
Deep-Learning-Based Automatic Detection and Segmentation of Brain Metastases with Small Volume for Stereotactic Ablative Radiotherapy

 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Brain Metastases Populations
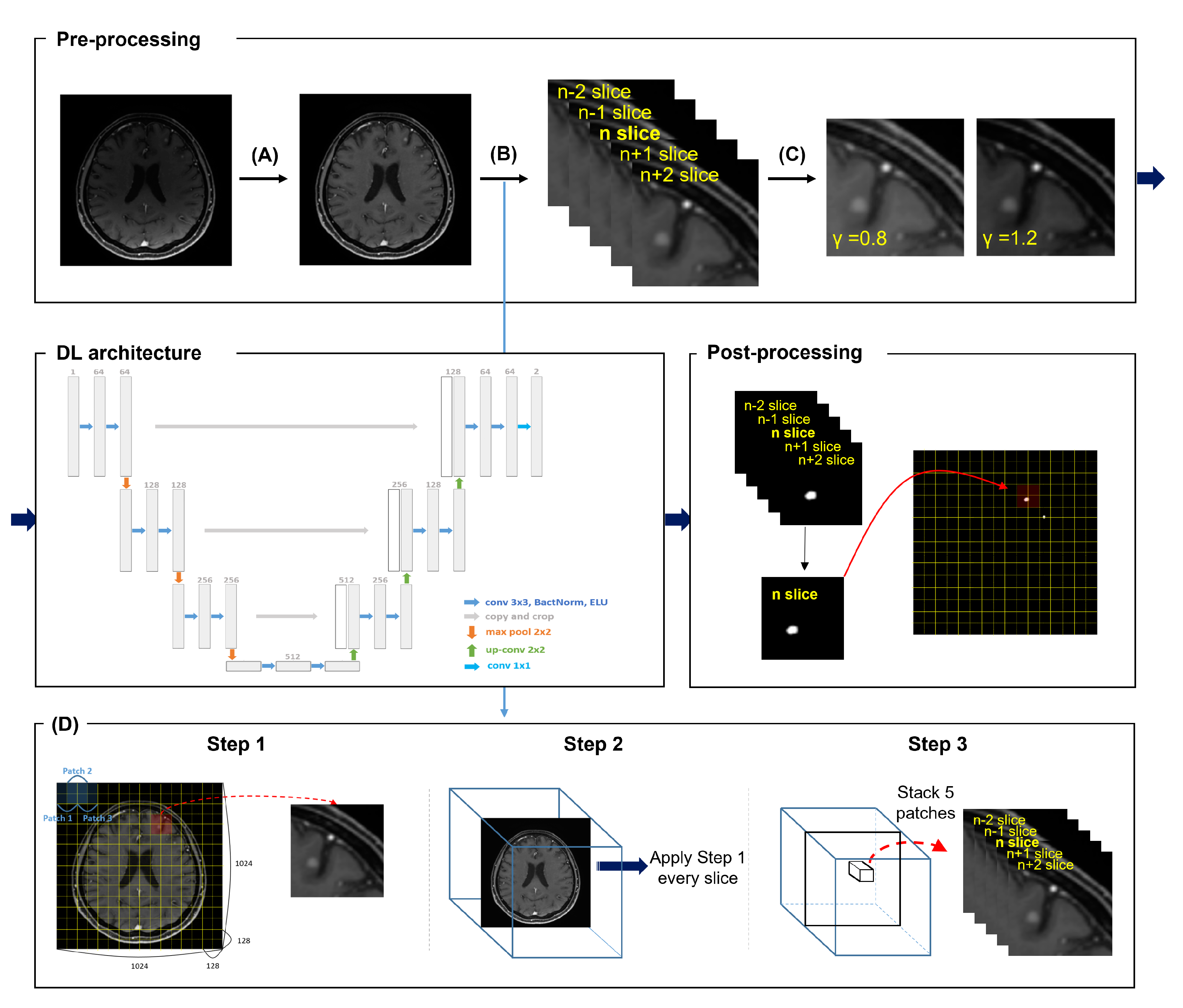
2.3. Deep Learning Strategy
2.4. Deep Learning Details
2.5. Statistical Analysis
3. Results
3.1. Detection Performance
3.2. Segmentation Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, X.; DeAngelis, L.M. Treatment of brain metastases. J. Clin. Oncol. 2015, 33, 3475. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2015. Cancer Res. Treat. 2018, 50, 303. [Google Scholar] [CrossRef] [PubMed]
- Arvold, N.D.; Lee, E.Q.; Mehta, M.P.; Margolin, K.; Alexander, B.M.; Lin, N.U.; Anders, C.K.; Soffietti, R.; Camidge, D.R.; Vogelbaum, M.A.; et al. Updates in the management of brain metastases. Neuro-oncology 2016, 18, 1043–1065. [Google Scholar] [CrossRef] [PubMed]
- Soffietti, R.; Abacioglu, U.; Baumert, B.; Combs, S.E.; Kinhult, S.; Kros, J.M.; Marosi, C.; Metellus, P.; Radbruch, A.; Villa Freixa, S.S.; et al. Diagnosis and treatment of brain metastases from solid tumors: Guidelines from the European Association of Neuro-Oncology (EANO). Neuro-oncology 2017, 19, 162–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achrol, A.S.; Rennert, R.C.; Anders, C.; Soffietti, R.; Ahluwalia, M.S.; Nayak, L.; Peters, S.; Arvold, N.D.; Harsh, G.R.; Steeg, P.S.; et al. Brain metastases. Nat. Rev. Dis. Prim. 2019, 5, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Hartgerink, D.; Van der Heijden, B.; De Ruysscher, D.; Postma, A.; Ackermans, L.; Hoeben, A.; Anten, M.; Lambin, P.; Terhaag, K.; Jochems, A.; et al. Stereotactic radiosurgery in the management of patients with brain metastases of non-small cell lung cancer: Indications, decision tools and future directions. Front. Oncol. 2018, 8, 154. [Google Scholar] [CrossRef] [Green Version]
- Dhermain, F.; Noël, G.; Antoni, D.; Tallet, A. Role of radiation therapy in brain metastases management. Cancer/Radiothérapie 2020, 24, 463–469. [Google Scholar] [CrossRef]
- Vinod, S.K.; Jameson, M.G.; Min, M.; Holloway, L.C. Uncertainties in volume delineation in radiation oncology: A systematic review and recommendations for future studies. Radiother. Oncol. 2016, 121, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.M.; Larochelle, H. Brain tumor segmentation with deep neural networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [Green Version]
- Losch, M. Detection and Segmentation of Brain Metastases with Deep Convolutional Networks. Master’s Thesis, KTH, Computer Vision and Active Perception, CVAP. 2015. Available online: http://urn.kb.se/resolve?urn=urn:nbn:se:kth:diva-173519 (accessed on 26 October 2016).
- Xue, J.; Wang, B.; Ming, Y.; Liu, X.; Jiang, Z.; Wang, C.; Liu, X.; Chen, L.; Qu, J.; Xu, S.; et al. Deep learning–based detection and segmentation-assisted management of brain metastases. Neuro-oncology 2020, 22, 505–514. [Google Scholar] [CrossRef]
- Bousabarah, K.; Ruge, M.; Brand, J.S.; Hoevels, M.; Rueß, D.; Borggrefe, J.; Hokamp, N.G.; Visser-Vandewalle, V.; Maintz, D.; Treuer, H.; et al. Deep convolutional neural networks for automated segmentation of brain metastases trained on clinical data. Radiat. Oncol. 2020, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Charron, O.; Lallement, A.; Jarnet, D.; Noblet, V.; Clavier, J.B.; Meyer, P. Automatic detection and segmentation of brain metastases on multimodal MR images with a deep convolutional neural network. Comput. Biol. Med. 2018, 95, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Grøvik, E.; Yi, D.; Iv, M.; Tong, E.; Rubin, D.; Zaharchuk, G. Deep learning enables automatic detection and segmentation of brain metastases on multisequence MRI. J. Magn. Reson. Imaging 2020, 51, 175–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dikici, E.; Ryu, J.L.; Demirer, M.; Bigelow, M.; White, R.D.; Slone, W.; Erdal, B.S.; Prevedello, L.M. Automated brain metastases detection framework for T1-weighted contrast-enhanced 3D MRI. IEEE J. Biomed. Health Inform. 2020, 24, 2883–2893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Styner, M.; Brechbuhler, C.; Szckely, G.; Gerig, G. Parametric estimate of intensity inhomogeneities applied to MRI. IEEE Trans. Med. Imaging 2000, 19, 153–165. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 bias correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef] [Green Version]
- Galdran, A.; Alvarez-Gila, A.; Meyer, M.I.; Saratxaga, C.L.; Araújo, T.; Garrote, E.; Aresta, G.; Costa, P.; Mendonça, A.M.; Campilho, A. Data-driven color augmentation techniques for deep skin image analysis. arXiv 2017, arXiv:1703.03702. [Google Scholar]
- Gupta, R.; Sailaja, R.M.; Panda, S.; Sharma, S.; Mittal, A. Foreground-Background Separation on GPU using order based approaches. In Proceedings of the Seventh Indian Conference on Computer Vision, Graphics and Image Processing, Chennai India, 12–15 December 2010; pp. 448–455. [Google Scholar]
- Ahmad, H.M.; Ghuffar, S.; Khurshid, K. Classification of breast cancer histology images using transfer learning. In Proceedings of the 2019 16th International Bhurban Conference on Applied Sciences and Technology (IBCAST), Islamabad, Pakistan, 8–12 January 2019; pp. 328–332. [Google Scholar]
- Chawla, N.V.; Japkowicz, N.; Kotcz, A. Special issue on learning from imbalanced data sets. ACM SIGKDD Explor. Newsl. 2004, 6, 1–6. [Google Scholar] [CrossRef]
- Yen, S.J.; Lee, Y.S. Under-sampling approaches for improving prediction of the minority class in an imbalanced dataset. In Intelligent Control and Automation; Springer: Berlin/Heidelberg, Germany, 2006; pp. 731–740. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation; Springer: Cham, Swithzerland, 2015; pp. 234–241. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. Pytorch: An imperative style, high-performance deep learning library. Adv. Neural Inf. Process. Syst. 2019, 32, 8024–8035. [Google Scholar]
- Clevert, D.A.; Unterthiner, T.; Hochreiter, S. Fast and accurate deep network learning by exponential linear units (elus). arXiv 2015, arXiv:1511.07289. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Dice, L.R. Measures of the amount of ecologic association between species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Dubuisson, M.; Jain, A. A modified Hausdorff distance for object matching. In Proceedings of the 12th International Conference on Pattern Recognition, Jerusalem, Israel, 9–13 October 1994; pp. 566–568. [Google Scholar]
- Sherer, M.V.; Lin, D.; Elguindi, S.; Duke, S.; Tan, L.T.; Cacicedo, J.; Dahele, M.; Gillespie, E.F. Metrics to evaluate the performance of auto-segmentation for radiation treatment planning: A critical review. Radiother. Oncol. 2021, 160, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Rava, P.; Rosenberg, J.; Jamorabo, D.; Sioshansi, S.; DiPetrillo, T.; Wazer, D.E.; Hepel, J. Feasibility and safety of cavity-directed stereotactic radiosurgery for brain metastases at a high-volume medical center. Adv. Radiat. Oncol. 2016, 1, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, J.; Yoo, E.; Lee, H.; Chang, J.H.; Kim, E.Y. Detection of small metastatic brain tumors: Comparison of 3D contrast-enhanced whole-brain black-blood imaging and MP-RAGE imaging. Investig. Radiol. 2012, 47, 136–141. [Google Scholar] [CrossRef]
- Jun, Y.; Eo, T.; Kim, T.; Shin, H.; Hwang, D.; Bae, S.H.; Park, Y.W.; Lee, H.J.; Choi, B.W.; Ahn, S.S. Deep-learned 3D black-blood imaging using automatic labelling technique and 3D convolutional neural networks for detecting metastatic brain tumors. Sci. Rep. 2018, 8, 9450. [Google Scholar]
- Fennema-Notestine, C.; Ozyurt, I.B.; Clark, C.P.; Morris, S.; Bischoff-Grethe, A.; Bondi, M.W.; Jernigan, T.L.; Fischl, B.; Segonne, F.; Shattuck, D.W.; et al. Quantitative evaluation of automated skull-stripping methods applied to contemporary and legacy images: Effects of diagnosis, bias correction, and slice location. Hum. Brain Mapp. 2006, 27, 99–113. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (65) | Train (+Valid) Set (53) | Test Set (12) | p Value |
|---|---|---|---|---|
| Age (years) | ||||
| Median (range) | 63 (19–87) | 63 (19–87) | 63 (26–81) | 0.869 |
| Sex | 1 | |||
| Male | 35 (54) | 29 (55) | 6 (50) | |
| Female | 30 (46) | 24 (45) | 6 (50) | |
| Primary cancer | 0.604 | |||
| Lung | 56 (86) | 45 (85) | 11 (92) | |
| Breast | 4 (6) | 4 (7) | - | |
| Others | 5 (8) | 4 (8) | 1 (8) | |
| Total number of BM | 603 | 545 | 58 | |
| >0.04 cc | 458 (76) | 414 (76) | 44 (76) | |
| ≤0.04 cc | 145 (24) | 131 (24) | 14 (24) | |
| Volumes of BM | ||||
| Max | 67.426 | 67.426 | 1.219 | |
| Min | 0.02 | 0.02 | 0.021 | |
| Median | 0.074 | 0.074 | 0.068 | |
| Mean | 0.552 | 0.592 | 0.158 |
| No. of BM Per Patient | No. of Patients | Sensitivity [%] |
|---|---|---|
| ≥10 | 3 | 93.5 |
| <10 | 9 | 100 |
| Total | 12 | 96.6 |
| Volume (cc) | No. of BM | Sensitivity [%] | No. of FPs | DICE | DWD | HD95 [mm] |
|---|---|---|---|---|---|---|
| >0.1 | 24 | 100 | 4 | 0.64 | 0.8 | 2.502 |
| ≤0.1 | 34 | 94.1 | 11 | 0.48 | 0.72 | 1.724 * |
| 0.08–0.1 | 1 | 100 | 2 | 0.82 | 0.9 | 1 |
| 0.06–0.08 | 10 | 100 | 2 | 0.53 | 0.78 | 1.979 |
| 0.04–0.06 | 9 | 100 | 2 | 0.56 | 0.75 | 1.608 |
| 0.02–0.04 | 14 | 85.7 | 5 | 0.38 | 0.63 | 1.689 * |
| Total | 58 | 96.6 | 15 | 0.55 | 0.75 | 2.057 |
| Authors | Median Vol. of BM [cc] | Sensitivity [%] | Avg. No. of FPs | DICE |
|---|---|---|---|---|
| Losch, M. et al. | NA | 82.8 | 7.7 | 0.66 |
| Charron, O. et al. | 0.5 | 93 | 4.4 | 0.79 |
| Xue, J. et al. | 2.22 | 96 | NA | 0.85 |
| Grovik, E. et al | NA | 83 | 3.4 | 0.79 |
| Dikici, E. et al. | 0.16 | 90 | 9.12 | NA |
| Bousabarah, K. et al. | 0.31 (train)/0.47 (test) | NA | NA | 0.71 |
| Our study | 0.074 (train)/0.068 (test) | 96.6 | 1.25 | 0.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, S.K.; Kim, T.H.; Chun, J.; Choi, B.S.; Kim, H.; Yang, S.; Yoon, H.I.; Kim, J.S. Deep-Learning-Based Automatic Detection and Segmentation of Brain Metastases with Small Volume for Stereotactic Ablative Radiotherapy. Cancers 2022, 14, 2555. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102555
Yoo SK, Kim TH, Chun J, Choi BS, Kim H, Yang S, Yoon HI, Kim JS. Deep-Learning-Based Automatic Detection and Segmentation of Brain Metastases with Small Volume for Stereotactic Ablative Radiotherapy. Cancers. 2022; 14(10):2555. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102555
Chicago/Turabian StyleYoo, Sang Kyun, Tae Hyung Kim, Jaehee Chun, Byong Su Choi, Hojin Kim, Sejung Yang, Hong In Yoon, and Jin Sung Kim. 2022. "Deep-Learning-Based Automatic Detection and Segmentation of Brain Metastases with Small Volume for Stereotactic Ablative Radiotherapy" Cancers 14, no. 10: 2555. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102555