
The Effect of Adjuvant Chemotherapy on Localized Extraskeletal Osteosarcoma: A Systematic Review

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
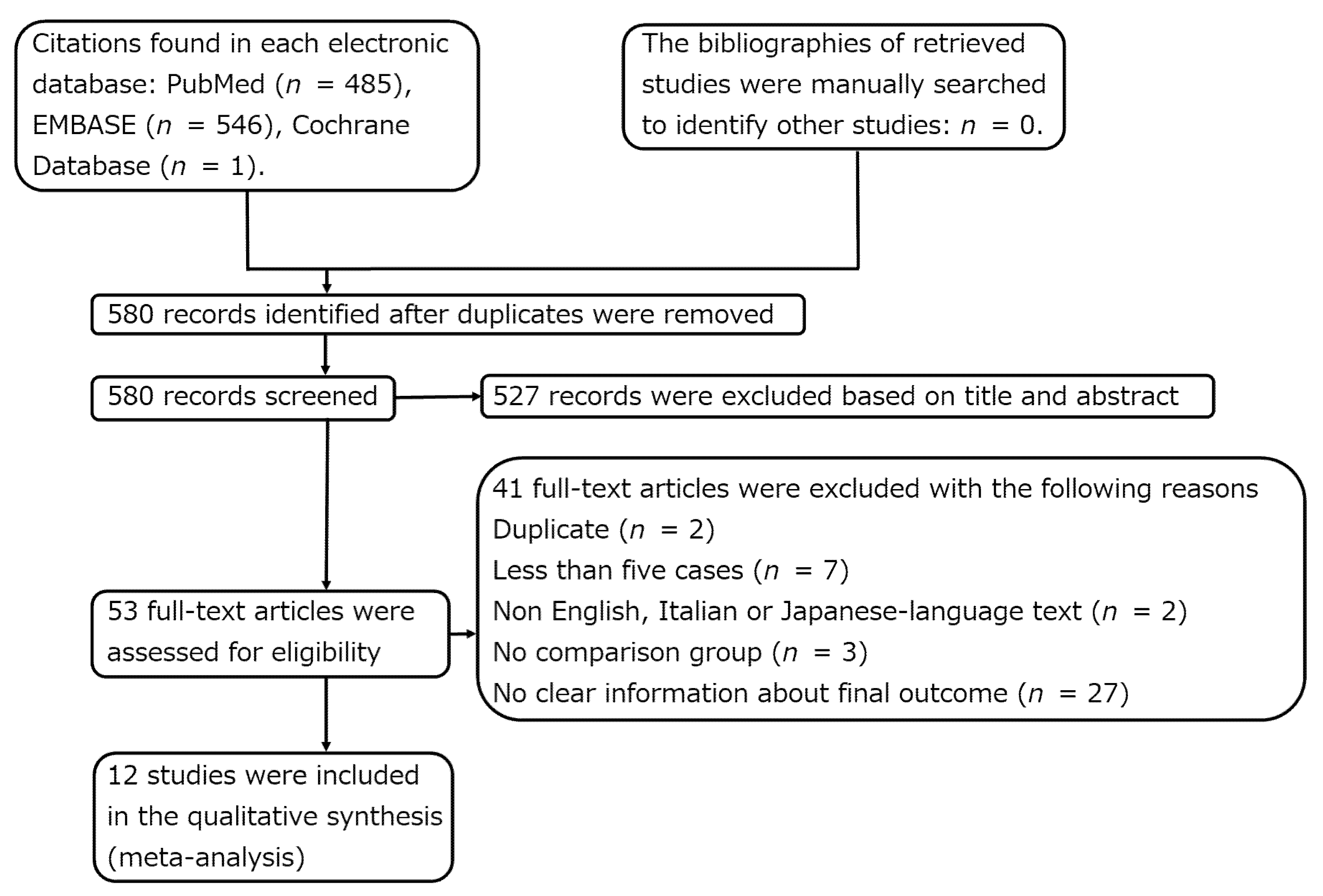
2.2. Literature Search and Study Selection
2.3. Data Collection and Presentation
2.4. Data Summary, Synthesis, and Meta-Analysis
2.5. Assessment of Methodological Quality
2.6. Search Results
2.7. Demographic Data and Ratio of the Patients Who Underwent Surgery and Adjuvant Chemotherapy or Surgery Alone
2.8. Methodological Quality of the Included Studies
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yamashita, K.; Hameed, M. Extraskeletal osteosarcoma. In WHO Classification of Tumours, 5th ed.; Soft Tissue and Bone Tumours; The WHO Classification of Tumours Editorial Board; International Arctic Research Center: Lyon, France, 2020; pp. 224–225. [Google Scholar]
- Longhi, A.; Bielack, S.S.; Grimer, R.; Whelan, J.; Windhager, R.; Leithner, A.; Gronchi, A.; Biau, D.; Jutte, P.; Krieg, A.H.; et al. Extraskeletal Osteosarcoma: A European Musculoskeletal Oncology Society Study on 266 Patients. Eur. J. Cancer 2017, 74, 9–16. [Google Scholar] [CrossRef]
- Heng, M.; Gupta, A.; Chung, P.W.; Healey, J.H.; Vaynrub, M.; Rose, P.S.; Houdek, M.T.; Lin, P.P.; Bishop, A.J.; Hornicek, F.J.; et al. The Role of Chemotherapy and Radiotherapy in Localized Extraskeletal Osteosarcoma. Eur. J. Cancer 2020, 125, 130–141. [Google Scholar] [CrossRef]
- Kattepur, A.K.; Gulia, A.; Jones, R.L.; Rastogi, S. Extraskeletal Osteosarcomas: Current Update. Future Oncol. 2021, 17, 825–835. [Google Scholar] [CrossRef]
- Gronchi, A.; Miah, A.B.; Dei Tos, A.P.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.Y.; Bolle, S.; et al. Soft Tissue and Visceral Sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2021, 32, 1348–1365. [Google Scholar] [CrossRef]
- von Mehren, M.; Randall, R.L.; Benjamin, R.S.; Boles, S.; Bui, M.M.; Conrad, E.U.; Ganjoo, K.N.; George, S.; Gonzalez, R.J.; Heslin, M.J.; et al. Soft Tissue Sarcoma, Version 2.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2016, 14, 758–786. [Google Scholar] [CrossRef] [Green Version]
- Paludo, J.; Fritchie, K.; Haddox, C.L.; Rose, P.S.; Arndt, C.A.S.; Marks, R.S.; Galanis, E.; Okuno, S.H.; Robinson, S.I. Extraskeletal Osteosarcoma: Outcomes and the Role of Chemotherapy. Am. J. Clin. Oncol. 2018, 41, 832–837. [Google Scholar] [CrossRef]
- Wakamatsu, T.; Kakunaga, S.; Takenaka, S.; Outani, H.; Hamada, K.; Imura, Y.; Hori, Y.; Naka, N.; Kudawara, I.; Yoshikawa, H.; et al. Prognostic Implication of Adjuvant/Neoadjuvant Chemotherapy Consisting of Doxorubicin and Ifosfamide in Patients with Extraskeletal Osteosarcoma. Int. J. Clin. Oncol. 2019, 24, 1311–1319. [Google Scholar] [CrossRef]
- Ahmad, S.A.; Patel, S.R.; Ballo, M.T.; Baker, T.P.; Yasko, A.W.; Wang, X.; Feig, B.W.; Hunt, K.K.; Lin, P.P.; Weber, K.L.; et al. Extraosseous Osteosarcoma: Response to Treatment and Long-Term Outcome. J. Clin. Oncol. 2002, 20, 521–527. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Bishop, A.J.; Livingston, J.A.; Araujo, D.M.; Moon, B.S.; Patel, S.; Wang, W.-L.; Lazar, A.J.; Roland, C.L.; Guadagnolo, B.A. Extraskeletal Osteosarcomas: A Case Made for Combined Modality Local Therapy with Radiation and Surgery. Am. J. Clin. Oncol. 2019, 42, 238–242. [Google Scholar] [CrossRef]
- Goldstein-Jackson, S.Y.; Gosheger, G.; Delling, G.; Berdel, W.E.; Exner, G.U.; Jundt, G.; Machatschek, J.-N.; Zoubek, A.; Jürgens, H.; Bielack, S.S.; et al. Extraskeletal Osteosarcoma Has a Favourable Prognosis When Treated like Conventional Osteosarcoma. J. Cancer Res. Clin. Oncol. 2005, 131, 520–526. [Google Scholar] [CrossRef]
- Lee, J.S.; Fetsch, J.F.; Wasdhal, D.A.; Lee, B.P.; Pritchard, D.J.; Nascimento, A.G. A Review of 40 Patients with Extraskeletal Osteosarcoma. Cancer 1995, 76, 2253–2259. [Google Scholar] [CrossRef]
- Lee, S.; Lee, M.R.; Lee, S.J.; Ahn, H.K.; Yi, J.; Yi, S.Y.; Seo, S.W.; Sung, K.-S.; Park, J.O.; Lee, J. Extraosseous Osteosarcoma: Single Institutional Experience in Korea. Asia Pac. J. Clin. Oncol. 2010, 6, 126–129. [Google Scholar] [CrossRef]
- Liao, Z.; Qiu, M.; Yang, J.; Yang, Y.; Zhu, L.; Yang, B.; Bai, X.; Xing, P.; Zhang, J.; Xing, R.; et al. Outcomes of Surgery and/or Combination Chemotherapy for Extraskeletal Osteosarcoma: A Single-Center Retrospective Study from China. Sci. Rep. 2019, 9, 4816. [Google Scholar] [CrossRef]
- Lidang Jensen, M.; Schumacher, B.; Myhre Jensen, O.; Steen Nielsen, O.; Keller, J. Extraskeletal Osteosarcomas: A Clinicopathologic Study of 25 Cases. Am. J. Surg. Pathol. 1998, 22, 588–594. [Google Scholar] [CrossRef]
- Makise, N.; Sekimizu, M.; Kubo, T.; Wakai, S.; Watanabe, S.-I.; Kato, T.; Kinoshita, T.; Hiraoka, N.; Fukayama, M.; Kawai, A.; et al. Extraskeletal Osteosarcoma: MDM2 and H3K27me3 Analysis of 19 Cases Suggest Disease Heterogeneity. Histopathology 2018, 73, 147–156. [Google Scholar] [CrossRef]
- Sio, T.T.; Vu, C.C.; Sohawon, S.; Van Houtte, P.; Thariat, J.; Novotny, P.J.; Miller, R.C.; Bar-Sela, G. Extraskeletal Osteosarcoma: An International Rare Cancer Network Study. Am. J. Clin. Oncol. 2016, 39, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Torigoe, T.; Yazawa, Y.; Takagi, T.; Terakado, A.; Kurosawa, H. Extraskeletal Osteosarcoma in Japan: Multiinstitutional Study of 20 Patients from the Japanese Musculoskeletal Oncology Group. J. Orthop. Sci. 2007, 12, 424–429. [Google Scholar] [CrossRef]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.-J.; Sheen, S.-S.; Hahn, S.; Jang, B.-H.; Son, H.-J. Testing a Tool for Assessing the Risk of Bias for Nonrandomized Studies Showed Moderate Reliability and Promising Validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [CrossRef]
- Qi, L.; Wan, L.; Ren, X.; Zhang, W.; Tu, C.; Li, Z. The Role of Chemotherapy in Extraskeletal Osteosarcoma: A Propensity Score Analysis of the Surveillance Epidemiology and End Results (SEER) Database. Med. Sci. Monit. 2020, 26, e925107. [Google Scholar] [CrossRef]
- Thampi, S.; Matthay, K.K.; Boscardin, W.J.; Goldsby, R.; DuBois, S.G. Clinical Features and Outcomes Differ between Skeletal and Extraskeletal Osteosarcoma. Sarcoma 2014, 2014, 902620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Z.; Patel, S.; Lewis, V.O.; Guadagnolo, B.A.; Lin, P.P. Should High-Grade Extraosseous Osteosarcoma Be Treated with Multimodality Therapy Like Other Soft Tissue Sarcomas? Clin. Orthop. Relat. Res. 2015, 473, 3604–3611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, L.E.; Healey, J.H.; Kuk, D.; Brennan, M.F. Analysis of Outcomes in Extraskeletal Osteosarcoma: A Review of Fifty-Three Cases. J. Bone Jt. Surg. Am. 2014, 96, e2. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Miao, R.; Jacobson, A.; Harmon, D.; Choy, E.; Hornicek, F.; Raskin, K.; Chebib, I.; DeLaney, T.F.; Chen, Y.-L.E. Extraskeletal Osteosarcoma: A Large Series Treated at a Single Institution. Rare Tumors 2018, 10, 2036361317749651. [Google Scholar] [CrossRef] [Green Version]
- McCarter, M.D.; Lewis, J.J.; Antonescu, C.R.; Brennan, M.F. Extraskeletal Osteosarcoma: Analysis of Outcome of a Rare Neoplasm. Sarcoma 2000, 4, 119–123. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Type of Study | Follow-Up (Years) | Total Number of Patients with Localized ESOS | Number of Patients in the Surgery and Adjuvant Chemotherapy Group | Number of Patients who Were Disease-Free for 5 Years in the Surgery and Adjuvant Chemotherapy Group | Number of Patients in the Surgery Group | Number of Patients who Were Disease-Free for 5 Years in the Surgery Group |
|---|---|---|---|---|---|---|---|---|
| Bishop et al. [11] | 2019 | SR | Median, 10 | 21 | 7 | 3 | 14 | 9 |
| Goldstein-Jackson et al. [12] | 2005 | MP | Median, 3.2 | 16 | 15 | 5 | 1 | 0 |
| Heng et al. [3] | 2020 | MR | Median, 3 | 368 | 178 | 91 | 190 | 95 |
| Lee et al. [13] | 1995 | SR | Mean, 5.9 | 18 | 2 | 0 | 16 | 4 |
| Lee et al. [14] | 2010 | SR | NR | 8 | 1 | 0 | 7 | 0 |
| Liao et al. [15] | 2019 | SR | Median, 3 | 19 | 15 | 4 | 4 | 1 |
| Lidang Jensen et al. [16] | 1998 | SR | Median, 1.3 | 24 | 5 | 1 | 19 | 2 |
| Longhi et al. [2] | 2017 | MR | Median, 1.9 | 207 | 121 | 67 | 86 | 23 |
| Makise et al. [17] | 2018 | SR | Median, 2.6 | 17 | 9 | 1 | 8 | 3 |
| Sio et al. [18] | 2016 | MR | Median, 3.8 | 33 | 13 | 7 | 20 | 11 |
| Torigoe et al. [19] | 2007 | MR | Mean, 3.8 | 17 | 13 | 3 | 4 | 2 |
| Wakamatsu et al. [8] | 2019 | MR | Median, 50.5 | 13 | 11 | 5 | 2 | 0 |
| Study | Percentage of Male Patients (Surgery + Adj Chemo vs. Surgery) | Age (Surgery + Adj Chemo vs. Surgery) | Percentage of Deeply Located Tumors (Surgery + Adj Chemo vs. Surgery) | Percentage of Tumors Located in the Trunk (Surgery + Adj Chemo vs. Surgery) | Tumor Size (cm) (Surgery + Adj Chemo vs. Surgery) | Proportion of Patient with an R0 Surgical Margin (Surgery + Adj Chemo vs. Surgery) | Percentage of Patients who Received Adjuvant Radiotherapy (Surgery + Adj Chemo vs. Surgery) | Histological Grade (Surgery + Adj Chemo vs. Surgery) | Chemotherapy Regimen | Assessment of Histological Response to Preoperative Chemotherapy |
|---|---|---|---|---|---|---|---|---|---|---|
| Bishop et al. [11] | NR | NR | NR | NR | Larger tumor of >5 cm was associated with chemotherapy use. | NR | NR | NR | NR | 99% or more necrosis: 50% |
| Goldstein-Jackson et al. [12] | NR | NR | NR | 20% vs. 100% | NR | 93% vs. 0% | NR | NR | DOX, CDDP, IFO, MTX, VP16, CBDCA | NR |
| Heng et al. [3] | 61% vs. 57% | Median, 55 vs. 64 | 87% vs. 75% | NR | Median, 8.8 vs. 8.1 | 86% vs. 83% | NR | High-grade: 100% | Osteosarcoma type: 48%, Soft tissue sarcoma type: 33%, Unknown: 19% | NR |
| Lee et al. [13] | 100% vs. 56% | Mean, 36 vs. 56 | NR | 0% vs. 25% | Mean, 12 vs. 8.8 | NR | 50% vs. 31% | NR | NR | NR |
| Lee et al. [14] | 0% vs. 57% | Mean, 15 vs. 67 | NR | 0% vs. 57% | Mean, 2 vs. 8 | NR | NR | High-grade: 60% | NR | NR |
| Liao et al. [15] | NR | NR | NR | NR | NR | NR | NR | High-grade: 77%, Low-grade: 23% | DOX, CDDP, IFO, MTX | NR |
| Lidang Jensen et al. [16] | 40% vs. 53% | Mean, 47 vs. 64 | 100% vs. 84% | 20% vs. 26% | Mean, 7 vs. 11 | NR | NR | High-grade: 100% | NR | NR |
| Longhi et al. [2] | NR | Adjuvant chemotherapy was administrated more frequently in patients younger than 65 years. >65 yrs: 21% vs. <65 yrs: 79% | NR | NR | NR | NR | NR | Most are high-grade | Osteosarcoma type: 58%, Soft tissue sarcoma type: 36% | NR |
| Makise et al. [17] | 56% vs. 50% | Mean, 53 vs. 56 | 89% vs. 63% | 44% vs. 63% | Mean, 8.7 vs. 12 | NR | NR | High-grade: 100% | NR | NR |
| Sio et al. [18] | NR | NR | NR | NR | NR | NR | NR | High-grade: 84%, Intermediate-grade: 14% | Mitomycin, DOX, CDDP, IFO, MTX, VP16 | 90% or more necrosis: 19% |
| Torigoe et al. [19] | 77% vs. 75% | Mean, 50 vs. 48 | NR | 46% vs. 25% | NR | 85% vs. 50% | 85% vs. 75% | NR | DTIC, DOX, CDDP, IFO, MTX, VP16, CBDCA, Taxol, THP, VDS | NR |
| Wakamatsu et al. [8] | 64% vs. 50% | Mean, 58 vs. 63 | NR | 45% vs. 0% | Mean, 9.7 vs. NR | 100% vs. 100% | NR | High-grade: 75%, Intermediate-grade: 25% | DOX/CDDP/ IFO/MTX/ VP16/EPI/ CBDCA | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsukamoto, S.; Mavrogenis, A.F.; Angelelli, L.; Righi, A.; Filardo, G.; Kido, A.; Honoki, K.; Tanaka, Y.; Tanaka, Y.; Errani, C. The Effect of Adjuvant Chemotherapy on Localized Extraskeletal Osteosarcoma: A Systematic Review. Cancers 2022, 14, 2559. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102559
Tsukamoto S, Mavrogenis AF, Angelelli L, Righi A, Filardo G, Kido A, Honoki K, Tanaka Y, Tanaka Y, Errani C. The Effect of Adjuvant Chemotherapy on Localized Extraskeletal Osteosarcoma: A Systematic Review. Cancers. 2022; 14(10):2559. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102559
Chicago/Turabian StyleTsukamoto, Shinji, Andreas F. Mavrogenis, Lucia Angelelli, Alberto Righi, Giuseppe Filardo, Akira Kido, Kanya Honoki, Yuu Tanaka, Yasuhito Tanaka, and Costantino Errani. 2022. "The Effect of Adjuvant Chemotherapy on Localized Extraskeletal Osteosarcoma: A Systematic Review" Cancers 14, no. 10: 2559. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102559