
Association of Diabetes Severity and Mortality with Lung Squamous Cell Carcinoma
by
 , and
, and
Chih-Hsiung Su
1,†, 
Wan-Ming Chen
2,3,†,
Mingchih Chen
2,
Ben-Chang Shia
2,3 and
Szu-Yuan Wu
2,3,4,5,6,7,8,9,10,* 1
Department of Accounting Information, Chihlee University of Technology, Taipei 22050, Taiwan
2
Graduate Institute of Business Administration, College of Management, Fu Jen Catholic University, Taipei 24205, Taiwan
3
Artificial Intelligence Development Center, Fu Jen Catholic University, Taipei 24205, Taiwan
4
Department of Food Nutrition and Health Biotechnology, College of Medical and Health Science, Asia University, Taichung 41354, Taiwan
5
Division of Radiation Oncology, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan 265501, Taiwan
6
Big Data Center, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan 265501, Taiwan
7
Department of Healthcare Administration, College of Medical and Health Science, Asia University, Taichung 41354, Taiwan
8
Cancer Center, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan 265501, Taiwan
9
Centers for Regional Anesthesia and Pain Medicine, Taipei Municipal Wan Fang Hospital, Taipei Medical University, Taipei 110301, Taiwan
10
Department of Management, College of Management, Fo Guang University, Yilan 26247, Taiwan
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Cancers 2022, 14(10), 2553; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102553
Submission received: 2 May 2022
/
Revised: 17 May 2022
/
Accepted: 21 May 2022
/
Published: 22 May 2022
(This article belongs to the Special Issue Advances in Lung Cancer Therapy)
Abstract
:Simple Summary
The survival impact of diabetes severity on lung cancer survival remains unclear. We performed head-to-head propensity score matching to estimate the survival impact of various adapted diabetes complications severity index (aDCSI) scores in patients with both diabetes and lung squamous cell carcinoma (SqCLC). The results indicated that diabetes severity (aDCSI ≥ 2) is an independent prognostic factor for the overall survival of patients with both diabetes and lung SqCLC who receive standard treatments. Prevention of diabetes progression is necessary for patients with diabetes; it affects not only diabetes control but also improves survival for patients with lung SqCLC.
Abstract
Purpose: The survival impact of diabetes severity on lung cancer remains unclear. We performed head-to-head propensity score matching to estimate the survival impact of various adapted diabetes complications severity index (aDCSI) scores in patients with both diabetes and lung squamous cell carcinoma (SqCLC). Patients and Methods: We enrolled patients with both diabetes and lung SqCLC and categorized them into the mild (aDCSI = 0–1) and moderate-to-severe (aDCSI ≥ 2) diabetes groups. The patients in both groups were matched at a 1:1 ratio. Results: the matching process yielded a final cohort of 5742 patients with both diabetes and lung SqCLC (2871 patients in the mild diabetes group and 2871 patients in the moderate-to-severe diabetes groups) who were eligible for further analysis. A multivariate Cox regression analysis revealed that the adjusted hazard ratio (aHR; 95% confidence interval) of all-cause death for the mild diabetes group relative to the moderate-to-severe diabetes group was 1.17 (1.08–1.28; p = 0.0005). Conclusion: severe diabetes (aDCSI ≥ 2) is an independent prognostic factor for OS among patients with both diabetes and lung SqCLC who receive standard treatments. Preventing diabetes progression is necessary for patients with diabetes because it not only supports diabetes control but also improves survival for patients with lung SqCLC.
1. Introduction
Having a high blood sugar level can damage various organ systems, especially the cardiovascular and nervous systems [1,2]. Diabetes can lead to cardiovascular disease, nephropathy, retinopathy, peripheral vascular disease, stroke, neuropathy, and metabolic complications [2]. Recent studies have verified that diabetes is linked to dementia, hearing loss, and specific forms of cancer [3,4,5]. Diabetes is associated with increased incidence and mortality in numerous types of cancer [6,7,8], and it may influence cancer progression and outcomes [9]. In addition, diabetes mellitus is a risk factor for all-cause death in patients with cancer [9].
Lung cancer is the leading and second leading cause of cancer death worldwide in men and women, respectively [10]. Diabetes may increase the risk of lung cancer, and it is associated with poor overall survival (OS) among women with lung cancer [11]. The potential mechanisms of poor survival in patients with both diabetes and lung cancer can be attributed to hyperinsulinemia and hyperglycemia with poor diabetes control and the occurrence of diabetic complications, which contribute to lung cancer progression and poorer survival outcomes among such patients [11]. Nevertheless, no study has produced clinical evidence to demonstrate the association of diabetes severity with the survival outcomes of lung cancer.
The adapted Diabetes Complications Severity Index (aDCSI) is used to assess diabetes severity for the purpose of predicting mortality rates, hospitalization rates, and medical costs [12]. However, the survival impact of diabetes severity on lung cancer remains unclear. In the current study, we performed head-to-head propensity score matching (PSM) to estimate the survival impact of various aDCSI scores among patients with both diabetes and lung squamous cell carcinoma (SqCLC). We focused on lung SqCLC because of the lack of heterogeneous treatments and the absence of evidence regarding the contribution of specific driver gene mutations to improved or poorer survival. Information on the association of diabetes severity with survival outcomes for lung SqCLC can serve as a valuable reference for health authorities, particularly in terms of the formulation of health policies aimed at preventing diabetes progression and improving survival in patients with lung SqCLC. Our findings help to clarify why patients who have similar clinical lung cancer stages and receive similar treatments exhibit different survival outcomes.
2. Patients and Methods
2.1. Data Sources and Study Cohort
From the Taiwan Cancer Registry database, we identified patients with mild diabetes or moderate-to-severe diabetes who received a diagnosis of lung SqCLC between 1 January 2008 and 31 December 2018. Patients were classified as having mild diabetes and moderate-to-severe diabetes if they had aDCSI scores of 0–1 and ≥2, respectively, during the 3 months following the date of a lung cancer diagnosis [2,12]. The aDCSI is a good measure of diabetes severity [13]. The complications severity index was categorized into 2 or 3 levels (no abnormality = 0, some abnormality = 1, and severe abnormality = 2), depending on the presence and severity of the complication. If no abnormalities were present, the patient received no score for that complication. If a patient had any complication classified as some abnormality, a 1 was added to the DCSI. If patients had any complication classified as severe abnormality, a 2 was added (Table S1) [2]. Due to severe abnormality, a 2 was added [2], we compared the OS between SqCLC patients with aDCSI scores of 0–1 and those with aDCSI scores of ≥2. The index date was the date of lung cancer diagnosis, and the follow-up duration was from the index date to 31 December 2019. The study protocols were reviewed and approved by the Institutional Review Board of Tzu-Chi Medical Foundation (IRB109-015-B). Furthermore, we used data from the cancer registry database of the Collaboration Center of Health Information Application, which archives cancer-related information regarding pathological types, cancer stages, and treatments [14,15,16,17]. The vital status and the cause of death of each patient were verified.
2.2. Patient Selection
Inclusion and Exclusion Criteria
Patients with diabetes were included if they were diagnosed as having lung SqCLC on the basis of pathological reports; were aged ≥20 years; and had lung SqCLC (stages I–IIIC) without metastasis as defined by the American Joint Committee on Cancer (AJCC, 8th edition). Patients with diabetes were excluded if they had a history of cancer before receiving their diagnosis of lung SqCLC, had distant metastasis, had lung cancer of an unknown pathological type, had missing data for sex, were aged <20 years, had unclear staging, or exhibited a non-SqCLC histology. In addition, we excluded patients with lung SqCLC if they did not receive surgery for stages I and II cancer, underwent concurrent chemoradiotherapy (CCRT) for stage III cancer after receiving their lung SqCLC diagnosis, received insufficient chemotherapy (concurrent chemotherapy comprising two agents with at least one containing platinum), or did not receive a platinum-based chemotherapy regimen. We also excluded patients who received only sequential chemotherapy and radiation therapy (RT), chemotherapy alone, or RT alone. Standard CCRT comprises concurrent chemotherapy with 2 agents containing platinum and thoracic RT with 6000 cGy administered in daily fractions [18,19,20].
2.3. PSM and Covariates
After adjustments were made for confounders, we used a time-dependent Cox proportional hazards model to calculate the time from the index date to all-cause death for patients with both lung SqCLC and mild or moderate-to-severe diabetes. To reduce the effects of potential confounders on the comparison of all-cause death between the mild and moderate-to-severe diabetes groups (which comprised patients with both diabetes and lung SqCLC), the patients included in the current study were propensity-score matched. The variables used for matching were sex, age, AJCC clinical stage, income level, urbanization, Charlson comorbidity index (CCI) score, comorbidities (for example, chronic obstructive pulmonary disease [COPD], chronic bronchitis, emphysema, acute upper respiratory tract infection, asthma, pneumoconiosis, cardiovascular diseases, acute myocardial infarction [AMI], stroke, tuberculosis [TB], obesity), current smoking habit, alcohol-related disease, and diabetes duration (1–1.99, 2–2.99, 3–3.99, 4–4.99, and ≥5 years) (Table 1). Repeated comorbidities were excluded from CCI scores to prevent repetitive adjustments in the multivariate analysis of the current study. Comorbidities were determined in accordance with the ICD-9-CM or ICD-10-CM codes in the main inpatient diagnosis records of a patient or if a patient made ≥2 outpatient visits within 1 year. Comorbidities that presented within the 6 months preceding the index date were recorded. Continuous variables are presented as means ± standard deviations or medians (first and third quartiles), where appropriate. We matched patients at a ratio of 1:1 by using the greedy method; sex, age, AJCC clinical stage, income level, urbanization, CCI score, comorbidities, current smoking habit, alcohol-related disease, and diabetes duration were propensity-score matched within a caliper of 0.2 [21]. Matching is a common technique for selecting controls with identical background covariates as study participants; investigators perform matching when it is necessary to control for and minimize the differences among study participants. In the current study, multivariate Cox regression analysis was performed to calculate hazard ratios with 95% confidence intervals (CIs) to determine whether the variables listed in Table 1 are the potential independent predictors of all-cause death.
2.4. Sensitivity Analysis
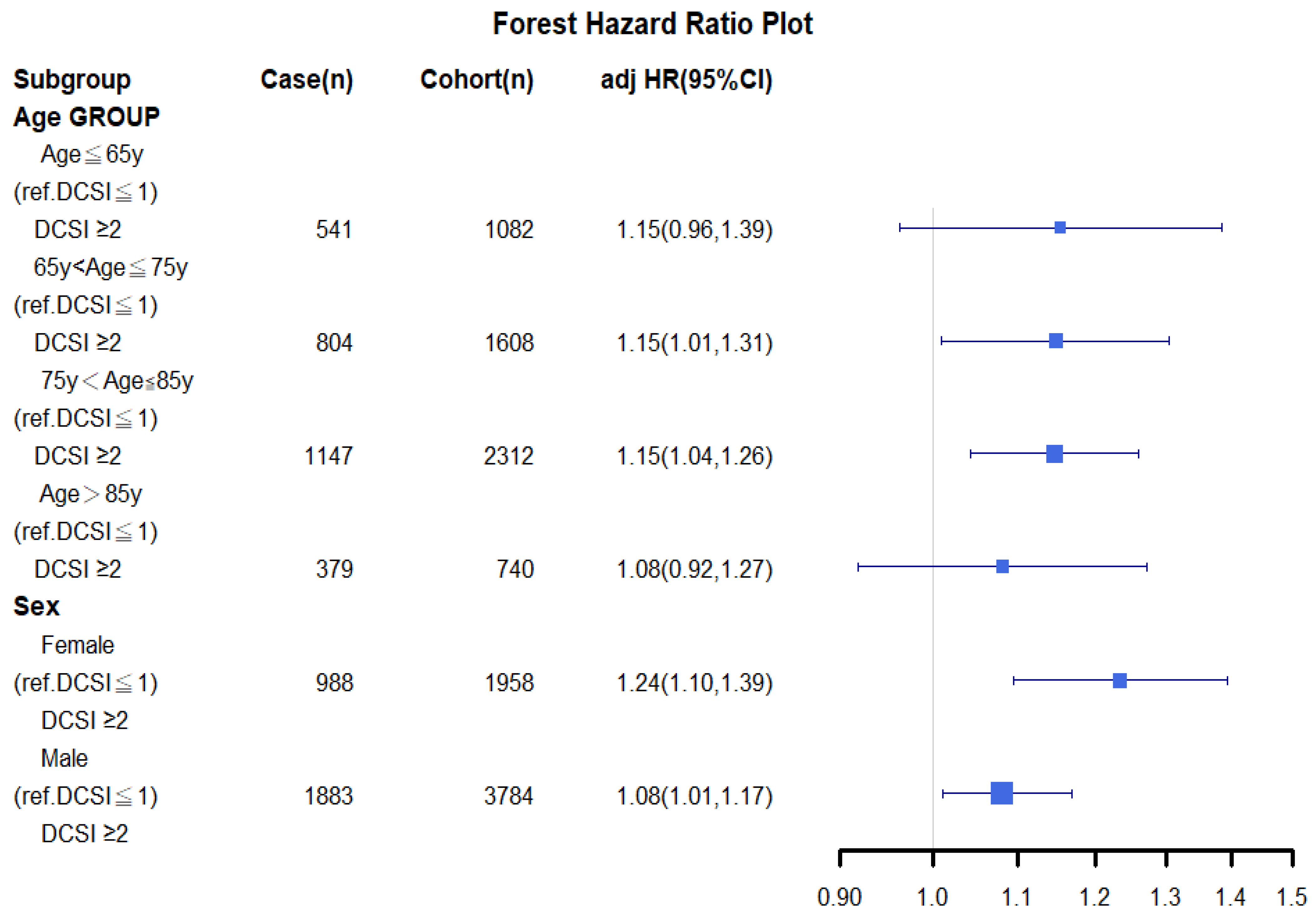
A sensitivity analysis of various cancer types was conducted using inverse probability of treatment weighting (IPTW) for all-cause death in propensity score–matched mild and moderate-to-severe diabetes groups; it was conducted to clarify the association of mortality with diabetes severity among patients stratified by age, sex, and clinical stage (Figure 1). All of the analyses were adjusted for the covariates in Table 2.
2.5. Statistical Analysis
All of the analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). The matching procedure was implemented using PROC PSMATCH in SAS [22]. In a two-tailed Wald test, p < 0.05 was regarded as significant. OS was estimated using the Kaplan–Meier method, and differences between the mild and moderate-to-severe diabetes groups with lung SqCLC were determined by performing a stratified log-rank test and subsequently comparing the survival curves (stratified according to matched sets) [23].
3. Results
3.1. PSM and Study Cohort
PSM yielded a final cohort of 5742 patients with lung SqCLC (2871 patients in the mild diabetes group [aDCSI = 0–1] and 2871 patients in the moderate-to-severe diabetes group [aDCSI ≥ 2]) who were eligible for further analysis; their characteristics are listed in Table 1. Age distribution was balanced between the two groups (Table 1). Furthermore, after head-to-head PSM was performed, no significant differences in sex, age, AJCC clinical stage, income level, urbanization, CCI score, comorbidities, current smoking habit, alcohol-related disease, and diabetes duration were observed between the two groups. All-cause death, the primary endpoint, significantly differed between the patients with lung SqCLC in the moderate-to-severe diabetes group and the patients with lung SqCLC in the mild diabetes group (p < 0.001; Table 1). Due to the high collinearity of diabetes severity, use of diabetic medications and number of diabetic medications taken were unmatched; adjustments were made for these variables in the multivariable Cox model. Table 1 reveals that relative to the patients in the mild diabetes group, the patients in the moderate-to-severe diabetes group took a significantly higher number of diabetic medications and were prescribed diabetic medications at a significantly higher frequency.
3.2. Prognostic Factors for All-Cause Death of Lung SqCLC after Multivariate Cox Regression Analysis
The results of a multivariate Cox regression analysis indicated that the patients with lung SqCLC and moderate-to-severe diabetes had a significantly shorter OS (Table 2) relative to the patients with lung SqCLC and mild diabetes. Except for older age (>65 years), male sex, and an aDCSI score of ≥2, no other significant differences were observed for explanatory variables. In the multivariate Cox regression analysis, the adjusted hazard ratio (aHR; 95% CI) of all-cause mortality for the patients with lung SqCLC and mild diabetes relative to the patients with lung SqCLC and moderate-to-severe diabetes was 1.17 (1.08–1.28; p = 0.0005). The aHRs (95% CIs) of all-cause mortality for the patients aged 66–75 years, 76–85 years, and >85 years (relative to the patients aged ≤65 years) were 1.33 (1.13–1.57), 2.03 (1.76–2.37), and 3.12 (2.60–3.71), respectively (Table 2). The aHR (95% CI) of all-cause mortality for the male patients with lung SqCLC relative to the female patients with lung SqCLC was 1.19 (1.10–1.34).
3.3. Sensitivity Analysis of All-Cause Mortality for Lung SqCLC between Mild and Moderate-to-Severe Diabetes Groups (Stratified by Sex and Age)
A stratified analysis of distinct groups stratified by age and sex on the basis of IPTW was performed, and the results are presented as a forest plot in Figure 1. Among the patients with lung SqCLC and moderate-to-severe diabetes, those aged <65 years, 65–74 years, 75–85 years, and >85 years had aHRs (95% CIs) of 1.15 (0.96–1.39), 1.15 (1.01–1.31), 1.15 (1.04–1.26), and 1.08 (0.92–1.27), respectively, indicating a significantly higher risk of mortality relative to the patients with lung SqCLC and mild diabetes for all age groups (Figure 1). Furthermore, among the patients with lung SqCLC and moderate-to-severe diabetes, female and male patients had aHRs (95% CI) of 1.24 (1.10–1.30) and 1.08 (1.01–1.17), respectively, for all-cause mortality relative to the patients with lung SqCLC and mild diabetes.
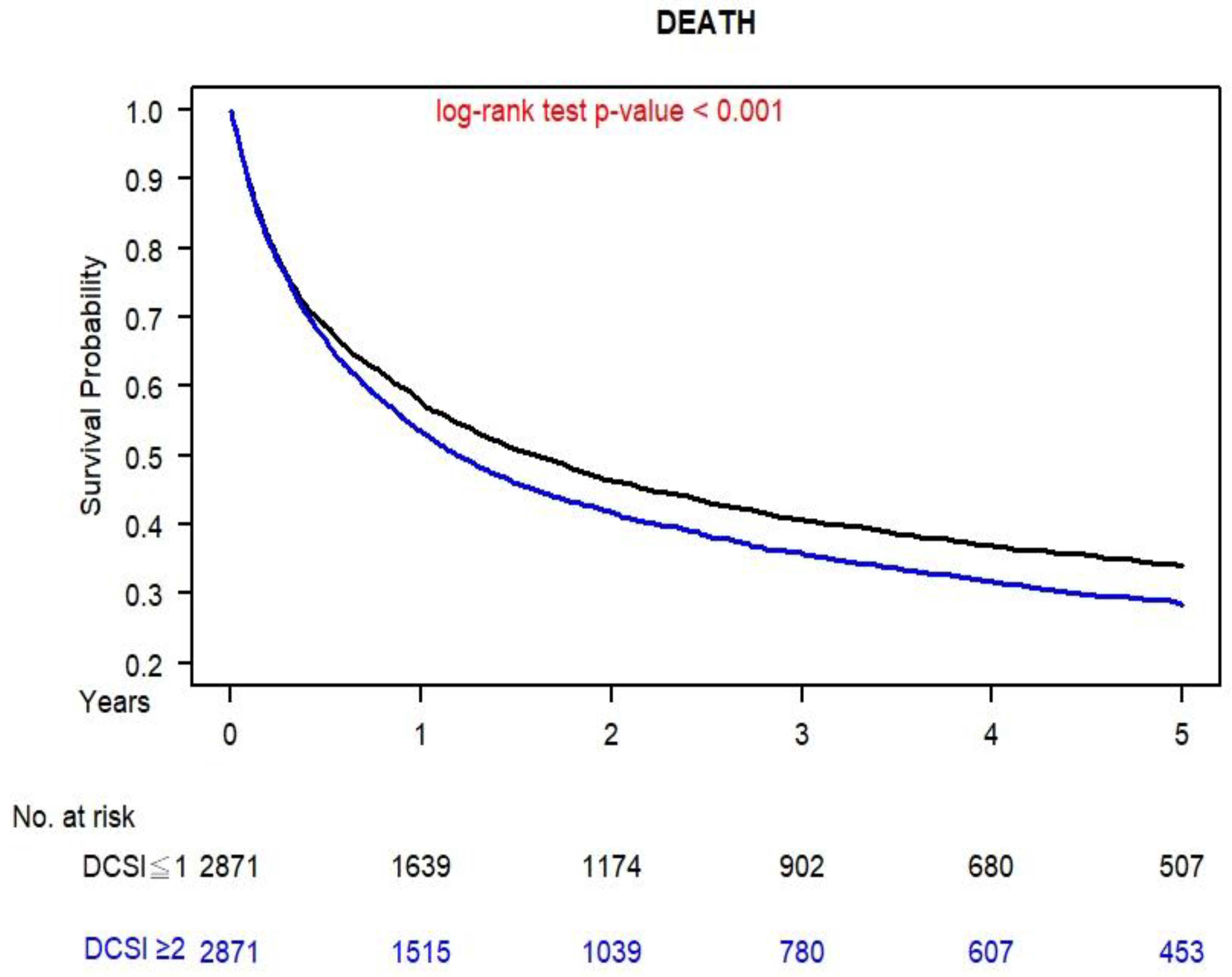
3.4. Kaplan–Meier Survival Curve of Mild and Moderate-to-Severe Diabetes Groups for of Lung SqCLC
Figure 2 presents the OS curves for the propensity score–matched patients with lung SqCLC and mild or moderate-to-severe diabetes; the curves were obtained using the Kaplan–Meier method. The 5-year OS for the patients with moderate-to-severe diabetes and those with mild diabetes were 40.12% and 32.94%, respectively (p < 0.001).
4. Discussion
Studies have reported that patients with both lung cancer and diabetes have a poorer survival rate than those with lung cancer but without diabetes [11,24,25,26]; this is especially true for women [11]. However, no clear data have been obtained with respect to the clinical stages of lung cancer and the types of lung cancer (SqCLC, adenocarcinoma, small cell carcinoma, and large cell carcinoma) [11,24,25,26]. Survival and treatments administered differ for distinct types of lung cancer [27], especially those involving driver gene mutations such as epidermal growth factor receptor mutation in lung adenocarcinoma [28,29]. Therefore, we focused on lung SqCLC, for which consistent treatments are administered for each stage, and no driver gene mutations are involved. Studies have indicated that diabetes is a poor prognostic factor of OS for lung cancer [11,24,25,26], but no evidence has been produced to demonstrate the association of diabetes severity with lung cancer survival. In our study, we conducted head-to-head PSM to mimic a randomized controlled trial (RCT) and estimate the survival impact of diabetes severity (aDCSI of 0–1 or ≥2) on lung SqCLC. Our large-scale study is the first to demonstrate that moderate-to-severe diabetes (aDCSI ≥ 2) can result in poor OS in patients with lung SqCLC who are receiving standard treatments (regardless of age and sex).
Diabetes can influence lung cancer progression and outcome through several mechanisms, including hyperglycemia, hyperinsulinemia, metabolic dysregulation in cancer cells, and chronic inflammation, all of which are associated with cell proliferation and cancer progression [30,31]. Elevated insulin levels, which represent insulin resistance, can promote cancer through the insulin-like growth factor-1 (IGF-1) pathway [32]. The IGF-1 pathway is regarded as a key promoter of tumor progression [33,34], and IGF-1 receptor inhibitors can contribute to cancer therapy [35,36]. In addition, hyperglycemia and metabolic dysregulation in cancer cells may accelerate the proliferation of lung cancer cells through epidermal growth factor expression, the reversal of the Warburg effect, and the reactivation of oxidative phosphorylation [37,38,39]. Furthermore, patients with both lung cancer and moderate-to-severe diabetes may receive fewer standard treatments for lung cancer relative to patients with only lung cancer because of the greater risk of chemotherapy-related toxicity [40]. At the time of writing, studies on mortality outcomes for individuals with both lung cancer and diabetes have produced conflicting results [41,42,43,44]. These conflicting data may be related to the survival impact of diabetes severity in patients with lung cancer, which can be attributed to the decision-making associated with cancer treatments, tumor response, and poor diabetes control combined with cancer progression [37,38,39,41,42,43,44]. Collectively, the aforementioned findings indicate that moderate-to-severe diabetes is proportionally related to the poor control of hyperglycemia, hyperinsulinemia, or chronic inflammation, which exacerbates metabolic dysregulation in lung cancer and results in poorer OS relative to mild diabetes with lung SqCLC.
Few studies have examined the effects of diabetes therapy on lung cancer outcomes, and those that did were retrospective studies with small sample sizes [11,45,46,47,48]. Studies have produced controversial data suggesting that the use of antidiabetic drugs (particularly metformin) reduces mortality in cancer patients [11,45,46,47,48]. By contrast, several studies have suggested that relative to various therapies (for example, insulin and sulfonylureas), metformin use improves survival outcomes for patients with non–small cell lung carcinoma [46,49]. Other studies have reported that metformin use has no effect or even leads to poorer survival for participants with lung cancer [47,48]. Although antidiabetic drugs were not matched in our study (Table 1), our results are consistent with the findings of the studies in which metformin or other antidiabetic drugs were revealed to have no anticancer effects [11,47,48]. The epidemiological data on the effects of various types of diabetes therapy on lung cancer outcomes are scarce and inconsistent; furthermore, the findings of relevant studies may have been affected by inconsistent or unclear selection of patients with lung cancer, unclear lung cancer histology, unclear clinical stages, and inhomogeneous confounding factors [46,47,48,49]. Our findings, which were obtaining after balancing covariates (Table 1) and eliminating selection bias, reveal that metformin and other antidiabetic drugs are not associated with survival outcomes for lung SqCLC (Table 2).
In the current study, only patients with both diabetes and lung SqCLC were enrolled for further analysis to avoid the influence of various survival effects, inconsistent treatments, and various driver gene mutations related to other types of lung cancer [27,28,29]. Additionally, almost all of the potential confounding factors associated with OS for lung SqCLC were matched (Table 1), with the exception being antidiabetic drug use for diabetes with varying levels of severity. After PSM was performed, all of the covariates were balanced between mild and moderate-to-severe diabetes with lung SqCLC. Evaluating lung SqCLC survival in patients with mild or moderate-to-severe diabetes through an RCT is challenging because lung SqCLC cannot be treated through tangible interventions [50]. Striking a balance among the confounding factors of lung SqCLC survival in patients with mild diabetes (case group) or moderate-to-severe diabetes (control group)—a main design requirement for RCTs—is difficult to achieve [50]. However, PSM can address this problem by maintaining a balance among the confounding factors for the case and control groups. PSM is the recommended strategy for estimating the effects of covariates in studies that may be affected by potential bias [21,51]. Our study is the first to use a PSM-based design to mimic an RCT for evaluating the real-world survival impact on patients with mild or moderate-to-severe diabetes along with lung SqCLC who are receiving standard treatments.
After PSM was performed, the multivariable Cox model did not reveal any significant difference in OS for most covariates between the mild and moderate-to-severe diabetes groups; the notable exceptions were age and sex. Thus, residual imbalances in sex and age may have remained in our population [52,53]. To clarify the effect of diabetes severity and the survival outcomes of lung SqCLC for patients who receive standard treatments, we conducted a sensitivity analysis of all-cause mortality for lung SqCLC and compared the mild and moderate-to-severe diabetes groups, which were stratified by sex and age. The aHRs for mortality were all more than 1 for patients from all age groups and both female and male patients. However, the aHRs of all-cause death for various levels of diabetes severity with lung SqCLC was not significantly different (Figure 1) for the age groups of ≤65 and >85 years because of the small sample sizes of these two age groups; nevertheless, their aHRs were more than 1. The current study is the first to verify that aDCSI is an independent prognostic factor for the OS of patients (regardless of age or sex) with both diabetes and lung SqCLC who are receiving standard treatments (Figure 1 and Figure 2).
Our study is also the first to verify the association of diabetes severity with the OS of patients with lung SqCLC who are receiving standard treatments. An aDCSI of ≥2 is an independent prognostic factor for the OS of patients with both diabetes and lung SqCLC who are receiving standard treatments. Our findings not only revealed that diabetes is a poor prognostic factor for OS in lung SqCLC but also that diabetes severity is an independent prognostic factor for the OS of patients with both diabetes and lung SqCLC who are receiving standard treatments. On the basis of the clinical stage, stratified results that were obtained after PSM, the complications, severity, and poor control of diabetes were revealed to be associated with poor OS in patients with both diabetes and lung SqCLC who were receiving standard treatments. Therefore, patients with diabetes who are also diagnosed with lung SqCLC should maintain excellent diabetes control and prevent their diabetes from progressing to a severe status (aDCSI ≥ 2) to improve their OS. Our results suggest that diabetes prevention medicine is associated with the oncologic outcomes of lung cancer. Our findings can serve as valuable references for endocrinologists, family medicine physicians, and oncologists. Additionally, we further clarified why patients with lung SqCLC can exhibit different survival outcomes even though they have similarly staged cancers and undergo standard treatments; this is a phenomenon that is especially prominent among patients with diabetes of varying severity. The prevention of diabetes progression (prevent aDCSI from progressing to ≥2) is an increasingly crucial public health objective for which health policies must be established. There is no solid data to prove the conceivable oncologic outcomes for lung SqCLC patients with different diabetes severity. Evidence-based data and findings from our study can support the imagines (the association of diabetes severity and mortality with lung SqCLC) to be true in the real-world, instead of conceivable hypothesis. Our study is also the first to verify the association of diabetes severity with the OS of patients with lung SqCLC who are receiving standard treatments. Moreover, the aDCSI score during the date of lung cancer diagnosis and our results hint prevention of diabetes progression is necessary for patients with diabetes; it affects not only diabetes control but also improves survival for patients with lung SqCLC. Clinical studies of lung cancer treatments have indicated that increasing the 5-year OS of patients with lung SqCLC by 8% through an intervention with p < 0.0001 is a difficult task [54]. Cancer treatments require substantial medical resources and represent a considerable financial burden for patients and governments [55]. By contrast, the prevention of diabetes progression is a straightforward and cost-effective endeavor that may be associated with an improved OS for patients with lung SqCLC.
The strength of our study is that it is the first large-scale, long-term follow-up, and comparative cohort study to compare the primary endpoints of OS between patients with diabetes who have aDCSI scores of 0–1 and those with aDCSI scores of ≥2. The covariates between the two groups were homogenous for the patients with lung SqCLC, and PSM was performed to eliminate selection bias (Table 1). To date, no study has estimated the survival effect of diabetes severity on all-cause death in patients with lung SqCLC who are receiving standard treatments (surgery for stages I and II and CCRT for stage III). Our study revealed that the poor prognostic factors for OS in patients with both diabetes and lung SqCLC are an aDCSI score of ≥2, male sex, and older age (Table 2); this finding is consistent with those of other cancer studies [56,57]. Among patients with both diabetes and lung SqCLC, those with an aDCSI score of ≥2 have poorer OS than those with an aDCSI of 0–1 (Figure 2). Research on lung SqCLC has been scant and has tended to not distinguish clearly between clinical stages; our study is the first to investigate the survival effects of aDCSI on all-cause death in patients with both diabetes and lung SqCLC (clear stages). Our findings should be considered in future clinical practice and prospective clinical trials to prevent the progression of diabetes to a DCSI level of ≥2; this goal can contribute to improving the OS of patients with both diabetes and lung SqCLC.
The current study has several limitations. First, because all of the enrolled patients with were Asian, their corresponding ethnic susceptibility relative to non-Asians remains unclear; therefore, caution should be taken when extrapolating our results to non-Asian populations. However, no study has reported significant differences in oncological outcomes between Asian and non-Asian survivors of lung SqCLC. Second, the diagnoses of all comorbid conditions were based on ICD-9-CM codes. The Taiwan Cancer Registry Administration randomly reviews charts and interviews patients to verify the accuracy of the diagnoses, and hospitals with outlier charges or practices may be audited and heavily penalized if malpractice or discrepancies are identified. Accordingly, to obtain crucial information on population specificity and disease occurrence, a large-scale randomized trial is required to compare carefully selected patients with both diabetes and lung SqCLC who are grouped on the basis of their aDCSI scores (0–1 or ≥2). Finally, the Taiwan Cancer Registry database does not contain information regarding dietary habits or body mass index, which may be risk factors for OS. Despite these limitations, the major strength of the current study is the use of data from a nationwide population-based registry with detailed baseline information. A lifelong follow-up was possible through the linkage of the registry with the national cause-of-death database. Given the magnitude and statistical significance of the observed effects in the current study, the aforementioned limitations are unlikely to have affected our conclusions.
5. Conclusions
Severe diabetes (aDCSI ≥ 2) is an independent prognostic factor of OS for patients with both diabetes and lung SqCLC who are receiving standard treatments. Preventing diabetes progression is necessary for patients with diabetes and lung SqCLC because it not only improves their diabetes control but also their OS in relation to lung SqCLC.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/cancers14102553/s1, Table S1: Adapted Diabetes Complications Severity Index.
Author Contributions
Conception and Design: C.-H.S., W.-M.C., M.C., B.-C.S. and S.-Y.W. Collection and Assembly of Data: C.-H.S., W.-M.C. and S.-Y.W. Data Analysis and Interpretation: C.-H.S., W.-M.C. and S.-Y.W. Administrative Support: S.-Y.W. Manuscript Writing: C.-H.S., W.-M.C., M.C., B.-C.S. and S.-Y.W. All authors have read and agreed to the published version of the manuscript.
Funding
Lo-Hsu Medical Foundation, LotungPoh-Ai Hospital, supports Szu-Yuan Wu’s work (Funding Number: 10908, 10909, 11001, 11002, 11003, 11006, and 11013). Fu Jen Catholic University supports Ben-Chang Shia’s work (Funding Number: A0110180 and A0110182).
Institutional Review Board Statement
The study protocols were reviewed and approved by the Institutional Review Board of Tzu-Chi Medical Foundation (IRB109-015-B).
Informed Consent Statement
Informed consent was waived because the data sets are covered under the Personal Information Protection Act.
Data Availability Statement
The datasets supporting the study conclusions are included within this manuscript and its additional files.
Conflicts of Interest
The authors declare no conflict of interests.
Abbreviations
| aHR | adjusted hazard ratio |
| CI | confidence interval |
| RCT | randomized controlled trial |
| PSM | propensity score matching |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
| ICD-10-CM | International Classification of Diseases, Tenth Revision, Clinical Modification |
| OS | overall survival |
| CCI | Charlson comorbidity index |
| IPTW | inverse probability of treatment weighting |
| NTD | New Taiwan dollars |
| y | years old |
| aDCSI | adapted diabetes complications severity index |
| HR | hazard ratio |
| AMI | acute myocardial infarction |
| TB | tuberculosis |
| COPD | chronic obstructive pulmonary disease |
| SqCLC | squamous cell carcinoma |
| AJCC | American Joint Committee on Cancer |
| CCRT | concurrent chemoradiotherapy |
| RT | radiation therapy |
| IGF-1 | insulin-like growth factor-1 |
| NSCLC | non–small cell lung carcinoma |
References
- Dwivedi, M.; Pandey, A.R. Diabetes mellitus and its treatment: An overview. J. Adv. Pharmacol. 2020, 1, 48–58. [Google Scholar]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Boyko, E.J.; et al. Diabetes complications severity index and risk of mortality, hospitalization, and healthcare utilization. Am. J. Manag. Care 2008, 14, 15–23. [Google Scholar] [PubMed]
- Arvanitakis, Z.; Wilson, R.; Bennett, D. Diabetes mellitus, dementia, and cognitive function in older persons. J. Nutr. Health Aging 2006, 10, 287. [Google Scholar] [PubMed]
- Kakarlapudi, V.; Sawyer, R.; Staecker, H. The effect of diabetes on sensorineural hearing loss. Otol. Neurotol. 2003, 24, 382–386. [Google Scholar] [CrossRef]
- Vigneri, P.; Frasca, F.; Sciacca, L.; Pandini, G.; Vigneri, R. Diabetes and cancer. J. Endocr.-Relat. Cancer 2009, 16, 1103–1123. [Google Scholar] [CrossRef] [Green Version]
- Barone, B.B.; Yeh, H.C.; Snyder, C.F.; Peairs, K.S.; Stein, K.B.; Derr, R.L.; Wolff, A.C.; Brancati, F.L. Long-term all-cause mortality in cancer patients with preexisting diabetes mellitus: A systematic review and meta-analysis. JAMA 2008, 300, 2754–2764. [Google Scholar] [CrossRef] [Green Version]
- Tsilidis, K.K.; Kasimis, J.C.; Lopez, D.S.; Ntzani, E.E.; Ioannidis, J.P. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies. BMJ 2015, 350, g7607. [Google Scholar] [CrossRef] [Green Version]
- Harding, J.L.; Shaw, J.E.; Peeters, A.; Cartensen, B.; Magliano, D.J. Cancer risk among people with type 1 and type 2 diabetes: Disentangling true associations, detection bias, and reverse causation. Diabetes Care 2015, 38, 264–270. [Google Scholar] [CrossRef] [Green Version]
- Giovannucci, E.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and cancer: A consensus report. Diabetes Care 2010, 33, 1674–1685. [Google Scholar] [CrossRef] [Green Version]
- Torre, L.A.; Siegel, R.L.; Jemal, A. Lung cancer statistics. J. Lung Cancer Pers. Med. 2016, 1–19. [Google Scholar]
- Luo, J.; Hendryx, M.; Qi, L.; Ho, G.Y.; Margolis, K.L. Pre-existing diabetes and lung cancer prognosis. Br. J. Cancer 2016, 115, 76–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wicke, F.S.; Glushan, A.; Schubert, I.; Koster, I.; Lubeck, R.; Hammer, M.; Beyer, M.; Karimova, K. Performance of the adapted Diabetes Complications Severity Index translated to ICD-10. Am. J. Manag. Care 2019, 25, e45–e49. [Google Scholar] [PubMed]
- Chang, H.Y.; Weiner, J.P.; Richards, T.M.; Bleich, S.N.; Segal, J.B. Validating the adapted diabetes complications severity index in claims data. Am. J. Manag. Care 2012, 18, 721–726. [Google Scholar] [PubMed]
- Zhang, J.; Lu, C.Y.; Chen, H.M.; Wu, S.Y. Neoadjuvant chemotherapy or endocrine therapy for invasive ductal carcinoma of the breast with high hormone receptor positivity and human epidermal growth factor receptor 2 negativity. JAMA Netw. Open 2021, 4, e211785. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.Y.; Chang, C.L.; Chen, C.I.; Huang, C.C. Comparison of acute and chronic surgical complications following robot-assisted, laparoscopic, and traditional open radical prostatectomy among men in Taiwan. JAMA Netw. Open 2021, 4, e2120156. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Hsu, C.H.; Lin, Y.C.; Wu, S.Y. Effects of 1-Year hospital volume on surgical margin and biochemical-failure-free survival in patients undergoing robotic versus nonrobotic radical prostatectomy: A nationwide cohort study from the national taiwan cancer database. Cancers 2021, 13, 488. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, C.Y.; Qin, L.; Chen, H.M.; Wu, S.Y. Breast-conserving surgery with or without irradiation in women with invasive ductal carcinoma of the breast receiving preoperative systemic therapy: A cohort study. Breast 2020, 54, 139–147. [Google Scholar] [CrossRef]
- Auperin, A.; Le Pechoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef]
- Vokes, E.E.; Herndon, J.E., 2nd; Kelley, M.J.; Cicchetti, M.G.; Ramnath, N.; Neill, H.; Atkins, J.N.; Watson, D.M.; Akerley, W.; Green, M.R.; et al. Induction chemotherapy followed by chemoradiotherapy compared with chemoradiotherapy alone for regionally advanced unresectable stage III Non-small-cell lung cancer: Cancer and Leukemia Group B. J. Clin. Oncol. 2007, 25, 1698–1704. [Google Scholar] [CrossRef]
- Belani, C.P.; Choy, H.; Bonomi, P.; Scott, C.; Travis, P.; Haluschak, J.; Curran, W.J., Jr. Combined chemoradiotherapy regimens of paclitaxel and carboplatin for locally advanced non-small-cell lung cancer: A randomized phase II locally advanced multi-modality protocol. J. Clin. Oncol. 2005, 23, 5883–5891. [Google Scholar] [CrossRef]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Y.; Yung, Y.-F.; Stokes, M. Propensity Score Methods for Causal Inference with the PSMATCH Procedure. In Proceedings of the SAS Global Forum 2017 Conference, Orlando, FL, USA, 2–5 April 2017. [Google Scholar]
- Austin, P.C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2014, 33, 1242–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergamino, M.; Rullan, A.J.; Saigi, M.; Peiro, I.; Montanya, E.; Palmero, R.; Ruffinelli, J.C.; Navarro, A.; Arnaiz, M.D.; Brao, I.; et al. Fasting plasma glucose is an independent predictor of survival in patients with locally advanced non-small cell lung cancer treated with concurrent chemoradiotherapy. BMC Cancer 2019, 19, 165. [Google Scholar] [CrossRef] [PubMed]
- Xin, W.X.; Fang, L.; Fang, Q.L.; Zheng, X.W.; Ding, H.Y.; Huang, P. Effect of hypoglycemic agents on survival outcomes of lung cancer patients with diabetes mellitus: A meta-analysis. Medicine 2018, 97, e0035. [Google Scholar] [CrossRef]
- Kurishima, K.; Watanabe, H.; Ishikawa, H.; Satoh, H.; Hizawa, N. Survival of patients with lung cancer and diabetes mellitus. Mol. Clin. Oncol 2017, 6, 907–910. [Google Scholar] [CrossRef] [Green Version]
- Oncology, National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (accessed on 30 September 2021).
- Zhang, Y.; Sun, Y.; Pan, Y.; Li, C.; Shen, L.; Li, Y.; Luo, X.; Ye, T.; Wang, R.; Hu, H.; et al. Frequency of driver mutations in lung adenocarcinoma from female never-smokers varies with histologic subtypes and age at diagnosis. Clin. Cancer Res. 2012, 18, 1947–1953. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.N.; Yan, H.H.; Wang, J.; Chu, X.Y.; Liu, Z.D.; Shen, Y.; Ma, H.T.; Fu, X.N.; Hu, J.; Zhou, N.K.; et al. Real-World survival outcomes based on EGFR mutation status in Chinese patients with lung adenocarcinoma after complete resection: Results from the ICAN study. JTO Clin. Res. Rep. 2022, 3, 100257. [Google Scholar] [CrossRef]
- Morss, A.S.; Edelman, E.R. Glucose modulates basement membrane fibroblast growth factor-2 via alterations in endothelial cell permeability. J. Biol. Chem. 2007, 282, 14635–14644. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Jimenez, C.; Garcia-Martinez, J.M.; Chocarro-Calvo, A.; De la Vieja, A. A new link between diabetes and cancer: Enhanced WNT/beta-catenin signaling by high glucose. J. Mol. Endocrinol. 2014, 52, R51–R66. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Alex, J.M.; Bast, F. Insulin receptor (IR) and insulin-like growth factor receptor 1 (IGF-1R) signaling systems: Novel treatment strategies for cancer. Med. Oncol. 2014, 31, 805. [Google Scholar] [CrossRef]
- Cardillo, T.M.; Trisal, P.; Arrojo, R.; Goldenberg, D.M.; Chang, C.H. Targeting both IGF-1R and mTOR synergistically inhibits growth of renal cell carcinoma in vitro. BMC Cancer 2013, 13, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodt, P.; Samani, A.; Navab, R. Inhibition of the type I insulin-like growth factor receptor expression and signaling: Novel strategies for antimetastatic therapy. Biochem. Pharmacol. 2000, 60, 1101–1107. [Google Scholar] [CrossRef]
- Singh, R.K.; Gaikwad, S.M.; Jinager, A.; Chaudhury, S.; Maheshwari, A.; Ray, P. IGF-1R inhibition potentiates cytotoxic effects of chemotherapeutic agents in early stages of chemoresistant ovarian cancer cells. Cancer Lett. 2014, 354, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Wilky, B.A.; Rudek, M.A.; Ahmed, S.; Laheru, D.A.; Cosgrove, D.; Donehower, R.C.; Nelkin, B.; Ball, D.; Doyle, L.A.; Chen, H.; et al. A phase I trial of vertical inhibition of IGF signalling using cixutumumab, an anti-IGF-1R antibody, and selumetinib, an MEK 1/2 inhibitor, in advanced solid tumours. Br. J. Cancer 2015, 112, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Vander Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef] [Green Version]
- Han, L.; Ma, Q.; Li, J.; Liu, H.; Li, W.; Ma, G.; Xu, Q.; Zhou, S.; Wu, E. High glucose promotes pancreatic cancer cell proliferation via the induction of EGF expression and transactivation of EGFR. PLoS ONE 2011, 6, e27074. [Google Scholar] [CrossRef]
- De Rosa, V.; Iommelli, F.; Monti, M.; Fonti, R.; Votta, G.; Stoppelli, M.P.; Del Vecchio, S. Reversal of Warburg Effect and Reactivation of Oxidative Phosphorylation by Differential Inhibition of EGFR Signaling Pathways in Non-Small Cell Lung Cancer. Clin. Cancer Res. 2015, 21, 5110–5120. [Google Scholar] [CrossRef] [Green Version]
- van de Poll-Franse, L.V.; Houterman, S.; Janssen-Heijnen, M.L.; Dercksen, M.W.; Coebergh, J.W.; Haak, H.R. Less aggressive treatment and worse overall survival in cancer patients with diabetes: A large population based analysis. Int J. Cancer 2007, 120, 1986–1992. [Google Scholar] [CrossRef]
- De Giorgio, R.; Barbara, G.; Cecconi, A.; Corinaldesi, R.; Mancini, A.M. Diabetes is associated with longer survival rates in patients with malignant tumors. Arch. Intern. Med. 2000, 160, 2217. [Google Scholar] [CrossRef]
- Park, S.M.; Lim, M.K.; Shin, S.A.; Yun, Y.H. Impact of prediagnosis smoking, alcohol, obesity, and insulin resistance on survival in male cancer patients: National Health Insurance Corporation Study. J. Clin. Oncol. 2006, 24, 5017–5024. [Google Scholar] [CrossRef]
- Hatlen, P.; Gronberg, B.H.; Langhammer, A.; Carlsen, S.M.; Amundsen, T. Prolonged survival in patients with lung cancer with diabetes mellitus. J. Thorac. Oncol. 2011, 6, 1810–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shieh, S.H.; Probst, J.C.; Sung, F.C.; Tsai, W.C.; Li, Y.S.; Chen, C.Y. Decreased survival among lung cancer patients with co-morbid tuberculosis and diabetes. BMC Cancer 2012, 12, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storozhuk, Y.; Hopmans, S.N.; Sanli, T.; Barron, C.; Tsiani, E.; Cutz, J.C.; Pond, G.; Wright, J.; Singh, G.; Tsakiridis, T. Metformin inhibits growth and enhances radiation response of non-small cell lung cancer (NSCLC) through ATM and AMPK. Br. J. Cancer 2013, 108, 2021–2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, B.X.; Yao, W.X.; Ge, J.; Peng, X.C.; Du, X.B.; Zhang, R.; Yao, B.; Xie, K.; Li, L.H.; Dong, H.; et al. Prognostic influence of metformin as first-line chemotherapy for advanced nonsmall cell lung cancer in patients with type 2 diabetes. Cancer 2011, 117, 5103–5111. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, P.J.; Rai, H.; Beukemann, M.; Xu, M.; Jain, A.; Sasidhar, M. The effect of metformin and thiazolidinedione use on lung cancer in diabetics. BMC Cancer 2012, 12, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, I.; Ferro, A.; Cohler, A.; Langenfeld, J.; Surakanti, S.G.; Aisner, J.; Zou, W.; Haffty, B.G.; Jabbour, S.K. Impact of metformin use on survival in locally-advanced, inoperable non-small cell lung cancer treated with definitive chemoradiation. J. Thorac. Dis. 2015, 7, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.J.; Gallagher, E.J.; Sigel, K.; Mhango, G.; Galsky, M.D.; Smith, C.B.; LeRoith, D.; Wisnivesky, J.P. Survival of patients with stage IV lung cancer with diabetes treated with metformin. Am. J. Respir Crit Care Med. 2015, 191, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Deaton, A.; Cartwright, N. Understanding and misunderstanding randomized controlled trials. Soc. Sci. Med. 2018, 210, 2–21. [Google Scholar] [CrossRef]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.L.; Collins, G.S.; Spence, J.; Daures, J.P.; Devereaux, P.J.; Landais, P.; Le Manach, Y. Double-adjustment in propensity score matching analysis: Choosing a threshold for considering residual imbalance. BMC Med. Res. Methodol. 2017, 17, 78. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Kim, H.J.; Lonjon, G.; Zhu, Y.; on behalf of AME Big-Data Clinical Trial Collaborative Group. Balance diagnostics after propensity score matching. Ann. Transl. Med. 2019, 7, 16. [Google Scholar] [CrossRef]
- Bertaglia, V.; Vallone, S.; Pacchiana, M.V.; Novello, S. Advanced squamous lung cancer: Therapeutic options, future directions, unmet needs and results of a monocentric survey. Lung Cancer Manag. 2017, 6, 93–107. [Google Scholar] [CrossRef] [PubMed]
- Carrera, P.M.; Kantarjian, H.M.; Blinder, V.S. The financial burden and distress of patients with cancer: Understanding and stepping-up action on the financial toxicity of cancer treatment. CA Cancer J. Clin. 2018, 68, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Tas, F.; Ciftci, R.; Kilic, L.; Karabulut, S. Age is a prognostic factor affecting survival in lung cancer patients. Oncol. Lett. 2013, 6, 1507–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, T.A.; Chen, P.H.; Wu, P.F.; Wang, T.N.; Chang, P.Y.; Ko, A.M.; Huang, M.S.; Ko, Y.C. Important prognostic factors for the long-term survival of lung cancer subjects in Taiwan. BMC Cancer 2008, 8, 324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Sensitivity analysis of sex- and age-stratified groups (using inverse probability of treatment weighting) for all-cause death in patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes. Abbreviations: aHR, adjusted hazard ratio; y, years; aDCSI, adapted Diabetes Complications Severity Index; CI, confidence interval; ref., reference group.
Figure 1.
Sensitivity analysis of sex- and age-stratified groups (using inverse probability of treatment weighting) for all-cause death in patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes. Abbreviations: aHR, adjusted hazard ratio; y, years; aDCSI, adapted Diabetes Complications Severity Index; CI, confidence interval; ref., reference group.

Figure 2.
Kaplan–Meier overall survival curves for patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes.
Figure 2.
Kaplan–Meier overall survival curves for patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes.


{kind=link}
{kind=link}
Table 1.
Characteristics of patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes (after propensity score matching).
Table 1.
Characteristics of patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes (after propensity score matching).
| aDCSI 0–1 | aDCSI ≥ 2 | ||||
|---|---|---|---|---|---|
| N = 2871 | % | N = 2871 | p-Value | ||
| Sex | |||||
| Female | 970 | 33.79% | 988 | 34.41% | 0.6163 |
| Male | 1901 | 66.21% | 1883 | 65.59% | |
| Age | 73.18 ± 10.94 | 74.73 ± 10.32 | 0.1019 | ||
| Age group (y) | |||||
| Age ≤ 65 | 541 | 18.84% | 541 | 18.84% | 0.9015 |
| 65 < Age ≤ 75 | 804 | 28.00% | 804 | 28.00% | |
| 75 < Age ≤ 85 | 1165 | 40.58% | 1147 | 39.95% | |
| Age > 85 | 361 | 12.57% | 379 | 13.20% | |
| AJCC clinical stage | |||||
| Stage I | 143 | 4.98% | 143 | 4.98% | 1.0000 |
| Stage II | 280 | 9.75% | 280 | 9.75% | |
| Stage IIIA | 725 | 25.25% | 725 | 25.25% | |
| Stage IIIB/C | 1723 | 60.01% | 1723 | 60.01% | |
| Income level (NTD) | |||||
| Low-income | 41 | 1.43% | 44 | 1.53% | 0.8372 |
| ≤10,000 | 968 | 33.72% | 970 | 33.79% | |
| 10,001–15,000 | 718 | 25.01% | 726 | 25.29% | |
| 15,001–20,000 | 918 | 31.97% | 914 | 31.83% | |
| 20,001–30,000 | 112 | 3.90% | 111 | 3.87% | |
| 30,001–45,000 | 68 | 2.37% | 65 | 2.26% | |
| >45,000 | 46 | 1.60% | 41 | 1.43% | |
| Urbanization | |||||
| Rural | 982 | 34.20% | 1014 | 35.32% | 0.3752 |
| Urban | 1889 | 65.80% | 1857 | 64.68% | |
| CCI Score | |||||
| ≥1 | 2341 | 81.54% | 2341 | 81.54% | 1.000 |
| Comorbidities | |||||
| COPD | 1948 | 67.85% | 1995 | 69.49% | 0.1812 |
| Chronic bronchitis | 1541 | 53.67% | 1544 | 53.78% | 0.9284 |
| Emphysema | 247 | 8.60% | 232 | 8.08% | 0.9357 |
| Acute upper respiratory tract infection | 1243 | 43.30% | 1271 | 44.27% | 0.4564 |
| Asthma | 1130 | 39.36% | 1151 | 40.09% | 0.6920 |
| Pneumoconiosis | 67 | 2.33% | 54 | 1.88% | 0.2323 |
| Cardiovascular diseases | 1537 | 54.54% | 1544 | 53.78% | 0.8205 |
| AMI | 208 | 7.24% | 216 | 7.52% | 0.8727 |
| Stroke | 324 | 11.28% | 325 | 11.32% | 0.9441 |
| TB | 395 | 13.76% | 397 | 13.83% | 0.9047 |
| Obesity | 74 | 2.58% | 70 | 2.44% | 0.8407 |
| Current smoking habit | 1109 | 38.63% | 1110 | 38.67% | 0.9451 |
| Alcohol-related disease | 431 | 15.01% | 434 | 15.11% | 0.7929 |
| Diabetic medication use | |||||
| Metformin | 1546 | 53.85% | 1682 | 58.59% | 0.0003 |
| Sulfonylurea | 1553 | 54.09% | 1714 | 59.70% | <0.0001 |
| Meglitinide | 298 | 10.38% | 355 | 12.37% | 0.0178 |
| α-glucosidase inhibitors | 468 | 16.30% | 632 | 22.01% | <0.0001 |
| Thiazolidinediones | 289 | 10.07% | 449 | 15.64% | <0.0001 |
| Dipeptidyl peptidase-4 inhibitors | 226 | 7.87% | 370 | 12.89% | <0.0001 |
| Glucagon-like peptide-1 | 201 | 7.00% | 374 | 13.02% | <0.0001 |
| SGLT2 inhibitors | 231 | 8.05% | 402 | 14.00% | <0.0001 |
| Insulin | 482 | 16.79% | 696 | 24.24% | <0.0001 |
| Number of diabetic medications taken | <0.0001 | ||||
| 0 | 765 | 26.65% | 522 | 18.18% | |
| 1 | 478 | 16.65% | 530 | 18.46% | |
| 2 | 413 | 14.39% | 352 | 12.26% | |
| ≥3 | 1215 | 42.32% | 1467 | 51.10% | |
| Diabetes Duration, Years; (Mean ± SD) | 4.63 ± 2.15 | 4.43 ± 2.13 | 0.8926 | ||
| 1–1.99 year | 142 | 4.95% | 148 | 5.15% | |
| 2–2.99 years | 281 | 9.79% | 285 | 9.93% | |
| 3–3.99 years | 724 | 25.22% | 727 | 25.32% | |
| 4–4.99 years | 1001 | 34.87% | 999 | 34.80% | |
| ≥5 years | 723 | 25.18% | 712 | 24.80% | |
| Death | 1907 | 66.42% | 2035 | 70.88% | 0.0003 |
| Mean follow-up, Year; (Mean ± SD) | 2.44 ± 3.24 | 2.18 ± 2.83 | <0.0001 | ||
| Median follow-up, Year; Median (IQR, Q1, Q2) | 1.37 (0.41, 3.87) | 1.13 (0.30, 3.77) | 0.0019 | ||
CCI, Charlson comorbidity index; IQR, interquartile range; SD, standard deviation; NTD, New Taiwan dollars; N, number; y, years; aDCSI, adapted Diabetes Complications Severity Index; N, number; y, years; SGLT2, sodium-glucose cotransporter-2; AMI, acute myocardial infarction; TB, tuberculosis; COPD, chronic obstructive pulmonary disease.
Table 2.
Multivariable Cox proportional regression analysis of all-cause death among propensity score–matched patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes.
Table 2.
Multivariable Cox proportional regression analysis of all-cause death among propensity score–matched patients with both lung squamous cell carcinoma and mild or moderate-to-severe diabetes.
| aHR * | 95% CI | p-Value | ||
|---|---|---|---|---|
| aDCSI scores (Ref. aDCSI: 0–1) | ||||
| aDCSI ≥2 | 1.17 | 1.08 | 1.28 | 0.0005 |
| Sex (Ref. female) | ||||
| Male | 1.19 | 1.10 | 1.34 | 0.0002 |
| Age (y; Ref. ≤ 65) | ||||
| 65 < Age ≤ 75 | 1.33 | 1.13 | 1.57 | 0.0004 |
| 75 < Age ≤ 85 | 2.03 | 1.76 | 2.37 | <0.0001 |
| Age > 85 | 3.12 | 2.60 | 3.71 | <0.0001 |
| AJCC clinical stage (Ref. Stage I) | ||||
| Stage II | 1.01 | 0.60 | 1.04 | 0.3644 |
| Stage IIIA | 1.11 | 0.89 | 1.36 | 0.2262 |
| Stage IIIB/C | 1.17 | 0.66 | 1.97 | 0.2120 |
| Income level, NTD (Ref. low income) | ||||
| ≤10,000 | 0.87 | 0.65 | 1.20 | 0.4762 |
| 10,001–15,000 | 0.85 | 0.63 | 1.20 | 0.4159 |
| 15,001–20,000 | 0.81 | 0.59 | 1.12 | 0.1876 |
| 20,001–30,000 | 0.71 | 0.44 | 1.05 | 0.1291 |
| 30,001–45,000 | 0.62 | 0.46 | 1.03 | 0.0589 |
| >45,000 | 0.45 | 0.25 | 1.04 | 0.0598 |
| Urbanization (Ref. rural) | ||||
| Urban | 0.97 | 0.87 | 1.09 | 0.7351 |
| CCI Scores (Ref. CCI = 0) | ||||
| CCI ≥ 1 | 1.01 | 0.89 | 1.15 | 0.9212 |
| Comorbidities | ||||
| COPD (Ref. No) | 0.96 | 0.85 | 1.05 | 0.1932 |
| Chronic bronchitis (Ref. No) | 0.94 | 0.86 | 1.03 | 0.1153 |
| Emphysema (Ref. No) | 1.01 | 0.92 | 1.09 | 0.9301 |
| Acute upper respiratory tract infection (Ref. No) | 1.17 | 0.87 | 1.66 | 0.2404 |
| Asthma (Ref. No) | 1.04 | 0.81 | 1.31 | 0.9156 |
| Pneumoconiosis (Ref. No) | 1.00 | 0.87 | 1.12 | 0.8635 |
| Cardiovascular diseases (Ref. No) | 1.20 | 0.89 | 1.68 | 0.2441 |
| AMI (Ref. No) | 1.15 | 0.86 | 1.40 | 0.3830 |
| Stroke (Ref. No) | 1.02 | 0.76 | 1.20 | 0.8721 |
| TB (Ref. No) | 1.04 | 0.80 | 1.14 | 0.5311 |
| Obesity (Ref. No) | 1.11 | 0.80 | 1.51 | 0.3420 |
| Current Smoking (Ref. No) | 1.20 | 0.94 | 1.50 | 0.2261 |
| Alcohol-related disease (Ref. No) | 1.25 | 0.90 | 1.51 | 0.3313 |
| Diabetic medication use | ||||
| Metformin | 0.82 | 0.66 | 1.08 | 0.1282 |
| Sulfonylurea | 0.99 | 0.70 | 1.15 | 0.6544 |
| Meglitinide | 0.97 | 0.89 | 1.10 | 0.6761 |
| α-glucosidase inhibitors | 1.02 | 0.91 | 1.17 | 0.4553 |
| Thiazolidinediones | 1.01 | 0.82 | 1.20 | 0.9241 |
| Dipeptidyl peptidase-4 inhibitors | 1.03 | 0.95 | 1.28 | 0.1029 |
| Glucagon-like peptide-1 | 0.95 | 0.90 | 1.04 | 0.1382 |
| SGLT2 inhibitors | 0.97 | 0.90 | 1.03 | 0.1764 |
| Insulin | 1.02 | 0.94 | 1.06 | 0.7253 |
| Number of diabetic medications taken (Ref. No antidiabetic drug) | ||||
| 1 | 1.14 | 0.81 | 1.29 | 0.2352 |
| 2 | 1.32 | 0.87 | 1.57 | 0.3486 |
| ≥3 | 1.23 | 0.90 | 1.43 | 0.3527 |
| Diabetes Duration (Ref. 1–1.99 years) | ||||
| 2–2.99 years | 1.01 | 0.92 | 1.32 | 0.2932 |
| 3–3.99 years | 1.04 | 0.88 | 1.09 | 0.6948 |
| 4–4.99 years | 1.08 | 0.90 | 1.16 | 0.2537 |
| ≥5 years | 1.09 | 0.81 | 1.21 | 0.9216 |
aHR, adjusted hazard ratio; CCI, Charlson comorbidity index; NTD, New Taiwan dollars; y, years; aDCSI, adapted Diabetes Complications Severity Index; CI, confidence interval; HR, hazard ratio; ref., reference group; N, number; y, years; SGLT2, sodium-glucose cotransporter-2; AMI, acute myocardial infarction; TB, tuberculosis; COPD, chronic obstructive pulmonary disease. * All covariates presented in Table 2 were adjusted.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Su, C.-H.; Chen, W.-M.; Chen, M.; Shia, B.-C.; Wu, S.-Y. Association of Diabetes Severity and Mortality with Lung Squamous Cell Carcinoma. Cancers 2022, 14, 2553. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102553
AMA Style
Su C-H, Chen W-M, Chen M, Shia B-C, Wu S-Y. Association of Diabetes Severity and Mortality with Lung Squamous Cell Carcinoma. Cancers. 2022; 14(10):2553. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102553
Chicago/Turabian StyleSu, Chih-Hsiung, Wan-Ming Chen, Mingchih Chen, Ben-Chang Shia, and Szu-Yuan Wu. 2022. "Association of Diabetes Severity and Mortality with Lung Squamous Cell Carcinoma" Cancers 14, no. 10: 2553. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102553
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.