
Viral and Genomic Drivers of Squamous Cell Neoplasms Arising in the Lacrimal Drainage System

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
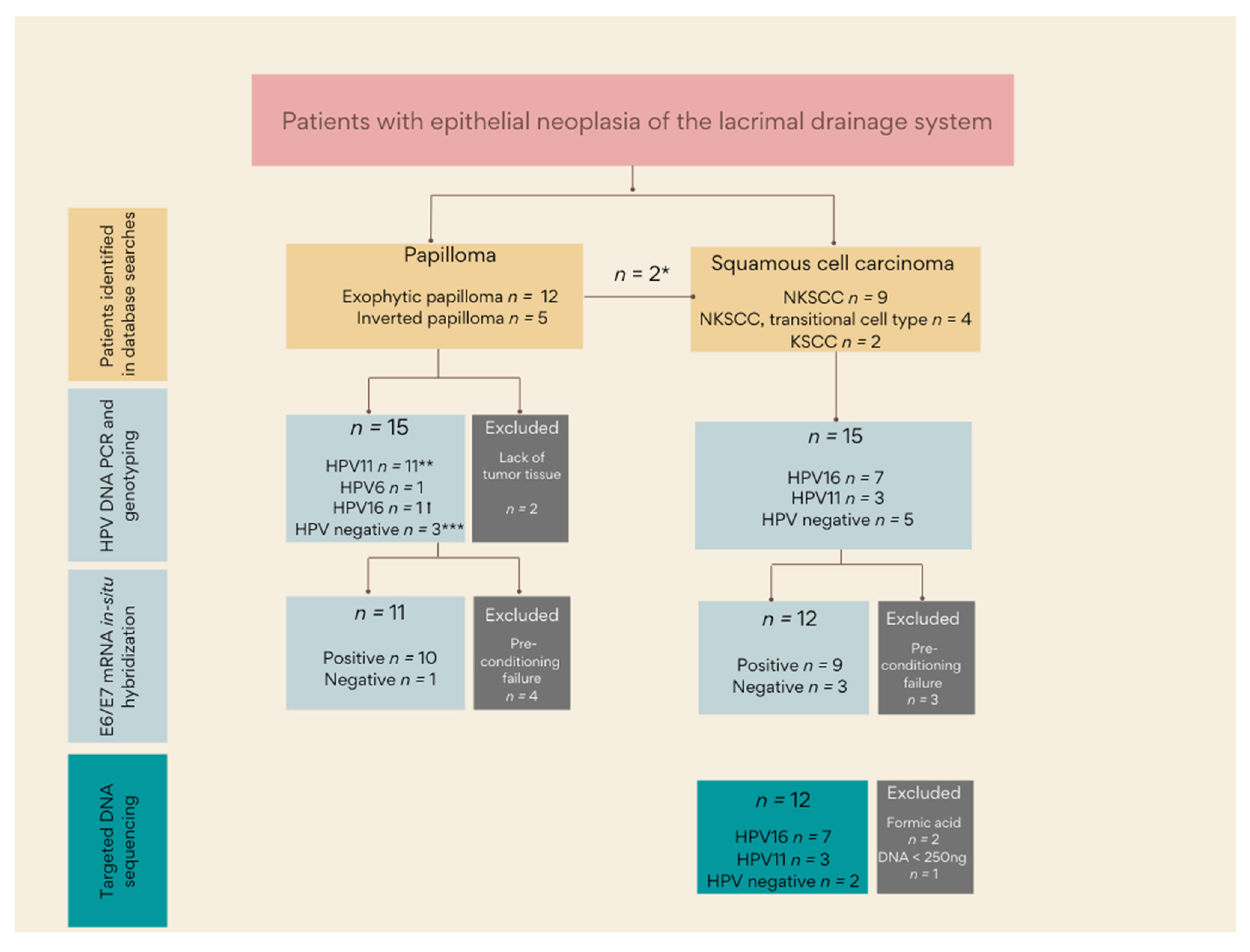
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. DNA Extraction
2.2.2. HPV DNA PCR and HPV Genotyping
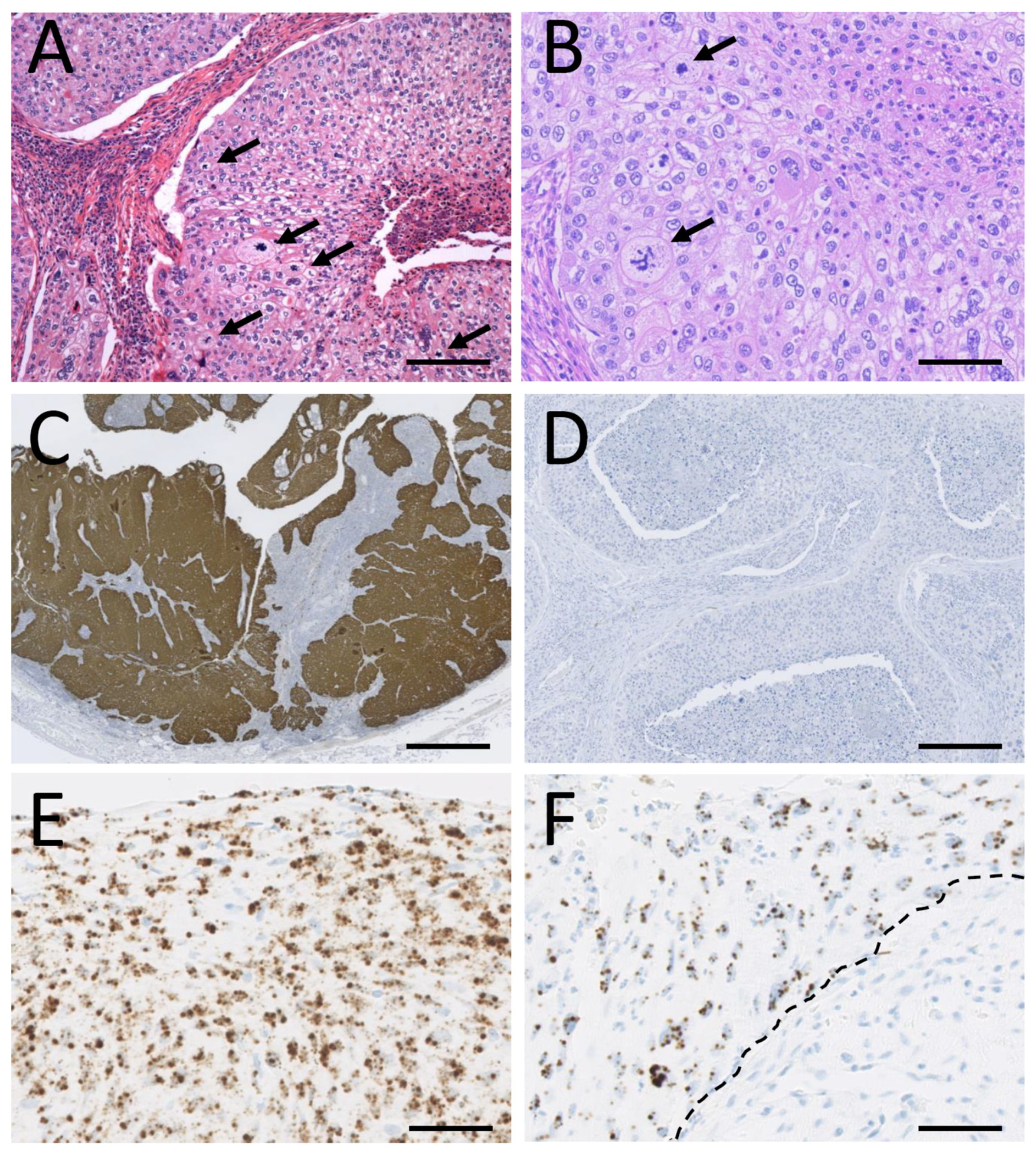
2.2.3. HPV E6/E7 mRNA In-Situ Hybridization
2.2.4. Immunohistochemistry
2.2.5. DNA Sequencing
2.2.6. Bioinformatic Analysis and Annotation
2.2.7. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Human Papillomavirus in LDS Papillomas and Squamous Cell Carcinomas
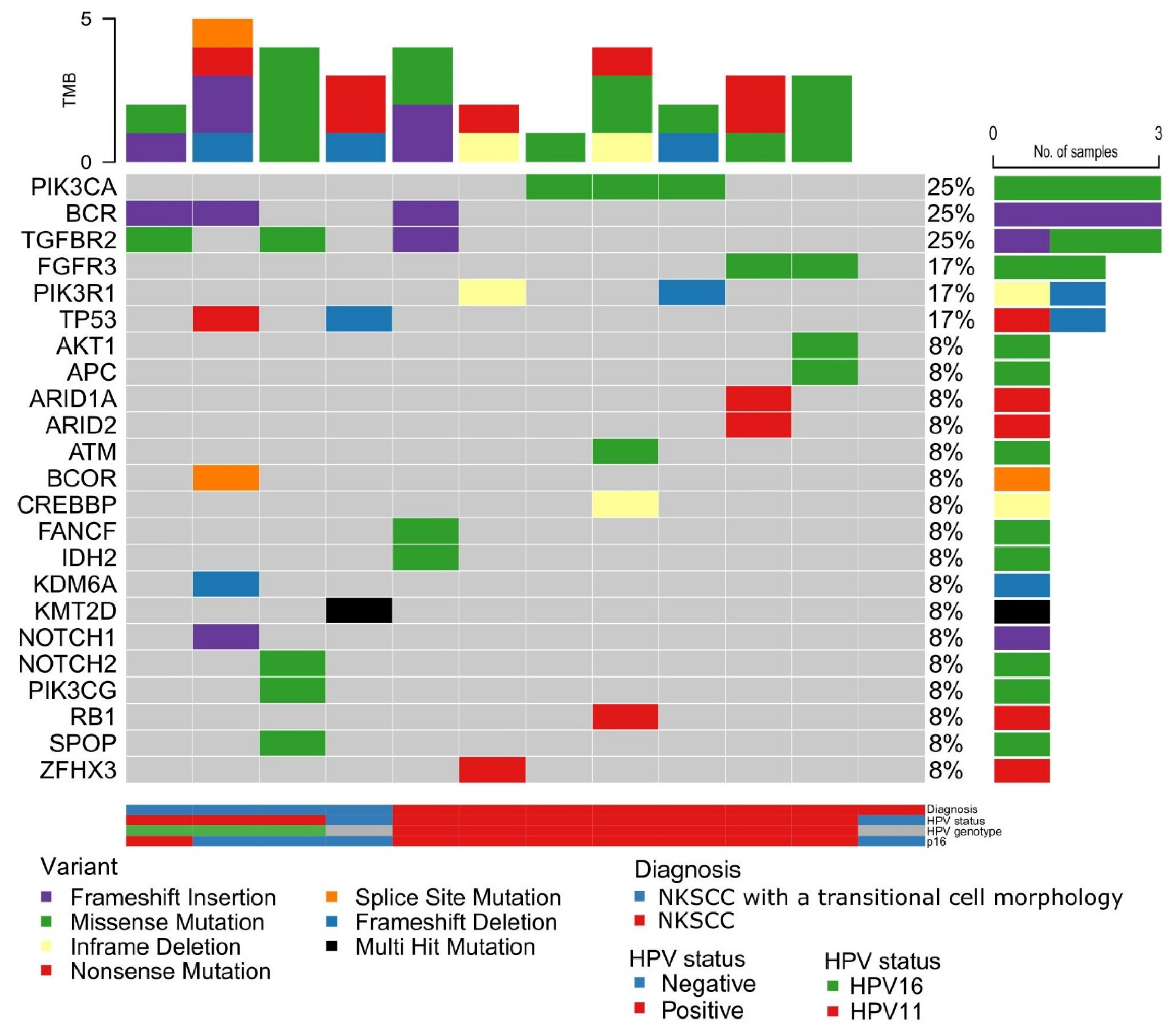
3.3. Genomic Aberrations in LDS Squamous Cell Carcinoma
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramberg, I.; Toft, P.B.; Heegaard, S. Carcinomas of the lacrimal drainage system. Surv. Ophthalmol. 2020, 6, 691–707. [Google Scholar] [CrossRef] [PubMed]
- Afrogheh, A.; Jakobiec, F.; Hammon, R.; Grossniklaus, H.; Rocco, J.; Lindeman, N.; Sadow, P.; Faquin, W. Evaluation for high-risk HPV in squamous cell carcinomas and precursor lesions arising in the conjunctiva and lacrimal sac. Am. J. Surg. Pathol. 2016, 40, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Madreperla, S.A.; Green, W.R.; Daniel, R.; Shah, K.V. Human papillomavirus in primary epithelial tumors of the lacrimal sac. Ophthalmology 1993, 100, 569–573. [Google Scholar] [CrossRef]
- Sjö, N.C.; von Buchwald, C.; Cassonnet, P.; Flamant, P.; Heegaard, S.; Norrild, B.; Prause, J.U.; Orth, G. Human papillomavirus: Cause of epithelial lacrimal sac neoplasia? Acta Ophthalmol. 2007, 85, 551–556. [Google Scholar] [CrossRef]
- Hongo, T.; Yamamoto, H.; Tanabe, M.; Yasumatsu, R.; Kuga, R.; Miyazaki, Y.; Jiromaru, R.; Hashimoto, K.; Tateishi, Y.; Sonoda, K.H.; et al. High-risk HPV-related squamous cell carcinoma in the conjunctiva and lacrimal sac: Clinicopathologic characteristics and diagnostic utility of p16 and Rb immunohistochemistry. Am. J. Surg. Pathol. 2022. [Google Scholar] [CrossRef]
- Jones, H.; Gane, S.; Rimmer, J.; Cuschieri, K.; Lund, V.J. HPV may not play a role in all lacrimal transitional cell papilloma. Rhinology 2020. [Google Scholar] [CrossRef]
- Ramberg, I.; Vieira, F.G.; Toft, P.B.; von Buchwald, C.; Funding, M.; Nielsen, F.C.; Heegaard, S. Genomic Alterations in Human Papillomavirus-Positive and -Negative Conjunctival Squamous Cell Carcinomas. Investig. Ophthalmol. Vis. Sci. 2021, 62, 11. [Google Scholar] [CrossRef]
- Ramberg, I.; Toft, P.B.; Georgsen, J.B.; Siersma, V.D.; Funding, M.; Jensen, D.H.; Von Buchwald, C.; Heegaard, S. Conjunctival intraepithelial neoplasia and carcinoma: Distinct clinical and histological features in relation to human papilloma virus status. Br. J. Ophthalmol. 2019, 105, 878–883. [Google Scholar] [CrossRef]
- Andrew, S. FastQC: A Quality Control Tool for High Throughput Sequence Data. Available online: http://www.bioinforma-427tics.babraham.ac.uk/projects/fastqc (accessed on 20 January 2022).
- Pedersen, B.S.; Quinlan, A.R. Mosdepth: Quick coverage calculation for genomes and exomes. Bioinformatics 2018, 34, 867–868. [Google Scholar] [CrossRef]
- Van der Auwera, G.A.; O’Connor, B.D. Genomics in the Cloud: Using Docker, GATK, and WDL in Terra, 1st ed.; O’Reilly Media: Sebastopol, CA, USA, 2020. [Google Scholar]
- Karczewski, K.J.; Francioli, L.C.; Tiao, G.; Cummings, B.B.; Alföldi, J.; Wang, Q.; Collins, R.L.; Laricchia, K.M.; Ganna, A.; Birnbaum, D.P.; et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature 2020, 581, 434–443. [Google Scholar] [CrossRef]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci. Signal. 2013, 6, pl1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjö, N.C.; von Buchwald, C.; Cassonnet, P.; Norrild, B.; Prause, J.U.; Vinding, T.; Heegaard, S. Human papillomavirus in normal conjunctival tissue and in conjunctival papilloma: Types and frequencies in a large series. Br. J. Ophthalmol. 2007, 91, 1014–1015. [Google Scholar] [CrossRef] [Green Version]
- Bishop, J.A. OSPs and ESPs and ISPs, Oh My! An Update on Sinonasal (Schneiderian) Papillomas. Head Neck Pathol. 2017, 11, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Yanofsky, V.R.; Patel, R.V.; Goldenberg, G. Genital warts: A comprehensive review. J. Clin. Aesthetic Dermatol. 2012, 5, 25–36. [Google Scholar]
- Lisan, Q.; Moya-Plana, A.; Bonfils, P. Association of krouse classification for sinonasal inverted papilloma with recurrence: A systematic review and meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 1104–1110. [Google Scholar] [CrossRef]
- Wang, J.; Ford, J.; Esmaeli, B.; Langer, P.; Esmaili, N.; Griepentrog, G.J.; Couch, S.M.; Nguyen, J.; Gold, K.G.; Duerksen, K.; et al. Inverted papilloma of the orbit and nasolacrimal system. Ophthalmic Plast. Reconstr. Surg. 2021, 37, 161–167. [Google Scholar] [CrossRef]
- McCormick, J.P.; Suh, J.D.; Lee, J.T.; Wells, C.; Wang, M.B. Role of High-Risk HPV Detected by PCR in Malignant Sinonasal Inverted Papilloma: A Meta-Analysis. Laryngoscope 2021, 132, 926–932. [Google Scholar] [CrossRef]
- Raemdonck, T.Y.; Van den Broecke, C.M.; Claerhout, I.; Decock, C.E. Inverted papilloma arising primarily from the lacrimal sac. Orbit 2009, 28, 181–184. [Google Scholar] [CrossRef]
- Bedard, M.C.; de Alarcon, A.; Kou, Y.F.; Lee, D.; Sestito, A.; Duggins, A.L.; Brusadelli, M.; Lane, A.; Wikenheiser-Brokamp, K.A.; Wells, S.I.; et al. HPV strain predicts severity of juvenile-onset recurrent respiratory papillomatosis with implications for disease screening. Cancers 2021, 13, 2556. [Google Scholar] [CrossRef]
- Gerein, V.; Rastorguev, E.; Gerein, J.; Draf, W.; Schirren, J. Incidence, age at onset, and potential reasons of malignant transformation in recurrent respiratory papillomatosis patients: 20 years experience. Otolaryngol. Head Neck Surg. 2005, 132, 392–394. [Google Scholar] [CrossRef] [PubMed]
- Egawa, N.; Egawa, K.; Griffin, H.; Doorbar, J. Human Papillomaviruses; Epithelial Tropisms, and the Development of Neoplasia. Viruses 2015, 7, 3863–3890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Agency for Research on Cancer. Monographs on the Evaluation of Carcinogenic Risks to Humans: Biological Agents; Cancer—International Agency for Research on Cancer, Ed.; IARC: Lyon, France, 2012; Volume 100B, pp. 255–296. [Google Scholar]
- Bosch, F.X.; Lorincz, A.; Muñoz, N.; Meijer, C.J.; Shah, K.V. The causal relation between human papillomavirus and cervical cancer. J. Clin. Pathol. 2002, 55, 244–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef] [Green Version]
- Pal, A.; Kundu, R. Human Papillomavirus E6 and E7: The Cervical Cancer Hallmarks and Targets for Therapy. Front. Microbiol. 2019, 10, 3116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaacson Wechsler, E.; Wang, Q.; Roberts, I.; Pagliarulo, E.; Jackson, D.; Untersperger, C.; Coleman, N.; Griffin, H.; Doorbar, J. Reconstruction of human papillomavirus type 16-mediated early-stage neoplasia implicates E6/E7 deregulation and the loss of contact inhibition in neoplastic progression. J. Virol. 2012, 86, 6358–6364. [Google Scholar] [CrossRef] [Green Version]
- The Cancer Genome Atlas Research Network. Integrated genomic and molecular characterization of cervical cancer. Nature 2017, 543, 378–384. [Google Scholar] [CrossRef]
- Bersani, C.; Sivars, L.; Haeggblom, L.; DiLorenzo, S.; Mints, M.; Ährlund-Richter, A.; Tertipis, N.; Munck-Wikland, E.; Näsman, A.; Ramqvist, T.; et al. Targeted sequencing of tonsillar and base of tongue cancer and human papillomavirus positive unknown primary of the head and neck reveals prognostic effects of mutated FGFR3. Oncotarget 2017, 8, 35339–35350. [Google Scholar] [CrossRef]
- Näsman, A.; Holzhauser, S.; Kostopoulou, O.N.; Zupancic, M.; Ährlund-Richter, A.; Du, J.; Dalianis, T. Prognostic markers and driver genes and options for targeted therapy in human-papillomavirus-positive tonsillar and base-of-tongue squamous cell carcinoma. Viruses 2021, 13, 910. [Google Scholar] [CrossRef]
- Hongo, T.; Yamamoto, H.; Jiromaru, R.; Nozaki, Y.; Yasumatsu, R.; Hashimoto, K.; Yoneda, R.; Sugii, A.; Taguchi, K.; Masuda, M.; et al. Clinicopathologic Significance of EGFR Mutation and HPV Infection in Sinonasal Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2021, 45, 108–118. [Google Scholar] [CrossRef]
- Taverna, C.; Agaimy, A.; Franchi, A. Towards a Molecular Classification of Sinonasal Carcinomas: Clinical Implications and Opportunities. Cancers 2022, 14, 1463. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HPV11-Positive Carcinoma (n = 3) | HPV-16 Positive Carcinoma (n = 7) | HPV-Negative Carcinoma (n = 5) | Total (n = 15) | |
|---|---|---|---|---|
| Age (years), median (range) | 46 (34–47) | 67 (59–82) | 52 (49–87) | 64 (34–87) |
| Gender | 1F/2M | 2F/5M | 3F/2M | 6F/9M |
| Previous history of LDS disease, n (%) | 2 (67) | 1 (14) | 2 (40) | 5 (33) |
| Diagnosis | ||||
| NKSCC, n (%) | 3 (100) | 7 (100) | 3 (60) | 13 (87) |
| KSCC, n (%) | 0 (0) | 0 (0) | 2 (40) | 2 (13) |
| Local invasion other than nasolacrimal duct, n (%) * | ||||
| Nasolacrimal duct | 1 (50) | 3 (42) | 0 (0) | 4 (31) |
| Orbit | 1 (50) | 3 (42) | 2 (59) | 6 (56) |
| Ethmoid cells | 0 (0) | 2 (29) | 1 (25) | 3 (23) |
| Maxillary sinus | 1 (50) | 2 (29) | 1 (25) | 4 (31) |
| Nasal cavity | 0 (0) | 0 (0) | 1 (25) | 1 (8) |
| Eyelids | 0 (0) | 1 (14) | 1 (25) | 2 (15) |
| Lacrimal bone | 0 (0) | 1 (14) | 0 (0) | 1 (8) |
| Positive surgical margins ** | 3 (100) | 3 (43) | 4 (100) | 10 (71) |
| Adjuvant therapy, n (%) ** | ||||
| Radiotherapy | 2 (100) | 3 (60) | 3 (100) | 8 (80) |
| Cisplatin | 0 (0) | 0 (0) | 1 (33) | 1 (10) |
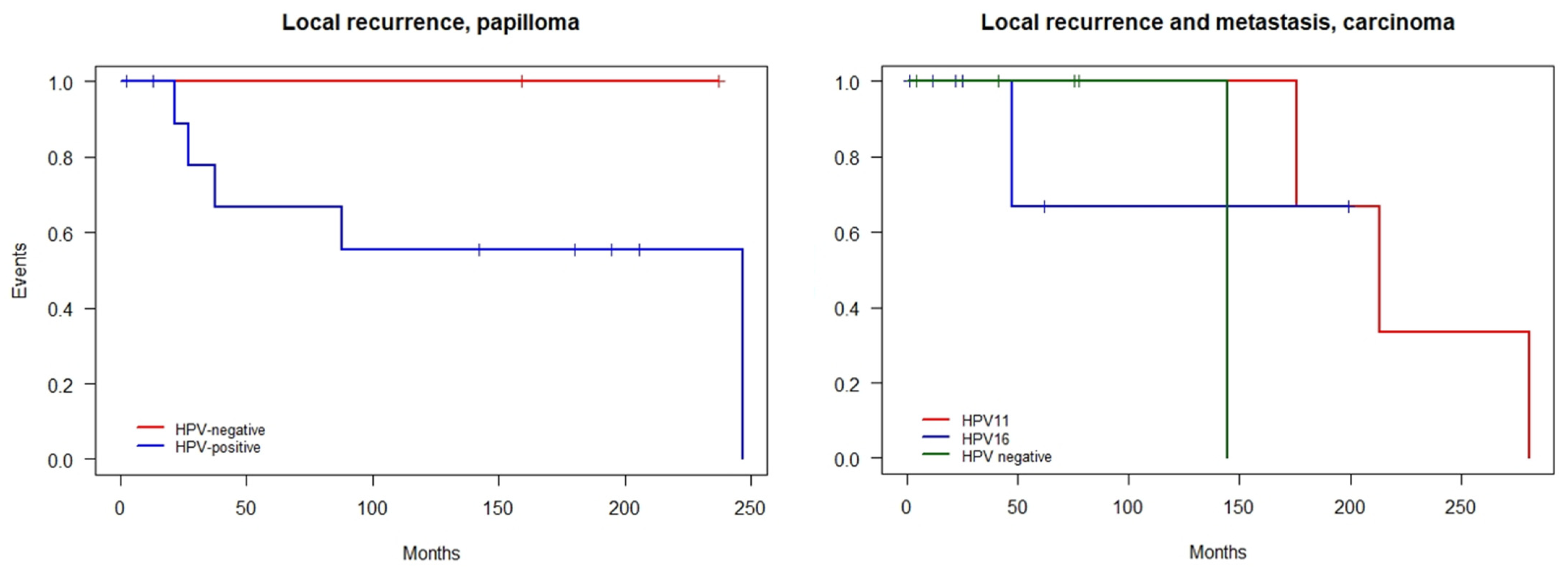
| Local recurrence, n (%) | 2 (67) | 0 (0) | 0 (0) | 2 (13) |
| Metastasis, n (%) | ||||
| Lymph nodes | 2 (67) | 1 (14) | 0 (0) | 3 (20) |
| Extranodal tissue | 0 (0) | 1 (14) | 0 (0) | 1 (7) |
| Follow-up (months), median (range) | 213.2 (175.6–280.6) | 25.1 (1.3–199.3) | 75.3 (4.3–144.7) | 75.3 (1.3–280.6) |
| LDS Papilloma | LDS Carcinoma | |
|---|---|---|
| Number of cases | 17 | 15 |
| Previous or concomitant HPV-related head-and-neck neoplasm, n (%) | 7/17 (41) | 4/15 (27) |
| HPV-positivity (DNA and mRNA), n (%) | 12/15 (80) | 10/15 (67) |
| HPV genotypes | HPV6, 11, 16 | HPV11, 16 |
| P16 positivity, n (%) | 4/15 (27) | 9/15 (60) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramberg, I.; Vieira, F.G.; Toft, P.B.; von Buchwald, C.; Heegaard, S. Viral and Genomic Drivers of Squamous Cell Neoplasms Arising in the Lacrimal Drainage System. Cancers 2022, 14, 2558. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102558
Ramberg I, Vieira FG, Toft PB, von Buchwald C, Heegaard S. Viral and Genomic Drivers of Squamous Cell Neoplasms Arising in the Lacrimal Drainage System. Cancers. 2022; 14(10):2558. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102558
Chicago/Turabian StyleRamberg, Ingvild, Filipe Garrett Vieira, Peter Bjerre Toft, Christian von Buchwald, and Steffen Heegaard. 2022. "Viral and Genomic Drivers of Squamous Cell Neoplasms Arising in the Lacrimal Drainage System" Cancers 14, no. 10: 2558. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102558