
The Role of Interstitial Brachytherapy for Breast Cancer Treatment: An Overview of Indications, Applications, and Technical Notes

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Implant Technique and Treatment Delivery
2.1. Catheter Insertion
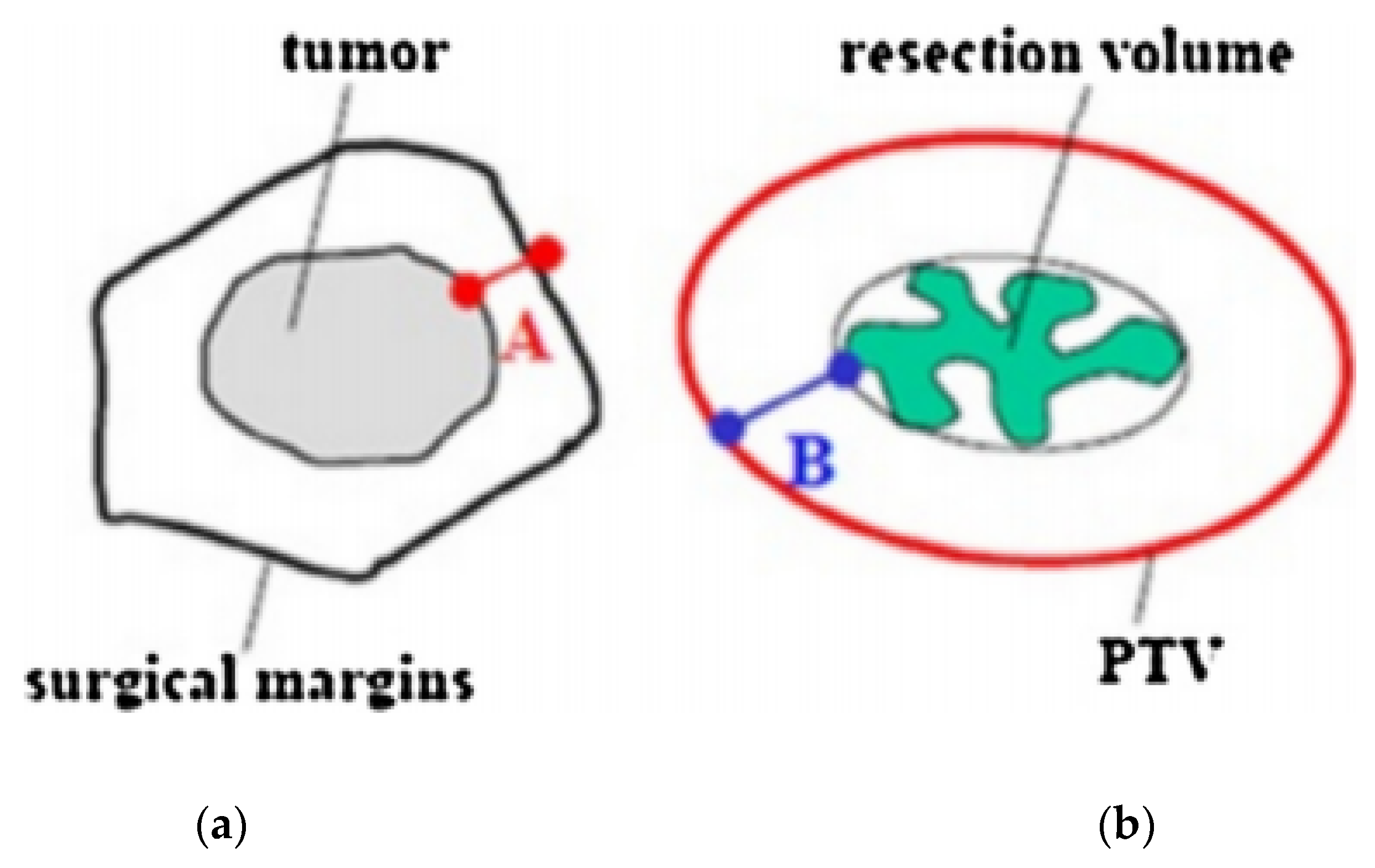
2.2. Target Definition and Delineation
2.3. Dosimetry
3. Brachytherapy Doses
4. Advantages and Disadvantages of the Technique
5. The Roles of Brachytherapy
5.1. Brachytherapy as Radiation Boost on the Tumor Bed
5.2. Brachytherapy to Perform Accelerated Partial Breast Irradiation (ABPI)
5.3. Brachytherapy as Salvage Treatment APBrI for Ipsilateral Breast Recurrence
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Bauer, M.; Margolese, R.; Poisson, R.; Pylch, Y.; Redmond, C.; Fisher, E.; Wolmark, N.; Deutsch, M.; Montague, E.; et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N. Engl. J. Med. 1985, 312, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.; Deutch, M.; Fisher, E.R.; Jeong, J.H.; Wolmark, N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veronesi, U.; Saccozzi, R.; Del Vecchio, M.; Banfi, A.; Clemente, C.; De Lena, M.; Gallus, G.; Greco, M.; Luini, A.; Marubini, E.; et al. Comparing radical mastectomy with quadrantectomy, axillary dissection, and radiotherapy in patients with small cancers of the breast. N. Engl. J. Med. 1981, 305, 6–11. [Google Scholar] [CrossRef]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubuni, E. Twenty year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N. Engl. J. Med. 2002, 347, 1227–1232. [Google Scholar] [CrossRef]
- Keynes, G. The place of radium in the treatment of cancer of the breast. Ann. Surg. 1937, 106, 619–630. [Google Scholar] [CrossRef]
- Polgar, C.; Fodor, J.; Major, T.; Sulyok, Z.; Kásler, M. Breast-conserving therapy with partial or whole breast irradiation: Ten-year results of the Budapest randomized trial. Radiother. Oncol. 2013, 108, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Ott, O.J.; Hildebrandt, G.; Potter, R.; Hammer, J.; Lotter, M.; Resch, A.; Sauer, R.; Strnad, V. Accelerated partial breast irradiation with multi-catheter brachytherapy: Local control, side effects and cosmetic outcome for 274 patients. Results of the GermanAustrian multi-centre trial. Radiother. Oncol. 2007, 82, 281–286. [Google Scholar] [CrossRef]
- Strnad, V.; Hildebrandt, G.; Pötter, R.; Hammer, J.; Hindemith, M.; Resch, A.; Spiegl, K.; Lotter, M.; Uter, W.; Bani, M.; et al. Accelerated partial breast irradiation: 5-year results of the German-ustrian multicenter phase II trial using interstitial multicatheter brachytherapy alone after breast-conserving surgery. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 17–24. [Google Scholar] [CrossRef]
- Polgar, C.; Major, T.; Fodor, J.; Sulyok, Z.; Somogyi, A.; Lovey, K.; Nemeth, G.; Klaser, M. Accelerated partial-breast irradiation using high-dose-rate interstitial brachytherapy: 12-year update of a prospective clinical study. Radiother. Oncol. 2010, 94, 274–279. [Google Scholar] [CrossRef]
- Hannoun-Levi, J.M.; Resch, A.; Gal, J.; Kauer-Dorner, D.; Strnad, V.; Niehoff, P.; Loessl, K.; Kovács, G.; Van Lim-bergen, E.; Polgár, C.; et al. Accelerated partial breast irradiation with interstitial brachytherapy as second conservative treatment for ipsilateral breast tumour recurrence: Multicentric study of the GEC-ESTRO Breast Cancer Working Group. Radiother. Oncol. 2013, 108, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Pierquin, B.; Wilson, J.-F.; Chassagne, D. The Paris System. In Modern Brachytherapy; Pierquin, B., Wilson, J.F., Chassagne, D., Eds.; Masson: Paris, France, 1987. [Google Scholar]
- Major, T.; Fröhlich, G.; Lövey, K.; Fodor, J.; Polgár, C. Dosimetric experience with accelerated partial breastirradiation using image-guided interstitial brachytherapy. Radiother. Oncol. 2009, 90, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Polgar, C.; Strnad, V.; Major, T. Brachytherapy for partial breast irradiation: The European experience. Semin. Radiat. Oncol. 2005, 15, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Polgar, C.; Van Limbergen, E.; Potter, R.; Kovacs, G.; Polo, A.; Lyczek, J.; Hildebrandt, G.; Niehoff, P.; Guinot, J.L.; Guedea, F.; et al. Patient selection for accelerated partial-breast irradiation (APBI) after breastconserving surgery: Recommendations of the Group Europeen de Curietherapie-European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) breast cancer working group based on clinical evidence (2009). Radiother. Oncol. 2010, 94, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Strnad, V.; Hannoun-Lévi, J.-M.; Guinot, J.-L.; Lössl, K.; Kauer-Dorner, D.; Resch, A.; Kovacs, G.; Major, T.; Van Limnergen, E. Recommendations from GEC ESTRO Breast Cancer Working Group (I): Target definition and target delineation for accelerated or boost partial breast irradiation using multicatheter interstitial brachytherapy after breast conserving closed cavity surgery. Radiother. Oncol. 2015, 115, 342–348. [Google Scholar] [CrossRef]
- Major, T.; Gutiérrez, C.; Guix, B.; van Limbergen, E.; Strnad, V.; Polgar, C. Recommendations from GEC ESTRO Breast Cancer Working Group (II): Target definition and target delineation for accelerated or boost partial breast irradiation using multicatheter interstitial brachytherapy after breast conserving open cavity surgery. Radiother. Oncol. 2016, 118, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Strnad, V.; Ott, O.J.; Hildebrandt, G.; Kauer-Dorner, D.; Knauerhase, H.; Major, T.; Lyczek, J.; Guinot, J.L.; Dunst, J.; Gutierrez miguelez, C.; et al. 5-year results of accelerated partial breast irradiation using sole interstitial multicatheter brachytherapy versus whole-breast irradiation with boost after breast-conserving surgery for low-risk invasive and in-situ carcinoma of the female breast: A randomised, phase 3, non-inferiority trial. Lancet 2016, 387, 229–238. [Google Scholar] [CrossRef]
- Sato, K.; Shimo, T.; Fuchikami, H.; Takeda, N.; Kato, M.; Okawa, T. Catheter-based delineation of lumpectomy cavity for accurate target definition in partial-breast irradiation with multicatheter interstitial brachytherapy. J. Contemp. Brachyther. 2019, 11, 108–115. [Google Scholar] [CrossRef]
- Strnad, V.; Major, T.; Polgar, C.; Lotter, M.; Guinot, J.L. ESTRO-ACROP guideline: Interstitial multi-catheter breast brachytherapy as Accelerated Partial Breast Irradiation alone or as boost—GEC-ESTRO Breast Cancer Working Group practical recommendations. Radiother. Oncol. 2018, 128, 411–420. [Google Scholar] [CrossRef] [Green Version]
- Chargari, C.; Van Limbergen, E.; Mahantshetty, U.; Deutsch, E.; Haie-Meder, C. Radiobiology of brachytherapy: The historical view based on linear quadratic model and perspectives for optimization. Cancer Radiother. 2018, 22, 312–318. [Google Scholar] [CrossRef]
- Georg, D.; Kirisits, C.; Hillbrand, M.; Dimopoulos, J.; Potter, R. Image-guided radiotherapy for cervix cancer: High-tech external beam therapy versus high-tech brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Yanez, L.; Ciudad, A.M.; Mehta, M.P.; Marisglia, H. What is the evidence for the clinical value of SBRT in cancer of the cervix? Rep. Pract. Oncol. Radiother. 2018, 23, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Otahal, B.; Dolezel, M.; Cvek, J.; Simetka, O.; Klat, J.; Knibel, L.; MOlenda, L.; Skacelikova, E.; Hlavka, A.; Felti, D. Dosimetric comparison of MRI-based HDR brachytherapy and stereotactic radiotherapy in patients with advanced cervical cancer: A virtual brachytherapy study. Rep. Pract. Oncol. Radiother. 2014, 19, 399–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chargari, C.; Deutsch, E.; Blanchard, P.; Gouy, S.; Martelli, H.; Guerin, F.; Dumas, I.; Bossi, A.; MOrice, P.; Viswanathan, A.; et al. Brachytherapy: An overview for clinicians. CA Cancer J. Clin. 2019, 69, 386–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, K.; Shimo, T.; Fuchikami, H.; Takeda, N.; Kato, M.; Okawa, T. Predicting adherence of dose-volume constraints for personalized partial-breast irradiation technique. Brachytherapy 2021, 20, 163–170. [Google Scholar] [CrossRef]
- Liljegren, G.; Holmberg, L.; Adami, H.O.; Weatman, G.; Graffman, S.; Bergh, J.; Uppsala-Orebro Breast Cancer Study Group. Sector resection with or without postoperative radiotherapy for stage I breast cancer: Five-year results of a randomized trial. J. Natl. Cancer Inst. 1994, 86, 717–722. [Google Scholar] [CrossRef] [Green Version]
- Veronesi, U.; Marubini, E.; Mariani, L.; Galimberti, V.; Luini, A.; Verosnesi, P.; Zucali, R. Radiotherapy after breast-conserving surgery in small breast carcinoma: Long-term results of a randomized trial. Ann. Oncol. 2001, 12, 997–1003. [Google Scholar] [CrossRef]
- Bartelink, H.; Horiot, J.C.; Poortmans, P.; Struikmans, H.; Van den Bogaert, W.; Batillot, I.; Fourquet, A.; Borger, J.; Jager, J.; Hoogenraad, L.; et al. Recurrence rates after treatment of breast cancer with standard radio- therapy with or without additional radiation. N. Engl. J. Med. 2001, 345, 1378–1387. [Google Scholar] [CrossRef]
- Polo, A.; Polgár, C.; Hannoun-Lévi, J.-M.; Guinot, J.-L.; Gutierrez, C.; Galalae, R.; VanLimbergen, E.; Strnad, V. Risk factors and state-of-the-art indications for boost irradiation in invasive breast carcinoma. Brachytherapy 2017, 16, 552–564. [Google Scholar] [CrossRef]
- Bartelink, H.; Maingon, P.; Poortmans, P.; Weltens, C.; Fourquet, A.; Jager, J.; Schinagl, D.; Dei, B.; Rodenhuis, C.; Horiot, J.C.; et al. Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a ran- domised phase 3 trial. Lancet Oncol. 2015, 16, 47–56. [Google Scholar] [CrossRef]
- Mansfield, C.M.; Komarnicky, L.T.; Schwartz, G.F.; Rosenberg, A.L.; Krishnan, L.; Jewell, W.R.; Rosato, F.E.; Moses, M.L.; Haghbin, M.; Taylor, J. Ten-year results in 1070 patients with stages I and II breast cancer treated by conservative surgery and radiation therapy. Cancer 1995, 75, 2328–2336. [Google Scholar] [CrossRef]
- Knauerhase, H.; Strietzel, M.; Gerber, B.; Reimer, T.; Fietkau, R. Tumor location, interval between surgery and radiotherapy, and boost technique influence local control after breast-conserving surgery and radiation: Retrospective analysis of monoinstitutional long-term results. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Polgár, C.; Jánváry, L.; Major, T.; Somogyi, A.; Takácsi-Nagy, Z.; Fröhlich, G.; Fodor, J. The role of high-dose-rate brachytherapy boost in breast-conserving therapy: Long-term results of the Hungarian National Institute of Oncology. Rep. Pract. Oncol. Radiother. 2010, 15, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poortmans, P.; Bartelink, H.; Horiot, J.C.; Struikmans, H.; Van den Bogaert, W.; Fourquet, A.; Jager, J.; Hoogenraad, W.; Rodrigus, P.; Wárlám-Rodenhuis, C.; et al. The influence of the boost technique on local control in breast conserving treatment in the EORTC ’boost versus no boost’ randomised trial. Radiother. Oncol. 2004, 72, 25–33. [Google Scholar] [CrossRef]
- Quéro, L.; Guillerm, S.; Taright, N.; Michaud, S.; Teixeira, L.; Cahen-Doidy, L.; Bourstyn, E.; Espié, M.; Hennequin, C. 10-Year follow-up of 621 patients treated using high-dose rate brachytherapy as ambulatory boost technique in conservative breast cancer treatment. Radiother. Oncol. 2017, 122, 11–16. [Google Scholar] [CrossRef]
- Clark, R.M.; McCulloch, P.B.; Levine, M.N.; Lipa, M.; Wilkinson, R.H.; Mahoney, L.J.; Basrur, V.R.; Nair, B.D.; McDermot, R.S.; Wong, C.S.; et al. Randomized clinical trial to assess the effectiveness of breast irradiation following lumpectomy and axillary dissection for node-negative breast cancer. J. Natl. Cancer Inst. 1996, 84, 683–689. [Google Scholar] [CrossRef]
- Liljegren, G.; Holmberg, L.; Bergh, J.; Lindgren, A.; Tabar, L.; Nordgren, H.; Adami, H.O. 10-year results after sector resection with or without postoperative radiotherapy for stage I breast cancer: A randomized trial. J. Clin. Oncol. 1999, 17, 2326–2333. [Google Scholar] [CrossRef]
- Fisher, E.R.; Anderson, S.; Redmond, C.; Fisher, B. Psilateral breast tumor recurrence and survival following lumpectomy and irradiation: Pathologic findings from NSABP protocol B-06. Semin. Surg. Oncol. 1992, 8, 161–166. [Google Scholar]
- Wazer, D.E.; Schmidt-Ullrich, R.K.; Ruthazer, R.; Schmid, C.H.; Graham, r.; Safari, H.; Rothschild, J.; McGrath, J.; Erban, J.K. Factors determing outcome for breast conserving irradiation with margin-directed dose escalation to the tumor bed. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 851–858. [Google Scholar] [CrossRef]
- Galalae, R.; Hannoun-Lévi, J.M. Accelerated partial breast irradiation by brachytherapy: Present evidence and future developments. Jpn. J. Clin. Oncol. 2020, 50, 743–752. [Google Scholar] [CrossRef]
- Correa, C.; Harris, E.E.; Leonardi, M.C.; Smith, B.D.; Taghian, A.G.; Thompson, A.M.; White, J.; Harris, J.R. Accelerated Partial Breast Irradiation: Executive summary for the update of an ASTRO Evidence-Based Consensus Statement. Pract. Radiat. Oncol. 2017, 7, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Shah, C.; Vicini, F.; Shaitelman, S.F.; Hepel, J.; Keisch, M.; Arthur, D.; Khan, A.J.; Kuske, R.; Patel, R.; Wazer, D.E. The American Brachytherapy Society consensus statement for accelerated partial-breast irradiation. Brachytherapy 2018, 17, 154–170. [Google Scholar] [CrossRef] [PubMed]
- Wazer, D.E.; Berle, L.; Graham, R.; Chung, M.; Rothschild, J.; Graves, T.; Cady, B.; Ulin, K.; Ruthazer, R.; DiPetrillo, T.A. Preliminary results of a phase I/II study of HDR brachytherapy alone for T1/T2 breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 889–897. [Google Scholar] [CrossRef]
- Perera, F.; Yu, E.; Engel, J.; Holliday, R.; Scott, L.; Chisela, F.; Venkatesan, V. Patterns of breast recurrence in a pilot study of brachytherapy confined to the lumpectomy site for early breast cancer with six years’ minimum follow-up. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 1239–1246. [Google Scholar] [CrossRef]
- Polgár, C.; Major, T.; Fodor, J.; Németh, G.; Orosz, Z.; Sulyok, Z.; Udvarhelyi, N.; Somogyi, A.; Takacsi-Nagy, Z.; Lovey, K.; et al. High-dose-rate brachytherapy alone versus whole breast radiotherapy with or without tumor bed boost after breast-conserving surgery: Seven-year results of a comparative study. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1173–1181. [Google Scholar] [CrossRef]
- Kaufman, S.A.; DiPetrillo, T.A.; Price, L.L.; Midle, J.B.; Wazer, D.E. Long-term outcome and toxicity in a Phase I/II trial using high-dose-rate multicatheter interstitial brachytherapy for T1/T2 breast cancer. Brachytherapy 2007, 6, 286–292. [Google Scholar] [CrossRef]
- Wallace, M.; Martinez, A.; Mitchell, C.; Chen, P.Y.; Ghilezan, M.; Benitez, P.; Brown, E.; Vicini, F. Phase I/II study evaluating early tolerance in breast cancer patients undergoing accelerated partial breast irradiation treated with the mammosite balloon breast brachytherapy catheter using a 2-day dose schedule. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 531–536. [Google Scholar] [CrossRef]
- Shah, C.; Badiyan, S.; Wilkinson, J.B.; Vicini, F.; Beitsch, P.; Keisch, M.; Arthur, D.; Lyden, M. Treatment efficacy with accelerated partial breast irradiation (APBI): Final analysis of the American Society of Breast Surgeons MammoSite® breast brachytherapy registry trial. Ann. Surg. Oncol. 2013, 20, 3279–3285. [Google Scholar] [CrossRef]
- Rabinovitch, R.; Winter, K.; Kuske, R.; Bolton, J.; Arthur, D.; Scroggins, T.; Vicini, F.; McCormick, B.; White, J. RTOG 95-17, a Phase II trial to evaluate brachytherapy as the sole method of radiation therapy for Stage I and II breast carcinoma-year-5 toxicity and cosmesis. Brachytherapy 2014, 13, 17–22. [Google Scholar] [CrossRef] [Green Version]
- White, J.; Winter, K.; Kuske, R.R.; Bolton, J.S.; Arthur, D.W.; Scroggins, T.; Rabinivitch, R.A.; Kelly, T.; Toonkel, L.M.; Vicini, F.A.; et al. Long-Term Cancer Outcomes From Study NRG Oncology/RTOG 9517: A Phase 2 Study of Accelerated Partial Breast Irradiation with Multicatheter Brachytherapy after Lumpectomy for Early-Stage Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1460–1465. [Google Scholar] [CrossRef] [Green Version]
- Wobb, J.L.; Shah, C.; Chen, P.Y.; Wallace, M.; Ye, H.; Jawad, M.S.; Grills, I.S. Brachytherapy-based Accelerated Partial Breast Irradiation Provides Equivalent 10-Year Outcomes to Whole Breast Irradiation: A Matched-Pair Analysis. Am. J. Clin. Oncol. 2016, 39, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, S.; Laplana, M.; Najjari, D.; Slocker, A.; Encina, X.; Pera, J.; Guedea, F.; Gutierrez, C. Advantages of intraoperative implant for interstitial brachytherapy for accelerated partial breast irradiation either frail patients with early-stage disease or in locally recurrent breast cancer. J. Contemp. Brachyther. 2018, 10, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hepel, J.T.; Yashar, C.; Leonard, K.L.; Einck, J.P.; Sha, S.; DiPetrillo, T.; Wiggins, D.; Graves, T.; Edmonson, D.; Wazer, D. Five fraction accelerated partial breast irradiation using noninvasive image-guided breast brachytherapy: Feasibility and acute toxicity. Brachytherapy 2018, 17, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Pohanková, D.; Sirák, I.; Jandík, P.; Kašaova, L.; Grepl, J.; Motyčka, P.; Asqar, A.; Paluska, P.; Ninger, V.; Bydžovská, I.; et al. Accelerated partial breast irradiation with perioperative multicatheter interstitial brachytherapy—A feasibility study. Brachytherapy 2018, 17, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.J.; Chen, P.Y.; Yashar, C.; Poppe, M.M.; Li, L.; Yehia, Z.A.; Vicini, F.A.; Moore, D.; Dale, R.; Arthur, D.; et al. Three-Fraction Accelerated Partial Breast Irradiation (APBI) Delivered with Brachytherapy Applicators Is Feasible and Safe: First Results from the TRIUMPH-T Trial. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Vicini, F.A.; Cecchini, R.S.; White, J.R.; Arthur, D.W.; Julian, T.B.; Rabinovitch, R.A.; Kuske, R.; Ganz, P.; Parda, D.S.; Scheier, M.F.; et al. Long-term primary results of accelerated partial breast irradiation after breast-conserving surgery for early-stage breast cancer: A randomised, phase 3, equivalence trial. Lancet 2019, 394, 2155–2164. [Google Scholar] [CrossRef]
- Mutter, R.W.; Hepel, J.T. Accelerated Partial Breast Radiation: Information on Dose, Volume, Fractionation, and Efficacy from Randomized Trials. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 1123–1128. [Google Scholar] [CrossRef]
- Vicini, F.A.; Cecchini, R.S.; White, J.R.; Julian, T.B.; Arthur, D.W.; Rabinovitch, R.A. Primary results of NSABP B-39/RTOG 0413 (NRG Oncology): A randomized phase III study of conventional whole breast irradiation versus partial breast irradiation for women with stage 0, I, or II breast cancer. In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 4–8 December 2018. [Google Scholar]
- Gaudet, M.; Pharand-Charbonneau, M.; Wright, D.; Nguyen, J.; Trudel-Sabourin, J.; Chelfi, M. Long-term results of multicatheter interstitial high-dose-rate brachytherapy for accelerated partial-breast irradiation. Brachytherapy 2019, 18, 211–216. [Google Scholar] [CrossRef]
- Maranzano, E.; Arcidiacono, F.; Italiani, M.; Anselmo, P.; Casale, M.; Terenzi, S.; Di Marzo, A.; Fabiani, S.; Draghini, L.; Trippa, F. Accelerated partial-breast irradiation with high-dose-rate brachytherapy: Mature results of a Phase II trial. Brachytherapy 2019, 18, 627–634. [Google Scholar] [CrossRef]
- Hannoun-Lévi, J.M.; Cham Kee, D.L.; Gal, J.; Schiappa, R.; Hannoun, A.; Gautier, M.; Boulahssass, R.; Peyrottes, I.; Barranger, E.; Ferrero, J.M.; et al. Accelerated partial breast irradiation for suitable elderly women using a single fraction of multicatheter interstitial high-dose-rate brachytherapy: Early results of the Single-Fraction Elderly Breast Irradiation (SiFEBI) Phase I/II trial. Brachytherapy 2018, 17, 407–414. [Google Scholar] [CrossRef]
- Hannoun-Lévi, J.M.; Lam Cham Kee, D.; Gal, J.; Schiappa, R.; Hannoun, A.; Fouche, Y.; Gautier, M.; Boulahssass, R.; Chand, M.E. Accelerated partial breast irradiation in the elderly: 5-Year results of the single fraction elderly breast irradiation (SiFEBI) phase I/II trial. Brachytherapy 2020, 19, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Ibarria, N.G.; Pinar, M.B.; García, L.; Cabezón, M.A.; Lloret, M.; Rey-Baltar, M.D.; Rdguez-Melcón, J.I.; Lara, P.C. Accelerated partial breast irradiation with interstitial multicatheter brachytherapy after breast-conserving surgery for low-risk early breast cancer. Breast 2020, 52, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Laplana, M.; Cozzi, S.; Najjari, D.; Martín, M.I.; Rodriguez, G.; Slocker, E.; Sancho, I.; Pla, M.J.; Garcia, M.; Gracia, R.; et al. Five-year results of accelerated partial breast irradiation: A single-institution retrospective review of 289 cases. Brachytherapy 2021, 20, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Hepel, J.T.; Leonard, K.L.; Rivard, M.; Benda, R.; Pittier, A.; Mastras, D.; Sha, S.; Smith, L.; Kerley, M.; Kocheril, P.G.; et al. Multi-institutional registry study evaluating the feasibility and toxicity of accelerated partial breast irradiation using noninvasive image-guided breast brachytherapy. Brachytherapy 2021, 20, 631–637. [Google Scholar] [CrossRef]
- Polgár, C.; Major, T.; Takácsi-Nagy, Z.; Fodor, J. Breast-Conserving Surgery Followed by Partial or Whole Breast Irradiation: Twenty-Year Results of a Phase 3 Clinical Study. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Garduño-Sánchez, S.; Villanego-Beltrán, I.; de Las Peñas-Cabrera, M.D.; Jaén-Olasolo, J. Comparison between Accelerated Partial Breast Irradiation with multicatheter interstitial brachytherapy and Whole Breast Irradiation, in clinical practice. Clin. Transl. Oncol. 2022, 24, 24–33. [Google Scholar] [CrossRef]
- Polgár, C.; Ott, O.J.; Hildebrandt, G.; Kauer-Dorner, D.; Knauerhase, H.; Major, T.; Lyczek, J.; Guinot, J.L.; Dunst, J.; Gutierrez Miguelez, C.; et al. Late side-effects and cosmetic results of accelerated partial breast irradiation with interstitial brachytherapy versus whole-breast irradiation after breast-conserving surgery for low-risk invasive and in-situ carcinoma of the female breast: 5-year results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 259–268. [Google Scholar] [CrossRef]
- Schäfer, R.; Strnad, V.; Polgár, C.; Uter, W.; Hildebrandt, G.; Ott, O.J.; Kauer-Dornes, D.; Knauerhase, H.; Majir, T.; Lyczek, J.; et al. Quality-of-life results for accelerated partial breast irradiation with interstitial brachytherapy versus whole-breast irradiation in early breast cancer after breast-conserving surgery (GEC-ESTRO): 5-year results of a randomised, phase 3 trial. Lancet Oncol. 2018, 19, 834–844. [Google Scholar] [CrossRef]
- Perrucci, E.; Lancellotta, V.; Bini, V.; Falcinelli, L.; Farneti, A.; Margaritelli, M.; Capezzali, G.; Palumbo, I.; Aristei, C. Quality of life and cosmesis after breast cancer: Whole breast radiotherapy vs. partial breast high-dose-rate brachytherapy. Tumori 2015, 101, 161–167. [Google Scholar] [CrossRef]
- Wadasadawala, T.; Maitre, P.; Sinha, S.; Parmar, V.; Pathak, R.; Gaikar, M.; Verma, S.; Sarin, R. Patient-reported quality of life with interstitial partial breast brachytherapy and external beam whole breast radiotherapy: A comparison using propensity-score matching. J. Contemp. Brachyther. 2021, 13, 387–394. [Google Scholar] [CrossRef]
- Wobb, J.L.; Shah, C.; Jawad, M.S.; Wallace, M.; Dilworth, J.T.; Grills, I.S.; Ye, H.; Chen, P.Y. Comparison of chronic toxicities between brachytherapy-based accelerated partial breast irradiation and whole breast irradiation using intensity modulated radiotherapy. Breast 2015, 24, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Daugherty, L.; Shaikh, T.; Reiff, J.; Perlingiero, D.; Alite, F.; Brady, L.; Komarnicky, L. Tumor bed-to-skin distance using accelerated partial-breast irradiation with the strut-adjusted volume implant device. Brachytherapy 2012, 11, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Cuttino, L.W.; Arthur, D.W.; Vicini, F.; Todor, D.; Julian, T.; Mukhopadhyay, M. Long-term results from the Contura multilumen balloon breast brachytherapy catheter phase 4 registry trial. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 1025–1029. [Google Scholar] [CrossRef] [PubMed]
- Gentilini, O.; Botteri, E.; Veronesi, P.; Sangalli, C.; Del Castillo, A.; Ballardini, B.; Galimberti, V.; Rietjens, M.; Colleoni, M.; Luini, A.; et al. Repeating conservative surgery after ipsilateral breast tumor reappearance: Criteria for selecting the best candidates. Ann. Surg. Oncol. 2012, 19, 3771–3776. [Google Scholar] [CrossRef]
- Walstra, C.J.E.F.; Schipper, R.; Poodt, I.G.M.; van Riet, Y.E.; Voogd, A.C.; van der Sangen, M.; Nieuwenhuijzen, G. European Journal of Surgical Oncology Repeat breast-conserving therapy for ipsilateral breast cancer recurrence: A systematic review. Eur. J. Surg. Oncol. 2019, 45, 1317–1327. [Google Scholar] [CrossRef]
- Hannoun-Levi, J.-M.; Ihrai, T.; Courdi, A. Local treatment options for ipsilateral breast tumour recurrence. Cancer Treat. Rev. 2013, 39, 737–741. [Google Scholar] [CrossRef]
- Hannoun Levi, J.M.; van Limbergen, E.; Gal, J.; Chand, M.E.; Schiappa, R.; Smanyko, V.; Kauer-Domer, D.; Pasqiuier, D.; Lemanski, C.; Racadot, S.; et al. Salvage mastectomy versus second conservative treatment for second ipsilateral breast tumor event: A propensity-score matched cohort analysis. Int. J. Radiat. Oncol. 2018, 102, S80. [Google Scholar] [CrossRef]
- Maulard, C.; Housset, M.; Brunel, P.; Delanian, S.; Taurelle, R.; Baillet, F. Use of perioperative or split-course interstitial brachytherapy techniques for salvage irradiation of isolated local recurrences after conservative management of breast cancer. Am. J. Clin. Oncol. 1995, 18, 348–352. [Google Scholar] [CrossRef]
- Hannoun-Levi, J.M.; Houvenaeghel, G.; Ellis, S.; Teissier, E.; Alzieu, C.; Lallement, M.; Cowen, D. Partial breast irradiation as second conservative treatment for local breast cancer recurrence. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1385–1392. [Google Scholar] [CrossRef]
- Niehoff, P.; Dietrich, J.; Ostertag, H.; Niehoff, P.; Dietrich, J.; Ostertag, H.; Schmid, A.; Kohr, P.; Kimmig, B.; Kovacs, G. High-dose-rate (HDR) or pulsed-doserate (PDR) perioperative interstitial intensity-modulated brachytherapy (IMBT) for local recurrences of previously irradiated breast or thoracic wall following breast cancer. Strahlenther. Onkol. 2006, 182, 102–107. [Google Scholar] [CrossRef]
- Chadha, M.; Feldman, S.; Boolbol, S.; Wang, L.; Harrison, L. The feasibility of a second lumpectomy and breast brachytherapy for localized cancer in a breast previously treated with lumpectomy and radiation therapy for breast cancer. Brachytherapy 2008, 7, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Guix, B.; Lejárcegui, J.A.; Tello, J.I.; Zanon, I.; Henriquez, I.; Finestre, F.; Martinez, A.; Ibiza, J.; Quinzanos, L.; Palombo, P.; et al. Exeresis and brachytherapy as salvage treatment for local recurrence after conservative treatment for breast cancer: Results of a ten-year pilot study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Hannoun-Levi, J.M.; Castelli, J.; Plesu, A.; Courdi, A.; Raoust, I.; Lallement, M.; Flipo, B.; Ettore, F.; Chapelier, C.; Follana, P.; et al. Second conservative treatment for ipsilateral breast cancer recurrence using high-dose rate interstitial brachytherapy: Preliminary clinical results and evaluation of patient satisfaction. Brachytherapy 2011, 10, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Kauer-dorner, D.; Pötter, R.; Resch, A.; Handl-Zeller, L.; Kirchheiner, K.; Schell, M.M.; Dorr, W. Partial breast irradiation for locally recurrent breast cancer within a second breast conserving treatment: Alternative to mastectomy? Results from a prospective trial. Radiother. Oncol. 2018, 102, 96–101. [Google Scholar] [CrossRef]
- Smanykó, V.; Mészáros, N.; Újhelyi, M.; Fröhlich, G.; Stelczer, G.; Major, T.; Mátrai, Z.; Polgár, C. Second breast-conserving surgery and interstitial brachytherapy vs. salvage mastectomy for the treatment of local recurrences: 5-year results. Brachytherapy 2019, 18, 411–419. [Google Scholar] [CrossRef]
- Montagne, L.; Gal, J.; Chand, M.; Schiappa, R.; Falk, A.; Kinj, R.; Gautier, M.; Hannoun-levi, J.M. GEC-ESTRO APBI classification as a decision-making tool for the management of 2nd ipsilateral breast tumor event. Breast Cancer Res. Treat. 2019, 176, 149–157. [Google Scholar] [CrossRef]
- Forster, T.; Akbaba, S.; Schmitt, D.; Krug, D.; El Shafie, R.; Oelmann-Avendano, J.; Lindel, K.; Koning, L.; Arians, N.; Bernhardt, D.; et al. Second breast conserving therapy after ipsilateral breast tumor recurrence—A 10-year experience of re-irradiation. J. Contemp. Brachyther. 2019, 11, 312–319. [Google Scholar] [CrossRef]
- Cozzi, S.; Jamal, D.N.; Slocker, A.; Tejedor, G.A.; Krengli, M.; Guedea, F.; Gutierrez, C. Second breast-conserving therapy with interstitial brachytherapy (APBI) as a salvage treatment in ipsilateral breast tumor recurrence: A retrospective study of 40 patients. J. Contemp. Brachyther. 2019, 11, 101–107. [Google Scholar] [CrossRef]
- Vavassori, A.; Riva, G.; Cavallo, I.; Spoto, R.; Dicuonzo, S.; Fodor, C.; Come, S.; Cambria, R.; Cattani, F.; Morra, A.; et al. High-dose-rate Brachytherapy as Adjuvant Local rEirradiation for Salvage Treatment of Recurrent breAst cancer (BALESTRA): A retrospective mono-institutional study. J. Contemp. Brachyther. 2020, 12, 207–215. [Google Scholar] [CrossRef]
- Chatzikonstantinou, G.; Strouthos, I.; Scherf, C.; Kohn, J.; Solbach, C.; Rodel, C.; Tselis, N. Interstitial multicatheter HDR-brachytherapy as accelerated partial breast irradiation after second breast-conserving surgery for locally recurrent breast cancer. J. Radiat. Res. 2021, 62, 465–472. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Organs | Constraints |
|---|---|
| Ipsilateral no target breast tissue | V90 < 10% V50 < 40% |
| Skin | D1 cm3 < 90% D0.2 cm3 < 100% |
| Ribs | D0.1 cm3 < 90% D1 cm3 < 80% |
| Heart | MHD < 8% D0.1 cm3 < 50% |
| Ipsilateral lung | MLD < 8% D0.1 cm3 < 60% |
| Study | Type of Study | Number of Patients | Follow Up (m) | Total Dose (Gy) (Dose for Fraction) and Technique | Outcomes | Toxicities > G2-3 (%) | Cosmesis Results |
|---|---|---|---|---|---|---|---|
| Mansfield C.M. et al., 1995 [32]. | Retrospective | 1070 | 40 | 45 + 20 Gy Ir-192 implant | 5y-10y LC 93–88%, PFS 93–79%, OS 92–77% | 6.5% (18 pts: Moderate/severe fibrosis | 91% (575 pts Excellent/good) |
| Knauerhase 2008 [33]. | Retrospective | 263 | 94 | electron boost of 6–14 Gy (median, 10 Gy) in 173 patients, with an interstitial boost of 8–12 Gy (median, 10 Gy) in 75 patients (single HDR boost technique), and with a photon (orthovoltage) boost of 7.5–9 Gy in 8 patients. | 5- and 10-year LRR of 0% and 5.9%, respectively, | Not reported | Not reported |
| Polgàr C. et al., 2009 [34]. | Prospective randomized study. | 207 (52 HDR BT) | 63.6 | 50 Gy WBI + 12–14, 25 Gy HDR BT | 5y-LTC (electron boost vs. HDR BT 94.2–91.4%) | 7.7 (4 pts: telangiectasia) 17.3 (9 pts: fibrosis) | 88.5% (46 pts: Excellent/good, |
| Poortmans et al., 2004 [35]. | prospective randomized multi-center trial. | 2661 (225–9% IBT) | 60 | 50 + 15 Gy with an iridium192 implant | 5y LF 6 pts 2.5% | 7.1% (16 pts: moderate/severe fibrosis | Not reported |
| Polgar C et al., 2010 [10]. | Retrospective | 100 | 94 | Single-fraction HDR boost: 8–10.35 Gy (10%) Fractionated multicatheter HDR boost: 3 × 4Gy, 3 × 4.75Gy, 2 × 6.4Gy (90%) | 5y LC: 4.5% 8y LC: 7% 8y OS: 80.4% | G3 fibrosis: 6.6% G3 telangiectasia: 2.2% | Excellent good: 56% |
| Bartelink 2015 [31]. | Randomized phase 3 trial | 2657 | 206.4 | 50 Gy WBI + 15 Gy HDR BT | -- | -- | -- |
| Quero et al., 2016 [36]. | Retrospective | 621 | 122 | 44 Gy WBI + 5 Gy × 2 fraction HDR BT | 10y LR: 7.4% 10y OS: 91% 10y DM 10.6% | Not reported | Excellent good: 80% |
| Study | Type of Study | Patients | BCT Dose | Outcomes | Toxicity | Cosmesis |
|---|---|---|---|---|---|---|
| Wazer et al., 2002 [44] | Prospective | 32 | 34 Gy (10 fr) | 4-y LRR 3% | Skin toxicity: G0-1 30 pts G2 3 pts Subcutaneous toxicity: G0 11 pts G1 3 pts G2 8 pts G 3 3 pts G4 8 pts Fat necrosis 8 pts | 0 pts poor 4 pts fair 5 pts good, 24 pts excellent |
| Perera et al., 2003 [45] | Prospective | 39 | 37.2 Gy (10 fr) | 5-y IBTR 16.2% | -- | -- |
| Polgar et al., 2004/2013 [7,46] | Prospective | 45 | 30.3 Gy (7 fz) 36.4 Gy (7 fz) | IBTR 6.7% 5-y IBTR rate 4.4% 7-y LRR 9% 7-y CSS 93.3% 7-y RFS 79.8% 10-y LRR 5.9% 10-y OS 80% 10-y CSS 94% 10-y DSS 85% | G1 fat necrosis 20% G2 fat necrosis 2.2% ≥G2 late toxicity 26.7% | 84.4% (7y)–81% (10y) excellent/good |
| Kaufman et al., 2007 [47] | Prospective | 32 | 34 Gy (10 fr) | 5-y LRR 6.1% n,3 treatment failures | Fat necrosis 27.3% (2y) 28.1% (5y) 17.9% (>5y) Skin toxicity 28.6% (>5y) G2-3 Subcutaneous toxicity 37.7% (>5y) Pain 17.9% (>5y) | Improved with longer follow up |
| Wallace et al., 2010 [48] | Prospective | 45 | 28 Gy (4 fr) | -- | Acute toxicity: G2 radiation dermatitis 9% G2 breast pain 13% G2 edema 2% G2 hyperpigmentation 2% G3 breast pain 13% Infection 13% Late toxicity: G2 radiation dermatitis 2% G2 induration 2% G2 hypopigmentation 2% G3 breast pain 2% Infection 5% seroma 30% fat necrosis n. 4 rib fractures 4% | 96% good/excellent |
| Strnad et al., 2011 [9] | Prospective | 99 HDR BCT 175 PDR BCT | HDR 32 Gy (8 fr) PDR 50 Gy | 5-y IBTR 2.9% 5-y LRFS 98% 5-y OS 97% 5-y DFS 96% | ≥G3 fibrosis 1(0.4%) ≥G3 telangiectasia 6(2.2%) | 90% good to excellent |
| Shah et al., 2013 [49] | Retrospective | 1449 | 34 Gy (10 fr) | 5-y IBTR rate 3.8% | overall fat necrosis rate 2.5% overall infections rate 9.6% overall symptomatic seroma rate 13.4% 2-y symptomatic seroma rate 0.6 % | 5-y good/excellent 91.3% 6-y good/excellent 90.5% 7-y good/excellent 90.6 % |
| Rabinovitch et al., 2014 [50] White et al., 2016 [51] RTOG 95-17 | Prospective | 65 HDR BCT 33 LDR BCT | HDR 34 Gy (10 fr) LDR 45 Gy (3.5-6d) | 10-y IBR 5.2% 10-y LRR 3.1% 10-y DFS 69.8% 10-y OS 78.0%, | G1-2 skin toxicity 78% G3 13% (no G4) skin dimpling/indentation 37% fibrosis 45% telangiectasias 45% skin catheter marks 54% symptomatic fat necrosis 15% Breast asymmetry 73% | 66–68% excellent-to-good |
| Wobb et al., 2016 [52] | Prospective | 481 (40% interstitial 60% applicator-based) | Not specified | 10-y IBTR rate 4% 10-y DFS 91% 10-y OS 75% | 14.4% ≥G2 seroma 12.3% telangiectasia 10.2% symptomatic fat necrosis 5.8% hyperpigmentation 3.3% infection rates | 95% good-to-excellent |
| Strnad et al., 2016 [20] Polgar et al., 2017 [15] GEC-ESTRO Trial | Prospective | 633 | 32 Gy (8 fr) 30.1 Gy (7 fr) | Cumulative incidence of local recurrence 1.44% | No G4 late toxicity 5-y risk of G2-3 skin late toxicity 3.2% 5-y risk of G2-3 subcutaneous tissue late toxicity 7.6% 5-y risk of G3 fibrosis 0% with APBI | 93% good-to-excellent |
| Cozzi et al., 2018 [53] | Retrospective | 83 (59 primary BC 24 recurrent BC) | 32 Gy (8 fr) 34 Gy (10 fr) | 3-y OS 87% recurrent BC 3-y DFS 89% recurrent BC 3-y OS 96% primary BC 3-y DFS 97.8% primary BC No local relapses | Acute toxicity: (1.6%) infectious mastitis (primary BC) 7(30.4%) infectious mastitis and 1(4.3%) hematoma (recurrent BC) Late toxicity: (primary/recurrent BC) G0-2 fibrosis 52(94.4%)/7(31.9%) G3 fibrosis 3(5.6%)/11(50%) mastitis 3(5.5%)/6(27.3%) hypochromic skin spots 8(14.8%)/8(36.4%) skin hyperpigmentation 4(7.4%)/3(13.6%) telangiectasia 1(1.9%)/7(3z1.8%) | Primary BC: 11.1% excellent 63% good 1.8% fair 0% poor 4.9%, no ratings available. Recurrent BC: 63% good 27.3% fair 32% poor 7%, no cosmetic ratings available. |
| Hepel et al., 2018 [54] | Prospective | 40 | 28.5 Gy (5 fr) | No local relapses | Acute G0-1 skin reaction 70% Acute G2 skin reaction 28% Acute G3 skin reaction 3% No ≥G3 late toxicity | -- |
| Pohanková et al., 2018 [55] | Retrospective | 125 | 34 Gy (10 fr) | No relapses | 2(1.8%) wound dehiscence 7(6.2%) inflammatory complications 6(4.4%) G1 radiodermatitis 3(2.7%) seroma No ≥G3 late toxicity | 92% excellent or good |
| Khan et al., 2018 [56] | Prospective | 200 | 22.5 Gy (3 fz) | n.1 IBTR n.1 regional nodal failure | Radiation dermatitis 31(15.5%, G3 1(0.5)) Breast pain 31(15.5%) Breast infection 3(1.5%) Breast edema 2(1%) Superficial tissue fibrosis 12(6%) Deep tissue fibrosis 22(11%) Seroma formation 8(4%) Hyperpigmentation 3(1.5%) Fat necrosis 1(0.5%) Nonhealing wound 2(1%, G3 2(1%)) Fatigue 1(0.5%) | 97.25% excellent or good |
| Vicini et al., 2018 [57,58,59] RTOG 0413 | Prospective | 2107 | 34 Gy (10 fr) BCT 38.5 Gy (10 fr) EBRT | 90(4%) IBTR 4.6% 10-y cumulative incidence of IBTR | 845(40%) G1 toxicity 921(44%) G2 toxicity 201(10%) G3 toxicity | Equivalent between APBI and WBI |
| Gaudet et al., 2019 [60] | Retrospective | 364 | 32 Gy (8 fr) | n.14 IBTR 5-y OS 95.1% 10-y OS 92.2% 5-y LRFS 96.2% 10-y LRFS 88.8% | -- | -- |
| Maranzano et al., 2019 [61] | Prospective | 133 | 32 Gy (8 fr) | 3(2%) IBTR 5-y OS 95% 5-y CSS 100% 10-y OS 84.55% 10-y CSS 100% 13-y OS 81.4% 13-y CSS 100% | Late toxicity related to the skin administered dose (≤55% of the PD vs. 55%) | 80% excellent |
| Hannoun-Lévi et al., 2018/2020 [62,63] | Prospective | 26 | 16 Gy (1 fr) | 5-y LRFS 100% 5-y MFS 95.5%, 5-y CSS 100% 5-y OS 88.5% | Acute toxicity G1 75.7% G2 22.8% G3 4.5% 31.8% breast fibrosis 13.6% puncture site inflammation 11.4% skin hyperpigmentation Late toxicity 1 G2 cytosteatonecrosis 2 G1 hypopigmentation (puncture site) 1 G1 breast fibrosis 1 G2 breast fibrosis | 81% excellent 19% good |
| Rodriguez-Ibarria et al., 2020 [64] | Prospective | 182 | 32 Gy (8 fr) | 5-y LR 1.1% 5-y DFS 97.2% 5-y OS 93.2% | n.1 G2 radiodermitis n.1 G2 hyperpigmentation n.3 G2 acute induration no G3 toxicity no G3-4 late toxicity 9(5.5%) breast induration 1(0.6%) chronic hyperpigmentation 4(2.4%) telangiectasia | -- |
| Laplana et al., 2021 [65] | Retrospective | 289 | 32 Gy (8 fr) 34 Gy (10 fr) 16 Gy (1 fr) | 5-y LC 98.9% 5-y DFS 96.7%, 5.y CSS 99.1% 5-y OS 95.6% | 14.8% fibrosis 8.8% skin discoloration at the catheter points 0.5% telangiectasia | 88.3% excellent or good |
| Hepel et al., 2021 [66] | Retrospective | 252 | 34–36 Gy (10 fr) 28.5 Gy (5 fr) | 2-y LRFS 98.3% 5-y LRFS 90.9% | Acute G0-1 radiodermatitis 77% Acute G2 radiodermatitis 19% Acute G3 radiodermatitis 4% G2 late toxicity 8.8% G3 late toxicity 1% | 62% excellent 36% good 2% fair/poor |
| Polgar et al., 2021 [67] | Prospective | 88 | 36.4 Gy (7 fz) | 5-y IBF 4% 10-y IBF 5.8% 20-y IBF 9.6% 5-y DFS 88.8% 10-y DFS 86.2% 20-y DFS 79.7% 5-y OS 93.7% 10-y OS 77.2% 20-y OS 59.5% 5-y CSS 98.4% 10-y CSS 94.9% 20-y CSS 92.6% | G2-3 late skin toxicities 17(13.6%) G2-3 fibrosis 18(14.4%) | 20-y 82.4% excellent or good |
| Garduño-Sánchez et al., 2022 [68] | Prospective | 76 | 32 Gy (4 fz) | Estimated 5-y OS 96.8% 10-y OS 77.7%, 5-y DFS 91.1% 10-y DFS 69.4% | Acute G1-2 dermatitis 51.4% Late thickening of skin 93.3% Late asymmetry 33.3% Late fibrosis 88.9 Late architectural distortion 83.3% Late retractions 44.8% Late liponecrosis 14.8%8.3 (Patient reported) 8.4 (Physician reported) (Assessed by VAS with 0–10 score) | - |
| Study | Type of Study | Number of Patients | Follow Up (m) | Total Dose (Gy) (Dose for Fraction) and Technique | Outcomes: OS, 3rtIBTE-FS § | Toxicities > G3 (%) | Cosmesis Result |
|---|---|---|---|---|---|---|---|
| Maulard C. et al. (1995) [80]. | Retrospective | 38 | 48 | 30 MIB-LDR | 5y-OS: 55% § 21% | 8 (2 pts: skin necrosis, 1 pts: severe breast pain) | 4 pts: good, 20 pts: acceptable, 9 pts: mediocre. |
| Hannoun-Levi J.M. et al. (2004) [81]. | Retrospective | 69 | 50.2 | 30–50 MIB-LDR | 91.8% (5y-OS) § 77.4% | 10.2 (2 Pts: necrosis requiring surgery) | Not reported |
| Niehoff P. et al. (2006) [82]. | Retrospective | 19 | 36 | 28 (2.5 BID) MIB-HDR/PDR | 68.7% (1y-OS) § 62.5% | 5 (1 pts: skin ulceration) | Not evaluated |
| Chadha M. et al. (2008) [83]. | Retrospective | 15 | 36 | 30–45 MIB-LDR | 100% (3y-OS) § 89% | 0 | 100% pts: Good or excellent |
| Guix B. et al. (2009) [84]. | Retrospective | 36 | 89 | 30 (2.5 BID) | 96.7% (10y-OS) § 89.4% | 0 | 96% pts: satisfactory |
| Hannoun-Levi J.M. et al. (2011) [85]. | Retrospective | 42 | 21 | 34 (3.4 BID) MIB-HDR | not reported § 3% | Not reported | 100% pts: satisfactory |
| Kauer-dorner D. et al. (2012) [86]. | Prospective | 39 | 57 | 34 (0.6–1) MIB-PDR | 87% (5y-OS) § 93 | 16.7 (1pts: breast fibrosis. 32pts: pain) | 3pts: excellent, 6 pts: good, 9pts: fair, 1pts: unacceptable |
| Hannoun-Levi J.M. et al. GEC-ESTRO (2013) [11]. | Prospective | 217 | 47 | 32 (4 BID) MIB-HDR 50 (0.6–1) MIB-LDR | 76.4% (10y-OS) § 94.4% | 10% grade 31% grade 4 (ulceration) | 52 pts: excellent, 40 pts: good, 14 pts: fair, 2 pts: poor |
| Smanyko V. et al. (2019) [87]. | Prospective | 195 | 52 | 22 (4.4 BID) MIB-HDR | 81% (5y-OS) § 94% | 8 | 70%: good |
| Montagne L. et al. (2019) [88]. | Retrospective | 159 | 71 | 28–34 MIB-HDR 30–55 MIB-LDR | 91.2% (6y-OS) § 97.4% | 1 pts: grade 4 ulceration | 122 pts: excellent/good. 6 pts: poor |
| Forster T. et al. (2019) [89]. | Retrospective | 19 | 65 | 49.8–50.4 (0.5–0.7) MIB-LDR 34.2–32 (3.4–3.8) MIB-HDR | 100% (10y-OS) § 100% | 0 | Not reported |
| Cozzi S. et al. (2019) [90]. | Retrospective | 40 | 61.5 | 32–34 (4–3.4 BID) MIB-HDR | 85.3% (5y-OS) § 96% | 3pts: 11 pts fibrosis G3, 3pts: fibrosis G4 | 100% satisfactory |
| Vavassori A. et al. (2020) [91]. | Retrospective | 31 | 73.7 | 34 (3.4 BID) MIB-HDR | 87.1% 85y-OS § 90.3% | 0 | 100% good |
| Chatzikonstantinou G. et al. (2021) [92]. | Retrospective | 20 | 69.6 | 32 (4 BID) MIB-HDR | 92.3% (5y-OS) § 86.8% | 0 | 6pts: excellent, 6pts: good, 3 pts: fair, 1 pt: poor |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cozzi, S.; Augugliaro, M.; Ciammella, P.; Botti, A.; Trojani, V.; Najafi, M.; Blandino, G.; Ruggieri, M.P.; Giaccherini, L.; Alì, E.; et al. The Role of Interstitial Brachytherapy for Breast Cancer Treatment: An Overview of Indications, Applications, and Technical Notes. Cancers 2022, 14, 2564. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102564
Cozzi S, Augugliaro M, Ciammella P, Botti A, Trojani V, Najafi M, Blandino G, Ruggieri MP, Giaccherini L, Alì E, et al. The Role of Interstitial Brachytherapy for Breast Cancer Treatment: An Overview of Indications, Applications, and Technical Notes. Cancers. 2022; 14(10):2564. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102564
Chicago/Turabian StyleCozzi, Salvatore, Matteo Augugliaro, Patrizia Ciammella, Andrea Botti, Valeria Trojani, Masoumeh Najafi, Gladys Blandino, Maria Paola Ruggieri, Lucia Giaccherini, Emanuele Alì, and et al. 2022. "The Role of Interstitial Brachytherapy for Breast Cancer Treatment: An Overview of Indications, Applications, and Technical Notes" Cancers 14, no. 10: 2564. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102564