A Few-Shot Learning Approach Assists in the Prognosis Prediction of Magnetic Resonance-Guided Focused Ultrasound for the Local Control of Bone Metastatic Lesions

 ,
,  , , ,
, , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Eligibility
2.2. MRgFUS Treatment
2.3. Cytokine Analysis
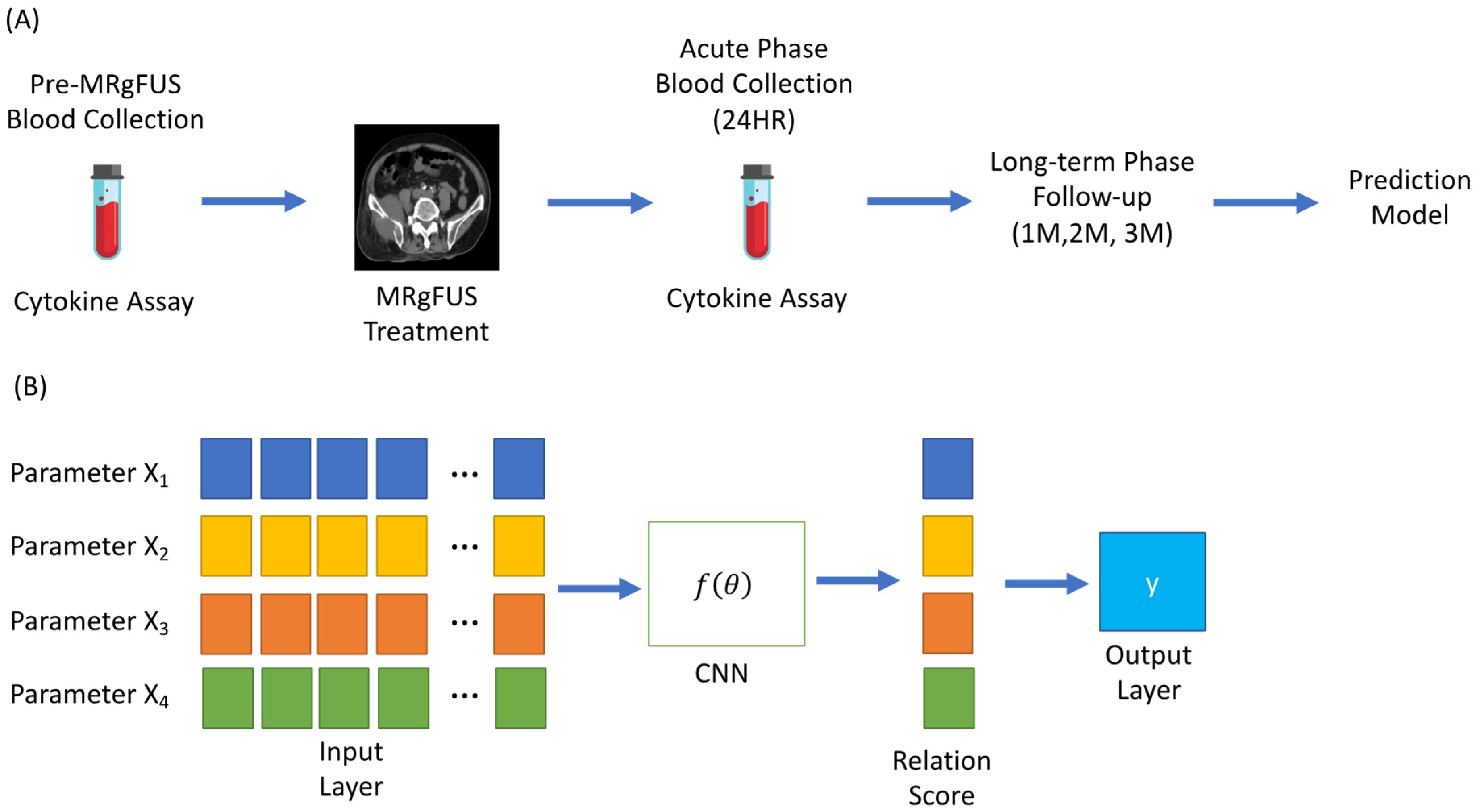
2.4. Few-Shot Learning and Predictive Model Construction
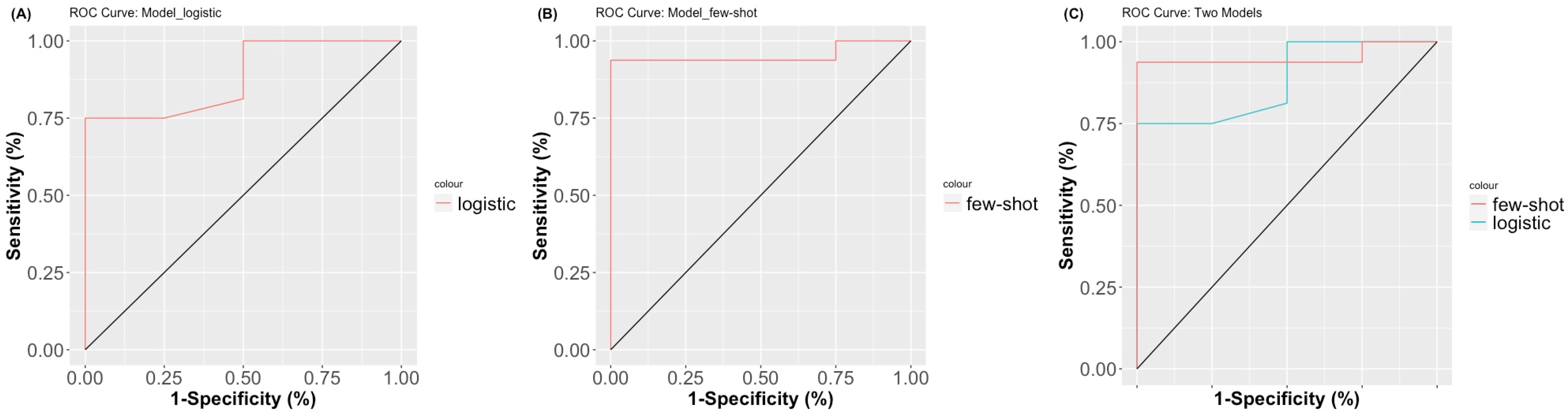
2.5. Model Comparison and Diagnosis
2.6. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Cytokine Changes and Clinical Response
3.3. Treatmet Parameters
3.4. Prediction Model of Clinical Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Falkmer, U.; Järhult, J.; Wersäll, P.; Cavallin-Ståhl, E. A systematic overview of radiation therapy effects in skeletal metastases. Acta Oncol. 2003, 42, 620–633. [Google Scholar] [CrossRef] [Green Version]
- Guo, Q.; Zhang, C.; Guo, X.; Tao, F.; Xu, Y.; Feng, G.; Han, X.; Ren, Z.; Zhang, H.; Zhang, P.; et al. Incidence of bone metastasis and factors contributing to its development and prognosis in newly diagnosed renal cell carcinoma: A population-based study. Cancer Manag. Res. 2018, 10, 2935–2944. [Google Scholar] [CrossRef] [Green Version]
- Macedo, F.; Ladeira, K.; Pinho, F.; Saraiva, N.; Bonito, N.; Pinto, L.; Gonçalves, F. Bone metastases: An overview. Oncol. Rev. 2017, 11, 321. [Google Scholar] [CrossRef] [PubMed]
- Azad, G.K.; Taylor, B.; Rubello, D.; Colletti, P.M.; Goh, V.; Cook, G. Molecular and Functional Imaging of Bone Metastases in Breast and Prostate Cancers. Clin. Nucl. Med. 2016, 41, e44–e50. [Google Scholar] [CrossRef] [PubMed]
- Harries, M.; Taylor, A.; Holmberg, L.; Agbaje, O.; Garmo, H.; Kabilan, S.; Purushotham, A. Incidence of bone metastases and survival after a diagnosis of bone metastases in breast cancer patients. Cancer Epidemiol. 2014, 38, 427–434. [Google Scholar] [CrossRef]
- Arneson, T.J.; Li, S.; Peng, Y.; Weinhandl, E.D.; Blaes, A.H.; Cetin, K.; Chia, V.M.; Stryker, S.; Pinzone, J.J.; Acquavella, J.F. Estimated number of prevalent cases of metastatic bone disease in the US adult population. Clin. Epidemiol. 2012, 4, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caissie, A.; Zeng, L.; Nguyen, J.; Zhang, L.; Jon, F.; Dennis, K.; Holden, L.; Culleton, S.; Koo, K.; Tsao, M.; et al. Assessment of Health-related Quality of Life with the European Organization for Research and Treatment of Cancer QLQ-C15-PAL after Palliative Radiotherapy of Bone Metastases. Clin. Oncol. 2012, 24, 125–133. [Google Scholar] [CrossRef]
- Janjan, N.A. Radiation for bone metastases: Conventional techniques and the role of systemic radiopharmaceuticals. Cancer 1997, 80, 1628–1645. [Google Scholar] [CrossRef]
- Wu, J.S.-Y.; Wong, R.K.; Johnston, M.; Bezjak, A.; Whelan, T. Meta-analysis of dose-fractionation radiotherapy trials for the palliation of painful bone metastases. Int. J. Radiat. Oncol. 2003, 55, 594–605. [Google Scholar] [CrossRef]
- Lee, H.-L.; Kuo, C.-C.; Tsai, J.-T.; Chen, C.-Y.; Wu, M.-H.; Chiou, J.-F. Magnetic Resonance-Guided Focused Ultrasound Versus Conventional Radiation Therapy for Painful Bone Metastasis. J. Bone Jt. Surg. 2017, 99, 1572–1578. [Google Scholar] [CrossRef]
- Namba, H.; Kawasaki, M.; Izumi, M.; Ushida, T.; Takemasa, R.; Ikeuchi, M. Effects of MRgFUS Treatment on Musculoskeletal Pain: Comparison between Bone Metastasis and Chronic Knee/Lumbar Osteoarthritis. Pain Res. Manag. 2019, 2019, 4867904. [Google Scholar] [CrossRef]
- Masciocchi, C.; Arrigoni, F.; La Marra, A.; Mariani, S.; Zugaro, L.; Barile, A. Treatment of focal benign lesions of the bone: MRgFUS and RFA. Br. J. Radiol. 2016, 89, 20150356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Errico, A. MRgFUS—Non invasive treatment for patients with painful bone metastasis. Nat. Rev. Clin. Oncol. 2014, 11, 303. [Google Scholar] [CrossRef] [PubMed]
- Anzidei, M.; Bazzocchi, A.; Gagliardo, C.; Catalano, C.; Napoli, A.; Scipione, R. HIFU for Bone Metastases and other Musculoskeletal Applications. Semin. Interv. Radiol. 2018, 35, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Catane, R.; Beck, A.; Inbar, Y.; Rabin, T.; Shabshin, N.; Hengst, S.; Pfeffer, R.; Hanannel, A.; Dogadkin, O.; Liberman, B.; et al. MR-guided focused ultrasound surgery (MRgFUS) for the palliation of pain in patients with bone metastases—preliminary clinical experience. Ann. Oncol. 2007, 18, 163–167. [Google Scholar] [CrossRef]
- Arrigoni, F.; Barile, A.; Zugaro, L.; Splendiani, A.; di Cesare, E.; Caranci, F.; Ierardi, A.M.; Floridi, C.; Angileri, A.S.; Reginelli, A.; et al. Intra-articular benign bone lesions treated with Magnetic Resonance-guided Focused Ultrasound (MRgFUS): Imaging follow-up and clinical results. Med. Oncol. 2017, 34, 55. [Google Scholar] [CrossRef]
- Marincola, B.C.; Pediconi, F.; Anzidei, M.; Miglio, E.; Di Mare, L.; Telesca, M.; Mancini, M.; D’Amati, G.; Monti, M.; Catalano, C.; et al. High-intensity focused ultrasound in breast pathology: Non-invasive treatment of benign and malignant lesions. Expert Rev. Med. Devices 2014, 12, 191–199. [Google Scholar] [CrossRef]
- Anzidei, M.; Marincola, B.C.; Bezzi, M.; Brachetti, G.; Nudo, F.; Cortesi, E.; Berloco, P.; Catalano, C.; Napoli, A. Magnetic Resonance–Guided High-Intensity Focused Ultrasound Treatment of Locally Advanced Pancreatic Adenocarcinoma. Investig. Radiol. 2014, 49, 759–765. [Google Scholar] [CrossRef]
- Gagliardo, C.; Geraci, L.; Napoli, A.; Giugno, A.; Cortegiani, A.; Canzio, D.; Giarratano, A.; Franzini, A.; Iacopino, D.G.; Catalano, C.; et al. Terapia chirurgica trans-cranica non invasiva mediante ultrasuoni focalizzati guidati da risonanza magnetica per il trattamento di disordini neurologici. Recenti Prog. Med. 2016, 107, 242–245. [Google Scholar]
- Chu, K.F.; Dupuy, D.E. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat. Rev. Cancer 2014, 14, 199–208. [Google Scholar] [CrossRef]
- Kim, H.; Park, B.K.; Kim, C.K. Spontaneous Regression of Pulmonary and Adrenal Metastases Following Percutaneous Radiofrequency Ablation of a Recurrent Renal Cell Carcinoma. Korean J. Radiol. 2008, 9, 470–472. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.-C.; Lee, H.-L.; Kuo, C.-C.; Chen, C.-Y.; Hsieh, K.L.-C.; Wu, M.-H.; Wen, Y.-C.; Yu, H.-W.; Hsu, F.-C.; Tsai, J.-T.; et al. Prognostic and predictive factors for clinical and radiographic responses in patients with painful bone metastasis treated with magnetic resonance-guided focused ultrasound surgery. Int. J. Hyperth. 2019, 36, 931–936. [Google Scholar] [CrossRef]
- Takaki, H.; Cornelis, F.; Kako, Y.; Kobayashi, K.; Kamikonya, N.; Yamakado, K. Thermal ablation and immunomodulation: From preclinical experiments to clinical trials. Diagn. Interv. Imaging 2017, 98, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Erinjeri, J.P.; Thomas, C.T.; Samoilia, A.; Fleisher, M.; Gonen, M.; Sofocleous, C.T.; Thornton, R.H.; Siegelbaum, R.H.; Covey, A.M.; Brody, L.A.; et al. Image-guided Thermal Ablation of Tumors Increases the Plasma Level of Interleukin-6 and Interleukin-10. J. Vasc. Interv. Radiol. 2013, 24, 1105–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, F.; Gravante, G.; Bhardwaj, N.; Strickland, A.; Basit, R.; West, K.; Sorge, R.; Dennison, A.; Lloyd, D.M. Changes in interleukin-1β and 6 after hepatic microwave tissue ablation compared with radiofrequency, cryotherapy and surgical resections. Am. J. Surg. 2010, 200, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, S.; Shimada, M.; Utsunomiya, T.; Imura, S.; Morine, Y.; Ikemoto, T.; Takasu, C.; Saito, Y.; Yamada, S. Epithelial–mesenchymal transition-related genes are linked to aggressive local recurrence of hepatocellular carcinoma after radiofrequency ablation. Cancer Lett. 2016, 375, 47–50. [Google Scholar] [CrossRef]
- Chalise, P.; Ni, Y.; Fridley, B.L. Network-based integrative clustering of multiple types of genomic data using non-negative matrix factorization. Comput. Biol. Med. 2020, 118, 103625. [Google Scholar] [CrossRef]
- Shen, R.; Olshen, A.B.; Ladanyi, M. Integrative clustering of multiple genomic data types using a joint latent variable model with application to breast and lung cancer subtype analysis. Bioinformatics 2009, 25, 2906–2912. [Google Scholar] [CrossRef]
- Xiao, Y.; Jin, Y.; Hao, K. Adaptive Prototypical Networks With Label Words and Joint Representation Learning for Few-Shot Relation Classification. arXiv 2021, arXiv:2101.03526. [Google Scholar] [CrossRef]
- Lu, H.-Y.; Fan, C.; Song, X.; Fang, W. A novel few-shot learning based multi-modality fusion model for COVID-19 rumor detection from online social media. PeerJ Comput. Sci. 2021, 7, e688. [Google Scholar] [CrossRef]
- Jiang, P.; Ning, W.; Shi, Y.; Liu, C.; Mo, S.; Zhou, H.; Liu, K.; Guo, Y. FSL-Kla: A few-shot learning-based multi-feature hybrid system for lactylation site prediction. Comput. Struct. Biotechnol. J. 2021, 19, 4497–4509. [Google Scholar] [CrossRef]
- Weng, J.; Ding, Y.; Hu, C.; Zhu, X.-F.; Liang, B.; Yang, J.; Cheng, J. Meta-neural-network for real-time and passive deep-learning-based object recognition. Nat. Commun. 2020, 11, 6309. [Google Scholar] [CrossRef]
- Sonabend, R.; Király, F.J.; Bender, A.; Bischl, B.; Lang, M. mlr3proba: An R package for machine learning in survival analysis. Bioinformatics 2021, 37, 2789–2791. [Google Scholar] [CrossRef] [PubMed]
- Lai, N.; Kan, M.; Han, C.; Song, X.; Shan, S. Corrections to “Learning to Learn Adaptive Classifier-Predictor for Few-Shot Learning” [Aug 21 3458-3470]. IEEE Trans. Neural Netw. Learn. Syst. 2021, 32, 3784. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Wu, W.; Huang, Y.; Ge, W.; Liu, S. Incomplete radiofrequency ablation accelerates proliferation and angiogenesis of residual lung carcinomas via HSP70/HIF-1α. Oncol. Rep. 2016, 36, 659–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Zu’Bi, M.; Mohan, A. Modelling of combination therapy using implantable anticancer drug delivery with thermal ablation in solid tumor. Sci. Rep. 2020, 10, 19366. [Google Scholar] [CrossRef]
- Wang, S.-W.; Sun, Y.-M. The IL-6/JAK/STAT3 pathway: Potential therapeutic strategies in treating colorectal cancer. Int. J. Oncol. 2014, 44, 1032–1040. [Google Scholar] [CrossRef] [Green Version]
- Larouche, J.; Sheoran, S.; Maruyama, K.; Martino, M.M. Immune Regulation of Skin Wound Healing: Mechanisms and Novel Therapeutic Targets. Adv. Wound Care 2018, 7, 209–231. [Google Scholar] [CrossRef]
- Qiu, Y.L.; Zheng, H.; Devos, A.; Selby, H.; Gevaert, O. A meta-learning approach for genomic survival analysis. Nat. Commun. 2020, 11, 6350. [Google Scholar] [CrossRef]
- Vassiliou, V.; Andreopoulos, D. Assessment of therapeutic response in patients with metastatic skeletal disease: Suggested modifications for the MDA response classification criteria. Br. J. Cancer 2010, 103, 925–926. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Number of Patents | 20 |
| Age, median (range), year | 63.95 10.57 (46–83) |
| Gender | |
| Male | 8 (40%) |
| Female | 12 (60%) |
| Pretreatment KPS, median (range) | 83 7.33 (70–90) |
| Primary Tumor | |
| Breast cancer | 6 (30%) |
| Lung cancer | 8 (40%) |
| Prostate cancer | 1 (5%) |
| Colon cancer | 3 (15%) |
| Renal cell carcinoma | 2 (10%) |
| Treated Site | |
| Rib | 1 (5%) |
| Sternum | 1 (5%) |
| Acetabulum | 1 (5%) |
| Ilium | 3 (15%) |
| Ischium | 1 (5%) |
| Sacroiliac joint | 6 (30%) |
| Sacrum | 5 (25%) |
| Scapula | 2 (10%) |
| Pre-treatment Pain Score (NRS) | |
| Mean ± std (range) | 6.65 ± 1.72 (4–9) |
| 4–6 | 9 (45%) |
| 7–10 | 11 (55%) |
| Cytokine | Pretreatment (Mean SD) | Post-Treatment (Mean SD) | p Value |
|---|---|---|---|
| IL-6 | 5.54 3.81 | 3.62 4.38 | 0.049 * |
| Exotaxin | 27.37 12.91 | 20.76 12.80 | 0.067 |
| IL-13 | 3.50 2.82 | 2.371 1.45 | 0.075 |
| IP-10 | 442.21 394.86 | 316.28 293.8 | 0.004 * |
| IL-1b | 1.64 1.43 | 1.85 2.27 | 0.514 |
| IL-1ra | 86.11 159.23 | 137.23 369.18 | 0.313 |
| IL-2 | 7.31 25.04 | 17.73 71.01 | 0.217 |
| IL-4 | 0.72 0.37 | 0.72 0.45 | 0.920 |
| IL-5 | 6.35 3.57 | 5.93 3.19 | 0.200 |
| IL-7 | 4.41 1.81 | 4.03 1.48 | 0.182 |
| IL-8 | 15.52 45.29 | 8.21 6.98 | 0.472 |
| IL-9 | 10.39 5.15 | 9.29 4.83 | 0.188 |
| IL-10 | 13.96 40.13 | 32.69 122.5 | 0.335 |
| IL-12 | 14.68 19.33 | 25.56 69.23 | 0.366 |
| IL-17 | 12.18 12.16 | 15.53 26.36 | 0.468 |
| FGF | 17.51 12.98 | 19.84 25.09 | 0.506 |
| G-CSF | 32.99 60.98 | 55.98 160.06 | 0.327 |
| INF-gamma | 48.21 33.46 | 48.94 40.01 | 0.889 |
| MCP-1 | 7.01 13.40 | 7.27 19.96 | 0.870 |
| MIP-1a | 2.223 2.74 | 2.362 4.36 | 0.759 |
| MIP-1b | 15.13 5.42 | 13.30 5.73 | 0.192 |
| PDGF | 129.72 128.51 | 203.48 278.72 | 0.296 |
| RANTES | 1388.5 306.75 | 1492.9 429.96 | 0.425 |
| TNF-α | 26.96 41.13 | 27.80 49.54 | 0.733 |
| VEGF | 10.06 11.96 | 15.26 35.62 | 0.394 |
| Treatment Parameters | Mean SD |
|---|---|
| Number of Sonication | 21.42 6.21 |
| Duration of treatment (min) | 74.38 41.21 |
| Average acoustic power (W) | 51.08 19.97 |
| Average energy applied (J) | 1029.93 360.46 |
| Temperature (°C) | 67.71 7.36 |
| Parameter | Univariate Analysis: Logistic Regression | Multivariable Analyses: Logistic Regression | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age, median (range), years | 0.96 | 0.83–1.07 | 0.51 | 1.02 | 0.83–1.24 | 0.81 |
| Gender (male vs. female) | 0.15 | 0.01–1.52 | 0.13 | |||
| Pretreatment pain score (NRS) | 0.85 | 0.41–1.66 | 0.64 | |||
| Pretreatment KPS | 1.27 | 1.05–1.74 | 0.04 * | 1.23 | 1.00–1.74 | 0.04 * |
| IL-1b | 1.46 | 0.61–10.39 | 0.53 | |||
| IL-6 | 0.72 | 0.48–0.96 | 0.04 * | 0.77 | 0.48–1.08 | 0.16 |
| Exotaxin | 0.94 | 0.83–1.03 | 0.19 | |||
| IL-10 | 1.08 | 0.98–1.87 | 0.68 | |||
| IL-13 | 1.13 | 0.75–2.23 | 0.62 | |||
| IP-10 | 0.99 | 0.98–0.99 | 0.07 | |||
| IL-17a | 1.06 | 0.95–1.36 | 0.43 | |||
| Relationship Formalization | Accuracy | AUC | AIC |
|---|---|---|---|
| Logistic regression: | 0.88 | 0.88 | 19.35 |
| Few-shot learning model: | 0.95 | 0.95 | 17.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, F.-C.; Lee, H.-L.; Chen, Y.-J.; Shen, Y.-A.; Tsai, Y.-C.; Wu, M.-H.; Kuo, C.-C.; Lu, L.-S.; Yeh, S.-D.; Huang, W.-S.; et al. A Few-Shot Learning Approach Assists in the Prognosis Prediction of Magnetic Resonance-Guided Focused Ultrasound for the Local Control of Bone Metastatic Lesions. Cancers 2022, 14, 445. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020445
Hsu F-C, Lee H-L, Chen Y-J, Shen Y-A, Tsai Y-C, Wu M-H, Kuo C-C, Lu L-S, Yeh S-D, Huang W-S, et al. A Few-Shot Learning Approach Assists in the Prognosis Prediction of Magnetic Resonance-Guided Focused Ultrasound for the Local Control of Bone Metastatic Lesions. Cancers. 2022; 14(2):445. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020445
Chicago/Turabian StyleHsu, Fang-Chi, Hsin-Lun Lee, Yin-Ju Chen, Yao-An Shen, Yi-Chieh Tsai, Meng-Huang Wu, Chia-Chun Kuo, Long-Sheng Lu, Shauh-Der Yeh, Wen-Sheng Huang, and et al. 2022. "A Few-Shot Learning Approach Assists in the Prognosis Prediction of Magnetic Resonance-Guided Focused Ultrasound for the Local Control of Bone Metastatic Lesions" Cancers 14, no. 2: 445. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020445