
Radioactive Iodine Treatment for Thyroid Cancer Patients Increases the Risk of Long-Term Gastrointestinal Disorders: A Nationwide Population-Based Cohort Analysis

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Ethics Considerations
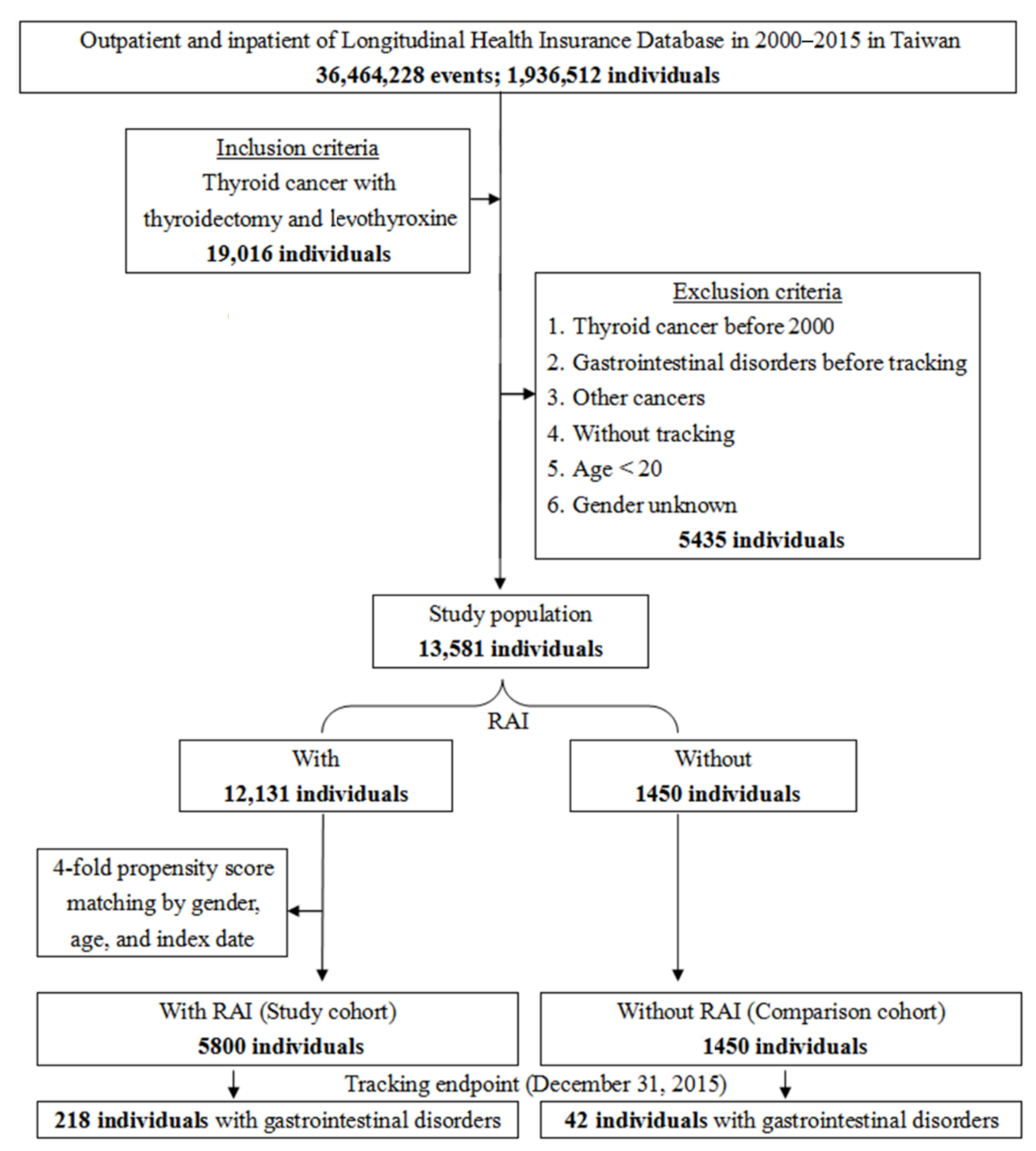
2.3. Study Design, Subjects, and Outcome
2.4. Comorbidities and Methods of Thyroid-Stimulating Hormone (TSH) Stimulation
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study and Control Cohorts
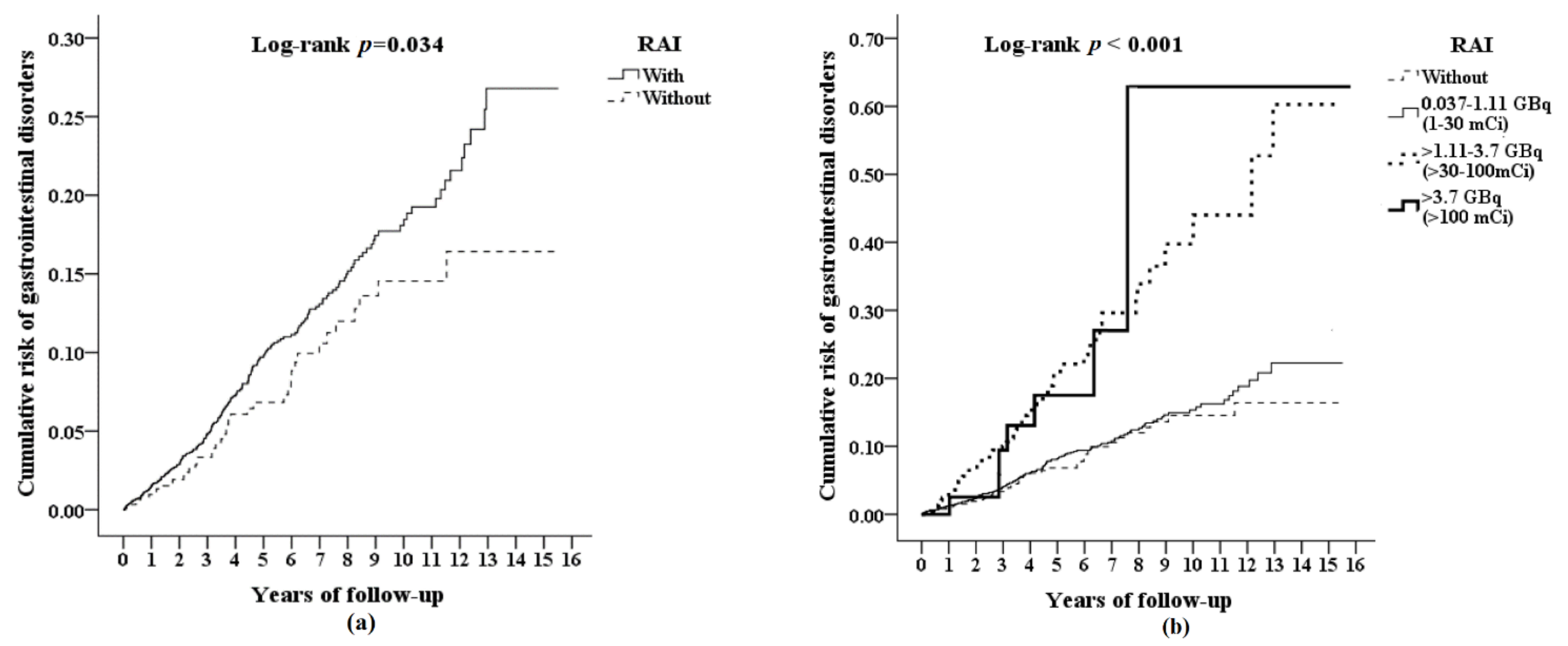
3.2. Cumulative Risk of Gastrointestinal Disorders
3.3. Risk Factors of Gastrointestinal Disorders
3.4. Cumulative RAI Dose and the Risk of Gastrointestinal Disorders
3.5. Risks of Subgroups of Gastrointestinal Disorders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Malvezzi, M.; Bosetti, C.; Garavello, W.; Bertuccio, P.; Levi, F.; Negri, E. Thyroid cancer mortality and incidence: A global overview. Int. J. Cancer 2015, 136, 2187–2195. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974–2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef] [PubMed]
- Ceresini, G.; Corcione, L.; Michiara, M.; Sgargi, P.; Teresi, G.; Gilli, A.; Usberti, E.; Silini, E.; Ceda, G.P. Thyroid cancer incidence by histological type and related variants in a mildly iodine-deficient area of Northern Italy, 1998 to 2009. Cancer 2012, 118, 5473–5480. [Google Scholar] [CrossRef]
- Zaballos, M.A.; Santisteban, P. Key signaling pathways in thyroid cancer. J. Endocrinol. 2017, 235, R43–R61. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Off. J. Am. Thyroid. Assoc. 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Cushing, S.L.; Palme, C.E.; Audet, N.; Eski, S.; Walfish, P.G.; Freeman, J.L. Prognostic factors in well-differentiated thyroid carcinoma. Laryngoscope 2004, 114, 2110–2115. [Google Scholar] [CrossRef]
- Fard-Esfahani, A.; Emami-Ardekani, A.; Fallahi, B.; Fard-Esfahani, P.; Beiki, D.; Hassanzadeh-Rad, A.; Eftekhari, M. Adverse effects of radioactive iodine-131 treatment for differentiated thyroid carcinoma. Nucl. Med. Commun. 2014, 35, 808–817. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.L. Complications of radioactive iodine treatment of thyroid carcinoma. J. Natl. Compr. Cancer Netw. JNCCN 2010, 8, 1277–1286. [Google Scholar] [CrossRef] [Green Version]
- Alexander, C.; Bader, J.B.; Schaefer, A.; Finke, C.; Kirsch, C.M. Intermediate and long-term side effects of high-dose radioiodine therapy for thyroid carcinoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1998, 39, 1551–1554. [Google Scholar]
- Van Nostrand, D.; Neutze, J.; Atkins, F. Side effects of “rational dose” iodine-131 therapy for metastatic well-differentiated thyroid carcinoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1986, 27, 1519–1527. [Google Scholar]
- Hong, E.P.; Park, J.W. Sample size and statistical power calculation in genetic association studies. Genom. Inform. 2012, 10, 117–122. [Google Scholar] [CrossRef]
- Brusselaers, N.; Lagergren, J. The Charlson Comorbidity Index in Registry-based Research. Methods Inf. Med. 2017, 56, 401–406. [Google Scholar] [CrossRef]
- Desouky, O.; Ding, N.; Zhou, G. Targeted and non-targeted effects of ionizing radiation. J. Radiat. Res. Appl. Sci. 2015, 8, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Vieja, A.D.L.; Santisteban, P. Role of iodide metabolism in physiology and cancer. Endocr. Relat. Cancer 2018, 25, R225–R245. [Google Scholar] [CrossRef]
- Mitsuma, T.; Rhue, N.; Hirooka, Y.; Kayama, M.; Yokoi, Y.; Mori, Y.; Ping, J.; Adachi, K.; Wago, T.; Ohtake, M. Organ distribution of iodide transporter (symporter) in the rat: Immunohistochemical study. Endocr. Regul. 1997, 31, 15–18. [Google Scholar]
- Nicola, J.P.; Basquin, C.; Portulano, C.; Reyna-Neyra, A.; Paroder, M. The Na+/I− symporter mediates active iodide uptake in the intestine. Am. J. Physiol. Cell Physiol. 2009, 296, C654–C662. [Google Scholar] [CrossRef] [Green Version]
- Altorjay, A.; Dohan, O.; Szilagyi, A.; Paroder, M.; Wapnir, I.L.; Carrasco, N. Expression of the Na+/I− symporter (NIS) is markedly decreased or absent in gastric cancer and intestinal metaplastic mucosa of Barrett esophagus. BMC Cancer 2007, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Bruno, R.; Giannasio, P.; Ronga, G.; Baudin, E.; Travagli, J.P.; Russo, D.; Filetti, S.; Schlumberger, M. Sodium iodide symporter expression and radioiodine distribution in extrathyroidal tissues. J. Endocrinol. Investig. 2004, 27, 1010–1014. [Google Scholar] [CrossRef]
- Johansson, L.; Leide-Svegborn, S.; Mattsson, S.; Nosslin, B. Biokinetics of iodide in man: Refinement of current ICRP dosimetry models. Cancer Biother. Radiopharm. 2003, 18, 445–450. [Google Scholar] [CrossRef]
- Brill, A.B.; Stabin, M.; Bouville, A.; Ron, E. Normal organ radiation dosimetry and associated uncertainties in nuclear medicine, with emphasis on iodine-131. Radiat. Res. 2006, 166, 128–140. [Google Scholar] [CrossRef]
- Coia, L.R.; Myerson, R.J.; Tepper, J.E. Late effects of radiation therapy on the gastrointestinal tract. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1213–1236. [Google Scholar] [CrossRef]
- Goldgraber, M.B.; Rubin, C.E.; Palmer, W.L.; Dobson, R.L.; Massey, B.W. The early gastric response to irradiation; a serial biopsy study. Gastroenterology 1954, 27, 1–20. [Google Scholar] [CrossRef]
- Henriksson, R.; Bergström, P.; Franzén, L.; Lewin, F.; Wagenius, G. Aspects on reducing gastrointestinal adverse effects associated with radiotherapy. Acta Oncol. 1999, 38, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Czito, B.; Meyer, J.; Willett, C. Overview of Gastrointestinal Toxicity of Radiation Therapy; Drews, R., Ed.; UpToDate: Waltham, MA, USA, 2017. [Google Scholar]
- Cosset, J.M.; Henry-Amar, M.; Burgers, J.M.; Noordijk, E.M.; Van der Werf-Messing, B.; Meerwaldt, J.H.; van der Schueren, E. Late radiation injuries of the gastrointestinal tract in the H2 and H5 EORTC Hodgkin’s disease trials: Emphasis on the role of exploratory laparotomy and fractionation. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 1988, 13, 61–68. [Google Scholar] [CrossRef]
- Sell, A.; Jensen, T.S. Acute gastric ulcers induced by radiation. Acta Radiol. Ther. Phys. Biol. 1966, 4, 289–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blesl, A.; Brcic, I.; Jaschke, W.; Öfner, D.; Fickert, P.; Plank, J. Chronic gastric ulcer disease complicating selective internal radiation therapy (SIRT) in a patient with cholangiocellular carcinoma. Z. Fur Gastroenterol. 2019, 57, 1304–1308. [Google Scholar] [CrossRef] [PubMed]
- Yumusak, N.; Sadic, M.; Akbulut, A.; Aydinbelge, F.N.; Koca, G.; Korkmaz, M. Beneficial effects of vitamin E on radioiodine induced gastrointestinal damage: An experimental and pathomorphological study. Bratisl. Lek. Listy 2019, 120, 263–269. [Google Scholar] [CrossRef]
- Sadic, M.; Aydinbelge, F.N.; Yumusak, N.; Karakok, E.; Akbulut, A.; Koca, G.; Korkmaz, M. Radioprotective effect of lycopene on the gastrointestinal tract after high-dose radioiodine administration in rat models. Nucl. Med. Commun. 2017, 38, 1041–1046. [Google Scholar] [CrossRef]
- Emami, B.; Lyman, J.; Brown, A.; Coia, L.; Goitein, M.; Munzenrider, J.E.; Shank, B.; Solin, L.J.; Wesson, M. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 109–122. [Google Scholar] [CrossRef]
- Brick, I.B. Effects of million volt irradiation on the gastrointestinal tract. A.M.A. Arch. Intern. Med. 1955, 96, 26–31. [Google Scholar] [CrossRef]
- Marshall, B.J.; Warren, J.R. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1984, 1, 1311–1315. [Google Scholar] [CrossRef]
- Arduc, A.; Dogan, B.A.; Ozuguz, U.; Tuna, M.M.; Gokay, F.; Tutuncu, Y.A.; Isik, S.; Aydin, Y.; Peksoy, I.; Berker, D.; et al. The effect of radioactive iodine treatment on 14C urea breath test results in patients with hyperthyroidism. Clin. Nucl. Med. 2014, 39, 1022–1026. [Google Scholar] [CrossRef]
- Gholamrezanezhad, A.; Mirpour, S.; Saghari, M.; Abdollahzadeh, J.; Pourmoslemi, A.; Yarmand, S. Radio-iodine therapy and Helicobacter pylori infection. Ann. Nucl. Med. 2008, 22, 917–920. [Google Scholar] [CrossRef]
- Xu, F.; Tang, L.; Yuan, H.; Liu, J.; Huang, G.; Song, S. Iodine-131 in Helicobacter pylori-positive patients: Preliminary accidental finding and in differentiated thyroid cancer. Nucl. Med. Commun. 2016, 37, 1136–1138. [Google Scholar] [CrossRef]
- Usluoğullari, C.A.; Demir Önal, E.; Özdemir, E.; Caner, S.; Ersoy, O.; Ersoy, R.; Çakir, B. What is the effect of radioiodine therapy on Helicobacter pylori infection? Turk. J. Med. Sci. 2014, 44, 520–523. [Google Scholar] [CrossRef]
- Ferrari, S.M.; Fallahi, P.; Elia, G.; Ragusa, F.; Ruffilli, I.; Paparo, S.R.; Antonelli, A. Thyroid autoimmune disorders and cancer. Semin. Cancer Biol. 2020, 64, 135–146. [Google Scholar] [CrossRef]
- Sharma, B.R.; Joshi, A.S.; Varthakavi, P.K.; Chadha, M.D.; Bhagwat, N.M.; Pawal, P.S. Celiac autoimmunity in autoimmune thyroid disease is highly prevalent with a questionable impact. Indian J. Endocrinol. Metab. 2016, 20, 97–100. [Google Scholar] [CrossRef]
- Starchl, C.; Scherkl, M.; Amrein, K. Celiac Disease and the Thyroid: Highlighting the Roles of Vitamin D and Iron. Nutrients 2021, 13, 1755. [Google Scholar] [CrossRef]
- Kahaly, G.J.; Frommer, L.; Schuppan, D. Celiac Disease and Glandular Autoimmunity. Nutrients 2018, 10, 814. [Google Scholar] [CrossRef] [Green Version]
- Iizuka, Y.; Katagiri, T.; Ogura, K.; Inoue, M.; Nakamura, K.; Mizowaki, T. Comparison of thyroid hormone withdrawal and recombinant human thyroid-stimulating hormone administration for adjuvant therapy in patients with intermediate- to high-risk differentiated thyroid cancer. Ann. Nucl. Med. 2020, 34, 736–741. [Google Scholar] [CrossRef]
- Klubo-Gwiezdzinska, J.; Burman, K.D.; Van Nostrand, D.; Mete, M.; Jonklaas, J.; Wartofsky, L. Radioiodine treatment of metastatic thyroid cancer: Relative efficacy and side effect profile of preparation by thyroid hormone withdrawal versus recombinant human thyrotropin. Thyroid. Off. J. Am. Thyroid. Assoc. 2012, 22, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Teng, C.J.; Hu, Y.W.; Chen, S.C.; Yeh, C.M.; Chiang, H.L.; Chen, T.J.; Liu, C.J. Use of Radioactive Iodine for Thyroid Cancer and Risk of Second Primary Malignancy: A Nationwide Population-Based Study. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef] [Green Version]
- Shahid, M.A.; Ashraf, M.A.; Sharma, S. Physiology, Thyroid Hormone; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Rosenthal, F.D.; Jones, C.; Lewis, S.I. Thyrotoxic vomiting. Br. Med. J. 1976, 2, 209–211. [Google Scholar] [CrossRef] [Green Version]
- Davis, P.J.; Davis, F.B. Hyperthyroidism in patients over the age of 60 years. Clinical features in 85 patients. Medicine 1974, 53, 161–181. [Google Scholar] [CrossRef]
- Koyuncu, A.; Aydintu, S.; Koçak, S.; Aydin, C.; Demirer, S.; Topçu, O.; Kuterdem, E. Effect of thyroid hormones on stress ulcer formation. ANZ J. Surg. 2002, 72, 672–675. [Google Scholar] [CrossRef]
- Suh, B.; Shin, D.W.; Park, Y.; Lim, H.; Yun, J.M.; Song, S.O.; Park, J.H.; Cho, B.; Guallar, E. Increased cardiovascular risk in thyroid cancer patients taking levothyroxine: A nationwide cohort study in Korea. Eur. J. Endocrinol. 2019, 180, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.Q.; Sridhar, S.; Hunt, R.H. Role of Helicobacter pylori infection and non-steroidal anti-inflammatory drugs in peptic-ulcer disease: A meta-analysis. Lancet 2002, 359, 14–22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | With RAI Study Cohort | Without RAI Comparison Cohort | p | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Total | 7250 | 5800 | 80.00 | 1450 | 20.00 | ||
| Gender | 0.999 | ||||||
| Male | 1505 | 20.76 | 1204 | 20.76 | 301 | 20.76 | |
| Female | 5745 | 79.24 | 459 | 79.24 | 1149 | 79.24 | |
| Age (years) | 47.40 ± 13.34 | 47.55 ± 13.22 | 46.79 ± 13.77 | 0.052 | |||
| Age groups (years) | 0.999 | ||||||
| 20–39 | 2190 | 30.21 | 1752 | 30.21 | 438 | 30.21 | |
| 40–59 | 3800 | 52.41 | 3040 | 52.41 | 760 | 52.41 | |
| 60–79 | 1205 | 16.62 | 964 | 16.62 | 241 | 16.62 | |
| ≥80 | 55 | 0.76 | 44 | 0.76 | 11 | 0.76 | |
| Helicobacter pylori infection | 0.365 | ||||||
| Without | 7248 | 99.97 | 5799 | 99.98 | 1449 | 99.93 | |
| With | 2 | 0.03 | 1 | 0.02 | 1 | 0.07 | |
| Obesity | 0.999 | ||||||
| Without | 7245 | 99.93 | 5796 | 99.93 | 1449 | 99.93 | |
| With | 5 | 0.07 | 4 | 0.07 | 1 | 0.07 | |
| Alcoholism | 0.613 | ||||||
| Without | 7249 | 99.99 | 5799 | 99.98 | 1450 | 100.00 | |
| With | 1 | 0.01 | 1 | 0.02 | 0 | 0.00 | |
| Chronic lymphocytic thyroiditis | 0.814 | ||||||
| Without | 7135 | 98.41 | 5707 | 98.40 | 1428 | 98.48 | |
| With | 115 | 1.59 | 93 | 1.60 | 22 | 1.52 | |
| Celiac disease | 0.944 | ||||||
| Without | 7038 | 97.08 | 5630 | 97.07 | 1408 | 97.10 | |
| With | 212 | 2.92 | 170 | 2.93 | 42 | 2.90 | |
| CCI_R | 0.10 ± 0.41 | 0.11 ± 0.42 | 0.09 ± 0.37 | 0.119 | |||
| rhTSH (Thyrogen) | 0.255 | ||||||
| Without | 7005 | 96.62 | 5611 | 96.74 | 1394 | 96.14 | |
| With | 245 | 3.38 | 189 | 3.26 | 56 | 3.86 | |
| Variables | Crude HR | 95% CI | 95% CI | p | Adjusted HR | 95% CI | 95% CI | p |
|---|---|---|---|---|---|---|---|---|
| RAI | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.360 | 1.077 | 1.892 | 0.034 * | 1.314 | 1.040 | 1.842 | 0.029 * |
| Gender | ||||||||
| Male | 1.565 | 1.193 | 2.054 | 0.001 * | 1.395 | 1.068 | 1.849 | 0.011 * |
| Female | Reference | Reference | ||||||
| Age groups (years) | ||||||||
| 20–39 | Reference | Reference | ||||||
| 40–59 | 1.927 | 1.200 | 3.092 | 0.007 * | 1.869 | 1.157 | 3.015 | 0.009 * |
| 60–79 | 2.963 | 1.851 | 4.744 | <0.001 * | 2.493 | 1.532 | 4.058 | <0.001 * |
| ≥80 | 5.292 | 3.132 | 8.943 | <0.001 * | 4.462 | 2.599 | 7.642 | <0.001 * |
| Helicobacter pylori infection | ||||||||
| Without | Reference | Reference | ||||||
| With | 7.511 | 1.052 | 53.604 | 0.044 * | 8.267 | 1.531 | 75.129 | 0.020 * |
| Obesity | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | − | − | 0.974 | 0.000 | − | − | 0.994 |
| Alcoholism | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | − | − | 0.83 | 0.000 | − | − | 0.956 |
| Chronic lymphocytic thyroiditis | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | − | − | 0.979 | 0.000 | − | − | 0.993 |
| Celiac disease | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | − | − | 0.988 | 0.000 | − | − | 0.997 |
| CCI_R | 1.458 | 1.302 | 1.633 | <0.001 * | 1.318 | 1.163 | 1.494 | <0.001 * |
| rhTSH (Thyrogen) | ||||||||
| Without | Reference | Reference | ||||||
| With | 7.065 | 0.789 | 459.780 | 0.832 | 2.301 | 0.341 | 86.010 | 0.897 |
| Dose of RAI | Populations | Events | PYs | Rate (per 105 PYs) | Adjusted HR | 95% CI | 95% CI | p |
|---|---|---|---|---|---|---|---|---|
| Without | 1450 | 42 | 3169.54 | 1325.11 | Reference | |||
| With | 5800 | 218 | 12,034.78 | 1811.42 | 1.314 | 1.040 | 1.842 | 0.029 * |
| 0.037–1.11 GBq (1–30 mCi) | 5391 | 162 | 10,522.26 | 1539.59 | 1.150 | 0.357 | 1.656 | 0.813 |
| >1.11–3.7 GBq (>30–100 mCi) | 357 | 48 | 1299.18 | 3694.62 | 2.183 | 1.497 | 3.578 | 0.002 * |
| >3.7 GBq (>100 mCi) | 52 | 8 | 213.34 | 3749.93 | 2.209 | 1.556 | 4.282 | 0.001 * |
| With RAI | Without RAI | With vs. Without (Reference) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome Subgroup | Events | PYs | Rate (per 105 PYs) | Events | PYs | Rate (per 105 PYs) | Ratio | Adjusted HR | 95% CI | 95% CI | p |
| Any of the listed gastrointestinal disorder | 218 | 12,034.78 | 1811.42 | 42 | 3169.54 | 1325.11 | 1.367 | 1.314 | 1.040 | 1.842 | 0.029 * |
| Ulcer | 212 | 12,034.78 | 1761.56 | 39 | 3169.54 | 1230.46 | 1.432 | 1.372 | 1.075 | 1.927 | 0.021 * |
| Gastric ulcer | 121 | 12,034.78 | 1005.42 | 23 | 3169.54 | 725.66 | 1.386 | 1.456 | 1.066 | 3.279 | 0.032 * |
| Duodenal ulcer | 47 | 12,034.78 | 390.53 | 7 | 3169.54 | 220.85 | 1.768 | 3.983 | 1.192 | 16.738 | 0.001 * |
| Peptic ulcer | 44 | 12,034.78 | 365.61 | 9 | 3169.54 | 283.95 | 1.288 | 1.299 | 0.482 | 5.411 | 0.243 |
| Gastrojejunal ulcer | 0 | 12,034.78 | 0.00 | 0 | 3169.54 | 0.00 | − | − | − | − | − |
| Malignant neoplasm of stomach | 5 | 12,034.78 | 41.55 | 3 | 3169.54 | 94.65 | 0.439 | 0.668 | 0.178 | 2.620 | 0.533 |
| Atrophic gastritis | 1 | 12,034.78 | 8.31 | 0 | 3169.54 | 0.00 | ∞ | ∞ | − | − | 0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Chung, C.-H.; Lin, L.-F.; Chiu, C.-H.; Chen, Y.-F.; Chang, C.-F.; Cheng, C.-Y.; Chien, W.-C. Radioactive Iodine Treatment for Thyroid Cancer Patients Increases the Risk of Long-Term Gastrointestinal Disorders: A Nationwide Population-Based Cohort Analysis. Cancers 2022, 14, 2505. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102505
Lee Y, Chung C-H, Lin L-F, Chiu C-H, Chen Y-F, Chang C-F, Cheng C-Y, Chien W-C. Radioactive Iodine Treatment for Thyroid Cancer Patients Increases the Risk of Long-Term Gastrointestinal Disorders: A Nationwide Population-Based Cohort Analysis. Cancers. 2022; 14(10):2505. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102505
Chicago/Turabian StyleLee, Yueh, Chi-Hsiang Chung, Li-Fan Lin, Chuang-Hsin Chiu, Yi-Feng Chen, Chao-Feng Chang, Cheng-Yi Cheng, and Wu-Chien Chien. 2022. "Radioactive Iodine Treatment for Thyroid Cancer Patients Increases the Risk of Long-Term Gastrointestinal Disorders: A Nationwide Population-Based Cohort Analysis" Cancers 14, no. 10: 2505. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102505