent or Metastatic Breast Cancer (PERUSE). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 766–773. [Google Scholar] [CrossRef] [Green Version]
- Finn, R.S.; Crown, J.P.; Lang, I.; Boer, K.; Bondarenko, I.M.; Kulyk, S.O.; Ettl, J.; Patel, R.; Pinter, T.; Schmidt, M.; et al. The Cyclin-Dependent Kinase 4/6 Inhibitor Palbociclib in Combination with Letrozole versus Letrozole Alone as First-Line Treatment of Oestrogen Receptor-Positive, HER2-Negative, Advanced Breast Cancer (PALOMA-1/TRIO-18): A Randomised Phase 2 Study. Lancet Oncol. 2015, 16, 25–35. [Google Scholar] [CrossRef]
- O’Shaughnessy, J.; Petrakova, K.; Sonke, G.S.; Conte, P.; Arteaga, C.L.; Cameron, D.A.; Hart, L.L.; Villanueva, C.; Jakobsen, E.; Beck, J.T.; et al. Ribociclib plus Letrozole versus Letrozole Alone in Patients with de Novo HR+, HER2- Advanced Breast Cancer in the Randomized MONALEESA-2 Trial. Breast Cancer Res. Treat. 2018, 168, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Baselga, J.; Campone, M.; Piccart, M.; Burris, H.A.I.; Rugo, H.S.; Sahmoud, T.; Noguchi, S.; Gnant, M.; Pritchard, K.I.; Lebrun, F.; et al. Everolimus in Postmenopausal Hormone-Receptor-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 366, 520–529. [Google Scholar] [CrossRef] [Green Version]
- Di Leo, A.; Jerusalem, G.; Petruzelka, L.; Torres, R.; Bondarenko, I.N.; Khasanov, R.; Verhoeven, D.; Pedrini, J.L.; Smirnova, I.; Lichinitser, M.R.; et al. Results of the CONFIRM Phase III Trial Comparing Fulvestrant 250 Mg with Fulvestrant 500 Mg in Postmenopausal Women with Estrogen Receptor-Positive Advanced Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 4594–4600. [Google Scholar] [CrossRef]
- Howell, A.; Sapunar, F. Fulvestrant Revisited: Efficacy and Safety of the 500-Mg Dose. Clin. Breast Cancer 2011, 11, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.C.; Slamon, D.J.; Ro, J.; Bondarenko, I.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Overall Survival with Palbociclib and Fulvestrant in Advanced Breast Cancer. N. Engl. J. Med. 2018, 379, 1926–1936. [Google Scholar] [CrossRef] [PubMed]
- Sledge, G.W.; Toi, M.; Neven, P.; Sohn, J.; Inoue, K.; Pivot, X.; Burdaeva, O.; Okera, M.; Masuda, N.; Kaufman, P.A.; et al. MONARCH 2: Abemaciclib in Combination with Fulvestrant in Women with HR+/HER2- Advanced Breast Cancer Who Had Progressed While Receiving Endocrine Therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2875–2884. [Google Scholar] [CrossRef]
- Slamon, D.J.; Neven, P.; Chia, S.; Fasching, P.A.; De Laurentiis, M.; Im, S.-A.; Petrakova, K.; Bianchi, G.V.; Esteva, F.J.; Martín, M.; et al. Phase III Randomized Study of Ribociclib and Fulvestrant in Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: MONALEESA-3. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2465–2472. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.; Pippen, J.; Pivot, X.; Lichinitser, M.; Sadeghi, S.; Dieras, V.; Gomez, H.L.; Romieu, G.; Manikhas, A.; Kennedy, M.J.; et al. Lapatinib Combined with Letrozole versus Letrozole and Placebo as First-Line Therapy for Postmenopausal Hormone Receptor-Positive Metastatic Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 5538–5546. [Google Scholar] [CrossRef] [Green Version]
- Villanueva, C.; Romieu, G.; Salvat, J.; Chaigneau, L.; Merrouche, Y.; N’guyen, T.; Vuillemin, A.T.; Demarchi, M.; Dobi, E.; Pivot, X. Phase II Study Assessing Lapatinib Added to Letrozole in Patients with Progressive Disease under Aromatase Inhibitor in Metastatic Breast Cancer-Study BES 06. Target. Oncol. 2013, 8, 137–143. [Google Scholar] [CrossRef]
- Moscetti, L.; Vici, P.; Gamucci, T.; Natoli, C.; Cortesi, E.; Marchetti, P.; Santini, D.; Giuliani, R.; Sperduti, I.; Mauri, M.; et al. Safety Analysis, Association with Response and Previous Treatments of Everolimus and Exemestane in 181 Metastatic Breast Cancer Patients: A Multicenter Italian Experience. The Breast 2016, 29, 96–101. [Google Scholar] [CrossRef]
- Jerusalem, G.; Mariani, G.; Ciruelos, E.M.; Martin, M.; Tjan-Heijnen, V.C.G.; Neven, P.; Gavila, J.G.; Michelotti, A.; Montemurro, F.; Generali, D.; et al. Safety of Everolimus plus Exemestane in Patients with Hormone-Receptor–Positive, HER2–Negative Locally Advanced or Metastatic Breast Cancer Progressing on Prior Non-Steroidal Aromatase Inhibitors: Primary Results of a Phase IIIb, Open-Label, Single-Arm, Expanded-Access Multicenter Trial (BALLET). Ann. Oncol. 2016, 27, 1719–1725. [Google Scholar] [CrossRef]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Rugo, H.S.; Turner, N.C.; Finn, R.S.; Joy, A.A.; Verma, S.; Harbeck, N.; Masuda, N.; Im, S.-A.; Huang, X.; Kim, S.; et al. Palbociclib plus Endocrine Therapy in Older Women with HR+/HER2- Advanced Breast Cancer: A Pooled Analysis of Randomised PALOMA Clinical Studies. Eur. J. Cancer Oxf. Engl. 1990 2018, 101, 123–133. [Google Scholar] [CrossRef]
- De Laurentiis, M.; Borstnar, S.; Campone, M.; Warner, E.; Bofill, J.S.; Jacot, W.; Dent, S.; Martin, M.; Ring, A.; Cottu, P.; et al. Full Population Results from the Core Phase of CompLEEment-1, a Phase 3b Study of Ribociclib plus Letrozole as First-Line Therapy for Advanced Breast Cancer in an Expanded Population. Breast Cancer Res. Treat. 2021, 189, 689–699. [Google Scholar] [CrossRef]
- Goetz, M.P.; Toi, M.; Campone, M.; Sohn, J.; Paluch-Shimon, S.; Huober, J.; Park, I.H.; Trédan, O.; Chen, S.-C.; Manso, L.; et al. MONARCH 3: Abemaciclib As Initial Therapy for Advanced Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 3638–3646. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 5). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Liposits, G.; Loh, K.P.; Soto-Perez-de-Celis, E.; Dumas, L.; Battisti, N.M.L.; Kadambi, S.; Baldini, C.; Banerjee, S.; Lichtman, S.M. PARP Inhibitors in Older Patients with Ovarian and Breast Cancer: Young International Society of Geriatric Oncology Review Paper. J. Geriatr. Oncol. 2019, 10, 337–345. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Falandry, C.; Weber, B.; Savoye, A.M.; Tinquaut, F.; Tredan, O.; Sevin, E.; Stefani, L.; Savinelli, F.; Atlassi, M.; Salvat, J.; et al. Development of a Geriatric Vulnerability Score in Elderly Patients with Advanced Ovarian Cancer Treated with First-Line Carboplatin: A GINECO Prospective Trial. Ann. Oncol. 2013, 24, 2808–2813. [Google Scholar] [CrossRef]
- Falandry, C.; Rousseau, F.; Mouret-Reynier, M.-A.; Tinquaut, F.; Lorusso, D.; Herrstedt, J.; Savoye, A.-M.; Stefani, L.; Bourbouloux, E.; Sverdlin, R.; et al. Efficacy and Safety of First-Line Single-Agent Carboplatin vs Carboplatin Plus Paclitaxel for Vulnerable Older Adult Women with Ovarian Cancer: A Randomized Clinical Trial. JAMA Oncol. 2021, 7, 853–861. [Google Scholar] [CrossRef]
- Pignata, S.; Breda, E.; Scambia, G.; Pisano, C.; Zagonel, V.; Lorusso, D.; Greggi, S.; De Vivo, R.; Ferrandina, G.; Gallo, C.; et al. A Phase II Study of Weekly Carboplatin and Paclitaxel as First-Line Treatment of Elderly Patients with Advanced Ovarian Cancer. A Multicentre Italian Trial in Ovarian Cancer (MITO-5) Study. Crit. Rev. Oncol. Hematol. 2008, 66, 229–236. [Google Scholar] [CrossRef] [PubMed]
- du Bois, A.; Luck, H.J.; Meier, W.; Adams, H.P.; Mobus, V.; Costa, S.; Bauknecht, T.; Richter, B.; Warm, M.; Schroder, W.; et al. A Randomized Clinical Trial of Cisplatin/Paclitaxel versus Carboplatin/Paclitaxel as First-Line Treatment of Ovarian Cancer. J. Natl. Cancer Inst. 2003, 95, 1320–1329. [Google Scholar] [CrossRef] [PubMed]
- Ozols, R.F.; Bundy, B.N.; Greer, B.E.; Fowler, J.M.; Clarke-Pearson, D.; Burger, R.A.; Mannel, R.S.; DeGeest, K.; Hartenbach, E.M.; Baergen, R. Phase III Trial of Carboplatin and Paclitaxel Compared with Cisplatin and Paclitaxel in Patients with Optimally Resected Stage III Ovarian Cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2003, 21, 3194–3200. [Google Scholar] [CrossRef]
- Hilpert, F.; du Bois, A.; Greimel, E.R.; Hedderich, J.; Krause, G.; Venhoff, L.; Loibl, S.; Pfisterer, J. Feasibility, Toxicity and Quality of Life of First-Line Chemotherapy with Platinum/Paclitaxel in Elderly Patients Aged ≥70 Years with Advanced Ovarian Cancer--a Study by the AGO OVAR Germany. Ann. Oncol. 2006, 18, 282–287. [Google Scholar] [CrossRef]
- Pignata, S.; Scambia, G.; Katsaros, D.; Gallo, C.; Pujade-Lauraine, E.; Placido, S.D.; Bologna, A.; Weber, B.; Raspagliesi, F.; Panici, P.B.; et al. Carboplatin plus Paclitaxel Once a Week versus Every 3 Weeks in Patients with Advanced Ovarian Cancer (MITO-7): A Randomised, Multicentre, Open-Label, Phase 3 Trial. Lancet Oncol. 2014, 15, 396–405. [Google Scholar] [CrossRef]
- Chan, J.K.; Brady, M.F.; Penson, R.T.; Huang, H.; Birrer, M.J.; Walker, J.L.; DiSilvestro, P.A.; Rubin, S.C.; Martin, L.P.; Davidson, S.A.; et al. Weekly vs. Every-3-Week Paclitaxel and Carboplatin for Ovarian Cancer. N. Engl. J. Med. 2016, 374, 738–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef]
- Perren, T.J.; Swart, A.M.; Pfisterer, J.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; Kurzeder, C.; et al. A Phase 3 Trial of Bevacizumab in Ovarian Cancer. N. Engl. J. Med. 2011, 365, 2484–2496. [Google Scholar] [CrossRef] [Green Version]
- Valabrega, G.; Pothuri, B.; Oaknin, A.; Graybill, W.; Sanchez, A.B.; Mccormick, C.; Baurain, J.-F.; Hoskins, P.; Denys, H.; O’Cearbhaill, R.E.; et al. Efficacy and Safety of Niraparib in Older Patients (Pts) with Advanced Ovarian Cancer (OC): Results from the PRIMA/ENGOT-OV26/GOG-3012 Trial. Ann. Oncol. 2020, 31, S619. [Google Scholar] [CrossRef]
- Papadimitriou, C.A.; Fountzilas, G.; Aravantinos, G.; Kalofonos, C.; Moulopoulos, L.A.; Briassoulis, E.; Gika, D.; Dimopoulos, M.-A. Second-Line Chemotherapy with Gemcitabine and Carboplatin in Paclitaxel-Pretreated, Platinum-Sensitive Ovarian Cancer Patients: A Hellenic Cooperative Oncology Group Study. Gynecol. Oncol. 2004, 92, 152–159. [Google Scholar] [CrossRef]
- Monk, B.J.; Herzog, T.J.; Kaye, S.B.; Krasner, C.N.; Vermorken, J.B.; Muggia, F.M.; Pujade-Lauraine, E.; Lisyanskaya, A.S.; Makhson, A.N.; Rolski, J.; et al. Trabectedin plus Pegylated Liposomal Doxorubicin in Recurrent Ovarian Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3107–3114. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Martin, A.; Gladieff, L.; Tholander, B.; Stroyakovsky, D.; Gore, M.; Scambia, G.; Kovalenko, N.; Oaknin, A.; Ronco, J.P.; Freudensprung, U.; et al. Efficacy and Safety Results from OCTAVIA, a Single-Arm Phase II Study Evaluating Front-Line Bevacizumab, Carboplatin and Weekly Paclitaxel for Ovarian Cancer. Eur. J. Cancer 2013, 49, 3831–3838. [Google Scholar] [CrossRef] [PubMed]
- Aghajanian, C.; Blank, S.V.; Goff, B.A.; Judson, P.L.; Teneriello, M.G.; Husain, A.; Sovak, M.A.; Yi, J.; Nycum, L.R. OCEANS: A Randomized, Double-Blind, Placebo-Controlled Phase III Trial of Chemotherapy with or without Bevacizumab in Patients with Platinum-Sensitive Recurrent Epithelial Ovarian, Primary Peritoneal, or Fallopian Tube Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 2039–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujade-Lauraine, E.; Ledermann, J.A.; Selle, F.; Gebski, V.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Poveda, A.; Pignata, S.; et al. Olaparib Tablets as Maintenance Therapy in Patients with Platinum-Sensitive, Relapsed Ovarian Cancer and a BRCA1/2 Mutation (SOLO2/ENGOT-Ov21): A Double-Blind, Randomised, Placebo-Controlled, Phase 3 Trial. Lancet Oncol. 2017, 18, 1274–1284. [Google Scholar] [CrossRef] [Green Version]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef] [PubMed]
- Fabbro, M.; Moore, K.N.; Dørum, A.; Tinker, A.V.; Mahner, S.; Bover, I.; Banerjee, S.; Tognon, G.; Goffin, F.; Shapira-Frommer, R.; et al. Efficacy and Safety of Niraparib as Maintenance Treatment in Older Patients (≥70 years) with Recurrent Ovarian Cancer: Results from the ENGOT-OV16/NOVA Trial. Gynecol. Oncol. 2019, 152, 560–567. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.E.; Biganzoli, L.; Canney, P.; Dirix, L.; Mauriac, L.; Chollet, P.; Batter, V.; Ngalula-Kabanga, E.; Dittrich, C.; Piccart, M. A Randomised Phase II Study of Two Different Schedules of Pegylated Liposomal Doxorubicin in Metastatic Breast Cancer (EORTC-10993). Eur. J. Cancer 2006, 42, 882–887. [Google Scholar] [CrossRef]
- Mirza, M.R.; Lundqvist, E.Å.; Birrer, M.J.; dePont Christensen, R.; Nyvang, G.-B.; Malander, S.; Anttila, M.; Werner, T.L.; Lund, B.; Lindahl, G.; et al. Niraparib plus Bevacizumab versus Niraparib Alone for Platinum-Sensitive Recurrent Ovarian Cancer (NSGO-AVANOVA2/ENGOT-Ov24): A Randomised, Phase 2, Superiority Trial. Lancet Oncol. 2019, 20, 1409–1419. [Google Scholar] [CrossRef]
- Omura, G.A.; Brady, M.F.; Look, K.Y.; Averette, H.E.; Delmore, J.E.; Long, H.J.; Wadler, S.; Spiegel, G.; Arbuck, S.G. Phase III Trial of Paclitaxel at Two Dose Levels, the Higher Dose Accompanied by Filgrastim at Two Dose Levels in Platinum-Pretreated Epithelial Ovarian Cancer: An Intergroup Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 2843–2848. [Google Scholar] [CrossRef]
- Kudelka, A.P.; Tresukosol, D.; Edwards, C.L.; Freedman, R.S.; Levenback, C.; Chantarawiroj, P.; Gonzalez de Leon, C.; Kim, E.E.; Madden, T.; Wallin, B.; et al. Phase II Study of Intravenous Topotecan as a 5-Day Infusion for Refractory Epithelial Ovarian Carcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1996, 14, 1552–1557. [Google Scholar] [CrossRef]
- McGuire, W.P.; Blessing, J.A.; Bookman, M.A.; Lentz, S.S.; Dunton, C.J. Topotecan Has Substantial Antitumor Activity as First-Line Salvage Therapy in Platinum-Sensitive Epithelial Ovarian Carcinoma: A Gynecologic Oncology Group Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2000, 18, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Safra, T.; Menczer, J.; Bernstein, R.; Shpigel, S.; Inbar, M.J.; Grisaru, D.; Golan, A.; Levy, T. Efficacy and Toxicity of Weekly Topotecan in Recurrent Epithelial Ovarian and Primary Peritoneal Cancer. Gynecol. Oncol. 2007, 105, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.; Alvarez, R.D.; Andrews, S.; Malone, J.; Bryant, C.; Heilbrun, L.K.; Smith, D.; Schimp, V.; Munkarah, A. Topotecan Weekly Bolus Chemotherapy for Relapsed Platinum-Sensitive Ovarian and Peritoneal Cancers. Gynecol. Oncol. 2008, 109, 346–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutch, D.G.; Orlando, M.; Goss, T.; Teneriello, M.G.; Gordon, A.N.; McMeekin, S.D.; Wang, Y.; Scribner, D.R.; Marciniack, M.; Naumann, R.W.; et al. Randomized Phase III Trial of Gemcitabine Compared with Pegylated Liposomal Doxorubicin in Patients with Platinum-Resistant Ovarian Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2007, 25, 2811–2818. [Google Scholar] [CrossRef] [PubMed]
- Naumann, R.W.; Coleman, R.L.; Burger, R.A.; Sausville, E.A.; Kutarska, E.; Ghamande, S.A.; Gabrail, N.Y.; Depasquale, S.E.; Nowara, E.; Gilbert, L.; et al. PRECEDENT: A Randomized Phase II Trial Comparing Vintafolide (EC145) and Pegylated Liposomal Doxorubicin (PLD) in Combination versus PLD Alone in Patients with Platinum-Resistant Ovarian Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 4400–4406. [Google Scholar] [CrossRef]
- Verschraegen, C.F.; Sittisomwong, T.; Kudelka, A.P.; de Paula Guedes, E.; Steger, M.; Nelson-Taylor, T.; Vincent, M.; Rogers, R.; Atkinson, E.N.; Kavanagh, J.J. Docetaxel for Patients with Paclitaxel-Resistant Müllerian Carcinoma. J. Clin. Oncol. 2000, 18, 2733–2739. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined with Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef]
- Coleman, R.L.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.; Scambia, G.; et al. Rucaparib Maintenance Treatment for Recurrent Ovarian Carcinoma after Response to Platinum Therapy (ARIEL3): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Lond. Engl. 2017, 390, 1949–1961. [Google Scholar] [CrossRef] [Green Version]
- Klotz, L.; Boccon-Gibod, L.; Shore, N.D.; Andreou, C.; Persson, B.-E.; Cantor, P.; Jensen, J.-K.; Olesen, T.K.; Schröder, F.H. The Efficacy and Safety of Degarelix: A 12-Month, Comparative, Randomized, Open-Label, Parallel-Group Phase III Study in Patients with Prostate Cancer. BJU Int. 2008, 102, 1531–1538. [Google Scholar] [CrossRef]
- Small, E.J.; Saad, F.; Chowdhury, S.; Oudard, S.; Hadaschik, B.A.; Graff, J.N.; Olmos, D.; Mainwaring, P.N.; Lee, J.Y.; Uemura, H.; et al. Apalutamide and Overall Survival in Non-Metastatic Castration-Resistant Prostate Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 1813–1820. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; de Bono, J.S.; Spears, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Ritchie, A.W.S.; Amos, C.L.; Gilson, C.; Jones, R.J.; et al. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. N. Engl. J. Med. 2017, 377, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy with Enzalutamide or Placebo in Men with Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar] [CrossRef]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez Soto, Á.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar] [CrossRef]
- Heyns, C.F.; Simonin, M.-P.; Grosgurin, P.; Schall, R.; Porchet, H.C.; South African Triptorelin Study Group. Comparative Efficacy of Triptorelin Pamoate and Leuprolide Acetate in Men with Advanced Prostate Cancer. BJU Int. 2003, 92, 226–231. [Google Scholar] [CrossRef]
- Ahmann, F.R.; Citrin, D.L.; deHaan, H.A.; Guinan, P.; Jordan, V.C.; Kreis, W.; Scott, M.; Trump, D.L. Zoladex: A Sustained-Release, Monthly Luteinizing Hormone-Releasing Hormone Analogue for the Treatment of Advanced Prostate Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1987, 5, 912–917. [Google Scholar] [CrossRef]
- Metz, R.; Namer, M.; Adenis, L.; Audhuy, B.; Bugat, R.; Colombel, P.; Couette, J.E.; Grise, P.; Khater, R.; LePorz, B. Zoladex as Primary Therapy in Advanced Prostatic Cancer. A French Cooperative Trial. Am. J. Clin. Oncol. 1988, 11 (Suppl. S2), S112–S114. [Google Scholar] [CrossRef]
- Gravis, G.; Fizazi, K.; Joly, F.; Oudard, S.; Priou, F.; Esterni, B.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. Androgen-Deprivation Therapy Alone or with Docetaxel in Non-Castrate Metastatic Prostate Cancer (GETUG-AFU 15): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2013, 14, 149–158. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef]
- de Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B.; Saad, F.; et al. Abiraterone and Increased Survival in Metastatic Prostate Cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef] [PubMed]
- Mulders, P.F.A.; Molina, A.; Marberger, M.; Saad, F.; Higano, C.S.; Chi, K.N.; Li, J.; Kheoh, T.; Haqq, C.M.; Fizazi, K. Efficacy and Safety of Abiraterone Acetate in an Elderly Patient Subgroup (Aged 75 and Older) with Metastatic Castration-Resistant Prostate Cancer after Docetaxel-Based Chemotherapy. Eur. Urol. 2014, 65, 875–883. [Google Scholar] [CrossRef]
- Ryan, C.J.; Smith, M.R.; de Bono, J.S.; Molina, A.; Logothetis, C.J.; de Souza, P.; Fizazi, K.; Mainwaring, P.; Piulats, J.M.; Ng, S.; et al. Abiraterone in Metastatic Prostate Cancer without Previous Chemotherapy. N. Engl. J. Med. 2013, 368, 138–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penson, D.F.; Armstrong, A.J.; Concepcion, R.; Agarwal, N.; Olsson, C.; Karsh, L.; Dunshee, C.; Wang, F.; Wu, K.; Krivoshik, A.; et al. Enzalutamide Versus Bicalutamide in Castration-Resistant Prostate Cancer: The STRIVE Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 2098–2106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.-E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased Survival with Enzalutamide in Prostate Cancer after Chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fizazi, K.; Scher, H.I.; Miller, K.; Basch, E.; Sternberg, C.N.; Cella, D.; Forer, D.; Hirmand, M.; de Bono, J.S. Effect of Enzalutamide on Time to First Skeletal-Related Event, Pain, and Quality of Life in Men with Castration-Resistant Prostate Cancer: Results from the Randomised, Phase 3 AFFIRM Trial. Lancet Oncol. 2014, 15, 1147–1156. [Google Scholar] [CrossRef]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in Metastatic Prostate Cancer before Chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for Advanced Prostate Cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [Green Version]
- Hervonen, P.; Joensuu, H.; Joensuu, T.; Claes, G.; Ray, M.; Ulrika, H.; Paul, N.; Tiina, L.; Akseli, H.; Igor, Z.; et al. Biweekly Docetaxel Is Better Tolerated than Conventional Three-Weekly Dosing for Advanced Hormone-Refractory Prostate Cancer. Anticancer Res. 2012, 32, 953–956. [Google Scholar]
- de Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.-P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus Cabazitaxel or Mitoxantrone for Metastatic Castration-Resistant Prostate Cancer Progressing after Docetaxel Treatment: A Randomised Open-Label Trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- De Bono, J.S.; Hardy-Bessard, A.-C.; Choung-So, K.; Geczi, L.; Ford, D.; Mouray, L.; Carles, J.; Parente, P.; Kacso, G.; Chadjaa, M.; et al. Phase III Non-Inferiority Study of Cabazitaxel (C) 20 Mg/M2 (C20) versus 25 Mg/M2 (C25) in Patients (Pts) with Metastatic Castration-Resistant Prostate Cancer (MCRPC) Previously Treated with Docetaxel (D). J. Clin. Oncol. 2016, 34, 5008. [Google Scholar] [CrossRef]
- Parker, C.; Finkelstein, S.E.; Michalski, J.M.; O’Sullivan, J.M.; Bruland, Ø.; Vogelzang, N.J.; Coleman, R.E.; Nilsson, S.; Sartor, O.; Li, R.; et al. Efficacy and Safety of Radium-223 Dichloride in Symptomatic Castration-Resistant Prostate Cancer Patients with or without Baseline Opioid Use From the Phase 3 ALSYMPCA Trial. Eur. Urol. 2016, 70, 875–883. [Google Scholar] [CrossRef] [Green Version]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef] [PubMed]
- Dreicer, R.; Manola, J.; Roth, B.J.; See, W.A.; Kuross, S.; Edelman, M.J.; Hudes, G.R.; Wilding, G. Phase III Trial of Methotrexate, Vinblastine, Doxorubicin, and Cisplatin versus Carboplatin and Paclitaxel in Patients with Advanced Carcinoma of the Urothelium. Cancer 2004, 100, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; de Mulder, P.; Schornagel, J.H.; Theodore, C.; Fossa, S.D.; van Oosterom, A.T.; Witjes, J.A.; Spina, M.; van Groeningen, C.J.; Duclos, B.; et al. Seven Year Update of an EORTC Phase III Trial of High-Dose Intensity M-VAC Chemotherapy and G-CSF versus Classic M-VAC in Advanced Urothelial Tract Tumours. Eur. J. Cancer 2006, 42, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; de Mulder, P.H.; Schornagel, J.H.; Théodore, C.; Fossa, S.D.; van Oosterom, A.T.; Witjes, F.; Spina, M.; van Groeningen, C.J.; de Balincourt, C.; et al. Randomized Phase III Trial of High-Dose-Intensity Methotrexate, Vinblastine, Doxorubicin, and Cisplatin (MVAC) Chemotherapy and Recombinant Human Granulocyte Colony-Stimulating Factor versus Classic MVAC in Advanced Urothelial Tract Tumors: European Organization for Research and Treatment of Cancer Protocol No. 30924. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 2638–2646. [Google Scholar]
- von der Maase, H. Gemcitabine in Locally Advanced and/or Metastatic Bladder Cancer. Crit. Rev. Oncol. Hematol. 2000, 34, 175–183. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]
- Bellmunt, J.; Théodore, C.; Demkov, T.; Komyakov, B.; Sengelov, L.; Daugaard, G.; Caty, A.; Carles, J.; Jagiello-Gruszfeld, A.; Karyakin, O.; et al. Phase III Trial of Vinflunine Plus Best Supportive Care Compared with Best Supportive Care Alone After a Platinum-Containing Regimen in Patients with Advanced Transitional Cell Carcinoma of the Urothelial Tract. J. Clin. Oncol. 2009, 27, 4454–4461. [Google Scholar] [CrossRef]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, J.E.; O’Donnell, P.H.; Balar, A.V.; McGregor, B.A.; Heath, E.I.; Yu, E.Y.; Galsky, M.D.; Hahn, N.M.; Gartner, E.M.; Pinelli, J.M.; et al. Pivotal Trial of Enfortumab Vedotin in Urothelial Carcinoma After Platinum and Anti-Programmed Death 1/Programmed Death Ligand 1 Therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 2592–2600. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Rosenberg, J.E.; Sonpavde, G.P.; Loriot, Y.; Durán, I.; Lee, J.-L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Wu, C.; et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Lonardi, S.; Sobrero, A.; Rosati, G.; Di Bartolomeo, M.; Ronzoni, M.; Aprile, G.; Massida, B.; Scartozzi, M.; Banzi, M.; Zampino, M.G.; et al. Phase III Trial Comparing 3-6 Months of Adjuvant FOLFOX4/XELOX in Stage II-III Colon Cancer: Safety and Compliance in the TOSCA Trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 2074–2081. [Google Scholar] [CrossRef] [PubMed]
- Iveson, T.J.; Kerr, R.S.; Saunders, M.P.; Cassidy, J.; Hollander, N.H.; Tabernero, J.; Haydon, A.; Glimelius, B.; Harkin, A.; Allan, K.; et al. 3 versus 6 Months of Adjuvant Oxaliplatin-Fluoropyrimidine Combination Therapy for Colorectal Cancer (SCOT): An International, Randomised, Phase 3, Non-Inferiority Trial. Lancet Oncol. 2018, 19, 562–578. [Google Scholar] [CrossRef] [Green Version]
- André, T.; Vernerey, D.; Mineur, L.; Bennouna, J.; Desrame, J.; Faroux, R.; Fratte, S.; Hug de Larauze, M.; Paget-Bailly, S.; Chibaudel, B.; et al. Three Versus 6 Months of Oxaliplatin-Based Adjuvant Chemotherapy for Patients with Stage III Colon Cancer: Disease-Free Survival Results From a Randomized, Open-Label, International Duration Evaluation of Adjuvant (IDEA) France, Phase III Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 1469–1477. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Oxaliplatin, Fluorouracil, and Leucovorin as Adjuvant Treatment for Colon Cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twelves, C.; Wong, A.; Nowacki, M.P.; Abt, M.; Burris, H.; Carrato, A.; Cassidy, J.; Cervantes, A.; Fagerberg, J.; Georgoulias, V.; et al. Capecitabine as Adjuvant Treatment for Stage III Colon Cancer. N. Engl. J. Med. 2005, 352, 2696–2704. [Google Scholar] [CrossRef]
- Alberts, S.R.; Sargent, D.J.; Nair, S.; Mahoney, M.R.; Mooney, M.; Thibodeau, S.N.; Smyrk, T.C.; Sinicrope, F.A.; Chan, E.; Gill, S.; et al. Effect of Oxaliplatin, Fluorouracil, and Leucovorin with or without Cetuximab on Survival among Patients with Resected Stage III Colon Cancer: A Randomized Trial. JAMA 2012, 307, 1383–1393. [Google Scholar] [CrossRef] [Green Version]
- Taieb, J.; Tabernero, J.; Mini, E.; Subtil, F.; Folprecht, G.; Van Laethem, J.-L.; Thaler, J.; Bridgewater, J.; Petersen, L.N.; Blons, H.; et al. Oxaliplatin, Fluorouracil, and Leucovorin with or without Cetuximab in Patients with Resected Stage III Colon Cancer (PETACC-8): An Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2014, 15, 862–873. [Google Scholar] [CrossRef]
- Cunningham, D.; Lang, I.; Marcuello, E.; Lorusso, V.; Ocvirk, J.; Shin, D.B.; Jonker, D.; Osborne, S.; Andre, N.; Waterkamp, D.; et al. Bevacizumab plus Capecitabine versus Capecitabine Alone in Elderly Patients with Previously Untreated Metastatic Colorectal Cancer (AVEX): An Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2013, 14, 1077–1085. [Google Scholar] [CrossRef]
- Madajewicz, S.; Waterhouse, D.M.; Ritch, P.S.; Khan, M.Q.; Higby, D.J.; Leichman, C.G.; Malik, S.K.; Hentschel, P.; Gill, J.F.; Zhao, L.; et al. Multicenter, Randomized Phase II Trial of Bevacizumab plus Folinic Acid, Fluorouracil, Gemcitabine (FFG) versus Bevacizumab plus Folinic Acid, Fluorouracil, Oxaliplatin (FOLFOX4) as First-Line Therapy for Patients with Advanced Colorectal Cancer. Investig. New Drugs 2010, 30, 772–778. [Google Scholar] [CrossRef]
- Zhao, C.; Zhang, H.; Ye, Y.; Sun, J.; Li, P. Meta-Analysis of TOMOX versus FOLFOX Regimens for the Treatment of Advanced Colorectal Cancer. Int. J. Clin. Exp. Med. 2016, 9, 5616–5629. [Google Scholar]
- Benavides, M.; Pericay, C.; Valladares-Ayerbes, M.; Gil-Calle, S.; Massutí, B.; Aparicio, J.; Dueñas, R.; González-Flores, E.; Carrato, A.; Marcuello, E.; et al. Oxaliplatin in Combination with Infusional 5-Fluorouracil as First-Line Chemotherapy for Elderly Patients with Metastatic Colorectal Cancer: A Phase II Study of the Spanish Cooperative Group for the Treatment of Digestive Tumors. Clin. Colorectal Cancer 2012, 11, 200–206. [Google Scholar] [CrossRef]
- Cassidy, J.; Tabernero, J.; Twelves, C.; Brunet, R.; Butts, C.; Conroy, T.; Debraud, F.; Figer, A.; Grossmann, J.; Sawada, N.; et al. XELOX (Capecitabine plus Oxaliplatin): Active First-Line Therapy for Patients with Metastatic Colorectal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 2084–2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twelves, C.J.; Butts, C.A.; Cassidy, J.; Conroy, T.; de Braud, F.; Diaz-Rubio, E.; Tabernero, J.M.; Schoffski, P.; Figer, A.; Brunet, R.; et al. Capecitabine/Oxaliplatin, a Safe and Active First-Line Regimen for Older Patients with Metastatic Colorectal Cancer: Post Hoc Analysis of a Large Phase II Study. Clin. Colorectal Cancer 2005, 5, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Feliu, J.; Salud, A.; Escudero, P.; Lopez-Gómez, L.; Bolaños, M.; Galán, A.; Vicent, J.-M.; Yubero, A.; Losa, F.; De Castro, J.; et al. XELOX (Capecitabine plus Oxaliplatin) as First-Line Treatment for Elderly Patients over 70 Years of Age with Advanced Colorectal Cancer. Br. J. Cancer 2006, 94, 969–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grande, C.; Quintero, G.; Candamio, S.; París Bouzas, L.; Villanueva, M.J.; Campos, B.; Gallardo, E.; Alvarez, E.; Casal, J.; Mel, J.R. Biweekly XELOX (Capecitabine and Oxaliplatin) as First-Line Treatment in Elderly Patients with Metastatic Colorectal Cancer. J. Geriatr. Oncol. 2013, 4, 114–121. [Google Scholar] [CrossRef]
- Seymour, M.T.; Thompson, L.C.; Wasan, H.S.; Middleton, G.; Brewster, A.E.; Shepherd, S.F.; O’Mahony, M.S.; Maughan, T.S.; Parmar, M.; Langley, R.E.; et al. Chemotherapy Options in Elderly and Frail Patients with Metastatic Colorectal Cancer (MRC FOCUS2): An Open-Label, Randomised Factorial Trial. Lancet Lond. Engl. 2011, 377, 1749–1759. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.-B.; Lee, N.-S.; Kim, H.-J.; Kim, K.-H.; Kim, H.-J.; Kim, C.-K.; Lee, K.-T.; Park, S.-K.; Won, J.-H.; Hong, D.-S.; et al. A Phase II Study of Irinotecan, 5-Fluorouracil and Leucovorin for Treatment in Patients with Previously Untreated Advanced Colorectal Cancer. Cancer Res. Treat. Cancer Res. Treat. 2006, 38, 72–77. [Google Scholar] [CrossRef]
- Falcone, A.; Ricci, S.; Brunetti, I.; Pfanner, E.; Allegrini, G.; Barbara, C.; Crinò, L.; Benedetti, G.; Evangelista, W.; Fanchini, L.; et al. Phase III Trial of Infusional Fluorouracil, Leucovorin, Oxaliplatin, and Irinotecan (FOLFOXIRI) Compared with Infusional Fluorouracil, Leucovorin, and Irinotecan (FOLFIRI) As First-Line Treatment for Metastatic Colorectal Cancer: The Gruppo Oncologico Nord Ovest. J. Clin. Oncol. 2007, 25, 1670–1676. [Google Scholar] [CrossRef]
- Moehler, M.; Ababneh, Y.; Verpoort, K.; Schmidt, B.; Musch, R.; Soeling, U.; Maintz, C.; Siebler, J.; Schimanski, C.C.; Galle, P.R.; et al. Efficacy and Safety of Irinotecan-Based Chemotherapy for Advanced Colorectal Cancer Outside Clinical Trials: An Observational Study. Oncol. Res. Treat. 2010, 33, 684–690. [Google Scholar] [CrossRef] [Green Version]
- Cutsem, E.V.; Lenz, H.-J.; Köhne, C.-H.; Heinemann, V.; Tejpar, S.; Melezínek, I.; Beier, F.; Stroh, C.; Rougier, P.; van Krieken, J.H.; et al. Fluorouracil, Leucovorin, and Irinotecan Plus Cetuximab Treatment and RAS Mutations in Colorectal Cancer. J. Clin. Oncol. 2015, 33, 692–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Kuang, M.; Gong, Y.; Cao, C.; Chen, J.; Tang, C. Survival Benefit and Safety of the Combinations of FOLFOXIRI ± Bevacizumab versus the Combinations of FOLFIRI ± Bevacizumab as First-Line Treatment for Unresectable Metastatic Colorectal Cancer: A Meta-Analysis. OncoTargets Ther. 2016, 9, 4833. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Bang, S.-M.; Cho, E.K.; Baek, J.H.; Oh, J.H.; Im, S.A.; Park, Y.S.; Shin, D.B.; Lee, J.H. First-Line Chemotherapy with Irinotecan plus Capecitabine for Advanced Colorectal Cancer. Oncology 2004, 66, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, T.; Lopez, T.; Vukelja, S.J.; Encarnacion, C.; Boehm, K.A.; Asmar, L. Results of a Phase II Open-Label Study of Capecitabine in Combination with Irinotecan as First-Line Treatment for Metastatic Colorectal Cancer. Clin. Colorectal Cancer 2005, 5, 50–56. [Google Scholar] [CrossRef]
- Borner, M.M.; Bernhard, J.; Dietrich, D.; Popescu, R.; Wernli, M.; Saletti, P.; Rauch, D.; Herrmann, R.; Koeberle, D.; Honegger, H.; et al. A Randomized Phase II Trial of Capecitabine and Two Different Schedules of Irinotecan in First-Line Treatment of Metastatic Colorectal Cancer: Efficacy, Quality-of-Life and Toxicity. Ann. Oncol. 2005, 16, 282–288. [Google Scholar] [CrossRef]
- Choi, C.K.K.; Chan, R.T.T.; Tung, S.Y.; Lui, L.; Siu, S.; Au, G.K.H.; Ho, J.W.C.; Law, W.L. Efficacy of Combination Chemotherapy with Irinotecan (CPT-11) plus Capecitabine in Patients with Metastatic or Advanced Colorectal Carcinoma—A Dual-Centre Phase II Study: The MAC-6. Clin. Oncol. 2008, 20, 168–175. [Google Scholar] [CrossRef]
- Skof, E.; Rebersek, M.; Hlebanja, Z.; Ocvirk, J. Capecitabine plus Irinotecan (XELIRI Regimen) Compared to 5-FU/LV plus Irinotecan (FOLFIRI Regimen) as Neoadjuvant Treatment for Patients with Unresectable Liver-Only Metastases of Metastatic Colorectal Cancer: A Randomised Prospective Phase II Trial. BMC Cancer 2009, 9, 120. [Google Scholar] [CrossRef] [Green Version]
- Gennatas, C.; Michalaki, V.; Gennatas, S.; Papalambros, E. Irinotecan plus Capecitabine as First-Line Chemotherapy in Advanced Colorectal Cancer. Anticancer Res. 2008, 28, 1923–1926. [Google Scholar]
- Kim, T.W.; Kang, W.K.; Chang, H.M.; Park, J.O.; Ryoo, B.Y.; Ahn, J.S.; Zang, D.Y.; Lee, K.H.; Kang, Y.K.; Kim, S.R.; et al. Multicenter Phase II Study of Oral Capecitabine plus Irinotecan as First-Line Chemotherapy in Advanced Colorectal Cancer: A Korean Cancer Study Group Trial. Acta Oncol. 2005, 44, 230–235. [Google Scholar] [CrossRef]
- Garcia-Alfonso, P.; Muñoz-Martin, A.; Mendez-Ureña, M.; Quiben-Pereira, R.; Gonzalez-Flores, E.; Perez-Manga, G. Capecitabine in Combination with Irinotecan (XELIRI), Administered as a 2-Weekly Schedule, as First-Line Chemotherapy for Patients with Metastatic Colorectal Cancer: A Phase II Study of the Spanish GOTI Group. Br. J. Cancer 2009, 101, 1039–1043. [Google Scholar] [CrossRef]
- Guion-Dusserre, J.-F.; Bertaut, A.; Ghiringhelli, F.; Vincent, J.; Quipourt, V.; Marilier, S.; Tharin, Z.; Bengrine-Lefevre, L. Folfirinox in Elderly Patients with Pancreatic or Colorectal Cancer-Tolerance and Efficacy. World J. Gastroenterol. 2016, 22, 9378. [Google Scholar] [CrossRef] [PubMed]
- Vasile, E.; Masi, G.; Fornaro, L.; Cupini, S.; Loupakis, F.; Bursi, S.; Petrini, I.; Di Donato, S.; Brunetti, I.M.; Ricci, S.; et al. A Multicenter Phase II Study of the Combination of Oxaliplatin, Irinotecan and Capecitabine in the First-Line Treatment of Metastatic Colorectal Cancer. Br. J. Cancer 2009, 100, 1720–1724. [Google Scholar] [CrossRef] [Green Version]
- Bajetta, E.; Verzoni, E.; Ferrario, E.; Dotti, K.; Gevorgyan, A.; Celio, L. Feasibility Study of Biweekly Capecitabine, Oxaliplatin, and Irinotecan in Patients with Untreated Advanced Gastric Cancer. Tumori J. 2009, 95, 43–47. [Google Scholar] [CrossRef]
- Recchia, F.; Nuzzo, A.; Lalli, A.; Di Lullo, L.; De Filippis, S.; Saggio, G.; Di Blasio, A.; Rea, S. Multicenter Phase II Study of CPT-11 Fractionated over Two Days with Bimonthly Leucovorin and 5-Fluorouracil in Patients with Metastatic Colorectal Cancer. Anticancer Res. 2003, 23, 2903–2908. [Google Scholar] [PubMed]
- Bécouarn, Y.; Senesse, P.; Thézenas, S.; Boucher, E.; Adenis, A.; Cany, L.; Jacob, J.H.; Cvitkovic, F.; Montoto-Grillot, C.; Ychou, M.; et al. A Randomized Phase II Trial Evaluating Safety and Efficacy of an Experimental Chemotherapy Regimen (Irinotecan + Oxaliplatin, IRINOX) and Two Standard Arms (LV5 FU2 + Irinotecan or LV5 FU2 + Oxaliplatin) in First-Line Metastatic Colorectal Cancer: A Study of the Digestive Group of the Fédération Nationale Des Centres de Lutte Contre Le Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2007, 18, 2000–2005. [Google Scholar] [CrossRef]
- Cunningham, D.; Zalcberg, J.R.; Rath, U.; Olver, I.; Van Cutsem, E.; Svensson, C.; Scitz, J.F.; Harper, P.; Kerr, D.; Perez-Manga, G.; et al. ‘Tomudex’ (ZD1694): Results of a Randomised Trial in Advanced Colorectal Cancer Demonstrate Efficacy and Reduced Mucositis and Leucopenia. Eur. J. Cancer 1995, 31, 1945–1954. [Google Scholar] [CrossRef]
- Cascinu, S.; Graziano, F.; Ferraù, F.; Catalano, V.; Massacesi, C.; Santini, D.; Silva, R.R.; Barni, S.; Zaniboni, A.; Battelli, N.; et al. Raltitrexed plus Oxaliplatin (TOMOX) as First-Line Chemotherapy for Metastatic Colorectal Cancer. A Phase II Study of the Italian Group for the Study of Gastrointestinal Tract Carcinomas (GISCAD). Ann. Oncol. 2002, 13, 716–720. [Google Scholar] [CrossRef]
- Feliu, J.; Castañón, C.; Salud, A.; Mel, J.R.; Escudero, P.; Pelegrín, A.; López-Gómez, L.; Ruiz, M.; González, E.; Juárez, F.; et al. Phase II Randomised Trial of Raltitrexed–Oxaliplatin vs Raltitrexed–Irinotecan as First-Line Treatment in Advanced Colorectal Cancer. Br. J. Cancer 2005, 93, 1230–1235. [Google Scholar] [CrossRef] [Green Version]
- Feliu, J.; Salud, A.; Escudero, P.; López-Gómez, L.; Pericay, C.; Castañón, C.; de Tejada, M.R.L.; Rodríguez-García, J.M.; Martínez, M.P.; Martín, M.S.; et al. Irinotecan plus Raltitrexed as First-Line Treatment in Advanced Colorectal Cancer: A Phase II Study. Br. J. Cancer 2004, 90, 1502–1507. [Google Scholar] [CrossRef]
- Loupakis, F.; Cremolini, C.; Masi, G.; Lonardi, S.; Zagonel, V.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Ronzoni, M.; Spadi, R.; et al. Initial Therapy with FOLFOXIRI and Bevacizumab for Metastatic Colorectal Cancer. N. Engl. J. Med. 2014, 371, 1609–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinemann, V.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.-E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; Seipelt, G.; et al. FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First-Line Treatment for Patients with Metastatic Colorectal Cancer (FIRE-3): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2014, 15, 1065–1075. [Google Scholar] [CrossRef]
- Yamazaki, K.; Nagase, M.; Tamagawa, H.; Ueda, S.; Tamura, T.; Murata, K.; Nakajima, T.E.; Baba, E.; Tsuda, M.; Moriwaki, T.; et al. Randomized Phase III Study of Bevacizumab plus FOLFIRI and Bevacizumab plus MFOLFOX6 as First-Line Treatment for Patients with Metastatic Colorectal Cancer (WJOG4407G). Ann. Oncol. 2016, 27, 1539–1546. [Google Scholar] [CrossRef]
- García-Alfonso, P.; Muñoz-Martin, A.J.; Alvarez-Suarez, S.; Jerez-Gilarranz, Y.; Riesco-Martinez, M.; Khosravi, P.; Martin, M. Bevacizumab in Combination with Biweekly Capecitabine and Irinotecan, as First-Line Treatment for Patients with Metastatic Colorectal Cancer. Br. J. Cancer 2010, 103, 1524–1528. [Google Scholar] [CrossRef]
- Garcia-Alfonso, P.; Chaves, M.; Muñoz, A.; Salud, A.; García-Gonzalez, M.; Grávalos, C.; Massuti, B.; González-Flores, E.; Queralt, B.; López-Ladrón, A.; et al. Capecitabine and Irinotecan with Bevacizumab 2-Weekly for Metastatic Colorectal Cancer: The Phase II AVAXIRI Study. BMC Cancer 2015, 15, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, Y.; Takahari, D.; Matsumoto, H.; Baba, H.; Nakamura, M.; Yoshida, K.; Yoshida, M.; Iwamoto, S.; Shimada, K.; Komatsu, Y.; et al. Leucovorin, Fluorouracil, and Oxaliplatin plus Bevacizumab versus S-1 and Oxaliplatin plus Bevacizumab in Patients with Metastatic Colorectal Cancer (SOFT): An Open-Label, Non-Inferiority, Randomised Phase 3 Trial. Lancet Oncol. 2013, 14, 1278–1286. [Google Scholar] [CrossRef]
- Uehara, K.; Hiramatsu, K.; Maeda, A.; Sakamoto, E.; Inoue, M.; Kobayashi, S.; Tojima, Y.; Yoshioka, Y.; Nakayama, G.; Yatsuya, H.; et al. Neoadjuvant Oxaliplatin and Capecitabine and Bevacizumab without Radiotherapy for Poor-Risk Rectal Cancer: N-SOG 03 Phase II Trial. Jpn. J. Clin. Oncol. 2013, 43, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Feliu, J.; Salud, A.; Safont, M.J.; García-Girón, C.; Aparicio, J.; Vera, R.; Serra, O.; Casado, E.; Jorge, M.; Escudero, P.; et al. First-Line Bevacizumab and Capecitabine-Oxaliplatin in Elderly Patients with MCRC: GEMCAD Phase II BECOX Study. Br. J. Cancer 2014, 111, 241–248. [Google Scholar] [CrossRef]
- Munemoto, Y.; Kanda, M.; Ishibashi, K.; Hata, T.; Kobayashi, M.; Hasegawa, J.; Fukunaga, M.; Takagane, A.; Otsuji, T.; Miyake, Y.; et al. Capecitabine and Oxaliplatin Combined with Bevacizumab Are Feasible for Treating Selected Japanese Patients at Least 75 Years of Age with Metastatic Colorectal Cancer. BMC Cancer 2015, 15, 786. [Google Scholar] [CrossRef] [Green Version]
- Naeim, A.; Ward, P.R.; Wang, H.-J.; Dichmann, R.; Liem, A.K.D.; Chan, D.; Patel, R.; Hu, E.H.L.; Tchekmedyian, N.S.; Wainberg, Z.A.; et al. A Phase II Trial of Frontline Capecitabine and Bevacizumab in Poor Performance Status and/or Elderly Patients with Metastatic Colorectal Cancer. J. Geriatr. Oncol. 2013, 4, 302–309. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Tabernero, J.; Lakomy, R.; Prenen, H.; Prausová, J.; Macarulla, T.; Ruff, P.; van Hazel, G.A.; Moiseyenko, V.; Ferry, D.; et al. Addition of Aflibercept to Fluorouracil, Leucovorin, and Irinotecan Improves Survival in a Phase III Randomized Trial in Patients with Metastatic Colorectal Cancer Previously Treated with an Oxaliplatin-Based Regimen. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 3499–3506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonker, D.J.; O’Callaghan, C.J.; Karapetis, C.S.; Zalcberg, J.R.; Tu, D.; Au, H.-J.; Berry, S.R.; Krahn, M.; Price, T.; Simes, R.J.; et al. Cetuximab for the Treatment of Colorectal Cancer. N. Engl. J. Med. 2007, 357, 2040–2048. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Plana, J.; Pericay, C.; Quintero, G.; Alonso, V.; Salud, A.; Mendez, M.; Salgado, M.; Saigi, E.; Cirera, L.; ACROSS Study Group. Biweekly Cetuximab in Combination with FOLFOX-4 in the First-Line Treatment of Wild-Type KRAS Metastatic Colorectal Cancer: Final Results of a Phase II, Open-Label, Clinical Trial (OPTIMIX-ACROSS Study). BMC Cancer 2014, 14, 865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soda, H.; Maeda, H.; Hasegawa, J.; Takahashi, T.; Hazama, S.; Fukunaga, M.; Kono, E.; Kotaka, M.; Sakamoto, J.; Nagata, N.; et al. Multicenter Phase II Study of FOLFOX or Biweekly XELOX and Erbitux (Cetuximab) as First-Line Therapy in Patients with Wild-Type KRAS/BRAF Metastatic Colorectal Cancer: The FLEET Study. BMC Cancer 2015, 15, 695. [Google Scholar] [CrossRef] [PubMed]
- Assenat, E.; Desseigne, F.; Thezenas, S.; Viret, F.; Mineur, L.; Kramar, A.; Samalin, E.; Portales, F.; Bibeau, F.; Crapez-Lopez, E.; et al. Cetuximab Plus FOLFIRINOX (ERBIRINOX) as First-Line Treatment for Unresectable Metastatic Colorectal Cancer: A Phase II Trial. Oncologist 2011, 16, 1557–1564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, M.J.; Hong, Y.S.; Kim, K.; Kim, S.Y.; Baek, J.Y.; Ryu, M.-H.; Lee, J.-L.; Chang, H.M.; Kim, M.-J.; Chang, H.J.; et al. Biweekly Cetuximab plus Irinotecan as Second-Line Chemotherapy for Patients with Irinotecan-Refractory and KRAS Wild-Type Metastatic Colorectal Cancer According to Epidermal Growth Factor Receptor Expression Status. Investig. New Drugs 2011, 30, 1607–1613. [Google Scholar] [CrossRef]
- Eng, C.; Bessudo, A.; Hart, L.L.; Severtsev, A.; Gladkov, O.; Müller, L.; Kopp, M.V.; Vladimirov, V.; Langdon, R.; Kotiv, B.; et al. A Randomized, Placebo-Controlled, Phase 1/2 Study of Tivantinib (ARQ 197) in Combination with Irinotecan and Cetuximab in Patients with Metastatic Colorectal Cancer with Wild-Type KRAS Who Have Received First-Line Systemic Therapy. Int. J. Cancer 2016, 139, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Peeters, M.; Price, T.J.; Cervantes, A.; Sobrero, A.F.; Ducreux, M.; Hotko, Y.; André, T.; Chan, E.; Lordick, F.; Punt, C.J.A.; et al. Randomized Phase III Study of Panitumumab with Fluorouracil, Leucovorin, and Irinotecan (FOLFIRI) Compared with FOLFIRI Alone as Second-Line Treatment in Patients with Metastatic Colorectal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 4706–4713. [Google Scholar] [CrossRef]
- Grothey, A.; Cutsem, E.V.; Sobrero, A.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Regorafenib Monotherapy for Previously Treated Metastatic Colorectal Cancer (CORRECT): An International, Multicentre, Randomised, Placebo-Controlled, Phase 3 Trial. Lancet 2013, 381, 303–312. [Google Scholar] [CrossRef]
- Aparicio, T.; Darut-Jouve, A.; Khemissa Akouz, F.; Montérymard, C.; Artru, P.; Cany, L.; Romano, O.; Valenza, B.; Le Foll, C.; Delbaldo, C.; et al. Single-Arm Phase II Trial to Evaluate Efficacy and Tolerance of Regorafenib Monotherapy in Patients over 70 with Previously Treated Metastatic Colorectal Adenocarcinoma FFCD 1404 – REGOLD. J. Geriatr. Oncol. 2020, 11, 1255–1262. [Google Scholar] [CrossRef]
- Mayer, R.J.; Van Cutsem, E.; Falcone, A.; Yoshino, T.; Garcia-Carbonero, R.; Mizunuma, N.; Yamazaki, K.; Shimada, Y.; Tabernero, J.; Komatsu, Y.; et al. Randomized Trial of TAS-102 for Refractory Metastatic Colorectal Cancer. N. Engl. J. Med. 2015, 372, 1909–1919. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, P.; Yilmaz, M.; Möller, S.; Zitnjak, D.; Krogh, M.; Petersen, L.N.; Poulsen, L.Ø.; Winther, S.B.; Thomsen, K.G.; Qvortrup, C. TAS-102 with or without Bevacizumab in Patients with Chemorefractory Metastatic Colorectal Cancer: An Investigator-Initiated, Open-Label, Randomised, Phase 2 Trial. Lancet Oncol. 2020, 21, 412–420. [Google Scholar] [CrossRef]
- Kuboki, Y.; Nishina, T.; Shinozaki, E.; Yamazaki, K.; Shitara, K.; Okamoto, W.; Kajiwara, T.; Matsumoto, T.; Tsushima, T.; Mochizuki, N.; et al. TAS-102 plus Bevacizumab for Patients with Metastatic Colorectal Cancer Refractory to Standard Therapies (C-TASK FORCE): An Investigator-Initiated, Open-Label, Single-Arm, Multicentre, Phase 1/2 Study. Lancet Oncol. 2017, 18, 1172–1181. [Google Scholar] [CrossRef]
- Kopetz, S.; Grothey, A.; Yaeger, R.; Van Cutsem, E.; Desai, J.; Yoshino, T.; Wasan, H.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N. Engl. J. Med. 2019, 381, 1632–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- André, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Schiller, J.H.; Harrington, D.; Belani, C.P.; Langer, C.; Sandler, A.; Krook, J.; Zhu, J.; Johnson, D.H. Comparison of Four Chemotherapy Regimens for Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2002, 346, 92–98. [Google Scholar] [CrossRef]
- Pilkington, G.; Boland, A.; Brown, T.; Oyee, J.; Bagust, A.; Dickson, R. A Systematic Review of the Clinical Effectiveness of First-Line Chemotherapy for Adult Patients with Locally Advanced or Metastatic Non-Small Cell Lung Cancer. Thorax 2015, 70, 359–367. [Google Scholar] [CrossRef] [Green Version]
- Patel, J.D.; Socinski, M.A.; Garon, E.B.; Reynolds, C.H.; Spigel, D.R.; Olsen, M.R.; Hermann, R.C.; Jotte, R.M.; Beck, T.; Richards, D.A.; et al. PointBreak: A Randomized Phase III Study of Pemetrexed Plus Carboplatin and Bevacizumab Followed by Maintenance Pemetrexed and Bevacizumab Versus Paclitaxel Plus Carboplatin and Bevacizumab Followed by Maintenance Bevacizumab in Patients with Stage IIIB or IV Nonsquamous Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2013, 31, 4349–4357. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Hellmann, M.D.; Brahmer, J.R.; Juergens, R.A.; Borghaei, H.; Gettinger, S.; Chow, L.Q.; Gerber, D.E.; Laurie, S.A.; Goldman, J.W.; et al. Nivolumab in Combination with Platinum-Based Doublet Chemotherapy for First-Line Treatment of Advanced Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 2969. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Kaiser, R.; Mellemgaard, A.; Douillard, J.-Y.; Orlov, S.; Krzakowski, M.; von Pawel, J.; Gottfried, M.; Bondarenko, I.; Liao, M.; et al. Docetaxel plus Nintedanib versus Docetaxel plus Placebo in Patients with Previously Treated Non-Small-Cell Lung Cancer (LUME-Lung 1): A Phase 3, Double-Blind, Randomised Controlled Trial. Lancet Oncol. 2014, 15, 143–155. [Google Scholar] [CrossRef]
- Font, A.; Moyano, A.J.; Puerto, J.M.; Tres, A.; Garcia-Giron, C.; Barneto, I.; Anton, A.; Sanchez, J.J.; Salvador, A.; Rosell, R. Increasing Dose Intensity of Cisplatin-Etoposide in Advanced Nonsmall Cell Lung Carcinoma: A Phase III Randomized Trial of the Spanish Lung Cancer Group. Cancer 1999, 85, 855–863. [Google Scholar] [CrossRef]
- Barlesi, F.; Chouaid, C.; Crequit, J.; Le Caer, H.; Pujol, J.-L.; Legodec, J.; Vergnenegre, A.; Le Treut, J.; Fabre-Guillevin, E.; Loundou, A.; et al. A Randomized Trial Comparing Adjuvant Chemotherapy with Gemcitabine plus Cisplatin with Docetaxel plus Cisplatin in Patients with Completely Resected Non-Small-Cell Lung Cancer with Quality of Life as the Primary Objective. Interact. Cardiovasc. Thorac. Surg. 2015, 20, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quoix, E.; Zalcman, G.; Oster, J.-P.; Westeel, V.; Pichon, E.; Lavolé, A.; Dauba, J.; Debieuvre, D.; Souquet, P.-J.; Bigay-Game, L.; et al. Carboplatin and Weekly Paclitaxel Doublet Chemotherapy Compared with Monotherapy in Elderly Patients with Advanced Non-Small-Cell Lung Cancer: IFCT-0501 Randomised, Phase 3 Trial. Lancet 2011, 378, 1079–1088. [Google Scholar] [CrossRef]
- Okamoto, I.; Schuette, W.H.W.; Stinchcombe, T.E.; Rodrigues-Pereira, J.; Antonio, B.S.; Chen, J.; Liu, J.; John, W.J.; Zinner, R.G. Meta-Analysis of Pemetrexed plus Carboplatin Doublet Safety Profile in First-Line Non-Squamous Non-Small Cell Lung Cancer Studies. Curr. Med. Res. Opin. 2017, 33, 937–941. [Google Scholar] [CrossRef]
- Karampeazis, A.; Vamvakas, L.; Kotsakis, A.; Christophyllakis, C.; Kentepozidis, N.; Chandrinos, V.; Agelidou, A.; Polyzos, A.; Tsiafaki, X.; Hatzidaki, D.; et al. Docetaxel plus Gemcitabine versus Gemcitabine in Elderly Patients with Advanced Non-Small Cell Lung Cancer and Use of a Geriatric Assessment: Lessons from a Prematurely Closed Hellenic Oncology Research Group Randomized Phase III Study. J. Geriatr. Oncol. 2016, 8, 23–30. [Google Scholar] [CrossRef]
- Brodowicz, T.; Krzakowski, M.; Zwitter, M.; Tzekova, V.; Ramlau, R.; Ghilezan, N.; Ciuleanu, T.; Cucevic, B.; Gyurkovits, K.; Ulsperger, E.; et al. Cisplatin and Gemcitabine First-Line Chemotherapy Followed by Maintenance Gemcitabine or Best Supportive Care in Advanced Non-Small Cell Lung Cancer: A Phase III Trial. Lung Cancer 2006, 52, 155–163. [Google Scholar] [CrossRef]
- Ciuleanu, T.; Brodowicz, T.; Zielinski, C.; Kim, J.H.; Krzakowski, M.; Laack, E.; Wu, Y.-L.; Bover, I.; Begbie, S.; Tzekova, V.; et al. Maintenance Pemetrexed plus Best Supportive Care versus Placebo plus Best Supportive Care for Non-Small-Cell Lung Cancer: A Randomised, Double-Blind, Phase 3 Study. Lancet 2009, 374, 1432–1440. [Google Scholar] [CrossRef]
- Shaw, A.T.; Kim, D.-W.; Nakagawa, K.; Seto, T.; Crinó, L.; Ahn, M.-J.; De Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus Chemotherapy in Advanced ALK-Positive Lung Cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.-W.; Mehra, R.; Tan, D.S.W.; Felip, E.; Chow, L.Q.M.; Camidge, D.R.; Vansteenkiste, J.; Sharma, S.; De Pas, T.; Riely, G.J.; et al. Activity and Safety of Ceritinib in Patients with ALK-Rearranged Non-Small-Cell Lung Cancer (ASCEND-1): Updated Results from the Multicentre, Open-Label, Phase 1 Trial. Lancet Oncol. 2016, 17, 452–463. [Google Scholar] [CrossRef] [Green Version]
- de Jong, W.K.; Groen, H.J.M.; Koolen, M.G.J.; Biesma, B.; Willems, L.N.A.; Kwa, H.-B.; van Bochove, A.; van Tinteren, H.; Smit, E.F. Phase III Study of Cyclophosphamide, Doxorubicin, and Etoposide Compared with Carboplatin and Paclitaxel in Patients with Extensive Disease Small-Cell Lung Cancer. Eur. J. Cancer 2007, 43, 2345–2350. [Google Scholar] [CrossRef] [PubMed]
- von Pawel, J.; Schiller, J.H.; Shepherd, F.A.; Fields, S.Z.; Kleisbauer, J.P.; Chrysson, N.G.; Stewart, D.J.; Clark, P.I.; Palmer, M.C.; Depierre, A.; et al. Topotecan versus Cyclophosphamide, Doxorubicin, and Vincristine for the Treatment of Recurrent Small-Cell Lung Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1999, 17, 658–667. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.E.R.; Ciuleanu, T.-E.; Tsekov, H.; Shparyk, Y.; Čučeviá, B.; Juhasz, G.; Thatcher, N.; Ross, G.A.; Dane, G.C.; Crofts, T. Phase III Trial Comparing Supportive Care Alone with Supportive Care with Oral Topotecan in Patients with Relapsed Small-Cell Lung Cancer. J. Clin. Oncol. 2006, 24, 5441–5447. [Google Scholar] [CrossRef] [PubMed]
- Dy, G.K.; Jett, J.R.; Geoffroy, F.J.; Krewer, K.D.; Tazelaar, H.; Maurer, M.; Rowland, K.; Mailliard, J.; Krook, J.; Dakhil, S.; et al. Topotecan and Paclitaxel in Previously Treated Patients with Relapsed Small Cell Lung Cancer: Phase II Trial of the North Central Cancer Treatment Group. J. Thorac. Oncol. 2006, 1, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Sekine, I.; Nishiwaki, Y.; Noda, K.; Kudoh, S.; Fukuoka, M.; Mori, K.; Negoro, S.; Yokoyama, A.; Matsui, K.; Ohsaki, Y.; et al. Randomized Phase II Study of Cisplatin, Irinotecan and Etoposide Combinations Administered Weekly or Every 4 Weeks for Extensive Small-Cell Lung Cancer (JCOG9902-DI). Ann. Oncol. 2003, 14, 709–714. [Google Scholar] [CrossRef]
- Lorigan, P.; Woll, P.J.; O’Brien, M.E.R.; Ashcroft, L.F.; Sampson, M.R.; Thatcher, N. Randomized Phase III Trial of Dose-Dense Chemotherapy Supported by Whole-Blood Hematopoietic Progenitors in Better-Prognosis Small-Cell Lung Cancer. J. Natl. Cancer Inst. 2005, 97, 666–674. [Google Scholar] [CrossRef]
- Lee, H.-S.; Lee, Y.-G.; Koo, D.-H.; Oh, S.; Nam, H.; Song, J.-U.; Lim, S.Y.; Lim, S.; Lee, S.-S. Efficacy and Safety of Ifosfamide in Combination with Carboplatin and Etoposide in Small Cell Lung Cancer. Cancer Chemother. Pharmacol. 2015, 76, 933–937. [Google Scholar] [CrossRef]
- Woll, P.J.; Hodgetts, J.; Lomax, L.; Bildet, F.; Cour-Chabernaud, V.; Thatcher, N. Can Cytotoxic Dose-Intensity Be Increased by Using Granulocyte Colony-Stimulating Factor? A Randomized Controlled Trial of Lenograstim in Small-Cell Lung Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1995, 13, 652–659. [Google Scholar] [CrossRef]
- Thatcher, N.; Qian, W.; Clark, P.I.; Hopwood, P.; Sambrook, R.J.; Owens, R.; Stephens, R.J.; Girling, D.J. Ifosfamide, Carboplatin, and Etoposide with Midcycle Vincristine Versus Standard Chemotherapy in Patients with Small-Cell Lung Cancer and Good Performance Status: Clinical and Quality-of-Life Results of the British Medical Research Council Multicenter Randomized LU21 Trial. J. Clin. Oncol. 2005, 23, 8371–8379. [Google Scholar] [CrossRef]
- Ardizzoni, A.; Tjan-Heijnen, V.C.G.; Postmus, P.E.; Buchholz, E.; Biesma, B.; Karnicka-Mlodkowska, H.; Dziadziuszko, R.; Burghouts, J.; Van Meerbeeck, J.P.; Gans, S.; et al. Standard versus Intensified Chemotherapy with Granulocyte Colony-Stimulating Factor Support in Small-Cell Lung Cancer: A Prospective European Organization for Research and Treatment of Cancer-Lung Cancer Group Phase III Trial-08923. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2002, 20, 3947–3955. [Google Scholar] [CrossRef] [PubMed]
- Masutani, M.; Ochi, Y.; Kadota, A.; Akusawa, H.; Kisohara, A.; Takahashi, N.; Koya, Y.; Horie, T. Dose-Intensive Weekly Alternating Chemotherapy for Patients with Small Cell Lung Cancer: Randomized Trial, Can It Improve Survival of Patients with Good Prognostic Factors? Oncol. Rep. 2000, 7, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, P.J.; McCoy, J.; Dunphy II, F.R.; Bearden III, J.D.; Weiss, G.R.; Giguere, J.K.; Atkins, J.N.; Dakhil, S.R.; Kelly, K.; Crowley, J.J.; et al. Phase II Trial of Paclitaxel, Carboplatin, and Topotecan with G-CSF Support in Previously Untreated Patients with Extensive Stage Small Cell Lung Cancer: Southwest Oncology Group 9914. J. Thorac. Oncol. 2006, 1, 991–995. [Google Scholar] [CrossRef] [PubMed]
- Sundstrøm, S.; Bremnes, R.M.; Kaasa, S.; Aasebø, U.; Hatlevoll, R.; Dahle, R.; Boye, N.; Wang, M.; Vigander, T.; Vilsvik, J.; et al. Cisplatin and Etoposide Regimen Is Superior to Cyclophosphamide, Epirubicin, and Vincristine Regimen in Small-Cell Lung Cancer: Results From a Randomized Phase III Trial with 5 Years’ Follow-Up. J. Clin. Oncol. 2002, 20, 4665–4672. [Google Scholar] [CrossRef]
- Noda, K.; Nishiwaki, Y.; Kawahara, M.; Negoro, S.; Sugiura, T.; Yokoyama, A.; Fukuoka, M.; Mori, K.; Watanabe, K.; Tamura, T.; et al. Irinotecan plus Cisplatin Compared with Etoposide plus Cisplatin for Extensive Small-Cell Lung Cancer. N. Engl. J. Med. 2002, 346, 85–91. [Google Scholar] [CrossRef]
- Fink, T.H.; Huber, R.M.; Heigener, D.F.; Eschbach, C.; Waller, C.; Steinhauer, E.U.; Virchow, J.C.; Eberhardt, F.; Schweisfurth, H.; Schroeder, M.; et al. Topotecan/Cisplatin Compared with Cisplatin/Etoposide as First-Line Treatment for Patients with Extensive Disease Small-Cell Lung Cancer: Final Results of a Randomized Phase III Trial. J. Thorac. Oncol. 2012, 7, 1432–1439. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Luft, A.; Szczesna, A.; Havel, L.; Kim, S.-W.; Akerley, W.; Pietanza, M.C.; Wu, Y.; Zielinski, C.; Thomas, M.; et al. Phase III Randomized Trial of Ipilimumab Plus Etoposide and Platinum Versus Placebo Plus Etoposide and Platinum in Extensive-Stage Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 3740–3748. [Google Scholar] [CrossRef]
- Hermes, A.; Bergman, B.; Bremnes, R.; Ek, L.; Fluge, S.; Sederholm, C.; Sundstrøm, S.; Thaning, L.; Vilsvik, J.; Aasebø, U.; et al. Irinotecan Plus Carboplatin Versus Oral Etoposide Plus Carboplatin in Extensive Small-Cell Lung Cancer: A Randomized Phase III Trial. J. Clin. Oncol. 2008, 26, 4261–4267. [Google Scholar] [CrossRef]
- Okamoto, H.; Naoki, K.; Narita, Y.; Hida, N.; Kunikane, H.; Watanabe, K. A Combination Chemotherapy of Carboplatin and Irinotecan with Granulocyte Colony-Stimulating Factor (G-CSF) Support in Elderly Patients with Small Cell Lung Cancer. Lung Cancer 2006, 53, 197–203. [Google Scholar] [CrossRef]
- Ardizzoni, A.; Manegold, C.; Debruyne, C.; Gaafar, R.; Buchholz, E.; Smit, E.F.; Lianes, P.; ten Velde, G.; Bosquee, L.; Legrand, C.; et al. European Organization for Research and Treatment of Cancer (EORTC) 08957 Phase II Study of Topotecan in Combination with Cisplatin as Second-Line Treatment of Refractory and Sensitive Small Cell Lung Cancer. Am. Assoc. Cancer Res. 2003, 9, 143–150. [Google Scholar]
- Skarlos, D.-V.; Dimopoulos, A.-M.; Kosmidis, P.; Papakostas, P.; Pavlidis, N.; Bacoyiannis, C.; Kiamouris, C.; Klouvas, G.; Gogas, H.; Fountzilas, G.; et al. Docetaxel and Gemcitabine Combination, as First-Line Treatment, in Patients with Extensive Disease Small-Cell Lung Cancer. A Phase II Study of the Hellenic Cooperative Oncology Group. Lung Cancer 2003, 41, 107–111. [Google Scholar] [CrossRef]
- Hainsworth, J.D.; Carrell, D.; Drengler, R.L.; Scroggin, C.; Greco, F.A. Weekly Combination Chemotherapy with Docetaxel and Gemcitabine as First-Line Treatment for Elderly Patients and Patients with Poor Performance Status Who Have Extensive-Stage Small Cell Lung Carcinoma. Cancer 2004, 100, 2437–2441. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Lima, C.M.; Herndon, J.E.; Lee, M.E.; Atkins, J.N.; Mauer, A.; Vokes, E.; Green, M.R. Phase II Trial of Irinotecan/Gemcitabine as Second-Line Therapy for Relapsed and Refractory Small-Cell Lung Cancer: Cancer and Leukemia Group B Study 39902. Ann. Oncol. 2007, 18, 331–337. [Google Scholar] [CrossRef]
- Furuse, K.; Fukuoka, M.; Nishiwaki, Y.; Kurita, Y.; Watanabe, K.; Noda, K.; Ariyoshi, Y.; Tamura, T.; Saijo, N. Phase III Study of Intensive Weekly Chemotherapy with Recombinant Human Granulocyte Colony-Stimulating Factor versus Standard Chemotherapy in Extensive-Disease Small-Cell Lung Cancer. The Japan Clinical Oncology Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1998, 16, 2126–2132. [Google Scholar] [CrossRef]
- Murray, N.; Livingston, R.B.; Shepherd, F.A.; James, K.; Zee, B.; Langleben, A.; Kraut, M.; Bearden, J.; Goodwin, J.W.; Grafton, C.; et al. Randomized Study of CODE Versus Alternating CAV/EP for Extensive-Stage Small-Cell Lung Cancer: An Intergroup Study of the National Cancer Institute of Canada Clinical Trials Group and the Southwest Oncology Group. J. Clin. Oncol. 1999, 17, 2300. [Google Scholar] [CrossRef]
- Edelman, M.J.; Chansky, K.; Gaspar, L.E.; Leigh, B.; Weiss, G.R.; Taylor, S.A.; Crowley, J.; Livingston, R.; Gandara, D.R. Phase II Trial of Cisplatin/Etoposide and Concurrent Radiotherapy Followed by Paclitaxel/Carboplatin Consolidation for Limited Small-Cell Lung Cancer: Southwest Oncology Group 9713. J. Clin. Oncol. 2004, 22, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Grilley-Olson, J.E.; Keedy, V.L.; Sandler, A.; Moore, D.T.; Socinski, M.A.; Stinchcombe, T.E. A Randomized Phase II Study of Carboplatin with Weekly or Every-3-Week Nanoparticle Albumin-Bound Paclitaxel (Abraxane) in Patients with Extensive-Stage Small Cell Lung Cancer. Oncologist 2015, 20, 105–106. [Google Scholar] [CrossRef]
- Noronha, V.; Sahu, A.; Patil, V.M.; Joshi, A.; Ramaswamy, A.; Chandrasekharan, A.; Kadam, N.; Prabhash, K. Weekly Paclitaxel as Metronomic Palliative Chemotherapy in Small Cell Lung Cancer. South Asian J. Cancer 2016, 5, 67. [Google Scholar] [CrossRef] [PubMed]
- van der Lee, I.; Smit, E.F.; van Putten, J.W.; Groen, H.J.; Schlösser, N.J.; Postmus, P.E.; Schramel, F.M. Single-Agent Gemcitabine in Patients with Resistant Small-Cell Lung Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. ESMO 2001, 12, 557–561. [Google Scholar] [CrossRef]
- Hoang, T.; Kim, K.; Jaslowski, A.; Koch, P.; Beatty, P.; McGovern, J.; Quisumbing, M.; Shapiro, G.; Witte, R.; Schiller, J.H. Phase II Study of Second-Line Gemcitabine in Sensitive or Refractory Small Cell Lung Cancer. Lung Cancer 2003, 42, 97–102. [Google Scholar] [CrossRef]
- Flinn, I.W.; van der Jagt, R.; Kahl, B.S.; Wood, P.; Hawkins, T.E.; MacDonald, D.; Hertzberg, M.; Kwan, Y.-L.; Simpson, D.; Craig, M.; et al. Randomized Trial of Bendamustine-Rituximab or R-CHOP/R-CVP in First-Line Treatment of Indolent NHL or MCL: The BRIGHT Study. Blood 2014, 123, 2944–2952. [Google Scholar] [CrossRef] [PubMed]
- Tilly, H.; Morschhauser, F.; Sehn, L.H.; Friedberg, J.W.; Trněný, M.; Sharman, J.P.; Herbaux, C.; Burke, J.M.; Matasar, M.; Rai, S.; et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 386, 351–363. [Google Scholar] [CrossRef] [PubMed]
- Crump, M.; Kuruvilla, J.; Couban, S.; MacDonald, D.A.; Kukreti, V.; Kouroukis, C.T.; Rubinger, M.; Buckstein, R.; Imrie, K.R.; Federico, M.; et al. Randomized Comparison of Gemcitabine, Dexamethasone, and Cisplatin versus Dexamethasone, Cytarabine, and Cisplatin Chemotherapy before Autologous Stem-Cell Transplantation for Relapsed and Refractory Aggressive Lymphomas: NCIC-CTG LY.12. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3490–3496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mounier, N.; Briere, J.; Gisselbrecht, C.; Emile, J.-F.; Lederlin, P.; Sebban, C.; Berger, F.; Bosly, A.; Morel, P.; Tilly, H.; et al. Rituximab plus CHOP (R-CHOP) Overcomes Bcl-2--Associated Resistance to Chemotherapy in Elderly Patients with Diffuse Large B-Cell Lymphoma (DLBCL). Blood 2003, 101, 4279–4284. [Google Scholar] [CrossRef] [Green Version]
- Jais, J.-P.; Haioun, C.; Molina, T.J.; Rickman, D.S.; de Reynies, A.; Berger, F.; Gisselbrecht, C.; Brière, J.; Reyes, F.; Gaulard, P.; et al. The Expression of 16 Genes Related to the Cell of Origin and Immune Response Predicts Survival in Elderly Patients with Diffuse Large B-Cell Lymphoma Treated with CHOP and Rituximab. Leukemia 2008, 22, 1917–1924. [Google Scholar] [CrossRef] [Green Version]
- Mounier, N.; Heutte, N.; Thieblemont, C.; Briere, J.; Gaulard, P.; Feugier, P.; Ghesquieres, H.; Van Den Neste, E.; Robu, D.; Tilly, H.; et al. Ten-Year Relative Survival and Causes of Death in Elderly Patients Treated with R-CHOP or CHOP in the GELA LNH-985 Trial. Clin. Lymphoma Myeloma Leuk. 2012, 12, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Peyrade, F.; Jardin, F.; Thieblemont, C.; Thyss, A.; Emile, J.-F.; Castaigne, S.; Coiffier, B.; Haioun, C.; Bologna, S.; Fitoussi, O.; et al. Attenuated Immunochemotherapy Regimen (R-MiniCHOP) in Elderly Patients Older than 80 Years with Diffuse Large B-Cell Lymphoma: A Multicentre, Single-Arm, Phase 2 Trial. Lancet Oncol. 2011, 12, 460–468. [Google Scholar] [CrossRef]
- Sancho, J.-M.; Fernández-Alvarez, R.; Gual-Capllonch, F.; González-García, E.; Grande, C.; Gutiérrez, N.; Peñarrubia, M.-J.; Batlle-López, A.; González-Barca, E.; Guinea, J.-M.; et al. R-COMP versus R-CHOP as First-Line Therapy for Diffuse Large B-Cell Lymphoma in Patients ≥60 Years: Results of a Randomized Phase 2 Study from the Spanish GELTAMO Group. Cancer Med. 2021, 10, 1314–1326. [Google Scholar] [CrossRef]
- Laribi, K.; Denizon, N.; Bolle, D.; Truong, C.; Besançon, A.; Sandrini, J.; Anghel, A.; Farhi, J.; Ghnaya, H.; Baugier de Materre, A. R-CVP Regimen Is Active in Frail Elderly Patients Aged 80 or over with Diffuse Large B Cell Lymphoma. Ann. Hematol. 2016, 95, 1705–1714. [Google Scholar] [CrossRef]
- Ösby, E.; Hagberg, H.; Kvaløy, S.; Teerenhovi, L.; Anderson, H.; Cavallin-Ståhl, E.; Holte, H.; Myhre, J.; Pertovaara, H.; Björkholm, M. CHOP Is Superior to CNOP in Elderly Patients with Aggressive Lymphoma While Outcome Is Unaffected by Filgrastim Treatment: Results of a Nordic Lymphoma Group Randomized Trial. Blood 2003, 101, 3840–3848. [Google Scholar] [CrossRef] [Green Version]
- Velasquez, W.S.; Cabanillas, F.; Salvador, P.; McLaughlin, P.; Fridrik, M.; Tucker, S.; Jagannath, S.; Hagemeister, F.B.; Redman, J.R.; Swan, F. Effective Salvage Therapy for Lymphoma with Cisplatin in Combination with High-Dose Ara-C and Dexamethasone (DHAP). Blood 1988, 71, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Johnson, P.W.M.; Sweetenham, J.W.; McCallum, P.; Norton, A.J.; Rohatiner, A.Z.S.; Lister, T.A. E-SHAP: Inadequate Treatment for Poor-Prognosis Recurrent Lymphoma. Ann. Oncol. 1993, 4, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Velasquez, W.S.; McLaughlin, P.; Tucker, S.; Hagemeister, F.B.; Swan, F.; Rodriguez, M.A.; Romaguera, J.; Rubenstein, E.; Cabanillas, F. ESHAP--an Effective Chemotherapy Regimen in Refractory and Relapsing Lymphoma: A 4-Year Follow-up Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1994, 12, 1169–1176. [Google Scholar] [CrossRef]
- Öztürk, M.A.; Barışta, İ.; Altundağ, M.K.; Türker, A.; Yalçın, Ş.; Çelik, İ.; Güllü, İ.; Güler, N.; Özışık, Y.; Kars, A.; et al. Modified ESHAP as Salvage Chemotherapy for Recurrent or Refractory Non-Hodgkin’s Lymphoma: Results of a Single-Center Study of 32 Patients. Chemotherapy 2002, 48, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Santoro, P.; Martinelli, G.; Ferrucci, P.F.; Mingrone, W.; Cocorocchio, E.; Conconi, A.; Peccatori, F.A.; Luzio, K.D.; Mazzetta, C.; Zucca, E.; et al. ACOD, a Modified CHOP Regimen for Elderly Patients with Aggressive Non-Hodgkin’s Lymphoma. Leuk. Lymphoma 2003, 44, 801–806. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Fountzilas, G.; Papageorgiou, E.; Kiamouris, C.; Mantzios, G.; Anagnostopoulos, A.; Nicolaides, C.; Economopoulos, T. Primary Treatment of Low-Grade Non-Hodgkin’s Lymphoma with the Combination of Fludarabine and Mitoxantrone: A Phase II Study of the Hellenic Cooperative Oncology Group. Leuk. Lymphoma 2002, 43, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Coiffier, B.; Lepage, E.; Briere, J.; Herbrecht, R.; Tilly, H.; Bouabdallah, R.; Morel, P.; Van Den Neste, E.; Salles, G.; Gaulard, P.; et al. CHOP Chemotherapy plus Rituximab Compared with CHOP Alone in Elderly Patients with Diffuse Large-B-Cell Lymphoma. N. Engl. J. Med. 2002, 346, 235–242. [Google Scholar] [CrossRef]
- Miura, K.; Konishi, J.; Miyake, T.; Makita, M.; Hojo, A.; Masaki, Y.; Uno, M.; Ozaki, J.; Yoshida, C.; Niiya, D.; et al. A Host-Dependent Prognostic Model for Elderly Patients with Diffuse Large B-Cell Lymphoma. Oncologist 2017, 22, 554–560. [Google Scholar] [CrossRef] [Green Version]
- Thieblemont, C.; Tilly, H.; Gomes da Silva, M.; Casasnovas, R.-O.; Fruchart, C.; Morschhauser, F.; Haioun, C.; Lazarovici, J.; Grosicka, A.; Perrot, A.; et al. Lenalidomide Maintenance Compared with Placebo in Responding Elderly Patients with Diffuse Large B-Cell Lymphoma Treated with First-Line Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2473–2481. [Google Scholar] [CrossRef]
- Visani, G.; Ferrara, F.; Alesiani, F.; Ronconi, S.; Catarini, M.; D’adamo, F.; Guiducci, B.; Bernardi, D.; Barulli, S.; Piccaluga, P.; et al. R-COMP 21 for Frail Elderly Patients with Aggressive B-Cell Non-Hodgkin Lymphoma: A Pilot Study. Leuk. Lymphoma 2008, 49, 1081–1086. [Google Scholar] [CrossRef]
- Miyata, Y.; Saito, A.M.; Yano, T.; Yoshida, I.; Suehiro, Y.; Harada, N.; Nagai, H. R-Mini CHP in ≥80-Year-Old Patients with Diffuse Large B-Cell Lymphoma: A Multicenter, Open-Label, Single-Arm Phase II Trial Protocol. Acta Med. Okayama 2018, 72, 315–318. [Google Scholar] [CrossRef]
- Merli, F.; Vitolo, U.; Luminari, S.; Mazza, P.; Stelitano, C.; Rossi, G.; Baldini, L.; Ilariucci, F.; Levis, A. R-CHOP vs R-Mini-CEOP in Elderly Patients with Diffuse Large B Cell Lymphoma: An Interim Report from Intergruppo Italiano Linfomi (IIL). Blood 2005, 106, 4729. [Google Scholar] [CrossRef]
- Bartlett, N.L.; Wilson, W.H.; Jung, S.-H.; Hsi, E.D.; Maurer, M.J.; Pederson, L.D.; Polley, M.-Y.C.; Pitcher, B.N.; Cheson, B.D.; Kahl, B.S.; et al. Dose-Adjusted EPOCH-R Compared with R-CHOP as Frontline Therapy for Diffuse Large B-Cell Lymphoma: Clinical Outcomes of the Phase III Intergroup Trial Alliance/CALGB 50303. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 1790–1799. [Google Scholar] [CrossRef] [PubMed]
- Mounier, N.; El Gnaoui, T.; Tilly, H.; Canioni, D.; Sebban, C.; Casasnovas, R.-O.; Delarue, R.; Sonet, A.; Beaussart, P.; Petrella, T.; et al. Rituximab plus Gemcitabine and Oxaliplatin in Patients with Refractory/Relapsed Diffuse Large B-Cell Lymphoma Who Are Not Candidates for High-Dose Therapy. A Phase II Lymphoma Study Association Trial. Haematologica 2013, 98, 1726–1731. [Google Scholar] [CrossRef]
- Tuscano, J.M.; Dutia, M.; Chee, K.; Brunson, A.; Reed-Pease, C.; Abedi, M.; Welborn, J.; O’Donnell, R.T. Lenalidomide plus Rituximab Can Produce Durable Clinical Responses in Patients with Relapsed or Refractory, Indolent Non-Hodgkin Lymphoma. Br. J. Haematol. 2014, 165, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonard, J.P.; Jung, S.-H.; Johnson, J.; Pitcher, B.N.; Bartlett, N.L.; Blum, K.A.; Czuczman, M.; Giguere, J.K.; Cheson, B.D. Randomized Trial of Lenalidomide Alone Versus Lenalidomide Plus Rituximab in Patients with Recurrent Follicular Lymphoma: CALGB 50401 (Alliance). J. Clin. Oncol. 2015, 33, 3635–3640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruan, J.; Shah, B.; Martin, P.; Schuster, S.J. Clinical Experience with Lenalidomide Alone or in Combination with Rituximab in Indolent B-Cell and Mantle Cell Lymphomas. Ann. Oncol. 2016, 27, 1226–1234. [Google Scholar] [CrossRef] [Green Version]
- Goy, A.; Sinha, R.; Williams, M.E.; Besisik, S.K.; Drach, J.; Ramchandren, R.; Zhang, L.; Cicero, S.; Fu, T.; Witzig, T.E. Single-Agent Lenalidomide in Patients with Mantle-Cell Lymphoma Who Relapsed or Progressed After or Were Refractory to Bortezomib: Phase II MCL-001 (EMERGE) Study. J. Clin. Oncol. 2013, 31, 3688–3695. [Google Scholar] [CrossRef]
- Salles, G.; Duell, J.; González Barca, E.; Tournilhac, O.; Jurczak, W.; Liberati, A.M.; Nagy, Z.; Obr, A.; Gaidano, G.; André, M.; et al. Tafasitamab plus Lenalidomide in Relapsed or Refractory Diffuse Large B-Cell Lymphoma (L-MIND): A Multicentre, Prospective, Single-Arm, Phase 2 Study. Lancet Oncol. 2020, 21, 978–988. [Google Scholar] [CrossRef]
- Abramson, J.S.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Wang, M.; Arnason, J.; Mehta, A.; Purev, E.; Maloney, D.G.; Andreadis, C.; et al. Lisocabtagene Maraleucel for Patients with Relapsed or Refractory Large B-Cell Lymphomas (TRANSCEND NHL 001): A Multicentre Seamless Design Study. Lancet Lond. Engl. 2020, 396, 839–852. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- Sermer, D.; Batlevi, C.; Palomba, M.L.; Shah, G.; Lin, R.J.; Perales, M.-A.; Scordo, M.; Dahi, P.; Pennisi, M.; Afuye, A.; et al. Outcomes in Patients with DLBCL Treated with Commercial CAR T Cells Compared with Alternate Therapies. Blood Adv. 2020, 4, 4669–4678. [Google Scholar] [CrossRef]
- Sesques, P.; Ferrant, E.; Safar, V.; Wallet, F.; Tordo, J.; Dhomps, A.; Karlin, L.; Brisou, G.; Vercasson, M.; Hospital-Gustem, C.; et al. Commercial Anti-CD19 CAR T Cell Therapy for Patients with Relapsed/Refractory Aggressive B Cell Lymphoma in a European Center. Am. J. Hematol. 2020, 95, 1324–1333. [Google Scholar] [CrossRef]
- Colombat, P.; Salles, G.; Brousse, N.; Eftekhari, P.; Soubeyran, P.; Delwail, V.; Deconinck, E.; Haïoun, C.; Foussard, C.; Sebban, C.; et al. Rituximab (Anti-CD20 Monoclonal Antibody) as Single First-Line Therapy for Patients with Follicular Lymphoma with a Low Tumor Burden: Clinical and Molecular Evaluation. Blood 2001, 97, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Federico, M.; Luminari, S.; Dondi, A.; Tucci, A.; Vitolo, U.; Rigacci, L.; Di Raimondo, F.; Carella, A.M.; Pulsoni, A.; Merli, F.; et al. R-CVP versus R-CHOP versus R-FM for the Initial Treatment of Patients with Advanced-Stage Follicular Lymphoma: Results of the FOLL05 Trial Conducted by the Fondazione Italiana Linfomi. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 1506–1513. [Google Scholar] [CrossRef]
- Marcus, R.; Davies, A.; Ando, K.; Klapper, W.; Opat, S.; Owen, C.; Phillips, E.; Sangha, R.; Schlag, R.; Seymour, J.F.; et al. Obinutuzumab for the First-Line Treatment of Follicular Lymphoma. N. Engl. J. Med. 2017, 377, 1331–1344. [Google Scholar] [CrossRef] [PubMed]
- Hiddemann, W.; Barbui, A.M.; Canales, M.A.; Cannell, P.K.; Collins, G.P.; Dürig, J.; Forstpointner, R.; Herold, M.; Hertzberg, M.; Klanova, M.; et al. Immunochemotherapy with Obinutuzumab or Rituximab for Previously Untreated Follicular Lymphoma in the GALLIUM Study: Influence of Chemotherapy on Efficacy and Safety. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2395–2404. [Google Scholar] [CrossRef]
- Martin, P.; Jung, S.-H.; Pitcher, B.; Bartlett, N.L.; Blum, K.A.; Shea, T.; Hsi, E.D.; Ruan, J.; Smith, S.E.; Leonard, J.P.; et al. A Phase II Trial of Lenalidomide plus Rituximab in Previously Untreated Follicular Non-Hodgkin’s Lymphoma (NHL): CALGB 50803 (Alliance). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 2806–2812. [Google Scholar] [CrossRef]




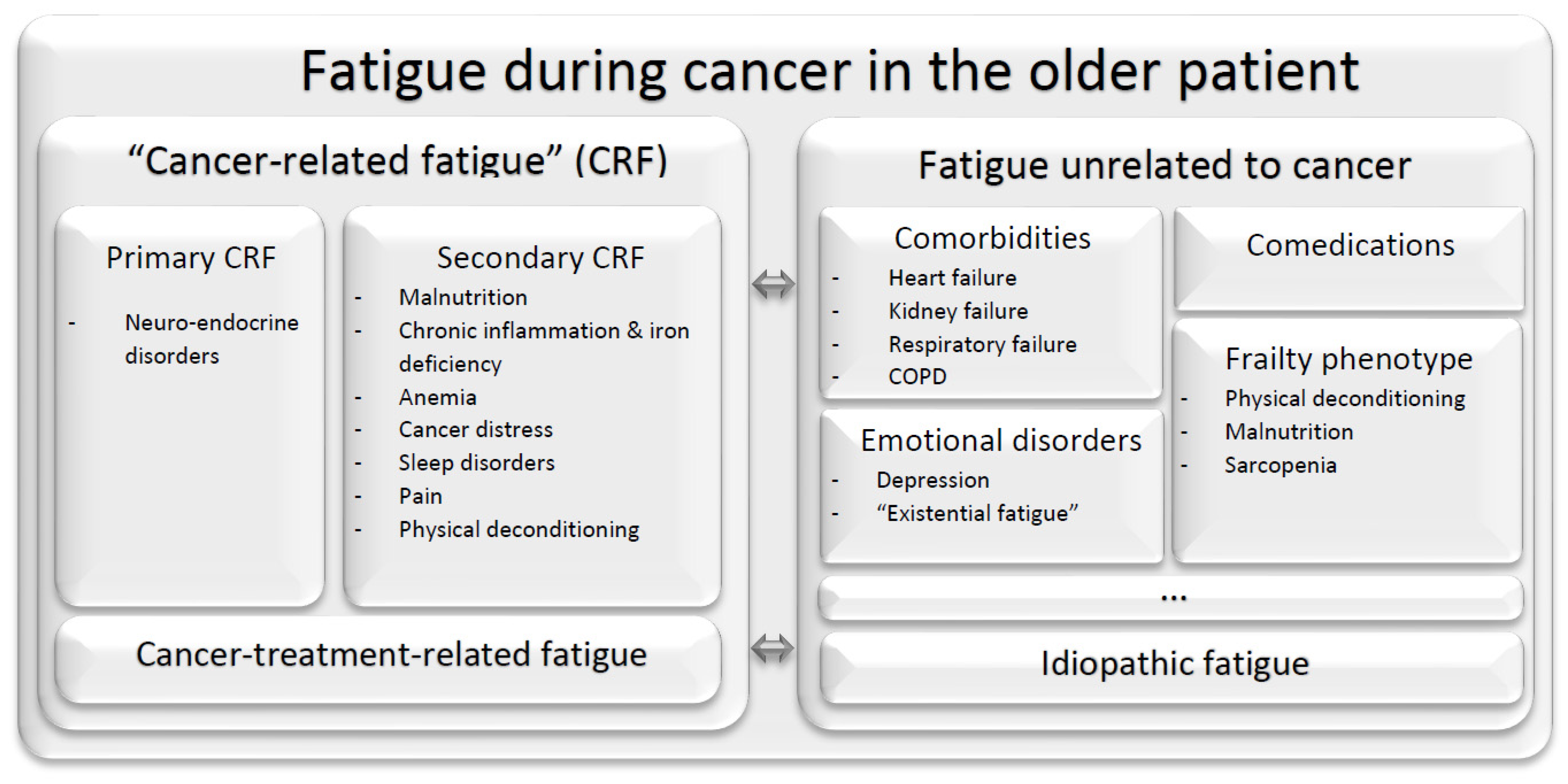{kind=link}
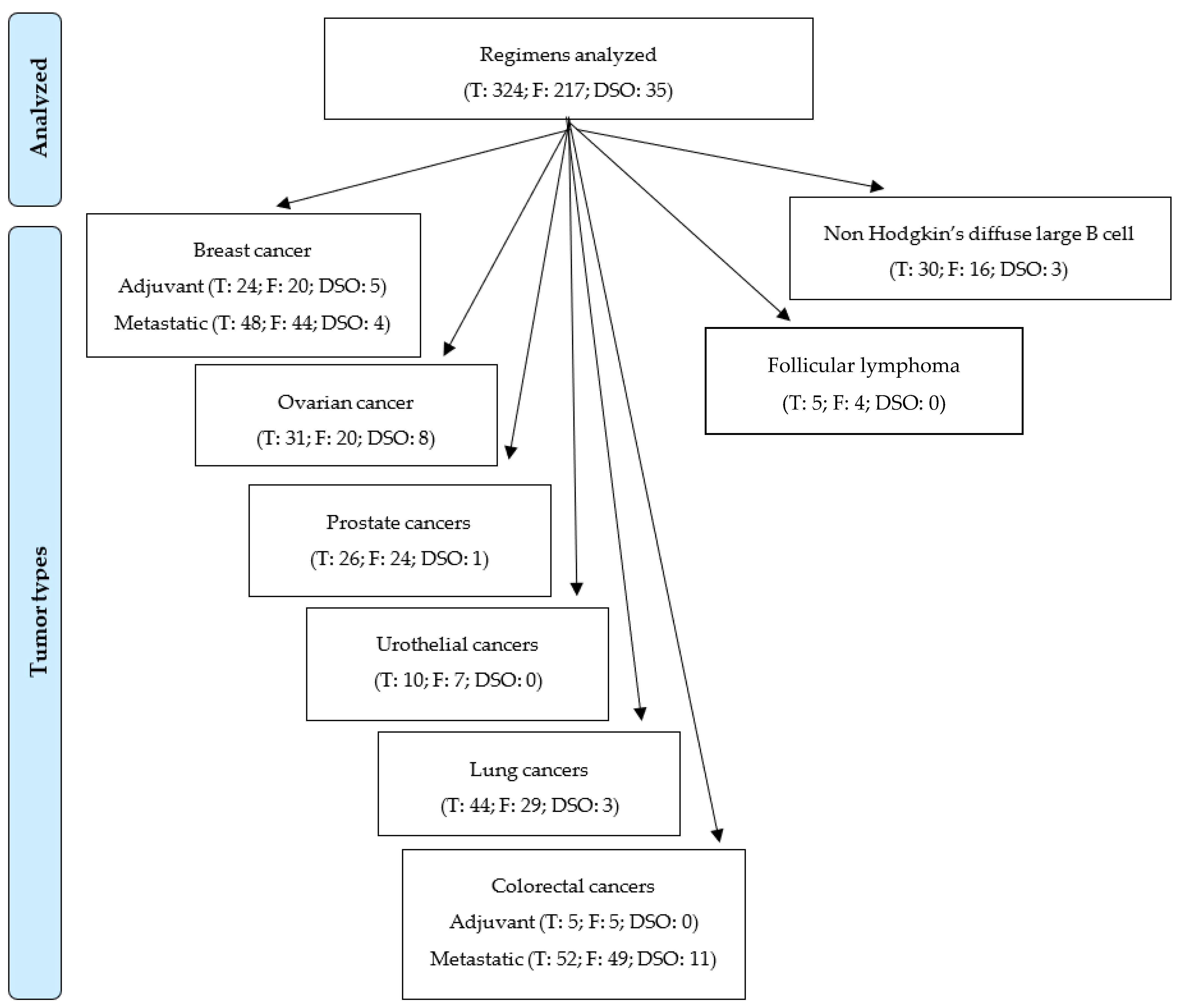{kind=link}
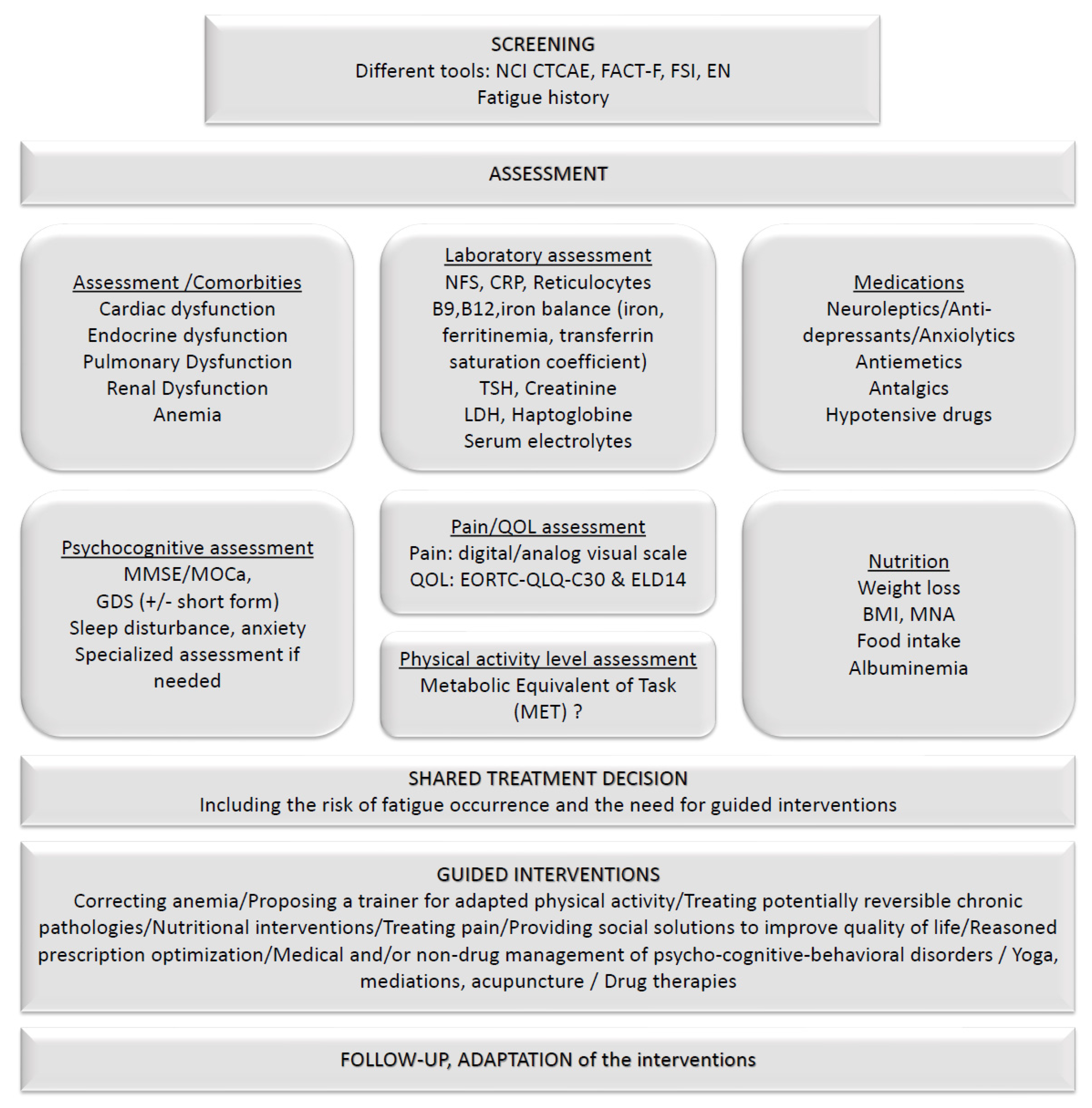{kind=link}
| Setting | Treatment Regimen and Reference | Fatigue Any-Grade (%) | Fatigue Gr ≥ 3 (%) | |
|---|---|---|---|---|
| Adjuvant | AC [27,36] | 49–77 | 2–4 | |
| AC → docetaxel [37,38] | nr | 22 | ||
| AC → paclitaxel [37] | nr | nr | ||
| A(E)C-[T/P] [29] | nr | 10 | ||
| <60 | nr | 9 | ||
| 60–64 | nr | 12 | ||
| >64 | nr | 16 | ||
| Paclitaxel → AC [39] | nr | nr | ||
| AT [36,40] | 51 | 9–16 | ||
| ddAT [29,38] | nr | 28 | ||
| <60 | nr | 25 | ||
| 60–64 | nr | 40 | ||
| >64 | nr | 35 | ||
| Doxorubicin → docetaxel [41] | nr | 7 | ||
| Doxorubicin/paclitaxel [42] | nr | nr | ||
| TAC [29,43] | 81 | 11 (asthenia)–12 | ||
| <60 | nr | 12 | ||
| 60–64 | nr | 13 | ||
| >64 | nr | 17 | ||
| DDG epirubicin/cyclophosphamide [44] | nr | 7 | ||
| Liposomal doxorubicin–cyclophosphamide ≥70 [45] | 88 | 8 | ||
| Docetaxel/cyclophosphamide [27] | 78 | 3 | ||
| CEF [44] | nr | 6 | ||
| FAC [43,46] | 71 (asthenia) | 3–6 | ||
| FAC ≥ w-paclitaxel ×8 [46] | nr | 8 | ||
| FAC 50 [47,48] | nr | nr | ||
| FEC 90/100 [49,50] | nr | nr | ||
| CMF [51,52] | nr | nr | ||
| CMF oral [53] | nr | nr | ||
| Doxorubicin → paclitaxel → cyclophosphamide [37] | nr | nr | ||
| Doxorubicin docetaxel [47,48] | nr | nr | ||
| FAC → paclitaxel [46] | nr | 8 | ||
| Capecitabine [26] | 26 | 1 | ||
| Trastuzumab/Docetaxel/Cyclophosphamide [54] | 54 | 4 | ||
| Trastuzumab/Paclitaxel [28] | nr (gr2: 20) | 2 | ||
| Trastuzumab paclitaxel for 12 weeks + trastuzumab for 9 months [28] | 22 | 2 | ||
| Docetaxel + carboplatin + trastuzumab for 52 weeks (TCH) [41] | nr | 7 | ||
| AC → TH [41] | nr | 7 | ||
| Tamoxifen (ABC) [30,31] | 3 (lethargy)–18 | 1 | ||
| Anastrozole (ABC) [31,32] | 1 (lethargy)–16 (asthenia) | 0 | ||
| Letrozole [33,55] | 30 | 1 | ||
| ≥70 [34] | 45 | nr | ||
| Exemestane [35] | 24 | 1 | ||
| Any adjuvant chemotherapy (CANTO) [25] Risk factors for post-treatment fatigue: | Severe fatigue (score ≥40%, EORTC QLQ-C30 fatigue item) | |||
| ~pre-treatment fatigue ~higher BMI ~younger age ~hormonal treatment | ~current smoking behavior ~worse anxiety ~insomnia ~pain at diagnosis | T1 (1 y): 36 T2 (2 y): 34 T3 (4 y): 32 | ||
| Metastatic | A → T [40] | nr | 7 | |
| AT [40] | nr | 16 | ||
| Paclitaxel 175 mg/m2/3w [56,57] | nr | 1–5 | ||
| Paclitaxel 90 mg/m2/3w/4 [56] | nr | 5 | ||
| Paclitaxel 80 mg/m2/w [56] | nr | 6 | ||
| Nab-paclitaxel 260 mg/m2/3w [57] | nr | 5 | ||
| Bevacizumab paclitaxel [58,59] | nr | 1–9 | ||
| Docetaxel 100 mg/m2/3w [60,61,62] | nr | 15–24 | ||
| Docetaxel 75 mg/m2/3w [61] | nr | 8 | ||
| Docetaxel 60 mg/m2/3w [61] | nr | 3 | ||
| Docetaxel capecitabine [60] | nr | 8 | ||
| Metronomic docetaxel capecitabine [63] | 60 | 13 | ||
| Gemcitabine vinorelbine [64] | nr | 24 | ||
| Vinorelbine [31,64] | 36 | 17 | ||
| Liposomal Pegylated Doxorubicin [65] | nr | nr | ||
| ≥70 [66] | 69 | 22 | ||
| Doxorubicin/vinorelbine [67] | nr | nr | ||
| Capecitabin [68,69,70,71] | 17–41 | 0–8 | ||
| Bevacizumab capecitabine [72] | nr | nr | ||
| Bevacizumab capecitabine vinorelbine [72] | nr | nr | ||
| Gemcitabine [73] | nr | nr | ||
| Eribulin [74,75] | 35–54 | 9 | ||
| Ixabepilone [31] | 10 | nr | ||
| Trastuzumab docetaxel (CLEOPATRAc) [76] | 38 | 2 | ||
| Trastuzumab paclitaxel [77] | 8 | nr | ||
| Trastuzumab + oral vinorelbine [78,79] | 42 | 4 | ||
| Trastuzumab vinorelbine everolimus (BOLERO-3) [79] | 43 | 12 | ||
| Trastuzumab emsantine (EMILIAi) [80] | 35 | 2 | ||
| Lapatinib capecitabine (EMILIAc and HER2CLIMBc) [80,81] | 28–43 | 4 | ||
| Pertuzumab–trastuzumab–docetaxel (CLEOPATRAi and PERUSE) [76,82] | 37 | 2–3 | ||
| Pertuzumab–trastuzumab–paclitaxel (PERUSE) [82] | nr | 2 | ||
| Pertuzumab–trastuzumab–nab-paclitaxel (PERUSE) [82] | nr | 2 | ||
| Tucatinib–trastuzumab–capecitabine [81] | 45 | 5 | ||
| Tamoxifen (ABC) [30,31] | 3 (lethargy)–18 | 1 | ||
| Anastrozole (ABC) [31,32] | 1.2 (lethargy)–16 (asthenia) | 0 | ||
| Letrozole (MONALEESA-2c) [30,31,83,84] | 11–27 | 0–1 | ||
| Exemestane [31,85] | 22–26 | 0 | ||
| Fulvestrant (CONFIRM, PALOMA-3c, MONARCH2c, and MONALEESA-3c) [86,87,88,89,90] | 31–44 | <1–3 | ||
| Lapatinib letrozole [91,92] | 21–33 (ctrl: 17) | 0–2 (ctrl: <1) | ||
| Exemestane–Everolimus [85,93,94] BALLET: sub-analysis by ages (<70 vs. ≥70, non-comparative) | 23 (asthenia)–50 29 vs. 21 | 2–4 6 vs. 3 | ||
| Palbociclib letrozole (PALOMA-1 and PALOMA-2) [83,95] | 37–40 (ctrl: 23–28) | 2–4 (ctrl: 1) | ||
| Palbociclib fulvestrant (PALOMA-3) [88] | 44 (ctrl: 31) | 3 (ctrl: 1) | ||
| Palbociclib-ET (pooled analysis PALOMA 1, 2, 3) | ||||
| <65 [96] | 40 (ctrl: 27) | 2 (ctrl: 1) | ||
| 65–74 [96] | 41 (ctrl: 28) | 3 (ctrl: 0) | ||
| ≥75 [96] | 37 (ctrl: 31) | 6 (ctrl: 0) | ||
| Ribociclib letrozole (MONALEESA-2, CompLEEment-1) [84,97] | 23–42 (ctrl: 27) | 1–2 (ctrl: 1) | ||
| Ribociclib fulvestrant (MONALEESA-3) [90] | 32 (ctrl: 33) | 2 (ctrl: <1) | ||
| Abemaciclib letrozole or anastrozole (MONARCH-3) [98] | 40 (ctrl: 32; gr2+: 17) | 2 (ctrl: 0) | ||
| Abemaciclib fulvestrant (MONARCH-2) [89] | 40 (ctrl: 27) | 3 (ctrl: <1) | ||
| Talazoparib (EMBRACA) [99] | 50 (ctrl: 43) | 2 (ctrl: 3) | ||
| Olaparib (OlympiaAD) [100] | 29 (ctrl: 23) | 3 (ctrl: 1) | ||
 : [30–40%];
: [30–40%];  : [20–30%];
: [20–30%];  : [10–20%];
: [10–20%];  : [5–10%];
: [5–10%];  : [0–5%];
: [0–5%];  : not reported. Data specific to older patients are underlined. Abbreviations: ctrl: control; ET: endocrine therapy; gr: grade; gr2+: grade 2 or more; nr: not reported.
: not reported. Data specific to older patients are underlined. Abbreviations: ctrl: control; ET: endocrine therapy; gr: grade; gr2+: grade 2 or more; nr: not reported.| Scheme | Treatment Regimen and Reference | Fatigue Any-Grade (%) | Fatigue Gr ≥ 3 (%) |
|---|---|---|---|
| First line | 3w-carboplatin monotherapy (ICON3) ≥70 (EWOT-3, EWOC-1) [66,106] | nr 73 | nr 8–15 |
| 3w-cisplatin 75 mg/m2 paclitaxel 185 mg/m2 (AGO OVAR-3) [108] | nr | nr | |
| 3w-cisplatin 75 mg/m2 paclitaxel 135 mg/m2 (GOG-158) [109] | nr | nr | |
| 3w-carboplatin AUC6 paclitaxel 185 mg/m2 (AGO OVAR-3) [108] | nr | nr | |
| ≥70 (AGO OVAR-3) [110] | nr | nr | |
| 3w-carboplatin AUC7.5 paclitaxel 175 mg/m2 (GOG-158) [109] | nr | nr | |
| 3w-carboplatin AUC5 paclitaxel 175 mg/m2 (MITO-2c) [107] | 44 | 3 | |
| ≥70 and GVS ≥3 (EWOC-1) [106] | 70 | 10 | |
| 3w-carboplatin AUC6 paclitaxel 175 mg/m2 (MITO-7) [111] | 48 | 5 | |
| 3w-carboplatin AUC5 PLD 30 mg/m2 (MITO-2i) [107] | 43 | 3 | |
| 3w-carboplatin AUC6 w-paclitaxel 80 mg/m2 (GOG262) [112] | nr | nr | |
| w-carboplatin AUC2 w-paclitaxel 60 mg/m2 (MITO-7) [111] | 55 | 4 | |
| Regimen specific to older patients 3w/4 carboplatin AUC2 + paclitaxel 60 mg/m2 (MITO-5, EWOC-1) (≥70) [107] | 38 | 0 | |
| ≥70 and GVS ≥3 (EWOC-1) [106] | 85 | 10 | |
| 15 mg/kg bevacizumab maintenance 3w-carboplatin AUC6 + paclitaxel 175 mg/m2 (GOG-218, PAOLAc) [113] | 32 | 1 | |
| 7.5 mg/kg bevacizumab maintenance 3w-carboplatin AUC6 + paclitaxel 175 mg/m2 (ICON7) [114] | nr | nr | |
| Olaparib maintenance (SOLO1) [103] | 63 (ctrl: 42) | 4 (ctrl: 2) | |
| Niraparib maintenance (PRIMA) [104] ≥65 [115] | 35 (ctrl: 30) nr | 2 (ctrl: <1) nr | |
| Rucaparib maintenance | |||
| Olaparib bevacizumab maintenance (PAOLA) [113] | 53 (ctrl: 32) | 5 (ctrl: 1) | |
| Platin-sensitive relapse | PLD/carboplatin [107] | 43 | 3 |
| Paclitaxel/carboplatin [107] | 44 | 3 | |
| Gemcitabine/cisplatin [116] | 28 | 2 | |
| Trabectidin/PLD [117] | nr | 6 | |
| Bevacizumab 3w-carboplatine w-paclitaxel (OCTAVIA) [118] | nr | nr | |
| Bevacizumab carboplatin gemcitabine 1000 mg/m2 J1,J8 (OCEANS) [119] | nr | nr | |
| Olaparib maintenance (SOLO2) [120] | 62 (ctrl: 37) | 4 (ctrl: 2) | |
| Niraparib maintenance (NOVA) [121] | 59 (ctrl: 41) | 8 (ctrl: 1) | |
| <70 [122] | nr | 8 (ctrl: 2) | |
| ≥70 [122] | nr | 8 (ctrl: 0) | |
| Rucaparib maintenance (ARIEL3) [123] | 69 (ctrl: 44) | 7 (ctrl: 3) | |
| Niraparib alone (w/o CT) (AVANOVA2) [124] | 39 | 2 | |
| Bevacizumab + niraparib w/o CT (AVANOVA2) [124] | 40 | 6 | |
| Platin-resistant relapse | Paclitaxel 175 mg/m2/3 sem [125] | nr | nr |
| Paclitaxel 175 mg/m2/3 sem [125] | nr | nr | |
| Paclitaxel 225 mg/m2/3 sem [125] | nr | nr | |
| Weekly paclitaxel | nr | nr | |
| 3w-topotecan [126,127] | 31–46 | 0–2 | |
| w-topotecan [128,129] | 32 | 2–22 | |
| PLD [117,130,131] | 22–44 | 1–6 | |
| Gemcitabine [130] | nr (gr2: 36) | 11 | |
| Docetaxel [132] | nr | nr | |
| Bevacizumab + chemotherapy (AURELIA) [133] | nr | 4 (ctrl: 10) |
: [30–40%]; : [20–30%]; : [10–20%]; : [5–10%]; : [0–5%]; : not reported. Data specific to older patients are underlined. Abbreviations: ctrl: control; gr: grade; gr2+: grade 2 or more; nr: not reported.| Setting | Treatment Regimen and Reference | Fatigue Any-Grade (%) | Fatigue Gr ≥3 (%) |
|---|---|---|---|
| Prostate cancers | |||
| Non metastatic castration resistant | ADT + apalutamide (SPARTAN) [136] | 33 (ctrl: 14) | 3 (ctrl: 1) |
| Metastatic castration sensitive | ADT [6] (LATITUDEc, STAMPEDEc, CHAARTEDc, TITANc, and SPARTANc) [136,137,138,139,140,141] | Any (FSS): 74% 14–20 | Severe (FSS): 14% <1–4 |
| LHRHa: | |||
| Leuprolide [135,142] | 6 | nr | |
| Goselerin [143,144] | nr | nr | |
| Triptorelin [142] | nr | nr | |
| Degarelix (induction 240 mg/maintenance 80 mg) | 3 | 0 | |
| ADT + abiraterone acetate (LATITUDEi and STAMPEDEi) [137,138] | 13 (ctrl: 14) | 2 (ctr: 2) | |
| ADT + enzalutamide (ENZAMET and ARCHES) [139,140] | 24 (ctrl: 20) | 2–6 (ctrl: 1–2) | |
| ADT + apalutamide (TITAN and SPARTAN) [136,141] | 20–32 (ctrl: 15–17) | 1–2 (ctrl: <1–1) | |
| ADT + docetaxel 75 mg/m2/3w (GETUG-AFU-15, E3805, and STAMPEDE) [145,146] | 74 (ctrl: 20) | 4–7 (ctrl: 1–4) | |
| Metastatic castration resistant | ADT + abiraterone acetate | ||
| After docetaxel (COU-AA-301) [147] <75 [148] ≥75 [148] In chemo-naive patients (COU-AA-302) [149] | 44 (ctrl: 43) 47 (ctrl: 45) 48 (ctrl: 42) 39 (ctrl: 34) | 8 (ctrl: 10) 8 (ctrl: 11) 13 (ctrl: 11) nr | |
| ADT + enzalutamide (STRIVE) [150] | 38 (ctrl: 28) | 5 (ctrl: 3) | |
| After docetaxel (AFFIRM) [151] At baseline [152] In chemo-naïve patients (PREVAIL) [153] | 34–62 (ctrl: 29, gr2+: 9) 64 (gr2+: 9) 36 (ctrl: 26) | 6 (ctrl: 7) 2 (ctrl: 2) nr | |
| 3w-docetaxel 75 mg/m2/3w [154] | 53 | 5 | |
| w-docetaxel 30 mg/m2/w [154] | 49 | 5 | |
| 2w-docetaxel 50 mg/m2 [155] | 65 (cyc; ctrl: 51) | 3 (cyc, ctrl: 3) | |
| Cabazitaxel 25 mg/m2/3w [156] | 37 | 5 | |
| Cabazitaxel 20 mg/m2/3w [157] | nr | nr | |
| Radium 223 chloride [158] | 24 (plb: 24) | 3 (plb: 6) | |
| Olaparib [159] | 41 (ctrl: 32) | 3 (ctrl: 5) | |
| Urothelial cancers | |||
| 1st line | MVAC [160,161] | nr | 24 |
| DDGc MVAC [161,162] | nr | nr | |
| Paclitaxel 225 mg/m2/carboplatin AUC6 [160] | nr | 10 | |
| Gemcitabine cisplatin [163] | nr | nr | |
| Gemcitabine weekly cisplatin [163] | nr | nr | |
| Gemcitabine carboplatin [163] | nr | nr | |
| Avelumab maintenance (JAVELIN Bladder 100) [164] | 18 (ctrl: 7) | 2 (ctrl: 1) | |
| 2nd line | Gemcitabine [163] | nr | nr |
| Vinflunine [165] | 50 (ctrl: 61) | 19 (ctrl: 18) | |
| Pembrolizumab (KEYNOTE-045) [166] | 14 (ctrl: 28) | 1 (ctrl: 4) | |
| 3rd line | Enfortumab vedotin (EV201, EV301) [167,168] | 31–50 (ctrl: 23) | 6 (ctrl: 5) |
: [30–40%]; : [20–30%]; : [10–20%]; : [5–10%]; : [0–5%]; : not reported. Data specific to older patients are underlined.| Scheme 3 | Treatment Regimen and Reference | Fatigue Any-Grade (%) | Fatigue Gr ≥3 (%) |
|---|---|---|---|
| Adjuvant | 5-FU/leucovorin (MOSAICc) [172,173] | 2–25 | <1–2 |
| Capecitabine [173] | 23 | 1 | |
| FOLFOX (MOSAICi and PETACC-8c) [172,174,175] | 63 | 4–5 | |
| XELOX/CAPOX 6mo (TOSCA, IDEA, SCOT, and HORG) [169,170,171] | SCOT: 90 (p = 0.022) TOSCA: 39 (asthenia) | SCOT: 8 IDEA: 5 (p = 0.0027) TOSCA: 4 (asthenia) | |
| XELOX/CAPOX 3mo (TOSCA, IDEA, SCOT, and HORG) [169,170,171] | SCOT: 86 (p = 0.022) TOSCA: 28 (asthenia, p < 0.0001) | SCOT: 8 IDEA: 3 (p = 0.0027) TOSCA: 1 (asthenia) | |
| Metastatic | Capecitabine ≥70 (AVEXc) [176] | 21–23 27 | 1 1 |
| FOLFOX [177,178] | 42 | 0–6 | |
| ≥72 [179] | 75 | 10 | |
| XELOX [180] | 62 | 9 | |
| ≥65 vs. < 65 [181] | 64 vs. 63 | 22 vs. 19 | |
| ≥70 [182] | 38 | 16 | |
| 2w-XELOX/CapeOX regimen specific to older patients (≥70) [183] | 46 | 6 | |
| FOCUS2 trial on older/frail patients not candidate for standard full-dose chemotherapy [184]: | |||
| 80% FU 80% FOLFOX (OxFU) 80% Cap (Capecitabine) 80% CapOx Fluorouracil vs. capecitabin (FU/FOLFOX vs. Cap/CapOx) Addition of oxaliplatin (FOLFOX/CpOx vs. FU/Cap) | nr (lethargy ≥ gr2: 38) nr (lethargy ≥ gr2: 42) nr (lethargy ≥ gr2: 36) nr (lethargy ≥ gr2: 43) lethargy ≥ gr2: 40 vs. 39 lethargy ≥ gr2: 37 vs. 43 | 7 (lethargy) 9 (lethargy) 13 (lethargy) 15 (lethargy) 8 vs. 14 (lethargy, p = 0.06) 10 vs. 12 (lethargy; p = 0.88) | |
| FOLFIRI [185,186,187,188,189] | 43–46 | 0–6 | |
| XELIRI [190,191,192,193,194,195] | 8–48 (≥gr2: 22%) | 0–8 | |
| CAPIRI [196] | nr | nr | |
| XELIRI weekly | nr | 5 | |
| XELIRI 2-weekly [197] | 57 | 13 | |
| FOLFOXIRI/FOLFIRINOX [186,189] | nr | 6 | |
| ≥70 [198] | 94 | 10 | |
| XELOXIRI [199] | 50 | 3 | |
| COI 2-weekly [200] | nr | nr | |
| IFL 21d [201] | 35 | 0–6 | |
| IRINOX [202] | 90 | 13 | |
| Raltitrexed [203] | nr | 5 | |
| TOMOX [178,204,205] | 35–53 | 4–16 | |
| TOMIRI [205,206] | 33–53 | 3–7 | |
| Bevacizumab–FOLFIRI [189,207,208,209] | 55–75 | 1–9 | |
| Bevacizumab XELIRI [210,211] | 67 | 7–17 | |
| Bevacizumab–FOLFOX [177,209,212] | 54–71 | 1–11 | |
| Bevacizumab XELOX [213] | 5 | 9 | |
| ≥70 [214] | 62 | 16 | |
| ≥75 [214,215] | 28–84 | 8 | |
| Bevacizumab–FOLFOXIRI [189,207] | nr | 12 | |
| Bevacizumab capecitabine | |||
| ≥70 (AVEXi) [176] | 24 | 4 | |
| ≥70/PS = 2 [216] | 67 | 13 | |
| Aflibercept–FOLFIRI [217] | 60 | 17 | |
| Cetuximab [218] | nr | 33 (ctrl: 26) | |
| Cetuximab–FOLFIRI [188,208] | 49 | <1–4 | |
| Cetuximab XELIRI [191] | nr | 5 (asthenia) | |
| Cetuximab–FOLFOX [219,220] | 66 | 8 | |
| Cetuximab XELOX [220] | nr | nr | |
| Cetuximab FOLFIRINOX [221] | nr | 32 | |
| Cetuximab-irinotecan [222,223] | 34–75 | 3–5 | |
| Panitumumab–FOLFIRI [224] | nr | nr | |
| Regorafenib [225] | 47 (ctrl: 28) | 9 (ctrl: 5) | |
| ≥70 (REGOLD) [226] | 90 | 45 | |
| TAS-102 (trifluridine–tipiracil) (RECOURSE) [227,228] | 35–85 (ctrl: 23) | 4–11 (ctrl: 6) | |
| Bevacizumab-TAS-102 (C-TASK FORCE) [228,229] | 24–85 | 0–7 | |
| Encorafenib cetuximab (BEACON) [230] | 30 (ctrl: 27) | 4 (ctrl: 4) | |
| Pembrolizumab (KEYNOTE 177) [231] | 38 (ctrl: 50) | 4 (ctrl: 9) |
: [30–40%]; : [20–30%]; : [10–20%]; : [5–10%]; : [0–5%]; : not reported. Data specific to older patients are underlined.| Setting | Treatment Regimen and Reference | Fatigue Any-Grade (%) | Fatigue Gr3 (%) |
|---|---|---|---|
| Non-small cell lung cancer | Docetaxel [238] | 27 | 4 |
| Docetaxel/carboplatin [233] | nr | 10–16 16 (weakness) 10 (asthenia) | |
| Etoposide/cisplatin [239] | nr | nr | |
| Paclitaxel/cisplatin [232,233] | nr | 9 (lethargy)- 15 (weakness) | |
| Docetaxel/cisplatin [232,233,240] | nr | 7–16 | |
| Vinorelbine/cisplatin [233] | nr | 9 | |
| Paclitaxel/carboplatin [232,233] | nr | 9–15 | |
| Carboplatin paclitaxel regimen specific to older patients (3w-carboplatin AUC6, w-paclitaxel 90mg/m2) (≥70) [241] | nr | 10 (asthenia) | |
| Pemetrexed/cisplatin [233] | nr | 7 | |
| Carboplatin/pemetrexed [242] PCb5 (Carboplatin AUC5) PCb6 (Carboplatin AUC6) | 11–48 11 48 | 0–3 0 3 | |
| Pembrolizumab/pemetrexed/cisplatin or carboplatin [236] | 41 | 6 | |
| Gemcitabine/cisplatin [232,233,240] | nr | 8–40 | |
| Gemcitabine/carboplatin [233] | nr | 40 | |
| Bevacizumab carboplatin/paclitaxel [234,235] | 20–45 | 3–5 | |
| Bevacizumab atezolizumab carboplatin/paclitaxel [235] | 22 | 3 | |
| Bevacizumab carboplatin/pemetrexed [234] | 53 | 11 | |
| Nivolumab 10mg/kg + gemcitabine/cisplatin [237] | 67 | 0 | |
| Nivolumab 10mg/kg + pemetrexed/cisplatin [237] | 80 | 7 | |
| Nivolumab 10mg/kg + paclitaxel/carboplatin [237] | 67 | 13 | |
| Nivolumab 5mg/kg + paclitaxel/carboplatin [237] | 71 | 0 | |
| Gemcitabine/docetaxel ≥70 [243] | nr 48 | nr 6 | |
| Gemcitabine (maintenance) [244] ≥70 [243] | nr 31 | nr 6 | |
| Pemetrexed (maintenance) [245] | 24 | 5 | |
| Bevacizumab pemetrexed (maintenance) [234] | 49 | 3 | |
| Bevacizumab (maintenance) [234] | 62 | 12 | |
| Erlotinib [233] | 3 | 0 | |
| Crizotinib [246] | 27 | 2 | |
| Ceritinib [247] | 47 | 5 | |
| Gefitinib [233] | nr | 3 | |
| Nintedanib-docetaxel [238] | 30 | 6 | |
| Small cell lung cancer | ACE [248] | nr | 13 |
| Topotecan [249,250] | 26 | 4 | |
| Topotecan/paclitaxel [251] | nr | 22 | |
| ICE [252,253,254] | nr | nr | |
| wICE [252] | nr | nr | |
| VICE [255,256] | 66 | nr | |
| DDG ACE [257] | nr | nr | |
| DDG ICE [253] | nr | nr | |
| DDG CAV → PE [258] | nr | nr | |
| Paclitaxel carboplatin topotecan [259] | nr | 12 | |
| CAV [249] | 34 | nr | |
| Etoposide/cisplatin [260,261,262,263] | 11 | <1–2 | |
| Etoposide/carboplatin [263,264] | 11 | <1 | |
| Irinotecan/carboplatin [264,265] | nr | nr | |
| Irinotecan/cisplatin [261] | nr | nr | |
| Ipilimumab-Etoposide/cisplatin [263] | 13 | 2 | |
| Topotecan/cisplatin [262,266] | 13 | 1–3 | |
| Docetaxel/gemcitabine [267] Age > 65 or PS=2 [268] | nr nr | nr 25 | |
| Irinotecan/gemcitabine [269] | nr | 9–15 | |
| CODE [270,271] | nr | nr | |
| CAV → PE [258,270,271] | nr | nr | |
| Paclitaxel/carboplatin [248] consolidation after CT-RT [272] | nr nr | 9 15 | |
| Nab P/C 3w [273] | nr | 1 | |
| Nab-P/C w [273] | nr | 0 | |
| wPaclitaxel 80mg/m2/sem [274] | 27 | 1 | |
| Gemcitabine [275,276] | nr | nr |
: [30–40%]; : [20–30%]; : [10–20%]; : [5–10%]; : [0–5%]; : not reported. Data specific to older patients are underlined.| Setting | Treatment Regimen and Reference | Fatigue Any-Grade (%) | Fatigue Gr3 (%) |
|---|---|---|---|
| Diffuse large B-cell lymphoma | CHOP-21 [286] CHOP: data specific to older patients (60–80) [280,281,282] | nr nr | nr nr |
| DHAP [287] | nr | nr | |
| ESHAP [288,289,290] | nr | nr | |
| CNOP [286] | nr | nr | |
| ACOD [291] | 3 | 0 | |
| Fludarabine/mitoxantrone [292] | nr | nr | |
| R-CHOP-21 [277,278] | 27–46 | 3 | |
| R-CHOP: data specific to older patients (>60) [280,281,282,284,293,294] | 49 | 0 | |
| R-CHOP–Lenalinomide maintenance: data specific to older patients (58–80) [295] | nr | nr | |
| R-miniCHOP regimen specific to older patients (≥80) [283] | nr | nr | |
| R-COMP [284,296]: data specific to older patients | 53 | 7 | |
| R-mini-CHP: regimen specific to older patients (≥80) [297] | nr | nr | |
| R-mini-CEOP regimen specific to “frail” patients (64–84 years) [298] | nr | nr | |
| R-CVP [277] | 53 | <1 | |
| R-mini-CVP regimen specific to older patients (≥80) [285] | 58 | 47 | |
| DA-EPOCH-R [299] | nr | nr | |
| R-pola-CHP 21 [278] | 26 | 1 | |
| R-DHAP [279] | nr | 9 | |
| R-GemOx [300] | nr | nr | |
| Lenalinomide–rituximab [301,302,303] | nr | 13–23 | |
| Lenalinomide [302,303,304] | 34 | 7–9 | |
| Tafasitamab–lenalidomide (L-MIND) [305] | 15 | 2 | |
| CAR-T Lisocabtagene maraleucel (TRANSCEND NHL 001) [306] | 44 | 1 | |
| CAR-T Axicabtagene ciloleucel (ZUMA-1) [307] | 51 | 2 | |
| CAR-T Tisagenlecleucel (JULIET) [308] | 25 | 6 | |
| CAR-T real life experience USA [309] | nr | nr | |
| France [310] | nr | nr | |
| Indolent lymphomas | Rituximab [311] | 22 | nr |
| Bendamustine-rituximab (BRIGHT) [277] | 44–58 | 3–4 | |
| R-CHOP (FOLL05 and BRIGHT) [277] | 46 | 2 | |
| R-CVP (FOLL05 and BRIGHT) [277] | 53 | <1 | |
| R-FM (FOLL05) [312] | nr | nr | |
| Rituximab-chemotherapy [313] | 37 | nr | |
| G-CHOP (GALLIUM) [314] | 16 | nr | |
| G-CVP (GALLIUM) [314] | 57 | nr | |
| G-Bendamustine (GALLIUM) [314] | 44 | nr | |
| Obinutuzumab-chemotherapy [313] | 36 | nr | |
| Revlimid–lenalidomide (CALGB 50803) [315] | 78 | 6 |
: [30–40%]; : [20–30%]; : [10–20%]; : [5–10%]; : [0–5%]; : not reported. Data specific to older patients are underlined.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
André, L.; Antherieu, G.; Boinet, A.; Bret, J.; Gilbert, T.; Boulahssass, R.; Falandry, C. Oncological Treatment-Related Fatigue in Oncogeriatrics: A Scoping Review. Cancers 2022, 14, 2470. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102470
André L, Antherieu G, Boinet A, Bret J, Gilbert T, Boulahssass R, Falandry C. Oncological Treatment-Related Fatigue in Oncogeriatrics: A Scoping Review. Cancers. 2022; 14(10):2470. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102470
Chicago/Turabian StyleAndré, Louise, Gabriel Antherieu, Amélie Boinet, Judith Bret, Thomas Gilbert, Rabia Boulahssass, and Claire Falandry. 2022. "Oncological Treatment-Related Fatigue in Oncogeriatrics: A Scoping Review" Cancers 14, no. 10: 2470. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102470