
Clinical and Economic Impact of a Multidisciplinary Follow-Up Program in Lymphoma Patients

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
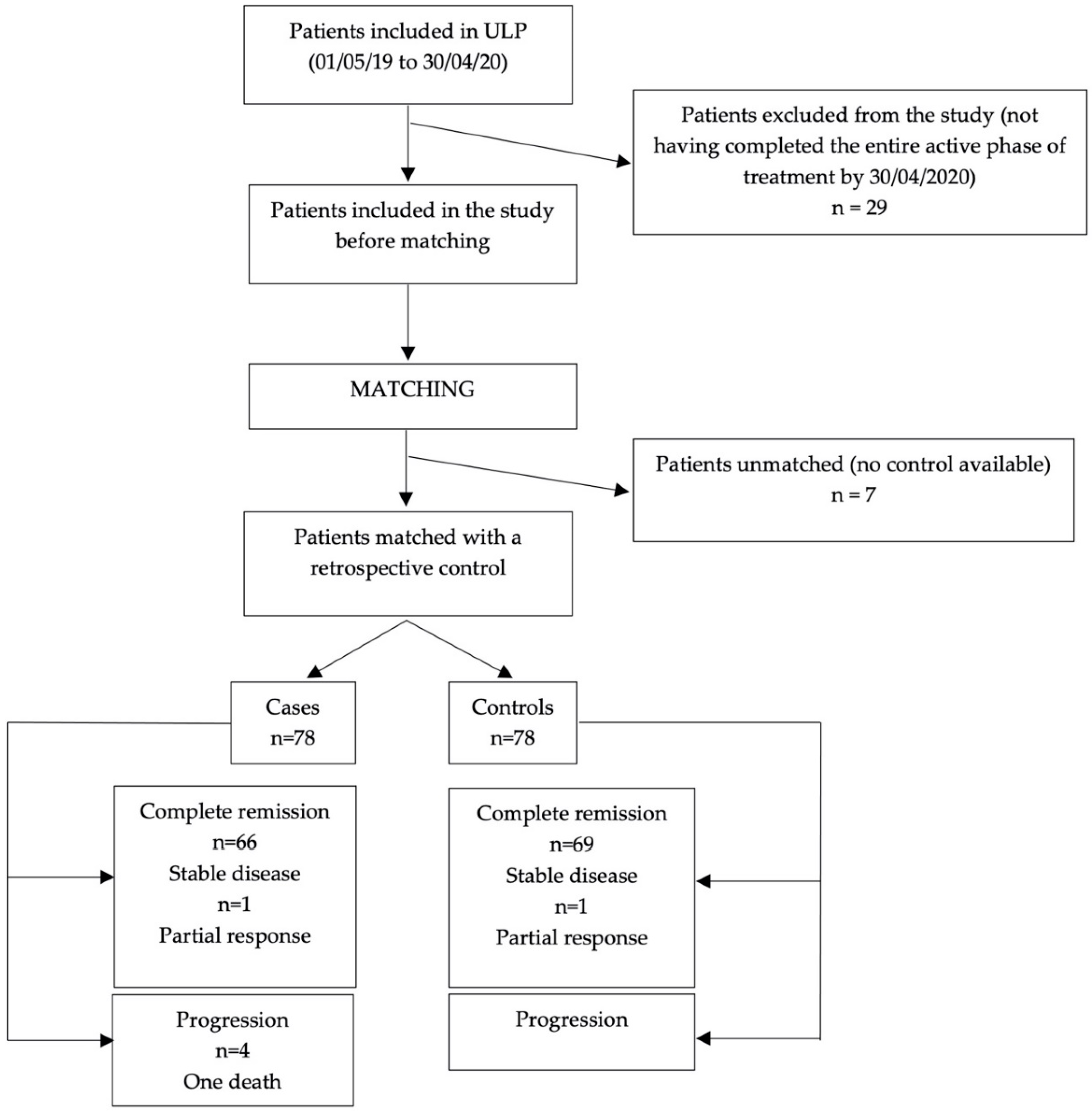
2.1. Study Design and Population
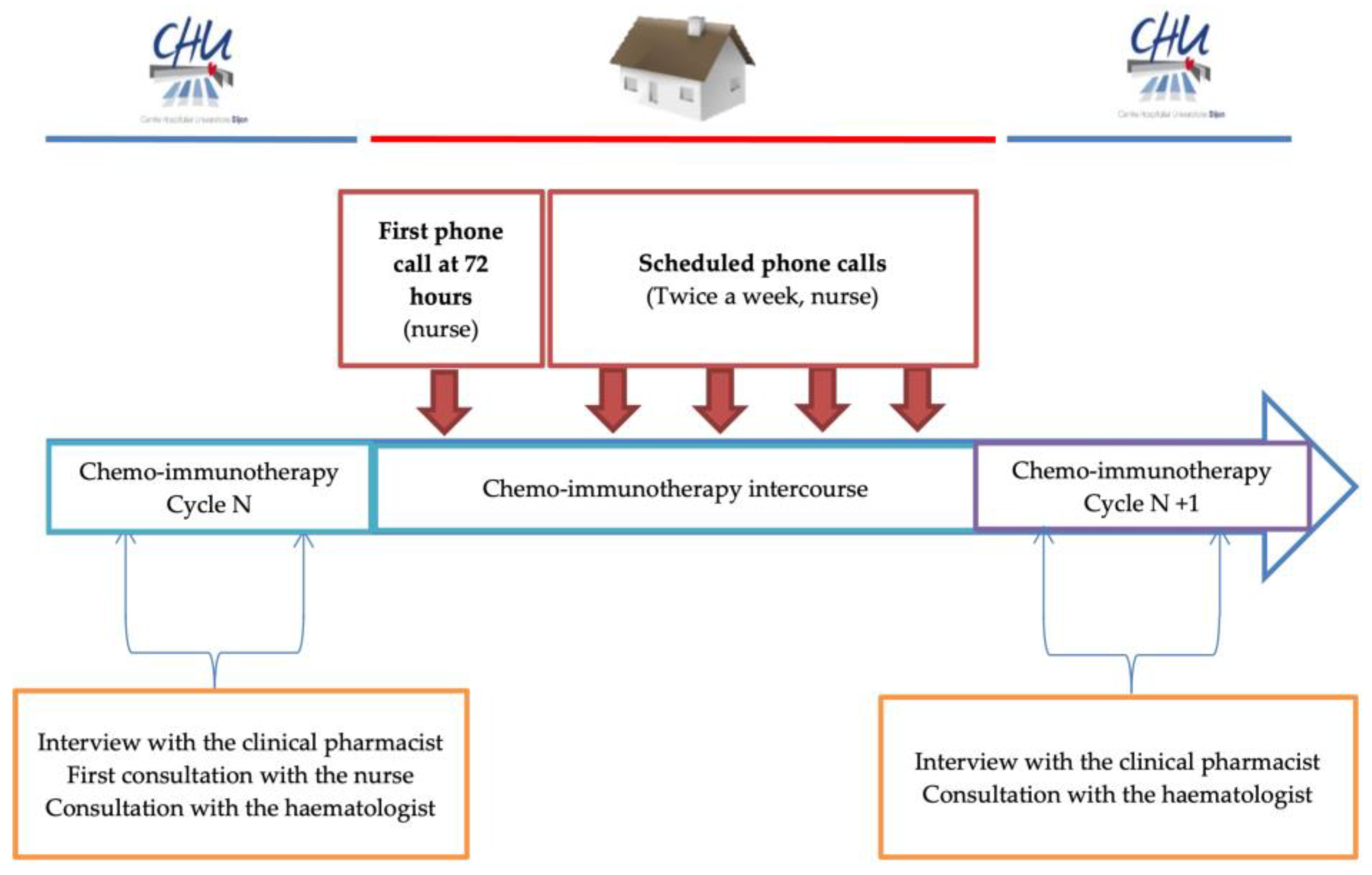
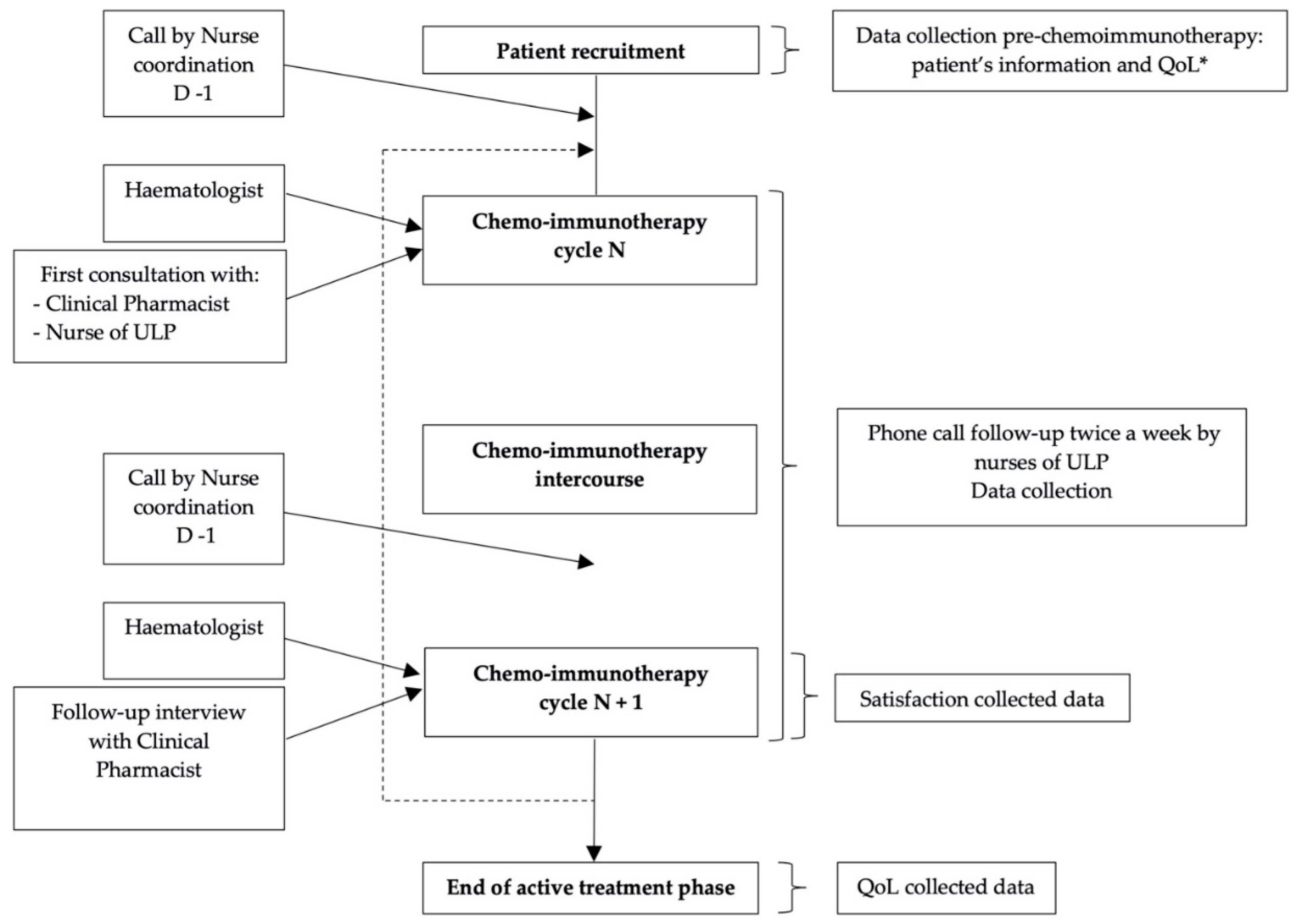
2.2. Description of the UMACOACH Lymphoma Program
2.2.1. Nurse Intervention
2.2.2. Pharmacist Interventions (PI)
2.3. Clinical and Economic Evaluation
2.3.1. Clinical Impact
2.3.2. Economic Impact
2.4. Quality of Life and Patient Satisfaction
2.5. Statistical Analyses
3. Results
3.1. ULP Description
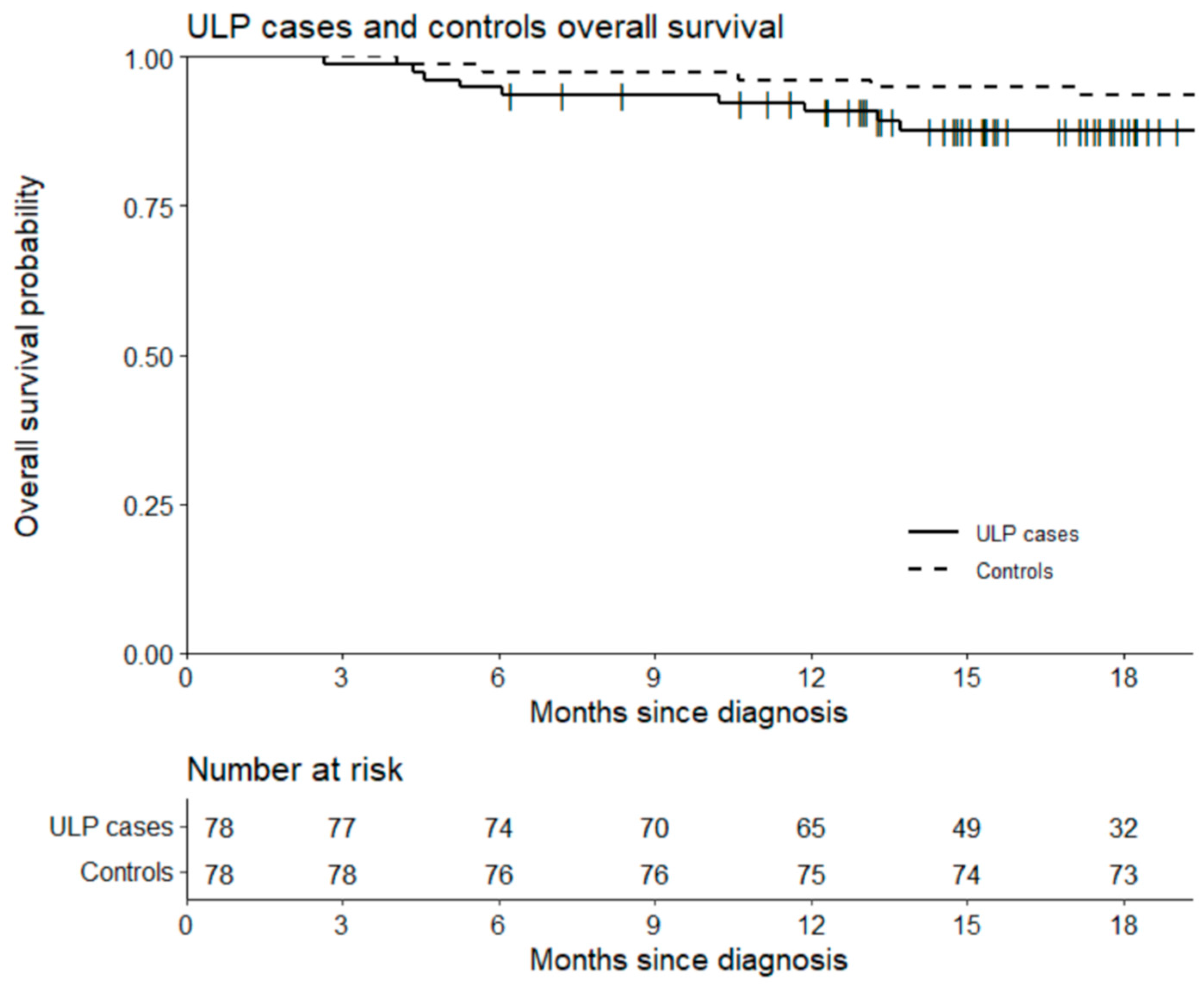
3.2. Clinical Impact
3.3. Economic Impact
3.4. Quality of Life and Satisfaction
3.4.1. Satisfaction
3.4.2. Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laurent, C.; Baron, M.; Amara, N.; Haioun, C.; Dandoit, M.; Maynadié, M.; Parrens, M.; Vergier, B.; Copie-Bergman, C.; Fabiani, B.; et al. Impact of Expert Pathologic Review of Lymphoma Diagnosis: Study of Patients From the French Lymphopath Network. J. Clin. Oncol. 2017, 35, 2008–2017. [Google Scholar] [CrossRef] [PubMed]
- Coiffier, B.; Lepage, E.; Brière, J.; Herbrecht, R.; Tilly, H.; Bouabdallah, R.; Morel, P.; Van Den Neste, E.; Salles, G.; Gaulard, P.; et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N. Engl. J. Med. 2002, 346, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Rossi, C.; Bastie, J.N. Actualités thérapeutiques dans les lymphomes non hodgkiniens et le lymphome de Hodgkin. Rev. Méd. Interne 2019, 40, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Le Gouill, S.; Thieblemont, C.; Oberic, L.; Moreau, A.; Bouabdallah, K.; Dartigeas, C.; Damaj, G.; Gastinne, T.; Ribrag, V.; Feugier, P.; et al. Rituximab after Autologous Stem-Cell Transplantation in Mantle-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 1250–1260. [Google Scholar] [CrossRef]
- Fitoussi, O.; Belhadj, K.; Mounier, N.; Parrens, M.; Tilly, H.; Salles, G.; Feugier, P.; Ferme, C.; Ysebaert, L.; Gabarre, J.; et al. Survival Impact of Rituximab Combined with ACVBP and Upfront Consolidation Autotransplantation in High-Risk Diffuse Large B-cell Lymphoma for GELA. Haematologica 2011, 96, 1136–1143. [Google Scholar] [CrossRef]
- Récher, C.; Coiffier, B.; Haioun, C.; Molina, T.J.; Fermé, C.; Casasnovas, O.; Thiéblemont, C.; Bosly, A.; Laurent, G.; Morschhauser, F.; et al. Intensified chemotherapy with ACVBP plus rituximab versus standard CHOP plus rituximab for the treatment of diffuse large B-cell lymphoma (LNH03-2B): An open-label randomised phase 3 trial. Lancet 2011, 378, 1858–1867. [Google Scholar] [CrossRef]
- Italiano, A.; Jardin, F.; Peyrade, F.; Saudes, L.; Tilly, H.; Thyss, A. Adapted CHOP plus rituximab in non-Hodgkin’s lymphoma in patients over 80 years old. Haematologica 2005, 90, 1281–1283. [Google Scholar]
- Peyrade, F.; Jardin, F.; Thieblemont, C.; Thyss, A.; Emile, J.F.; Castaigne, S.; Coiffier, B.; Haioun, C.; Bologna, S.; Fitoussi, O.; et al. Attenuated immunochemotherapy regimen (R-miniCHOP) in elderly patients older than 80 years with diffuse large B-cell lymphoma: A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2011, 12, 460–468. [Google Scholar] [CrossRef]
- André, M.P.E.; Girinsky, T.; Federico, M.; Reman, O.; Fortpied, C.; Gotti, M.; Casasnovas, O.; Brice, P.; Van der Maazen, R.; Re, A.; et al. Early Positron Emission Tomography Response-Adapted Treatment in Stage I and II Hodgkin Lymphoma: Final Results of the Randomized EORTC/LYSA/FIL H10 Trial. J. Clin. Oncol. 2017, 35, 1786–1794. [Google Scholar] [CrossRef]
- Skoetz, N.; Will, A.; Monsef, I.; Brillant, C.; Engert, A.; von Tresckow, B. Comparison of first-line chemotherapy including escalated BEACOPP versus chemotherapy including ABVD for people with early unfavourable or advanced stage Hodgkin lymphoma. Cochrane Database Syst. Rev. 2017, 5, CD007941. [Google Scholar] [CrossRef]
- Casasnovas, R.O.; Bouabdallah, R.; Brice, P.; Lazarovici, J.; Ghesquieres, H.; Stamatoullas, A.; Dupuis, J.; Gac, A.C.; Gastinne, T.; Joly, B.; et al. PET-adapted treatment for newly diagnosed advanced Hodgkin lymphoma (AHL2011): A randomised, multicentre, non-inferiority, phase 3 study. Lancet Oncol. 2019, 20, 202–215. [Google Scholar] [CrossRef]
- Trotman, J.; Barrington, S.F. The role of PET in first-line treatment of Hodgkin lymphoma. Lancet Haematol. 2021, 8, e67–e79. [Google Scholar] [CrossRef]
- Pettengell, R.; Schwenkglenks, M.; Bosly, A. Association of reduced relative dose intensity and survival in lymphoma patients receiving CHOP-21 chemotherapy. Ann. Hematol. 2008, 87, 429–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, H.; Hirakawa, T.; Inokuchi, K. Importance of Relative Dose Intensity in Chemotherapy for Diffuse Large B-cell Lymphoma. J. Clin. Exp. Hematop. 2011, 57, 1–5. Available online: https://pubmed.ncbi.nlm.nih.gov/21628854 (accessed on 28 May 2020). [CrossRef] [Green Version]
- De Grégori, J.; Pistre, P.; Boutet, M.; Porcher, L.; Devaux, M.; Pernot, C.; Chrétien, M.L.; Rossi, C.; Manfredi, S.; Dalac, S.; et al. Clinical and economic impact of pharmacist interventions in an ambulatory hematology-oncology department. J. Oncol. Pharm. Pract. 2020, 26, 1172–1179. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Resources. Common Terminology Criteria for Adverse Events (CTCAE); U.S. Department of Health and Human Resources: Washington, DC, USA, 2017; p. 147.
- Dalton, K.; Byrne, S. Role of the Pharmacist in Reducing Healthcare Costs: Current Insights. Integr. Pharm. Res. Pract. 2017, 6, 37–46. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC5774321 (accessed on 31 August 2020).
- Vo, T.H.; Bardet, J.D.; Charpiat, B.; Leyrissoux, C.; Gravoulet, J.; Allenet, B.; Conort, O.; Bedouch, P. Validation of a tool for reporting pharmacists’ interventions in everyday community pharmacy. J. Clin. Pharm. Ther. 2018, 43, 240–248. [Google Scholar] [CrossRef]
- Stämpfli, D.; Baumgartner, P.; Boeni, F.; Bedouch, P.; Lampert, M.L.; Hersberger, K.E. Translation and validation of a tool to assess the impact of clinical pharmacists’ interventions. Int. J. Clin. Pharm. 2019, 41, 56–64. [Google Scholar] [CrossRef]
- Vo, T.H.; Charpiat, B.; Chanoine, S.; Juste, M.; Roubille, R.; Rose, F.X.; Conort, O.; Allenet, B.; Bedouch, P.; Working Group “Valorization of Pharmacist Interventions”. Evaluation of the Potential Impact of Pharmacist Interventions: Development and Validation of the CLEO Multidimensional Tool; French Society of Clinical Pharmacy: Lyon, France, 2021; p. 254. [Google Scholar]
- Aapro, M.S.; Bohlius, J.; Cameron, D.A.; Dal Lago, L.; Donnelly, J.P.; Kearney, N.; Lyman, G.H.; Pettengell, R.; Tjan-Heijnen, V.C.; Walewski, J.; et al. 2010 update of EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur. J. Cancer 2011, 47, 8–32. [Google Scholar] [CrossRef]
- ASCO. Clinical Practice Guideline Update: Recommendations for the Use of White Blood Cell Growth Factors—The ASCO Post. Available online: https://www.ascopost.com/issues/november-10-2015/asco-clinical-practice-guideline-update-recommendations-for-the-use-of-white-blood-cell-growth-factors/ (accessed on 30 May 2020).
- Hryniuk, W.; Bush, H. The importance of dose intensity in chemotherapy of metastatic breast cancer. J. Clin. Oncol. 1984, 2, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Terada, Y.; Nakamae, H.; Aimoto, R.; Kanashima, H.; Sakamoto, E.; Aimoto, M.; Inoue, E.; Koh, H.; Nakane, T.; Takeoka, Y.; et al. Impact of relative dose intensity (RDI) in CHOP combined with rituximab (R-CHOP) on survival in diffuse large B-cell lymphoma. J. Exp. Clin. Cancer Res. 2009, 28, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyman, G.H.; Dale, D.C.; Friedberg, J.; Crawford, J.; Fisher, R.I. Incidence and predictors of low chemotherapy dose-intensity in aggressive non-Hodgkin’s lymphoma: A nationwide study. J. Clin. Oncol. 2004, 22, 4302–4311. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised Response Criteria for Malignant Lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef]
- Code de la Santé Publique—Article L710-6. Code de la Santé Publique. Available online: https://www.legifrance.gouv.fr/loda/article_lc/LEGIARTI000006694599/1994-10-11 (accessed on 28 May 2020).
- EORTC. Quality of Life Website. Available online: https://qol.eortc.org/ (accessed on 30 May 2020).
- Husson, O.; de Rooij, B.H.; Kieffer, J.; Oerlemans, S.; Mols, F.; Aaronson, N.K.; Van der Graaf, W.T.A.; Van de Poll-Franse, L.K. The EORTC QLQ-C30 Summary Score as Prognostic Factor for Survival of Patients with Cancer in the “Real-World”: Results from the Population-Based PROFILES Registry. Oncologist 2020, 25, e722–e732. [Google Scholar] [CrossRef] [Green Version]
- Osoba, D.; Rodrigues, G.; Myles, J.; Zee, B.; Pater, J. Interpreting the significance of changes in health-related quality-of-life scores. J. Clin. Oncol. 1998, 16, 139–144. [Google Scholar] [CrossRef]
- Borel, C.; Lamy, S.; Compaci, G.; Récher, C.; Jeanneau, P.; Nogaro, J.C.; Bauvin, E.; Despas, F.; Delpierre, C.; Laurent, G. A longitudinal study of non-medical determinants of adherence to R-CHOP therapy for diffuse large B-cell lymphoma: Implication for survival. BMC Cancer 2015, 15, 288. [Google Scholar] [CrossRef] [Green Version]
- Russo, F.; Svanera, G.; Cioppa, P.D.; Corazzelli, G.; Frigeri, F.; Capobianco, G.; LaStoria, S.; Pinto, A. The Impact of Relative Dose Intensity on Response and Survival in a Series of 180 Newly Diagnosed Patients with Hodgkin’s Lymphoma. Blood 2005, 106, 2671. [Google Scholar] [CrossRef]
- Bosly, A.; Bron, D.; Van Hoof, A.; De Bock, R.; Berneman, Z.; Ferrant, A.; Kaufman, L.; Dauwe, M.; Verhoef, G. Achievement of optimal average relative dose intensity and correlation with survival in diffuse large B-cell lymphoma patients treated with CHOP. Ann. Hematol. 2008, 87, 277–283. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All | HL | NHL | NHL Subtypes | |||
|---|---|---|---|---|---|---|---|
| DLBCL | FL | MCL | Others | ||||
| Total number of patients | 114 | 19 | 95 | 55 (58) | 17 (18) | 12 (13) | 11 (12) |
| Age (years) Median [Min-Max] | 66 [22–92] | 34 [21–83] | 69 [36–92] | 70 [36–92] | 62 [45–86] | 70 [44–77] | 59 [39–82] |
| Body surface area (m2) Median [Min-Max] | 1.8 [1.3–2.2] | 1.7 [1.36–2.2] | 1.8 [1.3–2.2] | 1.8 [1.3–2.2] | 1.8 [1.5–2] | 1.9 [1.6–2] | 1.8 [1.5–2] |
| Gender n (%) | |||||||
| Male | 64 (56) | 10 (53) | 54 (57) | 29 (53) | 10 (59) | 8 (67) | 7 (64) |
| Female | 50 (44) | 9 (47) | 41 (43) | 26 (47) | 7 (41) | 4 (33) | 4 (36) |
| Ann Arbor stage n (%) | |||||||
| I–II | 25 (22) | 12 (63) | 13 (14) | 10 (18) | 1 (6) | 0 | 2 (18) |
| III–IV | 89 (78) | 7 (37) | 82 (86) | 45 (82) | 16 (94) | 12 (100) | 9 (82) |
| Performance status (ECOG) n (%) | |||||||
| 0–1 | 90 (80) | 16 (84) | 74 (79) | 41 (75) | 14 (88) | 11 (92) | 8 (73) |
| 2–4 | 23 (20) | 3 (16) | 20 (21) | 14 (25) | 2 (12) | 1 (8) | 3 (27) |
| Age adjusted IPI n (%) | - | ||||||
| 0–1 | 32 (55) | - | 32 (55) | 30 (55) | - | - | 2 (67) |
| 2–3 | 26 (45) | 26 (45) | 25 (45) | - | - | 1 (33) | |
| Occupational status n (%) | |||||||
| Active | 6 (5) | 4 (21) | 2 (2) | 2 (4) | 0 | 0 | 0 |
| Inactive/jobless | 34 (30) | 11 (58) | 23 (24) | 8 (15) | 6 (35) | 3 (25) | 6 (55) |
| Retired | 74 (65) | 4 (21) | 70 (74) | 45 (82) | 11 (65) | 9 (75) | 5 (45) |
| Treatment regimens n (%) | |||||||
| R-CHOP | 59 (52) | 0 | 59 (62) | 36 (65) | 13 (76) | 8 (67) | 2 (18) |
| R-miniCHOP | 13 (11) | 0 | 13 (14) | 10 (18) | 3 (18) | 0 | 0 |
| R-ACVBP | 8 (7) | 0 | 8 (8) | 6 (11) | 0 | 0 | 2 (18) |
| BEACOPP | 5 (4) | 5 (26) | 0 | 0 | 0 | 0 | 0 |
| ABVD | 10 (9) | 10 (53) | 0 | 0 | 0 | 0 | 0 |
| Others | 19 (17) | 4 (21) | 15 (16) | 3 (5) | 1 (6) | 4 (33) | 7 (64) |
| Characteristics | Cases | Controls |
|---|---|---|
| Total number of patients | 78 | 78 |
| Lymphoma type | ||
| HL | 12 | 12 |
| NHL | 66 | 66 |
| DLBCL | 42 | 42 |
| FL | 12 | 12 |
| MCL | 10 | 10 |
| Others | 2 | 2 |
| Age (years) Median [Min-Max] | 65 [22–89] | 64 [22–96] |
| Body surface area (m2) Median [Min-Max] | 1.83 [1.4–2.2] | [1.3–2.2] |
| Gender n (%) | ||
| Male | 44 (56) | 40 (51) |
| Female | 34 (44) | 38 (49) |
| Ann Arbor stage n (%) | ||
| I–II | 28 (36) | 34 (44) |
| III–IV | 50 (64) | 44 (56) |
| Performance status (ECOG) n (%) | ||
| 0–1 | 65 (83) | 67 (86) |
| 2–4 | 13 (17) | 11 (14) |
| Age adjusted IPI n (%) | ||
| 0–1 | 23 (55) | 23 (55) |
| 2–3 | 19 (45) | 19 (45) |
| Occupational status n (%) | ||
| Active | 23 (30) | 29 (37) |
| Inactive/jobless | 5 (6) | 2 (3) |
| Retired | 50 (64) | 47 (60) |
| Treatment regimens n (%) | ||
| R-CHOP | 47 (60) | 48 (62) |
| R-miniCHOP | 7 (9) | 6 (8) |
| R-ACVBP | 6 (8) | 6 (8) |
| BEACOPP | 3 (4) | 3 (4) |
| ABVD | 7 (9) | 7 (9) |
| Others | 8 (10) | 8 (10) |
| Drug Related Problem (According to FSCP) | n (%) | PI (According to FSCP) | n (%) | ||
|---|---|---|---|---|---|
| PI category n = 300 | PI with prescribers (PIpr) n = 115 (38%) | Contra-indication/non-conformity to guidelines Drug or medical device not received by the patient Dosage problem (under or over dosage) Unjustified drug prescription Drug interaction Adverse drug reaction Improper prescription Drug omission Monitoring Therapeutic redundancy Pharmacodependence | 15 (13) 41 (36) 19 (17) 10 (9) 4 (3) 1 (1) 15 (13) 4 (3) 6 (5) 0 0 | Addition of a new drug Discontinuation or refusal to deliver Drug switch Choice of administration route Drug monitoring Optimisation of the dispensing/administration mode Dose adjustment | 45 (39) 30 (26) 01 (1) 4 (3) 8 (7) 27 (23) |
| PI with patients (PIpa) n = 185 (62%) | Improper prescription | 185 (100) | Optimisation of the dispensing/administration mode | 185 (100) | |
| Clinical Impact of PI n = 300 | Clinical impact of PI (according to CLEO) n (%) | ||||
| Harmful Null Minor Moderate Major Lethal Non determined | 0 2 (1) 219 (73) 63 (21) 16 (5) 0 0 | ||||
| Cases (n = 78) | Controls (n = 78) | p Value | |||||
|---|---|---|---|---|---|---|---|
| Adverse Events | All | Grade 1–2 | Grade 3–4 | All | Grade 1–2 | Grade 3–4 | |
| Anaemia | 77 (99) | 65 (83) | 12 (15) | 76 (97) | 62 (79) | 14 (18) | 0.672 |
| Thrombocytopenia | 59 (76) | 45 (58) | 14 (18) | 48 (61) | 32 (41) | 16 (21) | 0.288 |
| Neutropenia | 77 (99) | 2 (3) | 75 (96) | 78 (100) | 1 (1) | 77 (99) | 0.620 |
| Febrile neutropenia | 10 (13) | 0 | 10 (13) | 11 (14) | 1 (1) | 10 (13) | 0.524 |
| Infection without neutropenia | 27 (35) | 22 (28) | 5 (6) | 25 (32) | 13 (17) | 12 (15) | 0.038 |
| Diarrhea | 18 (23) | 17 (22) | 1 (1) | 9 (12) | 9 (12) | 0 | 0.667 |
| Constipation | 34 (44) | 33 (42) | 1 (1) | 21 (27) | 21 (27) | 0 | 0.618 |
| Haemorrhoids | 16 (21) | 16 (21) | 0 | 7 (9) | 7 (9) | 0 | - |
| Mucositis | 22 (28) | 19 (24) | 3 (4) | 17 (22) | 14 (18) | 3 (4) | 0.535 |
| Neuropathy | 31 (40) | 31 (40) | 0 | 18 (23) | 18 (23) | 0 | - |
| Pruritus/eruption | 13 (17) | 13 (17) | 0 | 8 (10) | 8 (10) | 0 | - |
| Pulmonary disorders (cough/dyspnea) | 18 (23) | 18 (23) | 0 | 4 (5) | 4 (5) | 0 | - |
| Cases (n = 78) | Controls (n = 78) | p Value | |
|---|---|---|---|
| Number of GCSF injection (total) | 1007 | 949 | |
| Patient receiving GCSF, n (%) | 74 (95) | 72 (92) | 0.746 |
| Patient receiving ASE, n (%) | 31 (40) | 11 (14) | 0.001 |
| Transfusions (total) | 140 | 157 | |
| Transfused patient, n (%) | 31 (40) | 34 (44) | 0.745 |
| Re-hospitalised patients | 35 (45) | 37 (47) | 0.872 |
| Re-hospitalisation (total) | 76 | 88 | |
| Outpatient department, n (%) | 54 (71) | 53 (60) | 0.217 |
| Hospitalisation, n (%) | 22 (29) | 34 (39) | |
| Intensive care unit, n (%) | 0 | 1 (1) | |
| Re-hospitalisation cause | |||
| Febrile neutropenia/Infection, n (%) | 17 (22) | 29 (33) | 0.179 |
| Blood transfusions, n (%) | 51 (67) | 42 (48) | |
| ARDI | |||
| <85%, n (%) | 6 (8) | 13 (18) | 0.138 |
| >85%, n (%) | 67 (92) | 60 (82) | |
| Delayed treatment (>7 days), n (%) | 23 (32) | 24 (33) | 1 |
| Questions n (%) | I Fully Agree | Moderately Agree | Disagree at All | Not Answered |
|---|---|---|---|---|
| Have regular phone calls reassured you, put you at ease? | 80 (99) | 1 (1) | 0 | 0 |
| Did the rhythm of the calls match to the difficulties related to the side effect you experienced? | 72 (89) | 8 (10) | 0 | 1 (1) |
| Much better than expected | As much as expected | A little less than expected | Not answered | |
| Did the listening and the time spent meet to your needs and expectations? | 52 (64) | 29 (36) | 0 | 0 |
| Were the given answers adapted to your needs? | 47 (58) | 33 (41) | 1 (1) | 0 |
| Very important | Quite important | Little important | Not answered | |
| Was it important for you to be assisted by a health professional in your care pathway (contact, telephone, advice, etc)? | 70 (86) | 11 (14) | 0 | 0 |
| Very satisfied | Satisfied | Unsatisfied | Not answered | |
| Are you satisfied with the explanations given by the pharmacist about treatment and their adverse drug effect? | 53 (65) | 24 (30) | 2 (2) | 2 (2) |
| Are you satisfied with the answers given by the pharmacist to your questions? | 53 (65) | 25 (31) | 2 (2) | 1 (1) |
| Are you satisfied with the written information you received (personalised pharmaceutical plan)? | 46 (57) | 32 (40) | 2 (2) | 1 (1) |
| Yes | No | Not answered | ||
| Has all the support provided by the various people involved (doctor, nurse, pharmacist) helped you to better understand your treatment? | 79 (98) | 2 (2) | 0 | |
| Would you recommend this type of phone follow-up to one of your relative? | 79 (98) | 2 (2) | 0 | |
| In the meantime, between phone appointments, have you encountered any difficulties in contacting the nurse? | 7 (9) | 74 (91) | 0 |
| Score | ||||
|---|---|---|---|---|
| Items | Visit | Mean | Evolution | p Value |
| Global health status | Before | 64.0 | 3.3 | 0.298 |
| After | 67.3 | |||
| Physical functioning | Before | 74.7 | 3.3 | 0.514 |
| After | 78.0 | |||
| Role functioning | Before | 69.5 | 12.1 | 0.077 |
| After | 81.6 | |||
| Emotional functioning | Before | 63.1 | 4.2 | 0.241 |
| After | 67.3 | |||
| Cognitive functioning | Before | 81.6 | 2.3 | 0.271 |
| After | 83.9 | |||
| Social functioning | Before | 71.0 | 0.6 | 0.975 |
| After | 71.6 | |||
| Fatigue | Before | 48.3 | −8.8 | 0.161 |
| After | 39.5 | |||
| Nausea and Vomiting | Before | 7.5 | −1.7 | 0.590 |
| After | 5.7 | |||
| Pain | Before | 29.9 | −9.2 | 0.182 |
| After | 20.7 | |||
| Dyspnea | Before | 20.7 | 6.9 | 0.277 |
| After | 27.6 | |||
| Insomnia | Before | 43.7 | −5.7 | 0.537 |
| After | 37.9 | |||
| Appetite Loss | Before | 25.3 | −8.0 | 0.300 |
| After | 17.2 | |||
| Constipation | Before | 29.9 | −3.4 | 0.912 |
| After | 26.4 | |||
| Diarrhoea | Before | 20.7 | −8.0 | 0.137 |
| After | 12.6 | |||
| Financial Difficulties | Before | 11.1 | −3.7 | 0.416 |
| After | 7.4 | |||
| QLQ-C30 Summary Score | Before | 72.2 | 5.1 | 0.199 |
| After | 77.3 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devaux, M.; Boulin, M.; Mounier, M.; Caillot, D.; Ahwij, N.; Herbin, A.; Bastie, J.N.; Favennec, C.; Robert, P.; Pistre, P.; et al. Clinical and Economic Impact of a Multidisciplinary Follow-Up Program in Lymphoma Patients. Cancers 2022, 14, 2532. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102532
Devaux M, Boulin M, Mounier M, Caillot D, Ahwij N, Herbin A, Bastie JN, Favennec C, Robert P, Pistre P, et al. Clinical and Economic Impact of a Multidisciplinary Follow-Up Program in Lymphoma Patients. Cancers. 2022; 14(10):2532. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102532
Chicago/Turabian StyleDevaux, Madeline, Mathieu Boulin, Morgane Mounier, Denis Caillot, Nuri Ahwij, Adélie Herbin, Jean Noël Bastie, Camille Favennec, Philippine Robert, Pauline Pistre, and et al. 2022. "Clinical and Economic Impact of a Multidisciplinary Follow-Up Program in Lymphoma Patients" Cancers 14, no. 10: 2532. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102532