
Pain after Interventional Radiology in Oncology: A Case-Control Study from a 5-Year Cohort

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Procedures
2.2. Design of the Studies
2.3. Outcomes
2.4. Statistical Analysis
3. Results
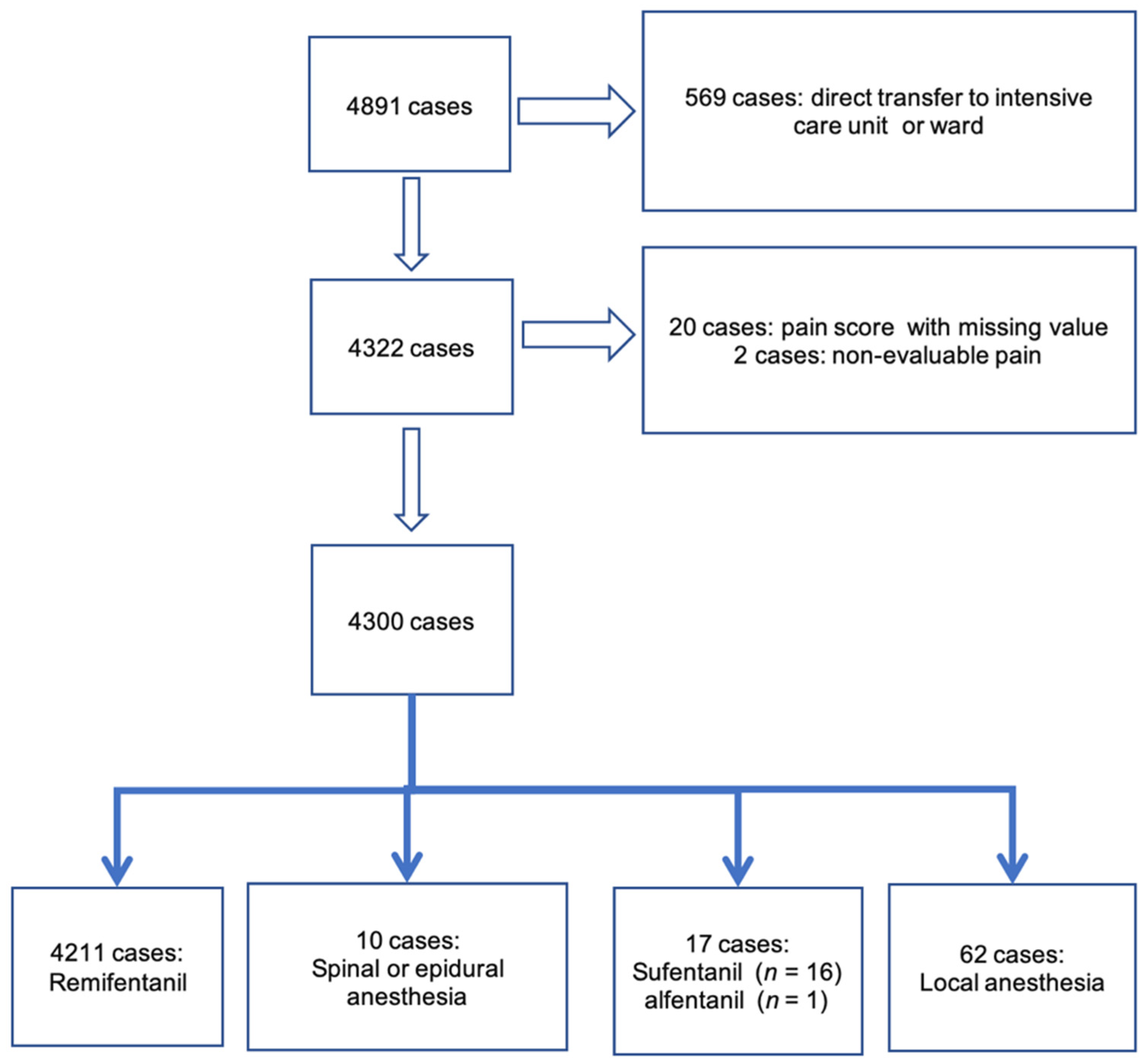
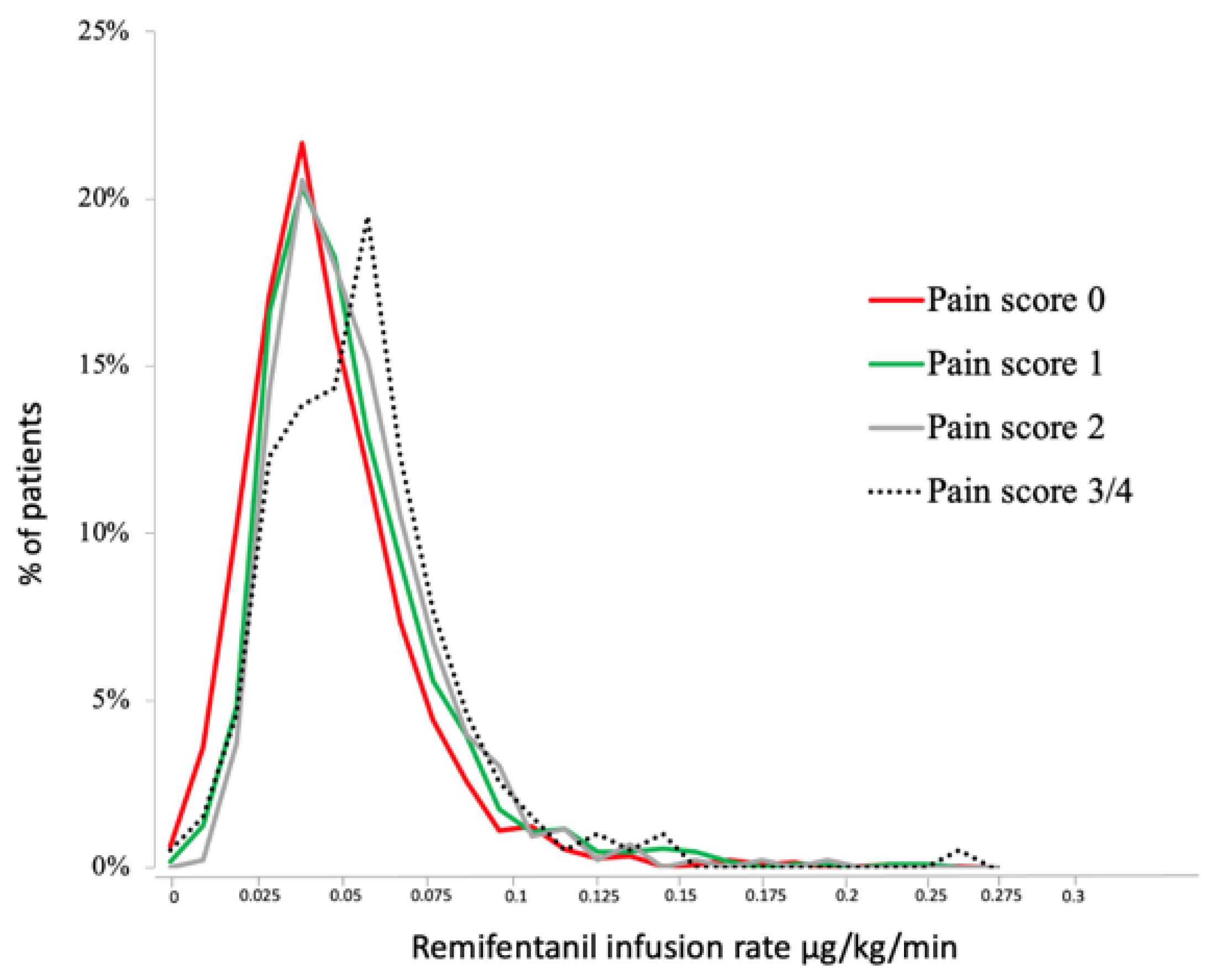
3.1. Cohort Study
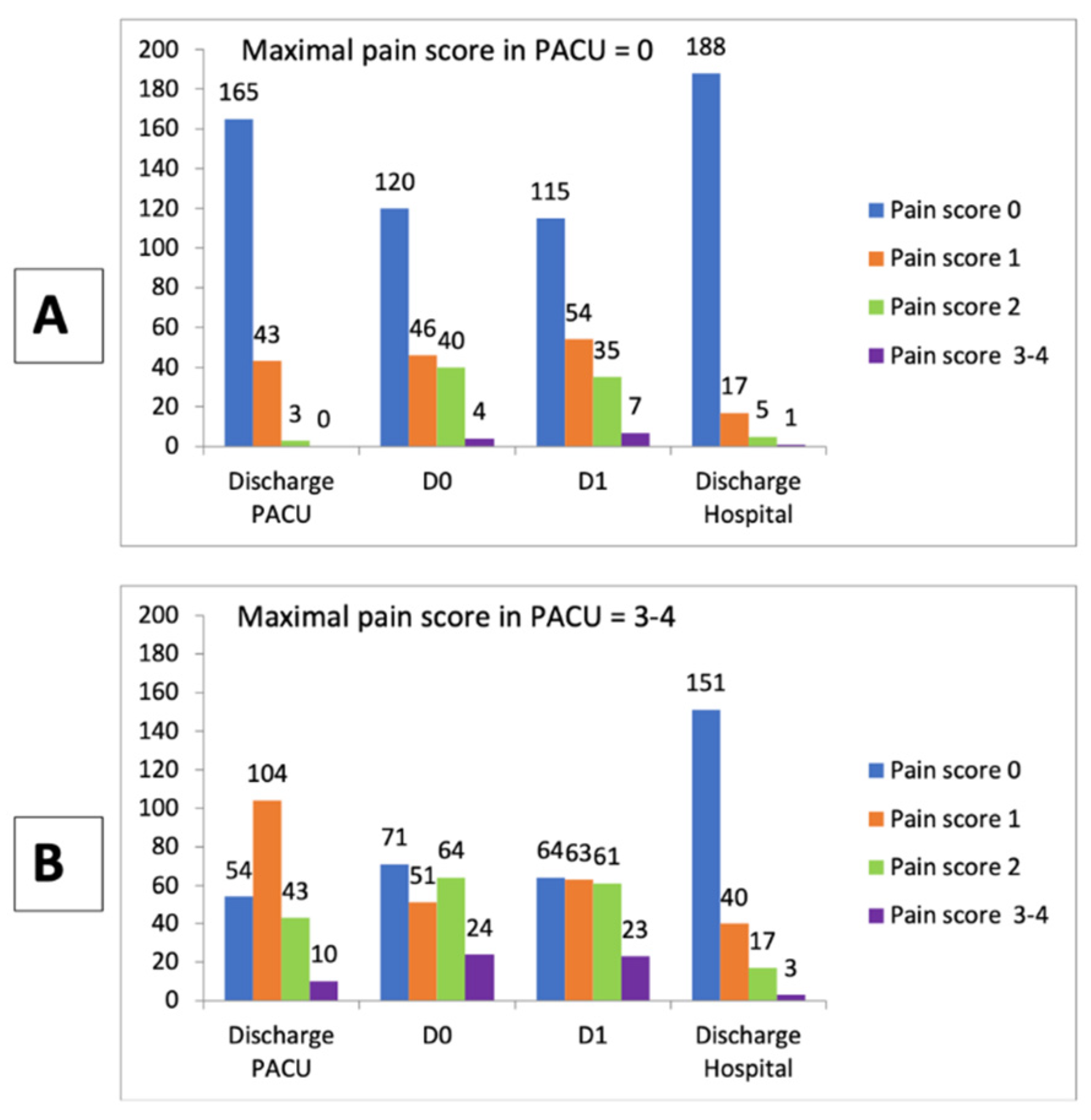
3.2. Case-Control Stud
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cashman, J.N.; Ng, L. The management of peri- and postprocedural pain in interventional radiology: A narrative review. Pain Manag. 2017, 7, 523–535. [Google Scholar] [CrossRef] [PubMed]
- England, A.; Tam, C.L.; Thacker, D.E.; Walker, A.L.; Parkinson, A.S.; Demello, W.; Bradley, A.; Tuck, J.; Laasch, H.-U.; Butterfield, J.; et al. Patterns, incidence and predictive factors for pain after interventional radiology. Clin. Radiol. 2005, 60, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Faramarzalian, A.; Armitage, K.B.; Kapoor, B.; Kalva, S.P. Medical management of tumor lysis syndrome, postprocedural pain, and venous thromboembolism following interventional radiology procedures. Semin. Interv. Radiol. 2015, 32, 209–216. [Google Scholar]
- Guo, J.-G.; Zhao, L.-P.; Rao, Y.-F.; Gao, Y.-P.; Guo, X.-J.; Zhou, T.-Y.; Feng, Z.-Y.; Sun, J.-H.; Lu, X.-Y. Novel multimodal analgesia regimen improves post-TACE pain in patients with hepatocellular carcinoma. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Garnon, J.; Meylheuc, L.; Cazzato, R.L.; Dalili, D.; Koch, G.; Auloge, P.; Bayle, B.; Gangi, A. Percutaneous extra-spinal cementoplasty in patients with cancer: A systematic review of procedural details and clinical outcomes. Diagn. Interv. Imaging 2019, 100, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Shiwani, T.H.; Shiwani, H. Intra-arterial anaesthetics for pain control in arterial embolisation procedures: A systematic review and meta-analysis. CVIR Endovasc. 2021, 4, 6. [Google Scholar] [CrossRef] [PubMed]
- Motamed, C.; Bourgain, J.L. An anaesthesia information management system as a tool for a quality assurance program: 10 years of experience. Anaesth. Crit. Care Pain Med. 2016, 35, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Weil, G.; Motamed, C.; Eghiaian, A.; Guye, M.L.; Bourgain, J.L. The use of a clinical database in an anesthesia unit: Focus on its limits. J. Clin. Monit. Comput. 2015, 29, 163–167. [Google Scholar] [CrossRef]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L. Sex, gender, and pain: A review of recent clinical and experimental findings. J. Pain 2009, 10, 447–485. [Google Scholar] [CrossRef] [Green Version]
- Lawal, O.D.; Gold, J.; Murthy, A.; Ruchi, R.; Bavry, E.; Hume, A.L.; Lewkowitz, A.K.; Brothers, T.; Wen, X. Rate and Risk Factors Associated With Prolonged Opioid Use After Surgery: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e207367. [Google Scholar] [CrossRef]
- Sundararajan, S.H.; Calamita, S.; Girgis, P.; Ngo, G.; Ranganathan, S.; Giglio, M.; Gendel, V.; Goyal, S.; Nosher, J.; Roychowdhury, S. Sequential Interventional Management of Osseous Neoplasms via Embolization, Cryoablation, and Osteoplasty. J. Oncol. 2019, 2019, 5247837. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Silverman, S.M.; Hansen, H.; Patel, V.B.; Manchikanti, L. A comprehensive review of opioid-induced hyperalgesia. Pain Physician 2011, 14, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Motamed, C.; Salazar, G.; Bourgain, J.-L. Incidence of severe postoperative pain after cancer surgery despite intraoperative anticipation: A case controlled study. Bull. Cancer 2010, 97, E37–E41. [Google Scholar] [CrossRef] [PubMed]
- Andreano, A.; Galimberti, S.; Franza, E.; Knavel, E.M.; Sironi, S.; Lee, F.T.; Meloni, M.F. Percutaneous microwave ablation of hepatic tumors: Prospective evaluation of postablation syndrome and postprocedural pain. J. Vasc. Interv. Radiol. 2014, 25, 97–105.E2. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Fu, G.; Li, B.; Li, Y.; Yang, X. Comparison of the effects of minimally invasive percutaneous pedicle screws osteosynthesis and open surgery on repairing the pain, inflammation and recovery of thoracolumbar vertebra fracture. Exp. Ther. Med. 2017, 14, 4091–4096. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, G.; Froud, T.; Lo, K.; Barbery, K.J.; Perez-Rojas, E.; Yrizarry, J. Pain analysis in patients with hepatocellular carcinoma: Irreversible electroporation versus radiofrequency ablation-initial observations. Cardiovasc. Interv. Radiol. 2013, 36, 176–182. [Google Scholar] [CrossRef]
- Fletcher, D.; Martinez, V. Opioid-induced hyperalgesia in patients after surgery: A systematic review and a meta-analysis. Br. J. Anaesth. 2014, 112, 991–1004. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Lim, H.-S.; Kim, M.-J.; Jeong, W.; Ko, S. High-dose intraoperative remifentanil infusion increases early postoperative analgesic consumption: A prospective, randomized, double-blind controlled study. J. Anesth. 2018, 32, 886–892. [Google Scholar] [CrossRef]
- Lo, C.; Schwindt, S.; Sharma, R.; Dubé, R.; Faraoni, D.; Steinberg, B.E.; Brown, S. Association Between Intraoperative Remifentanil Dosage and Postoperative Opioid Consumption in Adolescent Idiopathic Spine Surgery: A Retrospective Cohort Study. Anesth. Analg. 2021, 133, 984–990. [Google Scholar] [CrossRef]
- Aubrun, F.; Nouette-Gaulain, K.; Fletcher, D.; Belbachir, A.; Beloeil, H.; Carles, M.; Cuvillon, P.; Dadure, C.; Lebuffe, G.; Marret, E.; et al. Revision of expert panel’s guidelines on postoperative pain management. Anaesth. Crit. Care Pain Med. 2019, 38, 405–411. [Google Scholar] [CrossRef]
- Lv, N.; Kong, Y.; Mu, L.; Pan, T.; Xie, Q.; Zhao, M. Effect of perioperative parecoxib sodium on postoperative pain control for transcatheter arterial chemoembolization for inoperable hepatocellular carcinoma: A prospective randomized trial. Eur. Radiol. 2016, 26, 3492–3499. [Google Scholar] [CrossRef] [PubMed]
- Barragán-Campos, H.M.; Vallée, J.-N.; Lo, D.; Cormier, E.; Jean, B.; Rose, M.; Astagneau, P.; Chiras, J. Percutaneous vertebroplasty for spinal metastases: Complications. Radiology 2006, 238, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, C.W.; Reding, O.; Holmdahl, I.; Keosaian, J.; Xuan, Z.; McAneny, D.; Larochelle, M.; Liebschut, J. Opioid analgesic use after ambulatory surgery: A descriptive prospective cohort study of factors associated with quantities prescribed and consumed. BMJ Open 2021, 11, e047928. [Google Scholar] [CrossRef] [PubMed]
- Martinez, V.; Baudic, S.; Fletcher, D. Chronic postsurgical pain. Ann. Fr. Anesth. Reanim. 2013, 32, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Edgley, C.; Hogg, M.; De Silva, A.; Braat, S.; Bucknill, A.; Leslie, K. Severe acute pain and persistent post-surgical pain in orthopaedic trauma patients: A cohort study. Br. J. Anaesth. 2019, 123, 350–359. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Number of Patients | Number (%) of Patients/Pain Score | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3–4 | |||||
| Demographic Caracteristics | Sex | Female, n (%) | 2117 | 1260 (59.5) | 523 (24.7) | 208 (9.8) | 126 (6.0) | 0.04 |
| Male, n (%) | 2094 | 1274 (60.8) | 515 (24.6) | 220 (10.5) | 85 (4.1) | |||
| Age | Years, mean (SD) | 4211 | 60 (14) | 60 (15) | 59 (14) | 55 (14) | 0.0001 | |
| Duration | Minutes, mean (SD) | 4211 | 131 (53) | 143 (51) | 143 (50) | 155 (62) | 0.0001 | |
| Weight | kg, mean (SD) | 4211 | 71 (16) | 71 (17) | 69 (15) | 69 (15) | 0.07 | |
| Height | cm, mean (SD) | 4211 | 170 (9) | 169 (9) | 168 (9) | 168 (9) | 0.04 | |
| Type of Anesthesia, n (%) | General | 2966 | 1658 (55.9) | 801 (7.0) | 328 (11.1) | 179 (6.0) | 0.0001 | |
| Sedation | 1203 | 850 (70.7) | 225 (18.7) | 97 (8.1) | 31 (2.6) | GA versus other types of anesthesia | ||
| Regional and local anesthesia * | 41 | 22 (53.7) | 12 (29.3) | 2 (4.9) | 1 (2.4) | |||
| Intraoperative Analgesic | Paracetamol | n (%) | 3942 (100) | 2363 (93.3) | 979 (94.3) | 409 (95.5) | 191 (91) | 0.0399 |
| Dose in mg, mean (SD) | 0.99 (0.06) | 0.99 (0.05) | 0.99 (0.06) | 0.99 (0.06) | 0.99 (0.06) | |||
| Tramadol | n (%) | 3197 (100) | 1923 (75.9) | 817 (78.7) | 321 (75) | 136 (65) | 0.2688 | |
| Dose in mg, mean (SD) | 95 (15) | 95 (15) | 95 (15) | 94 (17) | 96 (14) | |||
| Ketoprofen | n (%) | 1914 (100) | 1098 (43.3) | 501 (48.3) | 241 (56.3) | 74 (35) | 0.0001 | |
| Dose in mg, mean (SD) | 95 (15) | 95 (15) | 96 (14) | 94 (17) | 97 (11) | |||
| Ketamine | n (%) | 2009 (100) | 1134 (44.7) | 545 (52.5) | 245 (57.24) | 85 (41) | 0.0001 | |
| Dose in mg, mean (SD) | 20 (10) | 19 (7) | 20 (9) | 18 (6) | 20 (7) | |||
| Nefopam | n (%) | 3478 (100) | 2054 (81) | 912 (87.9) | 353 (82.5) | 159 (75) | 0.0001 | |
| Dose in mg, mean (SD) | 20 (1) | 20 (2) | 20 (1) | 20 (0) | 20 (0) | |||
| Morphine | n (%) | 2171 (100) | 1214 (48) | 588 (57) | 247 (58) | 122 (58) | 0.0001 | |
| Dose in mg, mean (SD) | 5.1 (2.4) | 4.8 (2.1) | 4.9 (2.2) | 5.5 (2.9) | 5.8 (2.8) | |||
| Procedure by Type | Embolization | Chemo-embolization | 307 | 202 (65.8) | 60 (19.5) | 36 (11.7) | 9 (2.9) | N.A. |
| Arterial embolization | 246 | 149 (60.6) | 51 (20.7) | 29 (11.8) | 17 (6.9) | N.A. | ||
| Bone treatment | Cementoplasty total | 1036 | 622 (60.0) | 260 (25.1) | 98 (9.5) | 56 (5.4) | N.A. | |
| Osteosynthesis | 148 | 68 (45.9) | 38 (25.7) | 28 (18.9) | 14 (9.5) | N.A. | ||
| Tumor ablation | Cryotherapy | 709 | 382 53.9) | 202 28.5) | 82 (11.6) | 43 (6.1) | N.A. | |
| Microwave | 88 | 41 (46.6) | 31 (35.2) | 12 (13.6) | 4 (4.5) | N.A. | ||
| Radiofrequency | 647 | 353 (54.6) | 182 (28.1) | 78 (12.1) | 34 (5.3) | N.A. | ||
| Biopsy | 123 | 85 (69.1) | 27 (22.0) | 6 (4.9) | 5 (4.1) | N.A. | ||
| Gastrostomy, nephrostomy | 190 | 137 (72.1) | 36 (18.9) | 15 (7.9) | 2 (1.1) | N.A. | ||
| Biliary prosthesis or drainage | 300 | 177 (59.0 | 82 (27.3) | 27 (9.0) | 14 (4.7) | N.A. | ||
| Vascular ** | 310 | 236 (76.1) | 46 (14.8) | 15 (4.8) | 13 (4.2) | N.A. | ||
| Others *** | 107 | 82 (76.6) | 23 (21.5) | 2 (1.9) | 0.0 | N.A. | ||
| Parameters | Crude Odds Ratio [95% CI] | p-Value | Adjusted * Odds Ratio [95% CI] | p-Value |
|---|---|---|---|---|
| Duration of the procedure (minutes) | ||||
| First tercile (duration < 118 min) | Ref. | 0.016 | Ref. | 0.038 |
| Second tercile (118 min ≤ duration < 160 min) | 1.01 [0.63–1.61] | 0.94 [0.57–1.54] | ||
| Third tercile (duration ≥ 160 min) | 1.83 [1.14–2.94] | 1.70 [1.03–2.83] | ||
| Weight (kg) | ||||
| First tercile (weight < 62 kg) | Ref. | 0.919 | - | - |
| Second tercile (62 kg ≤ weight < 75 kg) | 1.00 [0.63–1.60] | - | ||
| Third tercile weight ≥ 75 kg) | 0.92 [0.58–1.47] | - | ||
| Height (m) | ||||
| First tercile (height < 1.64 m) | Ref. | 0.709 | - | - |
| Second tercile (1.64 m ≤ height < 1.75 m) | 0.84 [0.52–1.35] | - | ||
| Third tercile (height ≥ 1.75 m) | 0.85 [0.53–1.34] | - | ||
| Body mass index (BMI, kg/m²) | ||||
| Underweight (BMI < 18.5) | Ref. | 0.723 | - | - |
| Normal (18.5 ≤ BMI < 25) | 0.92 [0.46–1.86] | - | ||
| Overweight (25 ≤ BMI < 30) | 1.21 [0.57–2.58] | - | ||
| Obese (BMI ≥ 30) | 0.97 [0.43–2.21] | - | ||
| ASA Physical Status Classification System | ||||
| ASA I or ASA III | Ref. | 0.601 | - | - |
| ASA III or ASA IV or ASA V | 1.12 [0.74–1.68] | - | ||
| Anesthesia | ||||
| No general anesthesia | Ref. | 0.016 | Ref. | 0.022 |
| General anesthesia | 1.83 [1.12–2.98] | 1.84 [1.09–3.10] | ||
| Remifentanil dose (µg/kg/min) | ||||
| Low dose (dose < 0.032 µg/kg/min) | Ref. | 0.019 | Ref. | 0.005 |
| Medium dose (0.032 µg/kg/min ≤ dose < 0.043 µg/kg/min) | 0.98 [0.54–1.80] | 1.16 [0.62–2.20] | ||
| High dose (0.043 µg/kg/min ≤ dose < 0.055 µg/kg/min) | 1.73 [0.92–3.24] | 1.99 [1.03–3.83] | ||
| Very high dose (dose ≥ 0.055 µg/kg/min) | 1.90 [1.18–3.08] | 2.33 [1.39–3.88] | ||
| Intraoperative medication (yes/no) | ||||
| Paracetamol | 0.53 [0.25–1.13] | 0.098 | - | - |
| Nefopam | 0.65 [0.41–1.04] | 0.075 | - | - |
| Tramadol | 1.02 [0.69–1.52] | 0.919 | - | - |
| Ketoprofen (NSAID) | 0.53 [0.36–0.78] | 0.001 | 0.48 [0.32–0.73] | 0.001 |
| Morphine | 1.34 [0.91–1.96] | 0.142 | - | - |
| Ketamine | 0.86 [0.58–1.26] | 0.428 | - | - |
| Intraoperative morphine dose (mg) | 1.07 [1.01–1.14] | 0.023 | - | - |
| Medication taken before the procedure (yes/no) | ||||
| Long-term analgesic use | 1.48 [0.87–2.51] | 0.144 | - | - |
| Long-term use of psychotropic drugs | 1.03 [0.66–1.59] | 0.911 | - | - |
| Long-term opioid use | 1.60 [1.06–2.44] | 0.027 | 1.56 [1.00–2.44] | 0.050 |
| Use of benzodiazepines before the procedure | 1.41 [0.79–2.51] | 0.245 | - | - |
| History of anxiety or psychiatric illness | 0.48 [0.22–1.04] | 0.063 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayaden, N.; Sitbon, P.; Pages, A.; Tselikas, L.; Bourgain, J.-L. Pain after Interventional Radiology in Oncology: A Case-Control Study from a 5-Year Cohort. Cancers 2022, 14, 2576. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112576
Ayaden N, Sitbon P, Pages A, Tselikas L, Bourgain J-L. Pain after Interventional Radiology in Oncology: A Case-Control Study from a 5-Year Cohort. Cancers. 2022; 14(11):2576. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112576
Chicago/Turabian StyleAyaden, Narimane, Philippe Sitbon, Arnaud Pages, Lambros Tselikas, and Jean-Louis Bourgain. 2022. "Pain after Interventional Radiology in Oncology: A Case-Control Study from a 5-Year Cohort" Cancers 14, no. 11: 2576. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112576