
Neoadjuvant Carboplatin/Paclitaxel versus 5-Fluorouracil/Cisplatin in Combination with Radiotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Multicenter Comparative Study

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Neoadjuvant Chemoradiotherapy and Surgery
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Neoadjuvant Chemoradiotherapy Related Outcomes
3.3. Perioperative and Pathology Outcomes
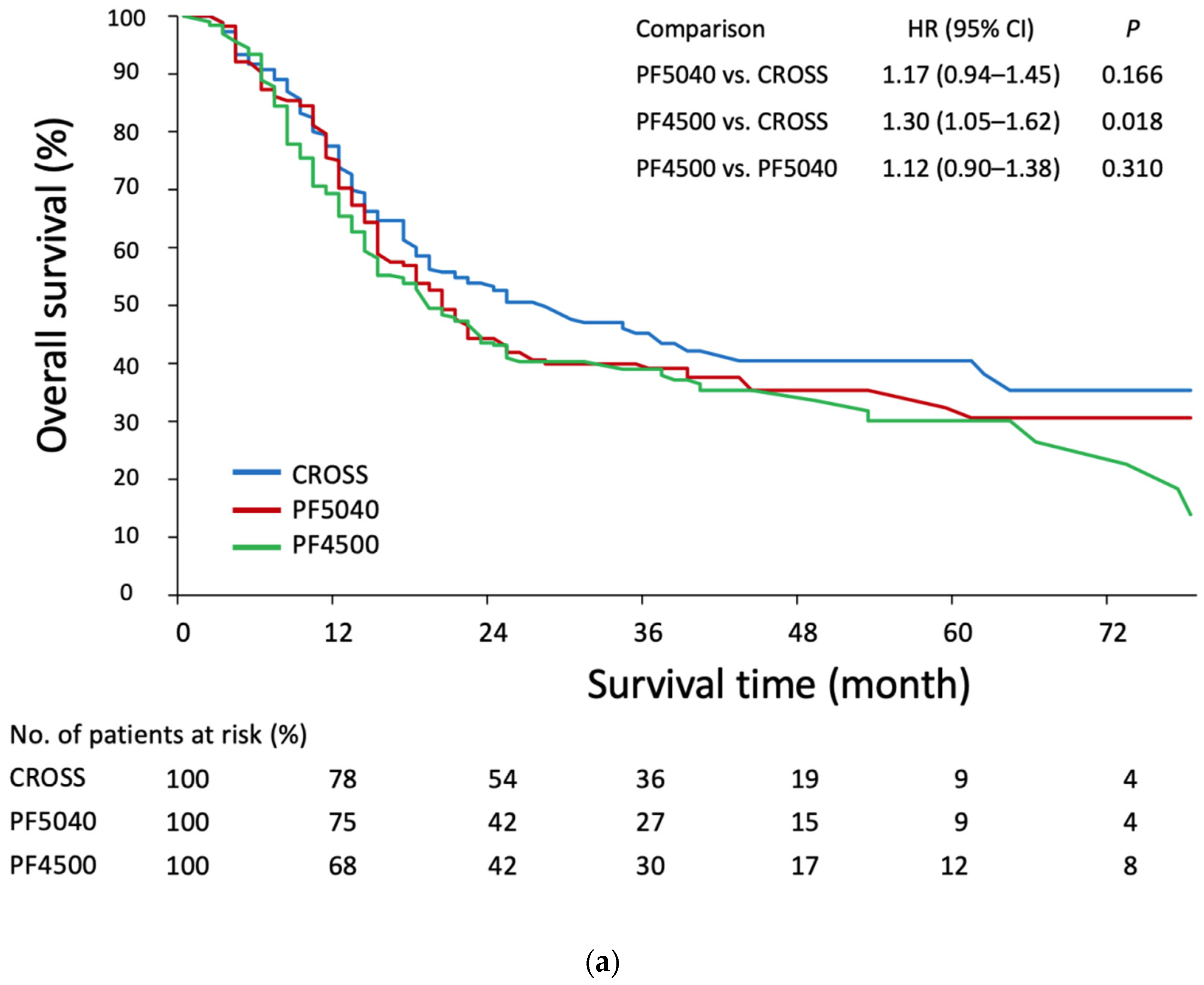
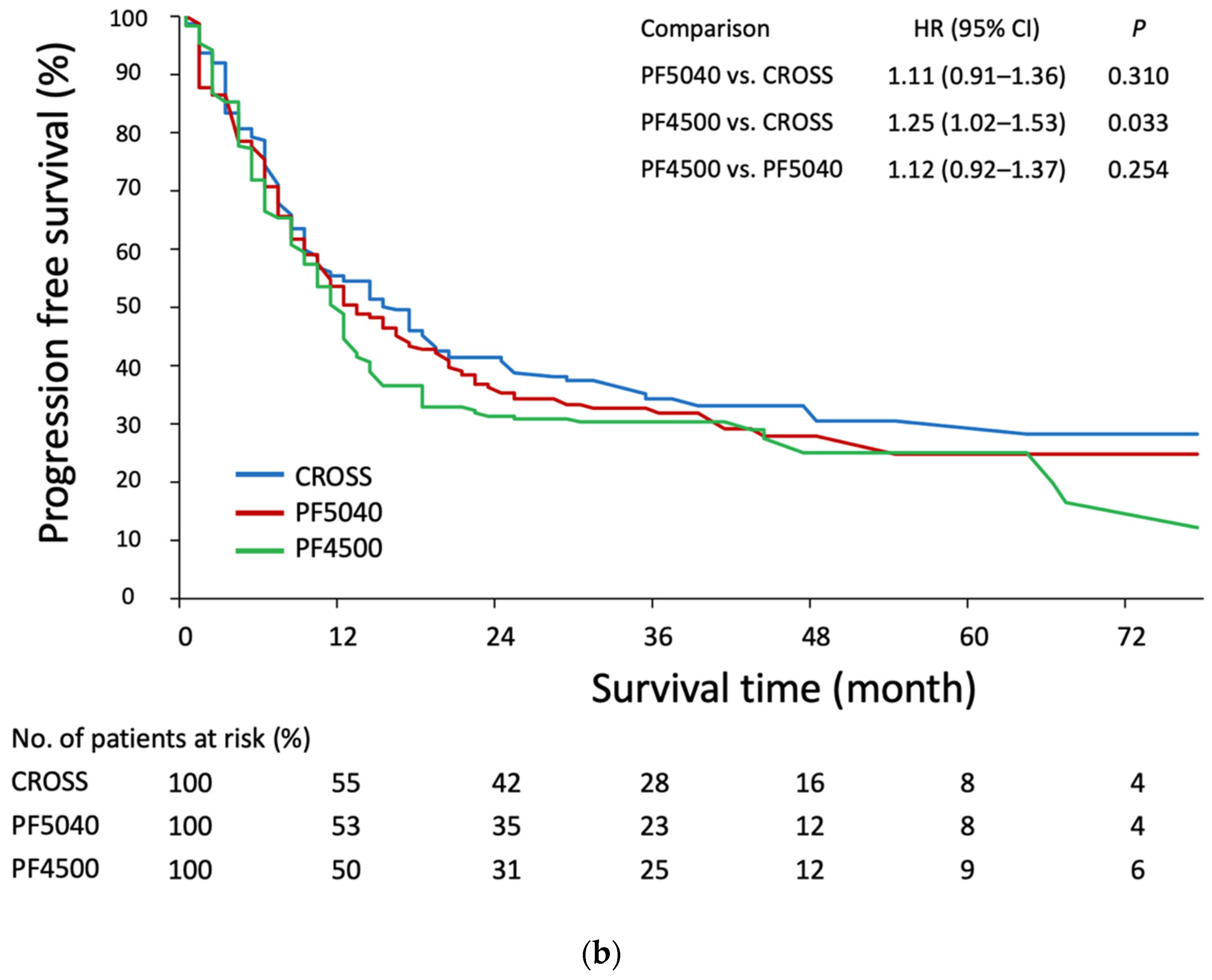
3.4. Survival Analysis
3.5. Survival Analysis in the CROSS and PF5040 Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, K.K.W.; Saluja, R.; Delos Santos, K.; Lien, K.; Shah, K.; Cramarossa, G.; Zhu, X.; Wong, R.K.S. Neoadjuvant treatments for locally advanced, resectable esophageal cancer: A network meta-analysis. Int. J. Cancer 2018, 143, 430–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, T.; Pai, E.; Singh, R.; Francis, N.J.; Pandey, M. Neoadjuvant strategies in resectable carcinoma esophagus: A meta-analysis of randomized trials. World J. Surg. Oncol. 2020, 18, 59. [Google Scholar] [CrossRef] [PubMed]
- Muro, K.; Lordick, F.; Tsushima, T.; Pentheroudakis, G.; Baba, E.; Lu, Z.; Cho, B.C.; Nor, I.M.; Ng, M.; Chen, L.T.; et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic oesophageal cancer: A JSMO–ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann. Oncol. 2019, 30, 34–43. [Google Scholar] [CrossRef]
- Lordick, F.; Mariette, C.; Haustermans, K.; Obermannová, R.; Arnold, D. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v50–v57. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Esophageal and Esophagogastric Junction Cancers. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1433 (accessed on 12 May 2022).
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [Green Version]
- Tepper, J.; Krasna, M.J.; Niedzwiecki, D.; Hollis, D.; Reed, C.E.; Goldberg, R.; Kiel, K.; Willett, C.; Sugarbaker, D.; Mayer, R. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J. Clin. Oncol. 2008, 26, 1086–1092. [Google Scholar] [CrossRef] [Green Version]
- Bedenne, L.; Michel, P.; Bouche, O.; Milan, C.; Mariette, C.; Conroy, T.; Pezet, D.; Roullet, B.; Seitz, J.F.; Herr, J.P.; et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J. Clin. Oncol. 2007, 25, 1160–1168. [Google Scholar] [CrossRef] [Green Version]
- Minsky, B.D.; Pajak, T.F.; Ginsberg, R.J.; Pisansky, T.M.; Martenson, J.; Komaki, R.; Okawara, G.; Rosenthal, S.A.; Kelsen, D.P. INT 0123 (Radiation Therapy Oncology Group 94-05) phase III trial of combined-modality therapy for esophageal cancer: High-dose versus standard-dose radiation therapy. J. Clin. Oncol. 2002, 20, 1167–1174. [Google Scholar] [CrossRef]
- Blom, R.L.G.M.; Sosef, M.N.; Nap, M.; Lammering, G.; Van Den Berkmortel, F.; Hulshof, M.C.C.M.; Meijer, S.L.; Wilmink, H.W.; Van Berge Henegouwen, M.I. Comparison of two neoadjuvant chemoradiotherapy regimens in patients with potentially curable esophageal carcinoma. Dis. Esophagus 2014, 27, 380–387. [Google Scholar] [CrossRef]
- Honing, J.; Smit, J.K.; Muijs, C.T.; Burgerhof, J.G.M.; De Groot, J.W.; Paardekooper, G.; Muller, K.; Woutersen, D.; Legdeur, M.J.C.; Fiets, W.E.; et al. A comparison of carboplatin and paclitaxel with cisplatinum and 5-fluorouracil in definitive chemoradiation in esophageal cancer patients. Ann. Oncol. 2014, 25, 638–643. [Google Scholar] [CrossRef]
- Huang, T.-C.; Hsu, C.-H.; Lin, C.-C.; Tu, Y.-K. Systematic review and network meta-analysis: Neoadjuvant chemoradiotherapy for locoregional esophageal cancer. Jpn. J. Clin. Oncol. 2015, 45, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Wong, I.Y.H.; Lam, K.O.; Zhang, R.Q.; Chan, W.W.L.; Wong, C.L.Y.; Chan, F.S.Y.; Kwong, D.L.W.; Law, S.Y.K. Neoadjuvant Chemoradiotherapy Using Cisplatin and 5-Fluorouracil (PF) Versus Carboplatin and Paclitaxel (CROSS Regimen) for Esophageal Squamous Cell Carcinoma (ESCC): A Propensity Score-matched Study. Ann. Surg. 2020, 272, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Tamtai, A.; Jiarpinitnun, C.; Hiranyatheb, P.; Unwanatham, N.; Sirachainun, E.; Supsamutchai, C.; Pattaranutaporn, P.; Ngamphaiboon, N. Tolerability and efficacy of concurrent chemoradiotherapy comparing carboplatin/paclitaxel versus platinum/5-FU regimen for locally advanced esophageal and esophagogastric junction cancers. Med. Oncol. 2017, 34, 157. [Google Scholar] [CrossRef] [PubMed]
- Xi, M.; Zhang, P.; Zhang, L.; Yang, Y.D.; Liu, S.L.; Li, Y.; Fu, J.H.; Liu, M.Z. Comparing docetaxel plus cisplatin versus fluorouracil plus cisplatin in esophageal squamous cell carcinoma treated with neoadjuvant chemoradiotherapy. Jpn. J. Clin. Oncol. 2017, 47, 683–689. [Google Scholar] [CrossRef] [Green Version]
- Ma, B.B.; Hui, E.P.; Mok, T.S. Population-based differences in treatment outcome following anticancer drug therapies. Lancet Oncol. 2010, 11, 75–84. [Google Scholar] [CrossRef]
- Zhang, H.Z.; Jin, G.F.; Shen, H.B. Epidemiologic differences in esophageal cancer between Asian and Western populations. Chin. J. Cancer 2012, 31, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Commission of the People’s Republic of China. Chinese guidelines for diagnosis and treatment of esophageal carcinoma 2018 (English version). Chin. J. Cancer Res. 2019, 31, 223–258. [Google Scholar] [CrossRef]
- Metzger, R.; Bollschweiler, E.; Vallböhmer, D.; Maish, M.; DeMeester, T.R.; Hölscher, A.H. High volume centers for esophagectomy: What is the number needed to achieve low postoperative mortality? Dis. Esophagus 2004, 14, 310–314. [Google Scholar] [CrossRef]
- Chang, C.M.; Yin, W.Y.; Wei, C.K.; Wu, C.C.; Su, Y.C.; Yu, C.H.; Lee, C.C. Adjusted Age-Adjusted Charlson Comorbidity Index Score as a Risk Measure of Perioperative Mortality before Cancer Surgery. PLoS ONE 2016, 11, e0148076. [Google Scholar] [CrossRef]
- Van der Schaaf, M.K.; Tilanus, H.W.; van Lanschot, J.J.; Johar, A.M.; Lagergren, P.; Lagergren, J.; Wijnhoven, B.P. The influence of preoperative weight loss on the postoperative course after esophageal cancer resection. J. Thorac. Cardiovasc. Surg. 2014, 147, 490–495. [Google Scholar] [CrossRef] [Green Version]
- Weimann, A.; Braga, M.; Harsanyi, L.; Laviano, A.; Ljungqvist, O.; Soeters, P.D.G.E.M.; Jauch, K.W.; Kemen, M.; Hiesmayr, J.M.; Horbach, T.; et al. ESPEN Guidelines on Enteral Nutrition: Surgery including organ transplantation. Clin. Nutr. 2006, 25, 224–244. [Google Scholar] [CrossRef] [PubMed]
- Van der Sluis, P.C.; Verhage, R.J.; van der Horst, S.; van der Wal, W.M.; Ruurda, J.P.; van Hillegersberg, R. A new clinical scoring system to define pneumonia following esophagectomy for cancer. Dig. Surg. 2014, 31, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.E.; D’Journo, X.B.; Griffin, S.M.; Holscher, A.H.; Hofstetter, W.L.; Jobe, B.A.; et al. International Consensus on Standardization of Data Collection for Complications Associated With Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann. Surg. 2015, 262, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Mandard, A.-M.; Dalibard, F.; Mandard, J.-C.; Marnay, J.; Henry-Amar, M.; Petiot, J.-F.; Roussel, A.; Jacob, J.-H.; Segol, P.; Samama, G.; et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Imai, K.; van Dyk, D.A. Causal Inference with General Treatment Regimes. J. Am. Stat. Assoc. 2004, 99, 854–866. [Google Scholar] [CrossRef]
- Robins, J.M.; Hernan, M.A.; Brumback, B. Marginal structural models and causal inference in epidemiology. Epidemiology 2000, 11, 550–560. [Google Scholar] [CrossRef]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.F.; Chen, H.S.; Wu, S.C.; Chen, H.C.; Hung, W.H.; Lin, C.H.; Wang, B.Y. Esophageal squamous cell carcinoma and prognosis in Taiwan. Cancer Med. 2018, 7, 4193–4201. [Google Scholar] [CrossRef]
- Steber, C.; Hughes, R.T.; McTyre, E.R.; Soike, M.; Farris, M.; Levine, B.J.; Pasche, B.; Levine, E.; Blackstock, A.W. Cisplatin/5-Fluorouracil (5-FU) Versus Carboplatin/Paclitaxel Chemoradiotherapy as Definitive or Pre-Operative Treatment of Esophageal Cancer. Cureus 2021, 13, e12574. [Google Scholar] [CrossRef]
- Yamano, T.; Yoshimura, M.; Kobayashi, M.; Beppu, N.; Hamanaka, M.; Babaya, A.; Tsukamoto, K.; Noda, M.; Matsubara, N.; Tomita, N. Malnutrition in rectal cancer patients receiving preoperative chemoradiotherapy is common and associated with treatment tolerability and anastomotic leakage. Int. J. Colorectal. Dis. 2016, 31, 877–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vetter, D.; Gutschow, C.A. Strategies to prevent anastomotic leakage after esophagectomy and gastric conduit reconstruction. Langenbeck’s Arch. Surg. 2020, 405, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Hinata, N.; Hussein, A.A.; George, S.; Trump, D.L.; Levine, E.G.; Omar, K.; Dasgupta, P.; Khan, M.S.; Hosseini, A.; Wiklund, P.; et al. Impact of suboptimal neoadjuvant chemotherapy on peri-operative outcomes and survival after robot-assisted radical cystectomy: A multicentre multinational study. BJU Int. 2017, 119, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Freischlag, K.; Sun, Z.; Adam, M.A.; Kim, J.; Palta, M.; Czito, B.G.; Migaly, J.; Mantyh, C.R. Association Between Incomplete Neoadjuvant Radiotherapy and Survival for Patients With Locally Advanced Rectal Cancer. JAMA Surg. 2017, 152, 558. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Takeuchi, H.; Mizusawa, J.; Igaki, H.; Ozawa, S.; Abe, T.; Nakamura, K.; Kato, K.; Ando, N.; Kitagawa, Y. Prognostic Impact of Postoperative Morbidity After Esophagectomy for Esophageal Cancer: Exploratory Analysis of JCOG9907. Ann. Surg. 2017, 265, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Booka, E.; Takeuchi, H.; Suda, K.; Fukuda, K.; Nakamura, R.; Wada, N.; Kawakubo, H.; Kitagawa, Y. Meta-analysis of the impact of postoperative complications on survival after oesophagectomy for cancer. BJS Open 2018, 2, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Visser, E.; van Rossum, P.S.N.; Ruurda, J.P.; van Hillegersberg, R. Impact of Lymph Node Yield on Overall Survival in Patients Treated with Neoadjuvant Chemoradiotherapy Followed by Esophagectomy for Cancer: A Population-based Cohort Study in the Netherlands. Ann. Surg. 2017, 266, 863–869. [Google Scholar] [CrossRef]
- Guo, X.; Wang, Z.; Yang, H.; Mao, T.; Chen, Y.; Zhu, C.; Yu, Z.; Han, Y.; Mao, W.; Xiang, J.; et al. Impact of Lymph Node Dissection on Survival after Neoadjuvant Chemoradiotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: From the Results of NEOCRTEC5010, a Randomized Multicenter Study. Ann. Surg. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Before IPTW (Original Cohort) | After IPTW | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CROSS (n = 124) | PF5040 (n = 105) | PF4500 (n = 105) | p Value | MASD | CROSS | PF5040 | PF4500 | p Value | MASD | |
| Male sex | 118 (95) | 92 (88) | 100 (95) | 0.061 | 0.30 | 94.6 | 90.5 | 93.5 | 0.17 | 0.16 |
| Age, years | 57.6 ± 8.9 | 57.3 ± 9.1 | 55.4 ± 9.9 | 0.19 | 0.23 | 57.3 ± 9.1 | 56.7 ± 9.1 | 56.4 ± 9.1 | 0.53 | 0.10 |
| * BMI, kg/m2 | 22.4 ± 3.6 | 22.1 ± 3.2 | 22.4 ± 3.7 | 0.81 | 0.09 | 22.4 ± 3.6 | 22.0 ± 3.1 | 22.6 ± 3.8 | 0.095 | 0.17 |
| ACCI score | 0.050 | 0.23 | 0.7 | 0.07 | ||||||
| 0 | 14 (11) | 10 (10) | 18 (17) | 13.5 | 11.4 | 13.5 | ||||
| 1−2 | 78 (63) | 53 (51) | 62 (59) | 61.1 | 58.0 | 58.5 | ||||
| ≥3 | 32 (26) | 42 (39) | 25 (24) | 25.4 | 30.6 | 28.1 | ||||
| Clinical T stage | 0.12 | 0.17 | 0.38 | 0.15 | ||||||
| 1 | 1 (0.8) | 3 (3) | 1 (1) | 1.1 | 2.9 | 1.6 | ||||
| 2 | 17 (14) | 11 (11) | 24 (23) | 15.7 | 11.2 | 16.0 | ||||
| 3 | 101 (82) | 88 (84) | 79 (75) | 80.3 | 83.9 | 80.9 | ||||
| 4 | 5 (4) | 3 (3) | 1 (1) | 2.9 | 2.0 | 1.5 | ||||
| Clinical N stage | <0.001 | 0.30 | 0.26 | 0.14 | ||||||
| 0 | 3 (2) | 7 (7) | 10 (10) | 3.4 | 6.0 | 6.6 | ||||
| 1 | 36 (29) | 61 (58) a | 46 (44) | 38.6 | 46.6 | 42.4 | ||||
| 2 | 68 (55) | 29 (28) a | 37 (35) a | 46.9 | 38.0 | 41.3 | ||||
| 3 | 17 (14) | 8 (8) | 12 (11) | 11.1 | 9.4 | 9.6 | ||||
| Clinical stage | 0.12 | 0.17 | 0.78 | 0.15 | ||||||
| I | 0 (0) | 1 (1) | 0 (0) | 0.0 | 0.8 | 0.0 | ||||
| II | 11 (9) | 14 (13) | 21 (20) | 12.8 | 12.4 | 14.6 | ||||
| III | 94 (76) | 80 (76) | 71 (68) | 74.7 | 76.3 | 74.3 | ||||
| IV | 19 (15) | 10 (10) | 13 (12) | 12.4 | 10.5 | 11.1 | ||||
| Tumor length, cm | 6.0 ± 2.8 | 5.5 ± 2.6 | 5.4 ± 3.0 | 0.17 | 0.22 | 5.7 ± 2.7 | 5.5 ± 2.6 | 5.6 ± 2.8 | 0.59 | 0.08 |
| Tumor location | 0.85 | 0.02 | 0.77 | 0.11 | ||||||
| Proximal | 26 (21) | 22 (21) | 23 (22) | 19.3 | 22.1 | 23.6 | ||||
| Middle | 61 (49) | 45 (43) | 50 (48) | 47.2 | 43.7 | 44.7 | ||||
| Distal | 37 (30) | 38 (36) | 32 (30) | 33.5 | 34.2 | 31.6 | ||||
| Years of nCRT | <0.001 | 0.53 | <0.001 | 0.29 | ||||||
| 2010–2012 | 3 (2) | 18 (17) a | 25 (23) a | 4.5 | 16.3 a | 16.3 a | ||||
| 2013–2015 | 41 (33) | 22 (21) | 31 (30) | 31.2 | 22.3 | 27.1 | ||||
| 2016–2018 | 80 (65) | 65 (62) | 49 (47) a | 64.3 | 61.4 | 56.6 | ||||
| Variable | CROSS | PF5040 | PF4500 | p Value |
|---|---|---|---|---|
| Chemotherapy completion rate (>80%) | 89.4 | 76.2 a | 92.0 b | <0.001 |
| Radiotherapy dose, cGy | 4401 ± 161 | 4957 ± 247 a | 4426 ± 149 b | <0.001 |
| Weight loss, % | −1.5 ± 5.8 | −3.0 ± 9.4 | −3.4 ± 8.4 a | 0.014 |
| Weight loss >10% | 8.5 | 16.5 a | 15.8 a | 0.01 |
| Surgical resection rate | 76.6 | 72.8 | 69.2 | 0.17 |
| Reason for not undergoing surgery | ||||
| Disease progression | 8.8 | 15.6 | 11.4 | 0.054 |
| Patient refusal | 7.3 | 9.0 | 12.7 | 0.13 |
| Poor physical conditions | 5.7 | 2.0 | 4.0 | 0.1 |
| Death during nCRT | 1.5 | 0.6 | 2.6 | 0.18 |
| Variable | CROSS | PF5040 | PF4500 | p Value |
|---|---|---|---|---|
| Time from termination of nCRT to surgery, days | 65 ± 31 | 61 ± 25 | 65 ± 18 | 0.16 |
| Thoracic approach | 0.2 | |||
| Thoracotomy | 5.0 | 2.5 | 2.0 | |
| Thoracoscopy | 95.0 | 97.5 | 98.0 | |
| Abdominal approach | <0.001 | |||
| Laparotomy | 10.8 | 31.5 a | 35.5 a | |
| Laparoscopy | 89.2 | 68.5 a | 64.5 a | |
| Type of resection | 0.004 | |||
| Ivor Lewis | 9.4 | 6.5 | 1.5 a | |
| McKeown | 90.6 | 93.5 | 98.5 a | |
| Postoperative complications | ||||
| Anastomotic leak | 9.7 | 24.5 a | 27.9 a | <0.001 |
| Chylothorax | 1.4 | 6.7 a | 5.6 | 0.026 |
| Pulmonary | 14.1 | 11.3 | 26.6 ab | <0.001 |
| Complication severity (Clavien-Dindo) | 0.001 | |||
| None | 45.7 | 44.7 | 29.3 ab | |
| Minor (1-3a) | 42.3 | 35.2 | 52.7 b | |
| Major or death (3b-5) | 12.0 | 20.1 | 18.0 | |
| Postoperative stay, days | 20.4 ± 15.2 | 24.2 ± 18.7 | 25.1 ± 17.8 a | 0.019 |
| 30-day mortality rate | 3.2 | 2.4 | 4.9 | 0.47 |
| ypT stage | <0.001 | |||
| T0 | 31.8 | 48.6 a | 38.1 | |
| T1 | 14.3 | 12.5 | 7.6 | |
| T2 | 13.2 | 13.0 | 22.8 ab | |
| T3 | 39.6 | 22.7 a | 21.4 a | |
| T4 | 1.1 | 3.3 | 10.0 ab | |
| ypN stage | <0.001 | |||
| N0 | 76.8 | 76.5 | 64.6 ab | |
| N1 | 18.3 | 18.0 | 23.4 | |
| N2 | 1.8 | 5.6 | 11.2 a | |
| N3 | 3.1 | 0.0 a | 0.8 | |
| ypM stage | 0.002 | |||
| M0 | 100.0 | 94.9 a | 96.5 a | |
| M1 | 0.0 | 5.1 a | 3.5 a | |
| Number of dissected nodes | 27.3 ± 12.8 | 18.4 ± 10.1 a | 23.0 ± 10.6 ab | <0.001 |
| Pathologically positive nodes | 0.64 ± 2.02 | 0.45 ± 1.09 | 0.83 ± 1.59 | 0.078 |
| ypCR | 29.5 | 45.3 a | 31.6 b | 0.002 |
| ypT0N+ | 3.0 | 3.2 | 6.5 | 0.2 |
| Surgical radicality | 0.52 | |||
| R0 | 91.1 | 90.8 | 87.5 | |
| R+ | 8.9 | 9.2 | 12.5 | |
| Tumor regression grade | <0.001 | |||
| TRG1 | 31.8 | 48.6 a | 38.1 | |
| TRG2 | 22.3 | 17.2 | 26.8 | |
| TRG3 | 24.4 | 28.4 | 23.7 | |
| TRG4 | 21.5 | 5.8 a | 11.4 a |
| Subgroup | HR (95% CI) PF5040 versus CROSS | p for Interaction |
|---|---|---|
| ACCI score | 0.19 | |
| 0–2 | 1.29 (1.001–1.66) | |
| ≥3 | 0.92 (0.60–1.42) | |
| Tumor length | 0.22 | |
| <8 cm | 1.10 (0.86–1.40) | |
| ≥8 cm | 1.54 (0.95–2.51) | |
| Years of nCRT | 0.5 | |
| 2010–2014 | 1.03 (0.71–1.51) | |
| 2015–2018 | 1.21 (0.93–1.59) | |
| Chemotherapy completion | <0.001 | |
| No | 3.81 (2.11–6.89) | |
| Yes | 0.88 (0.69–1.13) | |
| Surgical resection | 0.33 | |
| No | 1.36 (0.93–1.99) | |
| Yes | 1.08 (0.83–1.41) | |
| Number of resected nodes | 0.29 | |
| <15 | 0.83 (0.45–1.51) | |
| ≥15 | 1.20 (0.87–1.64) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, X.; Tsai, P.-C.; Chuang, K.-H.; Pai, C.-P.; Hsu, P.-K.; Li, S.-H.; Lu, H.-I.; van Lanschot, J.J.-B.; Chao, Y.-K. Neoadjuvant Carboplatin/Paclitaxel versus 5-Fluorouracil/Cisplatin in Combination with Radiotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Multicenter Comparative Study. Cancers 2022, 14, 2610. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112610
Gao X, Tsai P-C, Chuang K-H, Pai C-P, Hsu P-K, Li S-H, Lu H-I, van Lanschot JJ-B, Chao Y-K. Neoadjuvant Carboplatin/Paclitaxel versus 5-Fluorouracil/Cisplatin in Combination with Radiotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Multicenter Comparative Study. Cancers. 2022; 14(11):2610. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112610
Chicago/Turabian StyleGao, Xing, Ping-Chung Tsai, Kai-Hao Chuang, Chu-Pin Pai, Po-Kuei Hsu, Shau-Hsuan Li, Hung-I Lu, Joseph Jan-Baptist van Lanschot, and Yin-Kai Chao. 2022. "Neoadjuvant Carboplatin/Paclitaxel versus 5-Fluorouracil/Cisplatin in Combination with Radiotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Multicenter Comparative Study" Cancers 14, no. 11: 2610. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112610